
Personality and Pain Outcomes in Rheumatic Disease: The Mediating Role of Psychological Flexibility

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
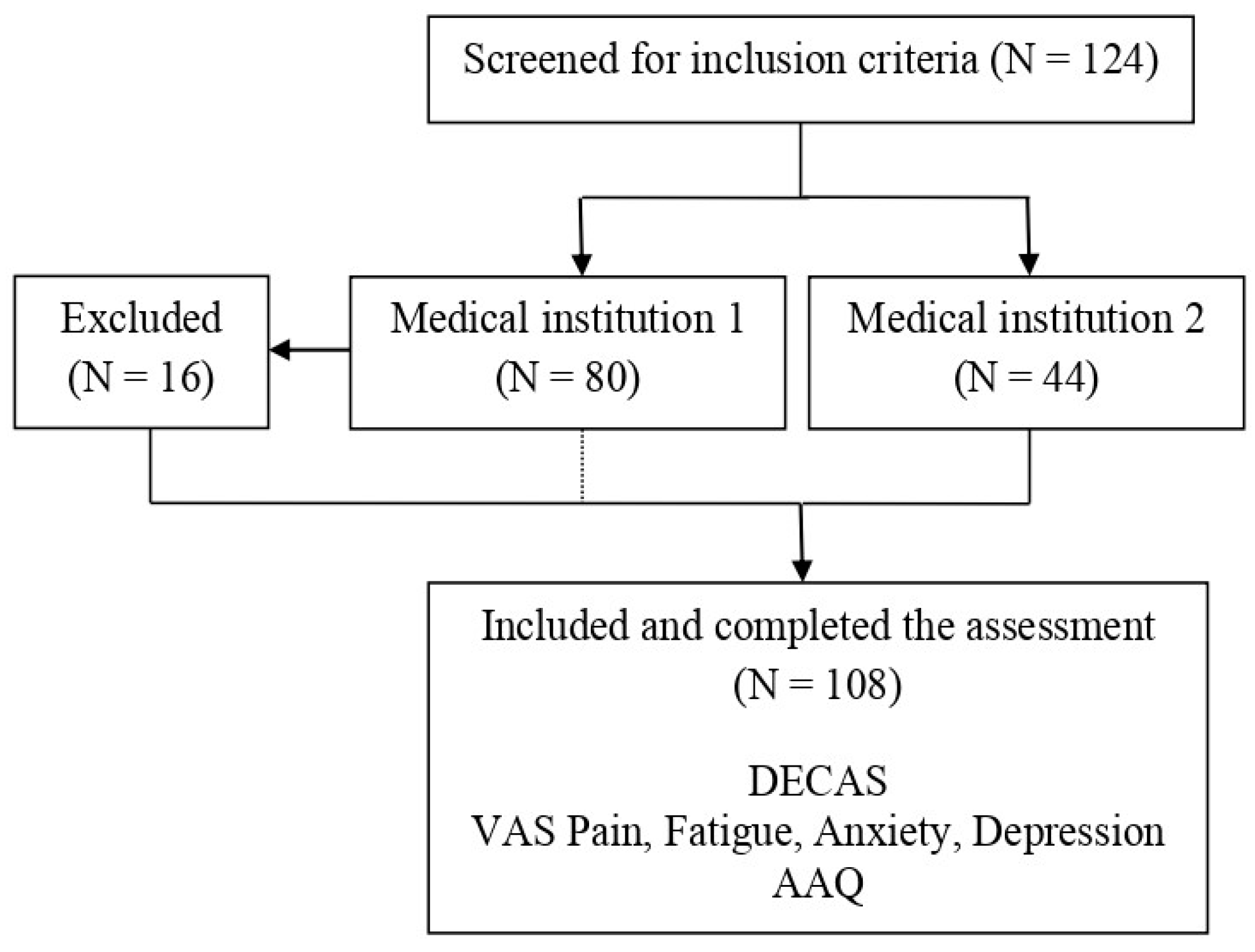
2.1. Participants
2.2. Ethical Considerations
2.3. Measures
2.4. Design and Procedure
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Correlations
3.3. Multiple Regression Models
3.4. Mediation Results
4. Discussion
4.1. Correlations and Multiple Regression Results
4.2. Results of the Mediation Analyses
4.3. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Nahin, R.L.; Feinberg, T.; Kapos, F.P.; Terman, G.W. Estimated Rates of Incident and Persistent Chronic Pain among US Adults, 2019–2020. JAMA Netw Open 2023, 6, e2313563. [Google Scholar] [CrossRef]
- De Ridder, D.; Adhia, D.; Vanneste, S. The Anatomy of Pain and Suffering in the Brain and Its Clinical Implications. Neurosci. Biobehav. Rev. 2021, 130, 125–146. [Google Scholar] [CrossRef]
- Van Damme, S.; Becker, S.; Van der Linden, D. Tired of pain? Toward a better understanding of fatigue in chronic pain. Pain 2018, 159, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Gómez Penedo, J.M.; Rubel, J.A.; Blättler, L.; Schmidt, S.J.; Stewart, J.; Egloff, N.; Grosse Holtforth, M. The Complex Interplay of Pain, Depression, and Anxiety Symptoms in Patients with Chronic Pain: A Network Approach. Clin. J. Pain 2020, 36, 249–259. [Google Scholar] [CrossRef]
- Kaiser, T.; Herzog, P.; Voderholzer, U.; Brakemeier, E.-L. Unraveling the Comorbidity of Depression and Anxiety in a Large Inpatient Sample: Network Analysis to Examine Bridge Symptoms. Depress. Anxiety 2021, 38, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Marian, S.; Costantini, G.; Macsinga, I.; Sava, F.A. The Dynamic Interplay of Anxious and Depressive Symptoms in a Sample of Undergraduate Students. J. Psychopathol. Behav. Assess. 2023, 45, 150–159. [Google Scholar] [CrossRef]
- Brandl, F.; Weise, B.; Mulej Bratec, S.; Jassim, N.; Hoffmann Ayala, D.; Bertram, T.; Ploner, M.; Sorg, C. Common and specific large-scale brain changes in major depressive disorder, anxiety disorders, and chronic pain: A transdiagnostic multimodal meta-analysis of structural and functional MRI studies. Neuropsychopharmacology 2022, 47, 1071–1080. [Google Scholar] [CrossRef]
- Olthof, M.; Hasselman, F.; Oude Maatman, F.; Bosman, A.M.T.; Lichtwarck-Aschoff, A. Complexity theory of psychopathology. J. Psychopathol. Clin. Sci. 2023, 132, 314–323. [Google Scholar] [CrossRef]
- Eaton, N.R.; Bringmann, L.F.; Elmer, T.; Fried, E.I.; Forbes, M.K.; Greene, A.L.; Krueger, R.F.; Kotov, R.; McGorry, P.D.; Mei, C.; et al. A review of approaches and models in psychopathology conceptualization research. Nat. Rev. Psychol. 2023, 2, 622–636. [Google Scholar] [CrossRef]
- Naylor, B.; Boag, S.; Gustin, S.M. New evidence for a pain personality? A critical review of the last 120 years of pain and personality. Scand. J. Pain 2017, 17, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Bucourt, E.; Martaillé, V.; Mulleman, D.; Goupille, P.; Joncker-Vannier, I.; Huttenberger, B.; Reveillere, C.; Courtois, R. Comparison of the Big Five personality traits in fibromyalgia and other rheumatic diseases. Jt. Bone Spine 2017, 84, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.; Ding, D. Which outcome variables are associated with psychological inflexibility/flexibility for chronic pain patients? A three level meta-analysis. Front. Psychol. 2022, 13, 1069748. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Morley, S. The psychological flexibility model: A basis for integration and progress in psychological approaches to chronic pain management. J. Pain 2014, 15, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Bergner, R.M. What Is Personality? Two Myths and a Definition. New Ideas Psychol. 2020, 57, 100759. [Google Scholar] [CrossRef]
- Sava, F.A.; Popa, R.I. Personality types based on the Big Five model. A cluster analysis over the Romanian population. Cogn. Brain Behav. 2011, 15, 359–384. [Google Scholar]
- McCrae, R.R.; Costa, P.T., Jr. Introduction to the empirical and theoretical status of the five-factor model of personality traits. In Personality Disorders and the Five-Factor Model of Personality, 3rd ed.; Widiger, T.A., Costa, P.T., Jr., Eds.; American Psychological Association: Washington, DC, USA, 2013; pp. 15–27. [Google Scholar] [CrossRef]
- Barlow, D.H.; Curreri, A.J.; Woodard, L.S. Neuroticism and Disorders of Emotion: A New Synthesis. Curr. Dir. Psychol. 2021, 30, 410–417. [Google Scholar] [CrossRef]
- Meng, W.; Adams, M.J.; Reel, P.; Rajendrakumar, A.; Huang, Y.; Deary, I.J.; Palmer, C.N.A.; McIntosh, A.M.; Smith, B.H. Genetic Correlations between Pain Phenotypes and Depression and Neuroticism. Eur. J. Hum. Genet. 2020, 28, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Hanney, W.J.; Wilson, A.T.; Smith, T.; Shiley, C.; Howe, J.; Kolber, M.J. Personality Type and Chronic Pain: The Relationship between Personality Profile and Chronic Low Back Pain Using Eysenck’s Personality Inventory. NeuroSci 2022, 3, 677–686. [Google Scholar] [CrossRef]
- Barlow, D.H.; Ellard, K.K.; Sauer-Zavala, S.; Bullis, J.R.; Carl, J.R. The Origins of Neuroticism. Perspect. Psychol. Sci. 2014, 9, 481–496. [Google Scholar] [CrossRef]
- Suso-Ribera, C.; Gallardo-Pujol, D. Personality and Health in Chronic Pain: Have We Failed to Appreciate a Relationship? Pers. Individ. Differ. 2016, 96, 7–11. [Google Scholar] [CrossRef]
- Bogg, T.; Roberts, B.W. Conscientiousness and Health-Related Behaviors: A Meta-Analysis of the Leading Behavioral Contributors to Mortality. Psychol. Bull. 2004, 130, 887–919. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.K.; Waite, L.; Van Wyngaarden, J.J.; Meyer, A.R.; Koppenhaver, S.L. Beyond yellow flags: The Big-Five personality traits and psychologically informed musculoskeletal rehabilitation. Musculoskelet. Care 2023, 21, 1161–1174. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, Processes and Outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef]
- Monestès, J.L.; Karekla, M.; Jacobs, N.; Michaelides, M.P.; Hooper, N.; Kleen, M.; Ruiz, F.J.; Miselli, G.; Presti, G.; Luciano, C.; et al. Experiential avoidance as a common psychological process in European cultures. Eur. J. Psychol. Assess. 2018, 34, 247–257. [Google Scholar] [CrossRef]
- Vaughan-Johnston, T.I.; Quickert, R.E.; MacDonald, T.K. Psychological Flexibility under Fire: Testing the Incremental Validity of Experiential Avoidance. Pers. Individ. Differ. 2017, 105, 335–349. [Google Scholar] [CrossRef]
- Akbari, M.; Seydavi, M.; Hosseini, Z.S.; Krafft, J.; Levin, M.E. Experiential avoidance in depression, anxiety, obsessive-compulsive related, and posttraumatic stress disorders: A comprehensive systematic review and meta-analysis. J. Context. Behav. Sci. 2022, 24, 65–78. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, C.; Coto-Lesmes, R.; Martínez-Loredo, V.; Cuesta-Izquierdo, M. Psychological Inflexibility, Anxiety and Depression: The Moderating Role of Cognitive Fusion, Experiential Avoidance and Activation. Psicothema 2022, 34, 240–248. [Google Scholar] [CrossRef]
- Popa, C.O.; Rus, A.V.; Lee, W.C.; Cojocaru, C.; Schenk, A.; Văcăraș, V.; Olah, P.; Mureșan, S.; Szasz, S.; Bredicean, C. The Relation between Negative Automatic Thoughts and Psychological Inflexibility in Schizophrenia. J. Clin. Med. 2022, 11, 871. [Google Scholar] [CrossRef]
- Cookson, C.; Luzon, O.; Newland, J.; Kingston, J. Examining the Role of Cognitive Fusion and Experiential Avoidance in Predicting Anxiety and Depression. Psychol. Psychother. Theory Res. Pract. 2020, 93, 456–473. [Google Scholar] [CrossRef]
- Karayannis, N.V.; Sturgeon, J.A.; Kemani, M.K.; Mackey, S.C.; Greco, C.M.; Wicksell, R.K.; McCracken, L.M. Pain acceptance and psychological inflexibility predict pain interference outcomes for persons with chronic pain receiving pain psychology. Scand. J. Pain. 2023, 23, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Kwok, S.S.; Chan, E.C.; Chen, P.P.; Lo, B.C. The “self” in pain: The role of psychological inflexibility in chronic pain adjustment. J. Behav. Med. 2016, 39, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Gentili, C.; Rickardsson, J.; Zetterqvist, V.; Simons, L.E.; Lekander, M.; Wicksell, R.K. Psychological Flexibility as a Resilience Factor in Individuals with Chronic Pain. Front. Psychol. 2019, 10, 2016. [Google Scholar] [CrossRef] [PubMed]
- Semcho, S.A.; Southward, M.W.; Stumpp, N.E.; MacLean, D.L.; Hood, C.O.; Wolitzky-Taylor, K.; Sauer-Zavala, S. Aversive reactivity: A transdiagnostic functional bridge between neuroticism and avoidant behavioral coping. J. Emot. Psychopathol. 2023, 1, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Maestre, C.; Esteve, R. Disposition and Adjustment to Chronic Pain. Curr. Pain. Headache Rep. 2013, 17, 312. [Google Scholar] [CrossRef] [PubMed]
- Steenhaut, P.; Rossi, G.; Demeyer, I.; De Raedt, R. How is personality related to well-being in older and younger adults? The role of psychological flexibility. Int. Psychogeriatr. 2019, 31, 1355–1365. [Google Scholar] [CrossRef]
- Sava, F. Inventarul de Personalitate DECAS; ArtPress: Timişoara, Romania, 2008. [Google Scholar]
- Begum, M.R.; Hossain, M.A. Validity and reliability of visual analogue scale (VAS) for pain measurement. J. Med. Case Rep. Rev. 2019, 2, 394–402. [Google Scholar]
- Modarresi, S.; Lukacs, M.J.; Ghodrati, M.; Salim, S.; MacDermid, J.C.; Walton, D.M.; CATWAD Consortium Group. A Systematic Review and Synthesis of Psychometric Properties of the Numeric Pain Rating Scale and the Visual Analog Scale for Use in People with Neck Pain. Clin. J. Pain 2021, 38, 132–148. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.E. Management of Fatigue in Rheumatoid Arthritis. RMD Open 2020, 6, e001084. [Google Scholar] [CrossRef]
- Wolfe, F. Fatigue assessments in rheumatoid arthritis: Comparative performance of visual analog scales and longer fatigue quetionnaires in 7760 patients. J. Rheumatol. 2004, 31, 1896–1902. [Google Scholar]
- Williams, V.S.; Morlock, R.J.; Feltner, D. Psychometric evaluation of a visual analog scale for the assessment of anxiety. Health Qual. Life Outcomes 2010, 8, 57. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Kohler, I.V.; Kämpfen, F. A Single-Item Visual Analogue Scale (VAS) Measure for Assessing Depression Among College Students. Community Ment. Health J. 2020, 56, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary Psychometric Properties of the Acceptance and Action Questionnaire–II: A Revised Measure of Psychological Inflexibility and Experiential Avoid-873 ance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef] [PubMed]
- Szabó, K.G.; Vargha, J.L.; Balázsi, R.; Bartalus, J.; Bogdan, V. Measuring Psychological Flexibility: Preliminary Data on the Pschometric Properties of the Romanian Version of the Acceptance and Action Questionnaire (AAQ-II). J. Cogn. Behav. Psychother. 2011, 11, 67–82. [Google Scholar]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2011, 48, 1–36. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. In R Foundation for Statistical Computing; R Core Team: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 22 April 2024).
- Doorley, J.D.; Goodman, F.R.; Kelso, K.C.; Kashdan, T.B. Psychological flexibility: What we know, what we do not know, and what we think we know. Soc. Pers. Psychol. Compass 2020, 14, 1–11. [Google Scholar] [CrossRef]
- Rizzo, J.M.; Schwartz, R.C. The effect of mindfulness, psychological flexibility, and emotional intelligence on self-efficacy and functional outcomes among chronic pain clients. J. Contemp. Psychother. 2021, 51, 109–116. [Google Scholar] [CrossRef]
- Zhang, R.P.; Tsingan, L. Extraversion and Neuroticism Mediate Associations Between Openness, Conscientiousness, and Agreeableness and Affective Well-Being. J. Happiness Stud. 2014, 15, 1377–1388. [Google Scholar] [CrossRef]
- Spark, A.; O’Connor, P.J. Extraversion Rather than Neuroticism Is the Dominant Trait Predictor of Forecasted Affect in Relation to Social Situations. Pers. Individ. Differ. 2020, 160, 109934. [Google Scholar] [CrossRef]
- Magariños López, M.; Lobato Rodríguez, M.J.; Menéndez García, Á.; García-Cid, S.; Royuela, A.; Pereira, A. Psychological Profile in Women with Chronic Pelvic Pain. J. Clin. Med. 2022, 11, 6345. [Google Scholar] [CrossRef]
- Rouch, I.; Strippoli, M.-P.F.; Dorey, J.-M.; Ranjbar, S.; Laurent, B.; von Gunten, A.; Preisig, M. Psychiatric disorders, personality traits, and childhood traumatic events predicting incidence and persistence of chronic pain: Results from the CoLaus| PsyCoLaus study. Pain. 2023, 164, 2084–2092. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Kaufman, S.B.; Smillie, L.D. Unique Associations Between Big Five Personality Aspects and Multiple Dimensions of Well-Being. J. Pers. 2018, 86, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Bar-Shalita, T.; Cermak, S.A. Multi-sensory responsiveness and personality traits predict daily pain sensitivity. Front. Integr. Neurosci. 2020, 13, 77. [Google Scholar] [CrossRef] [PubMed]
- Stephan, Y.; Sutin, A.R.; Luchetti, M.; Canada, B.; Terracciano, A. Personality and fatigue: Meta-analysis of seven prospective studies. Sci. Rep. 2022, 12, 9156. [Google Scholar] [CrossRef] [PubMed]
- Littlefield, A.K.; Lane, S.P.; Gette, J.A.; Watts, A.L.; Sher, K.J. The “Big Everything”: Integrating and investigating dimensional models of psychopathology, personality, personality pathology, and cognitive functioning. Personal. Disord. 2021, 12, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Lyon, K.A.; Juhasz, G.; Brown, L.J.E.; Elliott, R. Big Five personality facets explaining variance in anxiety and depressive symptoms in a community sample. J. Affect. Dis. 2020, 274, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Kadimpati, S.; Zale, E.L.; Hooten, M.W.; Ditre, J.W.; Warner, D.O. Associations between Neuroticism and Depression in Relation to Catastrophizing and Pain-Related Anxiety in Chronic Pain Patients. PLoS ONE 2015, 10, e0126351. [Google Scholar] [CrossRef] [PubMed]
- Mineka, S.; Williams, A.L.; Wolitzky-Taylor, K.; Vrshek-Schallhorn, S.; Craske, M.G.; Hammen, C.; Zinbarg, R.E. Five-year prospective neuroticism–stress effects on major depressive episodes: Primarily additive effects of the general neuroticism factor and stress. J. Abnorm. Psychol. 2020, 129, 646–657. [Google Scholar] [CrossRef] [PubMed]
- Latzman, R.D.; Masuda, A. Examining Mindfulness and Psychological Inflexibility within the Framework of Big Five Personality. Pers. Individ. Differ. 2013, 55, 129–134. [Google Scholar] [CrossRef]
- Ding, D.; Zheng, M. Associations Between Six Core Processes of Psychological Flexibility and Functioning for Chronic Pain Patients: A Three-Level Meta-Analysis. Front. Psychiatry 2022, 13, 893150. [Google Scholar] [CrossRef]
- Angarita-Osorio, N.; Pérez-Aranda, A.; Feliu-Soler, A.; Andrés-Rodríguez, L.; Borràs, X.; Suso-Ribera, C.; Slim, M.; Herrera-Mercadal, P.; Fernández-Vergel, R.; Blanco, M.E.; et al. Patients with Fibromyalgia Reporting Severe Pain but Low Impact of the Syndrome: Clinical and Pain-Related Cognitive Features. Pain. Pract. 2020, 20, 255–261. [Google Scholar] [CrossRef]
- Adamowicz, J.L.; Vélez-Bermúdez, M.; Thomas, E.B.K. Fatigue severity and avoidance among individuals with chronic disease: A meta-analysis. J. Psychosom. Res. 2022, 159, 110951. [Google Scholar] [CrossRef] [PubMed]
- Bardeen, J.R.; Fergus, T.A. The Interactive Effect of Cognitive Fusion and Experiential Avoidance on Anxiety, Depression, Stress and Posttraumatic Stress Symptoms. J. Context. Behav. Sci. 2016, 5, 1–6. [Google Scholar] [CrossRef]
- Spinhoven, P.; Drost, J.; de Rooij, M.; van Hemert, A.M.; Penninx, B.W. A Longitudinal Study of Experiential Avoidance in Emotional Disorders. Behav. Ther. 2014, 45, 840–850. [Google Scholar] [CrossRef]
- Owiredua, C.; Flink, I.; Vixner, L.; Äng, B.O.; Tseli, E.; Boersma, K. The Context Matters: A Retrospective Analysis of Life Stage at Chronic Pain Onset in Relation to Pain Characteristics and Psychosocial Outcomes. J. Pain. Res. 2020, 13, 2685–2695. [Google Scholar] [CrossRef] [PubMed]
- Planelles, B.; Margarit, C.; Inda, M.d.M.; Ballester, P.; Muriel, J.; Barrachina, J.; Ajo, R.; Esteban, M.D.; Peiró, A.M. Gender based differences, pharmacogenetics and adverse events in chronic pain management. Pharmacogenom. J. 2020, 20, 320–328. [Google Scholar] [CrossRef]
- Casale, R.; Atzeni, F.; Bazzichi, L.; Beretta, G.; Costantini, E.; Sacerdote, P.; Tassorelli, C. Pain in women: A perspective review on a relevant clinical issue that deserves prioritization. Pain. Ther. 2021, 10, 287–314. [Google Scholar] [CrossRef]
- Panayiotou, G.; Karekla, M.; Leonidou, C. Coping through avoidance may explain gender disparities in anxiety. J. Context. Behav. Sci. 2017, 6, 215–220. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Burton, C.L. Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspect. Psychol. Sci. 2013, 8, 591–612. [Google Scholar] [CrossRef]
- Åkerblom, S.; Perrin, S.; Fischer, M.R.; McCracken, L.M. Predictors and mediators of outcome in cognitive behavioral therapy for chronic pain: The contributions of psychological flexibility. J. Behav. Med. 2021, 44, 111–122. [Google Scholar] [CrossRef]
- Écija, C.; Luque-Reca, O.; Suso-Ribera, C.; Catala, P.; Peñacoba, C. Associations of Cognitive Fusion and Pain Catastrophizing with Fibromyalgia Impact through Fatigue, Pain Severity, and Depression: An Exploratory Study Using Structural Equation Modeling. J. Clin. Med. 2020, 9, 1763. [Google Scholar] [CrossRef]
- Wicksell, R.K.; Olsson, G.L.; Hayes, S.C. Psychological flexibility as a mediator of improvement in Acceptance and Commitment Therapy for patients with chronic pain following whiplash. Eur. J. Pain 2010, 14, 1059-e1. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Scott, W.; McCracken, L.M. Change in fatigue in acceptance and commitment therapy-based treatment for chronic pain and its association with enhanced psychological flexibility. Eur. J. Pain 2020, 24, 234–247. [Google Scholar] [CrossRef]
- Catala, P.; Gutierrez, L.; Écija, C.; Serrano del Moral, Á.; Peñacoba, C. Do Cognitive Abilities Influence Physical and Mental Fatigue in Patients with Chronic Pain after Walking According to a Clinical Guideline for Physical Exercise? Int. J. Environ. Res. Public Health 2021, 18, 13148. [Google Scholar] [CrossRef] [PubMed]
- Sutin, A.R.; Stephan, Y.; Luchetti, M.; Terracciano, A. The Prospective Association between Personality Traits and Persistent Pain and Opioid Medication Use. J. Psychosom. Res. 2019, 123, 109721. [Google Scholar] [CrossRef]
- Ehda, G.R.; Mousavi Nasab, S.M.H.; Ghavidel-Parsa, B.; Yazdi, F.; Moghadam, N.K. Personality and Pain Intensity in Rheumatoid Arthritis Patients: The Mediating Role of Pain Catastrophizing and Cognitive Emotion Regulation Strategies. Pers. Individ. Differ. 2022, 186, 111390. [Google Scholar] [CrossRef]
- Ecija, C.; Catala, P.; Lopez-Gomez, I.; Bedmar, D.; Peñacoba, C. What Does the Psychological Flexibility Model Contribute to the Relationship Between Depression and Disability in Chronic Pain? The Role of Cognitive Fusion and Pain Acceptance. Clin. Nurs. Res. 2022, 31, 217–229. [Google Scholar] [CrossRef]
- Stein, A.T.; Medina, J.L.; Rosenfield, D.; Otto, M.W.; Smits, J.A.J. Examining experiential avoidance as a mediator of the relation between anxiety sensitivity and depressive symptoms. Cogn. Behav. Ther. 2020, 49, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, L.; Todd, J.; Scott, A.; Gatzounis, R.; Menzies, R.E.; Meulders, A. Safety behaviours or safety precautions? The role of subtle avoidance in anxiety disorders in the context of chronic physical illness. Clin. Psychol. Rev. 2022, 92, 102126. [Google Scholar] [CrossRef]
- McCluskey, D.L.; Haliwa, I.; Wilson, J.; Keeley, J.W.; Shook, N.J. Experiential avoidance mediates the relation between mindfulness and anxiety. Curr. Psychol. 2022, 41, 3947–3957. [Google Scholar] [CrossRef]
- Ibrahim, M.E.; Weber, K.; Courvoisier, D.S.; Genevay, S. Big five personality traits and disabling chronic low back pain: Association with fear-avoidance, anxious and depressive moods. J. Pain Res. 2020, 13, 745–754. [Google Scholar] [CrossRef]
- Shepherd, L.; Reynolds, D.P.; Turner, A.; O’Boyle, C.P.; Thompson, A.R. The role of psychological flexibility in appearance anxiety in people who have experienced a visible burn injury. Burns 2019, 45, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Landi, G.; Pakenham, K.I.; Crocetti, E.; Tossani, E.; Grandi, S. The trajectories of anxiety and depression during the COVID-19 pandemic and the protective role of psychological flexibility: A four-wave longitudinal study. J. Affect. Disord. 2022, 307, 69–78. [Google Scholar] [CrossRef]
- Dansie, E.J.; Turk, D.C. Assessment of patients with chronic pain. Br. J. Anaesth. 2013, 111, 19–25. [Google Scholar] [CrossRef]
- Krueger, R.F.; Hobbs, K.A. An overview of the DSM-5 alternative model of personality disorders. Psychopathology 2020, 53, 126–132. [Google Scholar] [CrossRef]
- McCracken, L.M. Personalized pain management: Is it time for process-based therapy for particular people with chronic pain? Eur. J. Pain 2023, 27, 1044–1055. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Hofmann, S.G.; Ciarrochi, J. A process-based approach to psychological diagnosis and treatment: The conceptual and treatment utility of an extended evolutionary meta model. Clin. Psychol. Rev. 2020, 82, 101908. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G. Psychotherapeutic Interventions and Processes. Cogn. Behav. Pract. 2022, 29, 581–584. [Google Scholar] [CrossRef]
- Mauck, M.; Aylward, A.; Barton, C.; Birckhead, B.; Carey, T.; Dalton, D.; Fields, A.; Fritz, J.; Hassett, A.; Hoffmeyer, A.; et al. Evidence-based interventions to treat chronic low back pain: Treatment selection for a personalized medicine approach. Pain Rep. 2022, 7, e1019. [Google Scholar] [CrossRef]
- Coto-Lesmes, R.; Fernández-Rodríguez, C.; González-Fernández, S. Acceptance and Commitment Therapy in group format for anxiety and depression. A systematic review. J. Affect. Disord. 2020, 263, 107–120. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Overall (N = 108) | |
|---|---|
| Age | |
| Mean (SD) | 56.7 (11.3) |
| Gender (N, %) | |
| Female | 83 (76.9%) |
| Male | 25 (23.1%) |
| Marital status | |
| Divorced | 7 (6.5%) |
| Married | 89 (82.4%) |
| Single | 4 (3.7%) |
| Widowed | 8 (7.4%) |
| Education | |
| High school | 40 (37.0%) |
| Higher education | 32 (29.6%) |
| Middle school | 36 (33.3%) |
| Occupational status | |
| Employed | 47 (43.5%) |
| Retired | 50 (46.3%) |
| Unemployed | 11 (10.2%) |
| Diagnosis | |
| Chronic post-surgical pain | 4 (3.7%) |
| Coxarthrosis | 3 (2.8%) |
| Gonarthrosis | 4 (3.7%) |
| Osteoarthritis | 30 (27.8%) |
| Other arthritis types | 4 (3.7%) |
| Rheumatoid arthritis | 24 (22.2%) |
| Rheumatoid polyarthritis | 10 (9.3%) |
| Spondylosis | 29 (26.9%) |
| Variable | M | SD | Sk | Ku | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 47.55 | 11.11 | −0.33 | 0.08 | |||||||||
| 51.66 | 11.35 | 0.22 | −0.42 | 0.45 ** | ||||||||
| 47.34 | 9.36 | −0.36 | 0.44 | 0.23 * | 0.13 | |||||||
| 49.36 | 10.23 | 0.23 | 0.50 | −0.02 | −0.16 | −0.18 | ||||||
| 47.22 | 8.45 | 0.20 | −0.43 | 0.09 | 0.23 * | −0.14 | 0.35 ** | |||||
| 2.91 | 1.31 | 0.72 | 0.18 | −0.32 ** | −0.38 ** | −0.03 | −0.21 * | −0.46 ** | ||||
| 5.70 | 3.05 | −0.23 | −0.98 | −0.20 * | −0.33 ** | −0.15 | −0.12 | −0.15 | 0.39 ** | |||
| 5.93 | 2.94 | −0.23 | −1.05 | −0.22 * | −0.32 ** | −0.12 | −0.09 | −0.05 | 0.35 ** | 0.79 ** | ||
| 4.12 | 3.15 | 0.54 | −0.98 | −0.30 ** | −0.39 ** | −0.10 | −0.03 | −0.17 | 0.55 ** | 0.59 ** | 0.60 ** | |
| 3.81 | 3.11 | 0.69 | −0.75 | −0.32 ** | −0.42 ** | −0.11 | −0.07 | −0.22 * | 0.53 ** | 0.67 ** | 0.68 ** | 0.66 ** |
| Criteria | Predictor | B | SE | t | p | [95% CI] | F(df) | radj2 | |
|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||
| Psychological Flexibility | Intercept | 7.93 | 1.14 | 6.96 | <0.001 | 5.67 | 10.19 | 8.36 (7, 100) p < 0.001 | 0.32 |
| O | −0.02 | 0.01 | −1.70 | 0.09 | −0.04 | 0.00 | |||
| E | −0.03 | 0.01 | −2.38 | 0.02 | −0.05 | 0.00 | |||
| C | 0.00 | 0.01 | −0.24 | 0.81 | −0.03 | 0.02 | |||
| A | −0.02 | 0.01 | −1.80 | 0.07 | −0.04 | 0.00 | |||
| S | −0.05 | 0.01 | −3.27 | 0.001 | −0.08 | −0.02 | |||
| Age | −0.52 | 0.27 | −1.96 | 0.053 | −1.05 | 0.01 | |||
| Gender | 0.01 | 0.01 | 1.38 | 0.17 | −0.01 | 0.03 | |||
| Pain | Intercept | 12.30 | 2.93 | 4.21 | <0.001 | 6.50 | 18.11 | 4.47 (7, 100) p < 0.001 | 0.19 |
| O | 0.00 | 0.03 | 0.02 | 0.98 | −0.06 | 0.06 | |||
| E | −0.09 | 0.03 | −3.04 | 0.003 | −0.14 | −0.03 | |||
| C | −0.04 | 0.03 | −1.29 | 0.20 | −0.10 | 0.02 | |||
| A | −0.07 | 0.03 | −2.36 | 0.02 | −0.13 | −0.01 | |||
| S | 0.02 | 0.04 | 0.44 | 0.66 | −0.06 | 0.09 | |||
| Age | 0.05 | 0.02 | 2.03 | 0.045 | 0.00 | 0.10 | |||
| Sex | −1.79 | 0.68 | −2.61 | 0.01 | −3.15 | −0.43 | |||
| Fatigue | Intercept | 9.87 | 2.83 | 3.49 | <0.001 | 4.26 | 15.48 | 4.39 (7, 100) p < 0.001 | 0.18 |
| O | −0.01 | 0.03 | −0.42 | 0.68 | −0.07 | 0.04 | |||
| E | −0.08 | 0.03 | −2.98 | 0.003 | −0.14 | −0.03 | |||
| C | −0.02 | 0.03 | −0.65 | 0.52 | −0.08 | 0.04 | |||
| A | −0.07 | 0.03 | −2.36 | 0.02 | −0.12 | −0.01 | |||
| S | 0.06 | 0.04 | 1.60 | 0.11 | −0.01 | 0.13 | |||
| Age | 0.05 | 0.02 | 2.12 | 0.04 | 0.00 | 0.10 | |||
| Gender | −1.97 | 0.66 | −2.98 | 0.003 | −3.29 | −0.66 | |||
| Anxiety | Intercept | 11.41 | 3.06 | 3.73 | <0.001 | 5.34 | 17.47 | 3.99 (7, 100) p < 0.001 | 0.16 |
| O | −0.03 | 0.03 | −1.18 | 0.24 | −0.09 | 0.02 | |||
| E | −0.09 | 0.03 | −3.00 | 0.003 | −0.15 | −0.03 | |||
| C | −0.01 | 0.03 | −0.28 | 0.78 | −0.07 | 0.05 | |||
| A | −0.03 | 0.03 | −1.00 | 0.32 | −0.09 | 0.03 | |||
| S | 0.00 | 0.04 | −0.11 | 0.92 | −0.08 | 0.07 | |||
| Age | 0.03 | 0.03 | 1.00 | 0.32 | −0.03 | 0.08 | |||
| Gender | −1.32 | 0.72 | −1.85 | 0.07 | −2.74 | 0.10 | |||
| Depression | Intercept | 11.23 | 2.81 | 3.99 | <0.001 | 5.65 | 16.80 | 6.87 (7, 100) p < 0.001 | 0.28 |
| O | −0.03 | 0.03 | −1.17 | 0.25 | −0.09 | 0.02 | |||
| E | −0.09 | 0.03 | −3.43 | <0.001 | −0.15 | −0.04 | |||
| C | −0.01 | 0.03 | −0.38 | 0.70 | −0.07 | 0.05 | |||
| A | −0.05 | 0.03 | −1.61 | 0.11 | −0.10 | 0.01 | |||
| S | −0.01 | 0.04 | −0.22 | 0.83 | −0.08 | 0.06 | |||
| Age | 0.05 | 0.02 | 1.97 | 0.051 | 0.00 | 0.09 | |||
| Gender | −2.21 | 0.66 | −3.36 | 0.001 | −3.51 | −0.90 | |||
| Criteria | Predictor | B | SE | Z | p | [95% CI] | F(df) | radj2 | |
|---|---|---|---|---|---|---|---|---|---|
| LL | UL | ||||||||
| AAQ | O | −0.02 | 0.01 | −1.77 | 0.08 | −0.04 | 0.002 | 8.36 (7, 100) p < 0.001 | 0.33 |
| E | −0.03 | 0.01 | −2.47 | 0.01 | −0.05 | −0.01 | |||
| C | 0.00 | 0.01 | −0.25 | 0.81 | −0.03 | 0.02 | |||
| A | −0.02 | 0.01 | −1.87 | 0.06 | −0.04 | 0.001 | |||
| S | −0.05 | 0.01 | −3.40 | <0.001 | −0.07 | −0.02 | |||
| Age | 0.01 | 0.01 | 1.43 | 0.15 | −0.01 | 0.03 | |||
| Sex | −0.52 | 0.26 | −2.03 | 0.04 | −1.02 | −0.02 | |||
| Pain | AAQ | 0.57 | 0.24 | 2.36 | 0.02 | 0.10 | 1.04 | 4.72 (8, 99) p < 0.001 | 0.22 |
| O | 0.01 | 0.03 | 0.42 | 0.68 | −0.04 | 0.06 | |||
| E | −0.07 | 0.03 | −2.61 | 0.01 | −0.13 | −0.02 | |||
| C | −0.04 | 0.03 | −1.32 | 0.19 | −0.09 | 0.02 | |||
| A | −0.06 | 0.03 | −2.05 | 0.04 | −0.11 | −0.003 | |||
| S | 0.04 | 0.04 | 1.18 | 0.24 | −0.03 | 0.12 | |||
| Age | 0.04 | 0.02 | 1.82 | 0.07 | −0.003 | 0.09 | |||
| Sex | −1.49 | 0.66 | −2.28 | 0.02 | −2.77 | −0.21 | |||
| Fatigue | AAQ | 0.55 | 0.23 | 2.35 | 0.02 | 0.09 | 1.00 | 4.63 (8, 99) p < 0.001 | 0.21 |
| O | 0.00 | 0.03 | −0.05 | 0.96 | −0.05 | 0.05 | |||
| E | −0.07 | 0.03 | −2.54 | 0.01 | −0.12 | −0.02 | |||
| C | −0.02 | 0.03 | −0.63 | 0.53 | −0.07 | 0.04 | |||
| A | −0.06 | 0.03 | −2.06 | 0.04 | −0.11 | 0.00 | |||
| S | 0.08 | 0.04 | 2.35 | 0.02 | 0.01 | 0.15 | |||
| Age | 0.04 | 0.02 | 1.92 | 0.06 | 0.00 | 0.09 | |||
| Sex | −1.69 | 0.63 | −2.67 | 0.01 | −2.93 | −0.45 | |||
| Anxiety | AAQ | 1.17 | 0.23 | 5.05 | <0.001 | 0.72 | 1.63 | 7.20 (8, 99) p < 0.001 | 0.32 |
| O | −0.01 | 0.03 | −0.50 | 0.62 | −0.06 | 0.04 | |||
| E | −0.06 | 0.03 | −2.21 | 0.03 | −0.11 | −0.01 | |||
| C | −0.01 | 0.03 | −0.21 | 0.84 | −0.06 | 0.05 | |||
| A | −0.01 | 0.03 | −0.24 | 0.81 | −0.06 | 0.05 | |||
| S | 0.05 | 0.04 | 1.45 | 0.15 | −0.02 | 0.12 | |||
| Age | 0.01 | 0.02 | 0.45 | 0.65 | −0.03 | 0.05 | |||
| Sex | −0.71 | 0.63 | −1.12 | 0.26 | −1.95 | 0.53 | |||
| Depression | AAQ | 0.87 | 0.22 | 3.93 | <0.001 | 0.44 | 1.31 | 8.56 (8, 99) p < 0.001 | 0.36 |
| O | −0.02 | 0.03 | −0.62 | 0.54 | −0.06 | 0.03 | |||
| E | −0.07 | 0.03 | −2.80 | 0.01 | −0.12 | −0.02 | |||
| C | −0.01 | 0.03 | −0.33 | 0.74 | −0.06 | 0.04 | |||
| A | −0.03 | 0.03 | −1.06 | 0.29 | −0.08 | 0.02 | |||
| S | 0.03 | 0.03 | 0.99 | 0.32 | −0.03 | 0.10 | |||
| Age | 0.04 | 0.02 | 1.63 | 0.10 | −0.01 | 0.08 | |||
| Sex | −1.75 | 0.60 | −2.91 | <0.001 | −2.94 | −0.57 | |||
| Path | B | SE | z | p | 95% CI | ||
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| Pain r2 = 0.28 Δr2 = 0.06 | O → AAQ → Pain | −0.01 | −0.01 | 0.01 | 0.49 | 0.01 | −0.70 |
| E → AAQ → Pain | −0.01 | −0.02 | 0.01 | 0.48 | 0.01 | −0.72 | |
| C → AAQ → Pain | −0.01 | −0.01 | 0.01 | 0.73 | 0.01 | −0.35 | |
| A → AAQ → Pain | −0.01 | −0.01 | 0.01 | 0.50 | 0.01 | −0.67 | |
| S → AAQ → Pain | −0.01 | −0.04 | 0.02 | 0.46 | 0.01 | - 0.73 | |
| Total indirect | −0.13 | −0.22 | −0.04 | 0.01 | 0.05 | −2.70 | |
| Total direct | −0.08 | −0.21 | 0.06 | 0.26 | 0.07 | −1.13 | |
| Total effect | −0.20 | −0.31 | −0.10 | <0.001 | 0.05 | −3.83 | |
| Fatigue r2 = 0.27 Δr2 = 0.06 | O → AAQ → Fatigue | −0.01 | −0.02 | 0.01 | 0.20 | 0.01 | −1.30 |
| E → AAQ → Fatigue | −0.01 | −0.03 | 0.01 | 0.15 | 0.01 | −1.43 | |
| C → AAQ → Fatigue | −0.01 | −0.01 | 0.01 | 0.70 | 0.01 | −0.38 | |
| A → AAQ → Fatigue | −0.01 | −0.02 | 0.01 | 0.25 | 0.01 | −1.16 | |
| S → AAQ → Fatigue | −0.02 | −0.05 | 0.01 | 0.11 | 0.01 | −1.59 | |
| Total indirect | −0.11 | −0.20 | −0.02 | 0.02 | 0.05 | −2.39 | |
| Total direct | −0.04 | −0.17 | 0.01 | 0.53 | 0.07 | −0.63 | |
| Total effect | −0.15 | −0.25 | −0.05 | 0.003 | 0.05 | −2.93 | |
| Anxiety r2 = 0.37 Δr2 = 0.05 | O → AAQ → Anxiety | −0.02 | −0.04 | 0.01 | 0.08 | 0.01 | −1.76 |
| E → AAQ → Anxiety | −0.03 | −0.05 | −0.01 | 0.03 | 0.01 | −2.14 | |
| C → AAQ → Anxiety | −0.01 | −0.03 | 0.02 | 0.70 | 0.01 | −0.39 | |
| A → AAQ → Anxiety | −0.02 | −0.04 | 0.01 | 0.15 | 0.01 | −1.45 | |
| S → AAQ → Anxiety | −0.05 | −0.08 | −0.02 | 0.005 | 0.03 | −2.83 | |
| Total indirect | −0.18 | −0.27 | −0.08 | <0.001 | 0.05 | −3.70 | |
| Total direct | −0.01 | −0.14 | 0.11 | 0.83 | 0.06 | −0.24 | |
| Total effect | −0.19 | −0.29 | −0.09 | <0.001 | 0.05 | −3.58 | |
| Depression r2 = 0.41 Δr2 = 0.13 | O → AAQ → Depression | −0.01 | −0.02 | 0.01 | 0.16 | 0.01 | −1.41 |
| E → AAQ → Depression | −0.01 | −0.03 | 0.01 | 0.11 | 0.01 | −1.60 | |
| C → AAQ → Depression | −0.01 | −0.01 | 0.01 | 0.70 | 0.01 | −0.38 | |
| A → AAQ → Depression | −0.01 | −0.02 | 0.01 | 0.22 | 0.01 | −1.24 | |
| S → AAQ → Depression | −0.03 | −0.05 | 0.01 | 0.07 | 0.01 | −1.82 | |
| Total indirect | −0.17 | −0.26 | −0.08 | <0.001 | 0.05 | −3.72 | |
| Total direct | −0.06 | −0.18 | 0.07 | 0.38 | 0.06 | −0.88 | |
| Total effect | −0.22 | −0.32 | −0.13 | <0.001 | 0.05 | −4.42 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cojocaru, C.-M.; Popa, C.O.; Schenk, A.; Marian, Ș.; Marchean, H.; Suciu, B.A.; Szasz, S.; Popoviciu, H.; Mureșan, S. Personality and Pain Outcomes in Rheumatic Disease: The Mediating Role of Psychological Flexibility. Healthcare 2024, 12, 1087. https://doi.org/10.3390/healthcare12111087
Cojocaru C-M, Popa CO, Schenk A, Marian Ș, Marchean H, Suciu BA, Szasz S, Popoviciu H, Mureșan S. Personality and Pain Outcomes in Rheumatic Disease: The Mediating Role of Psychological Flexibility. Healthcare. 2024; 12(11):1087. https://doi.org/10.3390/healthcare12111087
Chicago/Turabian StyleCojocaru, Cristiana-Manuela, Cosmin Octavian Popa, Alina Schenk, Ștefan Marian, Horia Marchean, Bogdan Andrei Suciu, Simona Szasz, Horațiu Popoviciu, and Simona Mureșan. 2024. "Personality and Pain Outcomes in Rheumatic Disease: The Mediating Role of Psychological Flexibility" Healthcare 12, no. 11: 1087. https://doi.org/10.3390/healthcare12111087
APA StyleCojocaru, C.-M., Popa, C. O., Schenk, A., Marian, Ș., Marchean, H., Suciu, B. A., Szasz, S., Popoviciu, H., & Mureșan, S. (2024). Personality and Pain Outcomes in Rheumatic Disease: The Mediating Role of Psychological Flexibility. Healthcare, 12(11), 1087. https://doi.org/10.3390/healthcare12111087