_MD__MPH_PhD.png)
Exploring the Health-Related Quality of Life and the Lived Experience of Adolescents Following Invasive Meningococcal Disease

 , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment
2.3. Data Collection
2.4. Analysis
2.5. Role of the Funding Source
3. Results
- A.
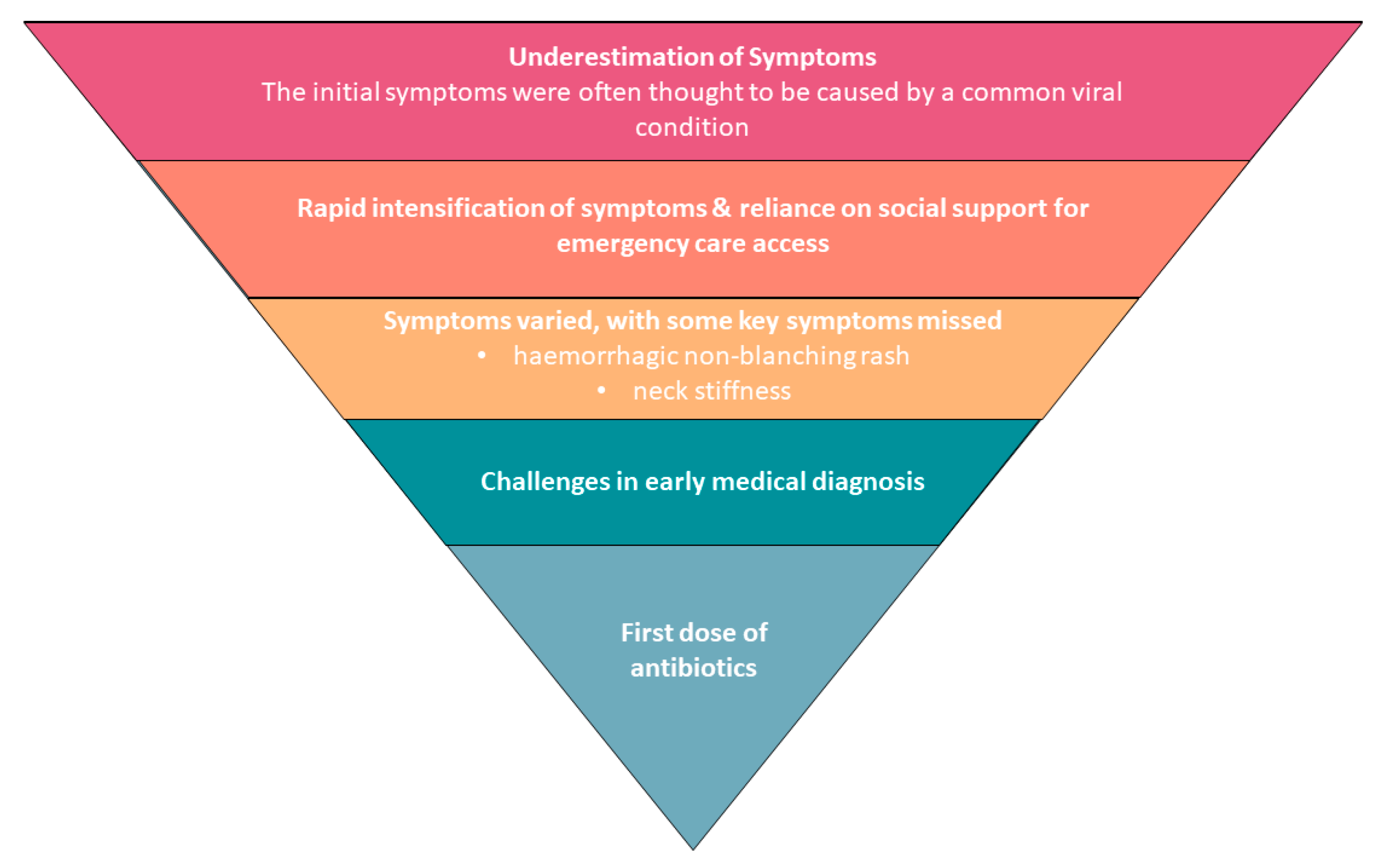
- Potential barriers to timely first dose of antibiotics
- (1)
- Underestimation of initial symptoms and then rapid progression of symptoms
- (2)
- Reliance on social support for emergency care access
- (3)
- Symptoms prompting seeking medical care varied, with some key symptoms missed
- (4)
- Challenges in early medical diagnosis
- B.
- The life-changing impact of meningococcal disease
- (5)
- Traumatic and life-changing experiences of IMD
- C.
- Ongoing HRQoL issues and impacts of IMD
- (6)
- IMD’s lingering impact on health-related quality of life
- (7)
- Gaps in the continuity of care post-discharge for patients and carers
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hart, C.A.; Thomson, A.P. Meningococcal disease and its management in children. BMJ (Clin. Res. Ed.) 2006, 333, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.J. Prevention of Meningococcal Infection in the United States: Current Recommendations and Future Considerations. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2016, 59, S29–S37. [Google Scholar] [CrossRef] [PubMed]
- Edmond, K.; Clark, A.; Korczak, V.S.; Sanderson, C.; Griffiths, U.K.; Rudan, I. Global and regional risk of disabling sequelae from bacterial meningitis: A systematic review and meta-analysis. Lancet Infect. Dis. 2010, 10, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Voss, S.S.; Nielsen, J.; Valentiner-Branth, P. Risk of sequelae after invasive meningococcal disease. BMC Infect. Dis. 2022, 22, 148. [Google Scholar] [CrossRef] [PubMed]
- Borg, J.; Christie, D.; Coen, P.G.; Booy, R.; Viner, R.M. Outcomes of meningococcal disease in adolescence: Prospective, matched-cohort study. Pediatrics 2009, 123, e502–e509. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Booy, R.; Johnson, H.; Edmunds, W.J.; Hudson, L.; Bedford, H.; Kaczmarski, E.; Rajput, K.; Ramsay, M.; Christie, D. Outcomes of invasive meningococcal serogroup B disease in children and adolescents (MOSAIC): A case-control study. Lancet Neurol. 2012, 11, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.L.; Bell, T.J.; Miller, J.M.; Misurski, D.A.; Bapat, B. Hospital costs, length of stay and mortality associated with childhood, adolescent and young adult meningococcal disease in the US. Appl. Health Econ. Health Policy 2011, 9, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Lahra, M.M.; Enriquez, R.P. Australian Meningococcal Surveillance Programme annual report, 2014. Commun. Dis. Intell. Q. Rep. 2016, 40, E221–E228. [Google Scholar] [PubMed]
- Pelton, S.I. The Global Evolution of Meningococcal Epidemiology Following the Introduction of Meningococcal Vaccines. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2016, 59, S3–S11. [Google Scholar] [CrossRef]
- Keshavan, M.S.; Giedd, J.; Lau, J.Y.; Lewis, D.A.; Paus, T. Changes in the adolescent brain and the pathophysiology of psychotic disorders. Lancet Psychiatry 2014, 1, 549–558. [Google Scholar] [CrossRef]
- Sander, J.; Bay, D.; Gedde-Dahl, T.W.; Borchgrevink, H.M.; Froholm, L.O.; Oftedal, S.I.; Vandvik, B. Late sequelae after meningococcal disease. A controlled study in young men. NIPH Ann. 1984, 7, 3–11. [Google Scholar] [PubMed]
- Young, N.; Thomas, M. Meningitis in adults: Diagnosis and management. Intern. Med. J. 2018, 48, 1294–1307. [Google Scholar] [CrossRef] [PubMed]
- van de Beek, D.; de Gans, J.; Spanjaard, L.; Weisfelt, M.; Reitsma, J.B.; Vermeulen, M. Clinical features and prognostic factors in adults with bacterial meningitis. N. Engl. J. Med. 2004, 351, 1849–1859. [Google Scholar] [CrossRef] [PubMed]
- Lepur, D.; Barsic, B. Community-acquired bacterial meningitis in adults: Antibiotic timing in disease course and outcome. Infection 2007, 35, 225–231. [Google Scholar] [CrossRef]
- Pelton, S.I. Meningococcal Disease Awareness: Clinical and Epidemiological Factors Affecting Prevention and Management in Adolescents. J. Adolesc. Health 2010, 46, S9–S15. [Google Scholar] [CrossRef]
- Thompson, M.J.; Ninis, N.; Perera, R.; Mayon-White, R.; Phillips, C.; Bailey, L.; Harnden, A.; Mant, D.; Levin, M. Clinical recognition of meningococcal disease in children and adolescents. Lancet 2006, 367, 397–403. [Google Scholar] [CrossRef]
- Wang, B.; Santoreneos, R.; Giles, L.; Haji Ali Afzali, H.; Marshall, H. Case fatality rates of invasive meningococcal disease by serogroup and age: A systematic review and meta-analysis. Vaccine 2019, 37, 2768–2782. [Google Scholar] [CrossRef] [PubMed]
- Eisen, D.P.; Hamilton, E.; Bodilsen, J.; Koster-Rasmussen, R.; Stockdale, A.J.; Miner, J.; Nielsen, H.; Dzupova, O.; Sethi, V.; Copson, R.K.; et al. Longer than 2 hours to antibiotics is associated with doubling of mortality in a multinational community-acquired bacterial meningitis cohort. Sci. Rep. 2022, 12, 672. [Google Scholar] [CrossRef]
- Weinberger, J.; Rhee, C.; Klompas, M. A Critical Analysis of the Literature on Time-to-Antibiotics in Suspected Sepsis. J. Infect. Dis. 2020, 222, S110–S118. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention Control. Expert Opinion on the Introduction of the Meningococcal B (4CMenB) Vaccine in the EU/EEA. Available online: https://www.ecdc.europa.eu/en/publications-data/expert-opinion-introduction-meningococcal-b-4cmenb-vaccine-eueea (accessed on 9 April 2024).
- Wallace, M.; Harcourt, D.; Rumsey, N. Adjustment to appearance changes resulting from meningococcal septicaemia during adolescence: A qualitative study. Dev. Neurorehabilit. 2007, 10, 125–132. [Google Scholar] [CrossRef]
- Orbell, S.; Schneider, H.; Esbitt, S.; Gonzalez, J.S.; Gonzalez, J.S.; Shreck, E.; Batchelder, A.; Gidron, Y.; Pressman, S.D.; Hooker, E.D.; et al. Health-Related Quality of Life. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 929–931. [Google Scholar]
- Stevens, K.; Palfreyman, S. The use of qualitative methods in developing the descriptive systems of preference-based measures of health-related quality of life for use in economic evaluation. Value Health 2012, 15, 991–998. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.A.; Ware, J.E., Jr.; Lu, J.F.; Sherbourne, C.D. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med. Care 1994, 32, 40–66. [Google Scholar] [CrossRef] [PubMed]
- Marshall, H.; McMillan, M.; Wang, B.; Booy, R.; Afzali, H.; Buttery, J.; Blyth, C.C.; Richmond, P.; Shaw, D.; Gordon, D.; et al. AMEND study protocol: A case-control study to assess the long-term impact of invasive meningococcal disease in Australian adolescents and young adults. BMJ Open 2019, 9, e032583. [Google Scholar] [CrossRef] [PubMed]
- Fusch, P.; Ness, L. Are We There Yet? Data Saturation in Qualitative Research. Qual. Rep. 2015, 20, 1408–1416. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Socioeconomic Indexes for Areas (SEIFA). Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 9 May 2024).
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Sims-Schouten, W.; Riley, S.C.E.; Willig, C. Critical Realism in Discourse Analysis. Theory Psychol. 2016, 17, 101–124. [Google Scholar] [CrossRef]
- Glimåker, M.; Johansson, B.; Grindborg, Ö.; Bottai, M.; Lindquist, L.; Sjölin, J. Adult Bacterial Meningitis: Earlier Treatment and Improved Outcome Following Guideline Revision Promoting Prompt Lumbar Puncture. Clin. Infect. Dis. 2015, 60, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- WHO. Defeating Meningitis by 2030: A Global Road Map; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Bullen, C. Taking public health to the streets: The 1998 Auckland Meningococcal Disease Awareness Program. Health Educ. Behav. 2000, 27, 363–370. [Google Scholar] [CrossRef]
- Guimont, C.; Hullick, C.; Durrheim, D.; Ryan, N.; Ferguson, J.; Massey, P. Invasive meningococcal disease—Improving management through structured review of cases in the Hunter New England area, Australia. J. Public Health 2010, 32, 38–43. [Google Scholar] [CrossRef]
- Meningococcal B Immunisation Program. Available online: https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/conditions/immunisation/immunisation+programs/meningococcal+b+immunisation+program (accessed on 13 December 2023).
- Queensland MenB Vaccination Program. Available online: https://www.health.qld.gov.au/clinical-practice/guidelines-procedures/diseases-infection/immunisation/meningococcal-b (accessed on 5 April 2024).
- Wisemantel, M.; Maple, M.; Massey, P.D.; Osbourn, M.; Kohlhagen, J. Psychosocial Challenges of Invasive Meningococcal Disease for Children and their Families. Aust. Soc. Work. 2018, 71, 478–490. [Google Scholar] [CrossRef]
- Nguyen, H.; Butow, P.; Dhillon, H.; Sundaresan, P. A review of the barriers to using Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs) in routine cancer care. J. Med. Radiat. Sci. 2021, 68, 186–195. [Google Scholar] [CrossRef]
- Olbrich, K.J.; Muller, D.; Schumacher, S.; Beck, E.; Meszaros, K.; Koerber, F. Systematic Review of Invasive Meningococcal Disease: Sequelae and Quality of Life Impact on Patients and Their Caregivers. Infect. Dis. Ther. 2018, 7, 421–438. [Google Scholar] [CrossRef] [PubMed]
- Marten, O.; Koerber, F.; Bloom, D.; Bullinger, M.; Buysse, C.; Christensen, H.; De Wals, P.; Dohna-Schwake, C.; Henneke, P.; Kirchner, M.; et al. A DELPHI study on aspects of study design to overcome knowledge gaps on the burden of disease caused by serogroup B invasive meningococcal disease. Health Qual. Life Outcomes 2019, 17, 87. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.; Muscara, F.; Anderson, V.A.; McCarthy, M.C. Early Traumatic Stress Responses in Parents Following a Serious Illness in Their Child: A Systematic Review. J. Clin. Psychol. Med. Settings 2016, 23, 53–66. [Google Scholar] [CrossRef] [PubMed]
- Yi-Frazier, J.P.; Fladeboe, K.; Klein, V.; Eaton, L.; Wharton, C.; McCauley, E.; Rosenberg, A.R. Promoting Resilience in Stress Management for Parents (PRISM-P): An intervention for caregivers of youth with serious illness. Fam. Syst. Health J. Collab. Fam. Healthc. 2017, 35, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Shewbridge, A.; Harris, J.; Green, J.S. Benefits of multidisciplinary teamwork in the management of breast cancer. Breast Cancer (Dove Med. Press) 2013, 5, 79–85. [Google Scholar] [CrossRef]
- Bonevski, B.; Randell, M.; Paul, C.; Chapman, K.; Twyman, L.; Bryant, J.; Brozek, I.; Hughes, C. Reaching the hard-to-reach: A systematic review of strategies for improving health and medical research with socially disadvantaged groups. BMC Med. Res. Methodol. 2014, 14, 42. [Google Scholar] [CrossRef]

{kind=link}
| Participant Characteristics | N (%) | |
|---|---|---|
| Sex | ||
| Female | 21 (70%) | |
| Male | 9 (30%) | |
| Location | ||
| South Australia | 21 (70%) | |
| Victoria | 9 (30%) | |
| Age at admission | ||
| 15–19 | 16 (53%) | |
| 20–24 | 14 (47%) | |
| IRSD (deciles) * | ||
| 1–2 (most disadvantaged) | 2 (7%) | |
| 3–4 | 6 (20%) | |
| 5–6 | 1 (3%) | |
| 7–8 | 4 (13%) | |
| 9–10 (least disadvantaged) | 17 (57%) | |
| Charlson Comorbidity Index score | ||
| 0 (No pre-existing comorbidity) | 28 (93%) | |
| 1 | 2 (7%) | |
| >2 | 0 (0%) | |
| Disease type | ||
| Septicemia | 12 (40%) | |
| Meningitis | 2 (7%) | |
| Mixed meningitis and septicemia | 16 (53%) | |
| Meningococci serogroup | ||
| B | 30 (100%) | |
| Theme | Description | Responses |
|---|---|---|
| 1. Underestimation of initial symptoms and then rapid progression of symptoms | The initial symptoms were often thought to be caused by a common viral condition. |
|
| Many participants described a rapid intensification of their symptoms, indicating to them, or others, that their condition was more serious than initially thought. |
| |
| 2. Reliance on social support for emergency care access | Many participants described receiving assistance from family or friends to access medical care. This help was often required due to their rapid deterioration, which rendered them unable to help themselves. The participants highlighted their family, friends, and caregivers’ vital roles in identifying their condition’s seriousness and initiating and facilitating access to emergency medical services. |
|
| 3. Symptoms prompting seeking medical care varied, with some key symptoms missed | The symptoms prompting seeking medical care varied and ranged from confusion or loss of consciousness to severe gastrointestinal symptoms, rash, headaches, neck stiffness, seizures, and joint pain, many in combination with each other. In some instances, a hemorrhagic non-blanching rash, a distinct symptom associated with meningococcal disease, or neck stiffness, a key sign of meningitis, did not prompt individuals to seek urgent medical assistance. |
|
| 4. Challenges in early medical diagnosis | Some participants had delays in treatment despite presenting to a healthcare provider. Ten participants reported having more than one presentation to a healthcare setting before they received an accurate diagnosis and appropriate treatment. These were primarily presentations to a general practitioner, and to a lesser extent, in acute care settings. |
|
| Theme | Subthemes | Description | Responses |
|---|---|---|---|
| 5. Traumatic and life-changing experience of IMD | Difficulty coming to terms with their experience | Due to the severity of their condition and treatment, many participants had a scant recollection of their intensive care admission when they were critically unwell. However, they were often confronted at a later stage with how close they came to death. Some are still struggling to come to terms with their experience. |
|
| Adverse impact on caregivers | As well as being traumatic for the participants, having a child experience IMD had traumatic effects on the caregivers as well. The participants described the ongoing issues their parents experienced as they recovered from their infection. |
|
| Theme | Subthemes | Description | Responses |
|---|---|---|---|
| 6. IMD’s lingering impact on health-related quality of life | Lingering psychological impacts | Beyond the impacts of the initial hospitalization for IMD, the participants described the ongoing HRQoL challenges they had or were continuing to experience. Many survivors reported psychological impacts such as depression and anxiety that persisted up to and beyond one year post-hospitalization. |
|
| Lingering effects on memory and concentration | Survivors also reported cognitive challenges, including issues with memory loss and concentration difficulties. |
| |
| Lingering physical effects | Chronic headaches, pain, and fatigue were the next most commonly reported sequelae by the survivors. Other reported sequelae included weakened immune systems, tinnitus, lower fitness levels, poor sleep, skin rashes, photosensitivity, weight loss, and altered temperature regulation. |
| |
| Impact on education and employment | Lingering psychological, cognitive, and physical impacts disrupted the education and professional lives of many of the survivors. These impacts range from minor disruptions to significant hardship in returning to full-time work or study. |
| |
| 7. Gaps in the continuity of care post-discharge for patients and carers | Participants described the time after being discharged from the hospital as a time of unmet health needs. Most of the participants reported high-quality care whilst in hospital despite the effects of IMD. However, some felt that the level of care and follow-up they received after being discharged was not proportionate to the severity of the effects of IMD and the ongoing issues the participants experienced. |
| |
| As well as experiencing ongoing adverse effects from IMD, the participants cited the lack of follow-up as compounding their distress due to fear of the unknown. With limited follow-up and resources, some participants were unable to reconcile their experiences, as they had no frame of reference for what was expected and whether they would fully recover. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McMillan, M.; McDonough, J.; Angliss, M.; Buttery, J.; Saunders, L.; Mathew, S.M.; Shaw, D.; Gordon, D.; Warner, M.S.; Nelson, R.; et al. Exploring the Health-Related Quality of Life and the Lived Experience of Adolescents Following Invasive Meningococcal Disease. Healthcare 2024, 12, 1075. https://doi.org/10.3390/healthcare12111075
McMillan M, McDonough J, Angliss M, Buttery J, Saunders L, Mathew SM, Shaw D, Gordon D, Warner MS, Nelson R, et al. Exploring the Health-Related Quality of Life and the Lived Experience of Adolescents Following Invasive Meningococcal Disease. Healthcare. 2024; 12(11):1075. https://doi.org/10.3390/healthcare12111075
Chicago/Turabian StyleMcMillan, Mark, Joshua McDonough, Margaret Angliss, Jim Buttery, Lynda Saunders, Suja M. Mathew, David Shaw, David Gordon, Morgyn S. Warner, Renjy Nelson, and et al. 2024. "Exploring the Health-Related Quality of Life and the Lived Experience of Adolescents Following Invasive Meningococcal Disease" Healthcare 12, no. 11: 1075. https://doi.org/10.3390/healthcare12111075
APA StyleMcMillan, M., McDonough, J., Angliss, M., Buttery, J., Saunders, L., Mathew, S. M., Shaw, D., Gordon, D., Warner, M. S., Nelson, R., Hannah, R., & Marshall, H. S. (2024). Exploring the Health-Related Quality of Life and the Lived Experience of Adolescents Following Invasive Meningococcal Disease. Healthcare, 12(11), 1075. https://doi.org/10.3390/healthcare12111075