
Nurses Response to the Physical and Psycho-Social Care Needs of Patients with COVID-19: A Mixed-Methods Study
 , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
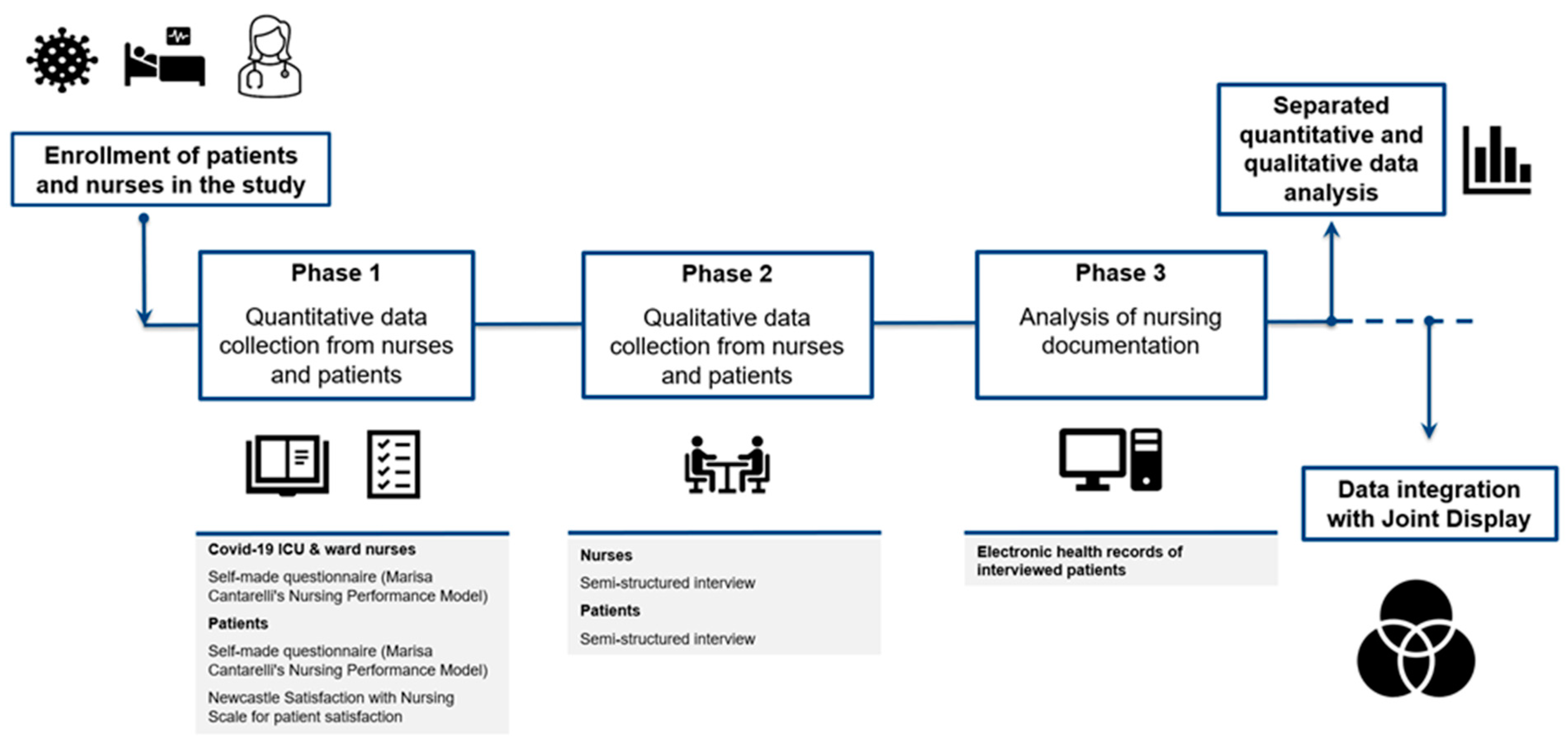
2.1. Study Design
Context
2.2. The Quantitative Study Phase
2.2.1. Participants
Nurses
Patients
2.2.2. Data Collection
The Nurse Questionnaire
The Patient Questionnaire
2.2.3. Data Analysis
2.3. Qualitative Study Phase
2.3.1. Qualitative Approach
2.3.2. Characteristics of the Investigators and Reflexivity
2.3.3. Participant Recruitment and Sampling
2.3.4. Nurse Interview Recruitment
2.3.5. Patient Interview Recruitment
2.3.6. Data Analysis
2.3.7. Rigor Qualitative Phase
2.4. Analysis of the Nursing Documentation
2.5. Quantitative and Qualitative Data Integration and Rigor in Relational to Mixed Methods Research
3. Results
3.1. Quantitative Phase—Nurses and Patients Surveys
3.2. Qualitative Phase
3.2.1. Nurse Interviews
3.2.2. Macro-Theme: “The Context”
3.2.3. The Clinical/Professional Context
“…they were fine until that moment, so they even talked to you, but maybe after only half an hour they were dead. So, also this unpredictability, this way of dying was so rapid, that you didn’t have time to realize it…”(Nurse 6)
“…giving each other a hug, which in theory okay you couldn’t, but there many times someone did it anyway and I was never able to say no, because in any case you see a mother, 90 or 80 years old, with her daughter, they haven’t seen each other, she’s sick, a hug, they’re wearing a mask, so hug each other, her overcoat is lifted up, it’s okay, hug her, if she’s already in there, for me there’s no problem.”(Nurse 1)
3.2.4. The Organizational Context
“…the collaboration between the various services […] with palliative care, even the relationships with the doctors were different, the doctors were from outside the hospital, so they had other ideas, other ways of helping each other, and then the support between us was fundamental.”(Nurse 5)
3.3. Macro-Theme: “Nurses’ Experiences and Emotions”
3.3.1. You Won’t Believe It until You See It
“What I remember most, it’s bad to say but those faces deformed by pronation, prolonged pronation and then damaged faces, swollen faces, that left a bit of an impression on me.”(Nurse 15)
3.3.2. It Was a Nice Experience
“I think I’ve grown up a bit, I can talk for forty minutes without crying; I’ve grown a little, maybe I’ve learned how to better process the most critical situations and challenge myself more, and to start again as if I didn’t know anything.”(Nurse 9)
“if we managed to do what we did during the first wave, it was also because we felt the support of the people who were outside, and I believe that this tiredness we have now is also because you feel that there isn’t any more support.”(Nurse 7)
3.3.3. Your Own Emotions
“(…) I was afraid of infecting my family; in fact, I didn’t see my parents and my in-laws, who are old, in their eighties, for four months.”(Nurse 11)
“Not thinking what’s outside. Once the doors are closed, I completely disconnect, in fact I still can’t talk about it very easily today, a bit of that experience remains; I try to keep it in a corner.”(Nurse 10)
3.3.4. Confrontation with Death
“… She died in the afternoon, I was looking after her that morning; it was nice anyway, she didn’t suffer and so this is what counts most for me…”(Nurse 1)
“Instead of crying, this made me feel angry, and with some feelings of rebellion, I said: “I’ll resuscitate her anyway, if it’s a colleague who has a heart failure, if it’s you I’ll resuscitate her anyway.”(Nurse 11)
3.3.5. You Own Resources
“the fear was there, but the urge and the willingness to go and take part in this experience, and lend a hand was even stronger (…)”(Nurse 1)
“Experience certainly helps, it has helped and continues to help a lot.”(Nurse 8)
“….super supportive colleagues, during the night, when one is having a moment of discouragement, there was immediately another one who was ready to listen to and understand the other person’s experiences and feelings.”(Nurse 10)
3.3.6. I No Longer Want to Be a Nurse
“(…) for two weeks I was already on the verge of saying “no, I’ve had enough, I give up, I’m stopping, I don’t want to be a nurse anymore”, but what’s the point of being a nurse in this way?”(Nurse 10)
3.4. Macro Theme: “Facilitators and Barriers to Patient Care
3.4.1. Interprofessional Collaboration
“I found an exceptional team and colleagues, there really was incredible solidarity, a spirit of collaboration, everyone really united for one purpose, which was to face this pandemic.”(Nurse 11)
3.4.2. Support from Superiors
“He was just asking “how are you?” or the department heads, who were also there, three department heads who managed to collaborate together, would arrive and ask “how are you?”(Nurse 7)
3.4.3. Being an Expert
“I believe I have given my small contribution as a person who has worked with critically ill patients for more than twenty years, who however knows how to recognize certain changes, knows how to anticipate, perhaps even situations that may evolve in a negative way.”(Nurse 7)
3.4.4. Lack of Specific Competencies
“people who did not have training supported those who worked directly on the patient or in any case if they did something on the patient they were directly supervised, controlled and evaluated by those who were responsible for the patient.”(Nurse 8)
3.4.5. Standardization of Care
“During the technical phase we are all a bit like robots, so we just go in with it, we know what we have to do and we do it, as I was saying, in a standardized way.”(Nurse 15)
3.5. Macro-Theme: “Nursing Care”
3.5.1. The Nursing Care Approach to COVID-19 Patients
“…I set myself smart goals, I have to achieve them in a certain amount of time in order to have a tangible result.”(Nurse 11)
“In reality our approach is a global approach, in the sense that we were not just focused on one thing, the real problem was breathing, but in reality, there are all the other things that are part of our care.”(Nurse 13)
3.5.2. Assessment of Patients and Their Needs
“a precarious balance … dictated by the fact that this virus was unknown, there were no data, it was not well understood how it behaved and consequently how we should behave.”(Nurse 16)
“…they didn’t always realize that they were struggling, so it wasn’t always a need that they expressed, or they started to express it when it was already a bit late.”(Nurse 9)
“For us it was really important to understand what our patients needed, because it was very important to help them at that moment, in total solitude, in total discomfort, it was a priority to understand what they needed… we just couldn’t understand what the need was; this caused enormous distress for patients and enormous distress for staff.”(Nurse 10)
“It’s not that I just turn the knobs of the ventilator, I turn patients on their hips, I auscultate them to understand if there are any secretions, I understand if inhalations are needed, I understand if some positions help them.”(Nurse 11)
“Generally, we almost never assess respiratory rates, but more or less now this happens in all hospitals, here this was the first sign, the first of all it was the respiratory rate, together the temperature. So, also your way of viewing nursing changes.”(Nurse 3)
3.5.3. Professional Objectives and Priorities
“let’s set ourselves a goal, we have to extubate him within four days, it’s a goal we set ourselves; we then realize that we can’t? Well, okay, let’s talk about it again, but let’s set real, achievable objectives.”(Nurse 10)
“it was a bit as if we were at war, so the important thing was to go straight to the point and making sure that patients got well.”(Nurse 11)
3.5.4. Professional Performance
“…there was someone who was also looking for a presence, simply having someone close by, wanting to talk, keeping you there to talk, or trying to talk, to let you know something, to know something about their family, in my opinion this was what they were looking for mostly.”(Nurse 8)
“Speaking, for example, with a tracheotomized, ventilated patient is, in my opinion, one of the most difficult things, in the sense that the movement of the lips does not always correspond to what someone actually wants to say to you, so […] sometimes it’s frustrating because maybe the patient is telling you something and you make various attempts trying to understand what he’s telling you…”(Nurse 13)
“…this lady in the end had been treated for more than a month and then seeing her again after she recovered, the first contacts with family members, and the video-calls with family members was something that left you speechless.”(Nurse 8)
“maybe they die like this because I’m not capable of… and instead they say to you “look, it’s not your fault, but it’s just the situation that…” so if not in a normal case of accompaniment you maybe have time, maybe you have a way to… you didn’t have it there and you had to quickly understand what to do to not make them suffer.”(Nurse 5)
“Even for the vital signs, taking the respiratory rate is not something we all did every day, so I also had to get back into it again. Okay, I really have to count the breaths, understand… that is, they are also new things that we didn’t do before; the use of the Venturi, that was also new, so even the healthcare assistants didn’t know it, so they turned up the oxygen, but they didn’t know what they were doing, so we also had to supervise a bit.”(Nurse 6)
3.5.5. The Outcomes of Nursing Care
“…a lot of patients thanked you, so that was nice, because they had also understood our level of stress.”(Nurse 1)
3.6. Macro-Theme: “The Professional Role”
3.6.1. A Multifaceted Role
“among our skills which, in my opinion, which is perhaps one of the most important parts, is that of communication, of the relationships… because when a patient is going through weaning and is making it, and therefore the supports offered by machines begin to be a little less important, the difference that emerges a little is the communicational-relational part.”(Nurse 13)
3.6.2. Fundamental Care
“in my opinion we, needed to go back to the origins a bit, in terms of treatment […] it’s not that I’m not for protocols, protocols are fine, I’m for rules, but every now and then we need to go back to the basics a little more.”(Nurse 3)
3.7. Patient Interviews
3.7.1. Macro-Theme: My Needs/Problems
3.7.2. I Had No Information or It Was Incomplete
“even later they told me “he must be intubated”, but I didn’t understand anything, I understood that they had to intubate me, but I… and then I understood that they said “no, but before doing so we have to inform the relatives at home and everything”, I couldn’t see anything, I was practically alive but always with an empty brain, not thinking about anything, and then they intubated me.”(Patient 12)
“that’s what they didn’t explain to me; if they had explained to me as soon as they woke me up and told me “you can’t talk because we intubated you, you can’t walk because you’ve been sedated, tomorrow you will try, you will start walking”, then maybe I would have felt less anxious.”(Patient 15)
3.7.3. Putting Together All the Pieces of the Jigsaw Puzzle
“…because then even when you are back in the ward you start putting together all the pieces of the jigsaw puzzle, you receive all the various news. And again, long sleepless nights, I think that probably started sleeping in the last few days… and then automatically also…, and there all the pieces of the puzzle of everything that happened come together, it was an incredible thing, that is, it seemed as if you were in a film, a very unusual thing.”(Patient 2)
3.7.4. Physical Problems
“The fever. Breathing, I breathed quite well. Afterwards, it was the fever that made you feel tired, the fever.”(Patient 11)
3.7.5. Psychological Problems
“They were long, I didn’t shave for a fortnight, I had little hair, very little, I shaved my hair every week, I look old, aged… I showed them, I showed them the photo because I had myself photographed in the hospital…, and afterwards I said to myself “I’m ugly and old.”(Patient 7)
3.7.6. Communication/Relational Problems
“I was down in intensive care and there was a young lady who said to me “try to say a word”, I couldn’t do it, well, this is what I remember, that I couldn’t speak. And after that she gave me a pen and paper and said “try it”, I couldn’t hold it, I couldn’t hold either the pen or the paper.”(Patient 1)
3.8. Macro-Theme: My Emotions
3.8.1. Worry and Fear
“We could hear everything, and the doctor came many times a day with this gentleman “look, we have to intubate him”, “no no no…”. Then they told him “look, now let’s call his wife, the daughter of this gentleman” and they called them, but before calling them, the doctor came, told him “the last thing I can tell him is if he doesn’t want to be intubated he has three days left to live” and then his wife and daughter arrived and they talked, I don’t know, and they took him away, I don’t know if they intubated him, and after a couple of days like this, I wasn’t aware of anything anymore, I didn’t understand anything anymore, I didn’t react, I didn’t think about anything anymore, my brain was empty..”(Patient 12)
“I didn’t know anymore… and then I thought that with all the movement that was down there, because it seemed as if we were at war, because I saw it, I saw these ambulances, the tents, curtains… it seemed to be a war, because the soldiers took me here in their ambulance, it was the whole environment, I’m saying something really horrible happened here…”(Patient 7)
“No, I don’t want to blame everyone. I was there in a room, I don’t remember if the room number ended with six or two, I don’t know that, there was the possibility to move along the corridor from the door of my room to the window; there was no balcony, there was a balcony window there, which you could open, but it had bars, it looked like a prison.”(Patient 8)
3.8.2. Frustration and Helplessness
“…when you are there in a room, also embarrassed by certain things you have to do, because all of a sudden you are naked in front of a woman, a nurse ok, but you are there naked, in short, and for me it is extremely important to have never felt humiliated…”(Patient 3)
3.8.3. Priorities That Changed
“and then all of a sudden you’re in a situation where everything you thought about in the ambulance no longer has any importance. You are there and all of a sudden… you slip into a condition where all the material things, but unfortunately also affections, are no longer a priority… in that moment you slip, and you no longer think about anything or anyone… and all of a sudden you’re just focused on yourself, but not in a selfish way, it’s just that you can’t do anything about it…”(Patient 3)
3.9. Macro-Theme: “What Helped Me”
3.9.1. Internal Factors
“The first thing is to go back home and see my family. Then I still have several things to do. So, I don’t want to die now, I have various works to put together, in my atelier, there in the garden; I still have various things to do, and I can’t die now…”(Patient 5)
3.9.2. External Factors
“They removed the tube, they put a microphone here, something to be able to make a video call, so that I could talk to my family at home. That was very good for me, I was happy, and that’s what I think helped me react most, the video call I made;”(Patient 5)
3.10. Macro-Theme: “Nursing Care”
3.10.1. Caring Activities
“Always, everything, even when they washed me, when they came to wash me, they explained to me: “here we’ll put this cream because we have another cream for your feet”, this nurse did everything… you can’t be any better than that.”(Patient 12)
3.10.2. Professionalism
“…yes, various times, this humanity was expressed in various way, it was expressed by just being there, by leaning over you, and also perhaps even extremely, on the one hand the virtual caress, but perhaps also just feeling a caress. People, especially older people, I think… have an incredible need to be touched, to have a caress, so if a nurse does that to you at a certain moment it’s like a positive electric shock, it’s joy; …”(Patient 3)
3.10.3. How Nurses Are Perceived
“Well, then after a while I didn’t see her anymore because she was moved to another ward… This happened all the time: you establish a certain relationship with this nurse, but then I didn’t see her anymore, and that… that was a bit of a shame.”(Patient 2)
3.11. Results from the Clinical Patient Records
3.12. Integration of the Qualitative and Quantitative Findings
4. Discussion
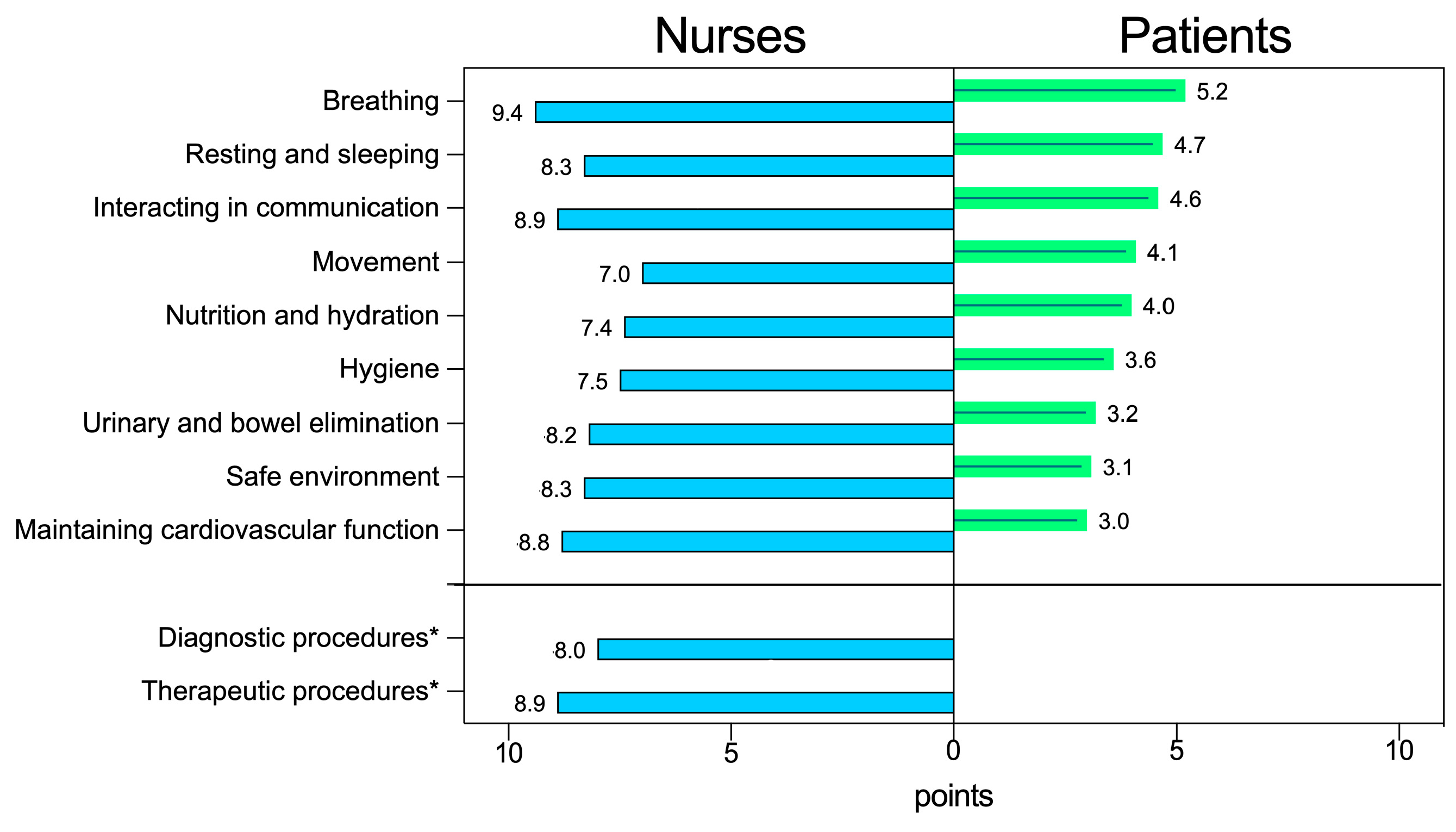
4.1. Nursing Care Needs (NCNs): Survey with Patients and Nurses
4.2. Healthcare Interventions: Survey with Patients and Nurses
4.3. The Nurses’ Experiences of the Situation: Data from Nurse Interviews
4.4. The Professional Role: (Data from Nurse Interviews)
4.5. Facilitators and Barriers: Data from Nurse Interviews
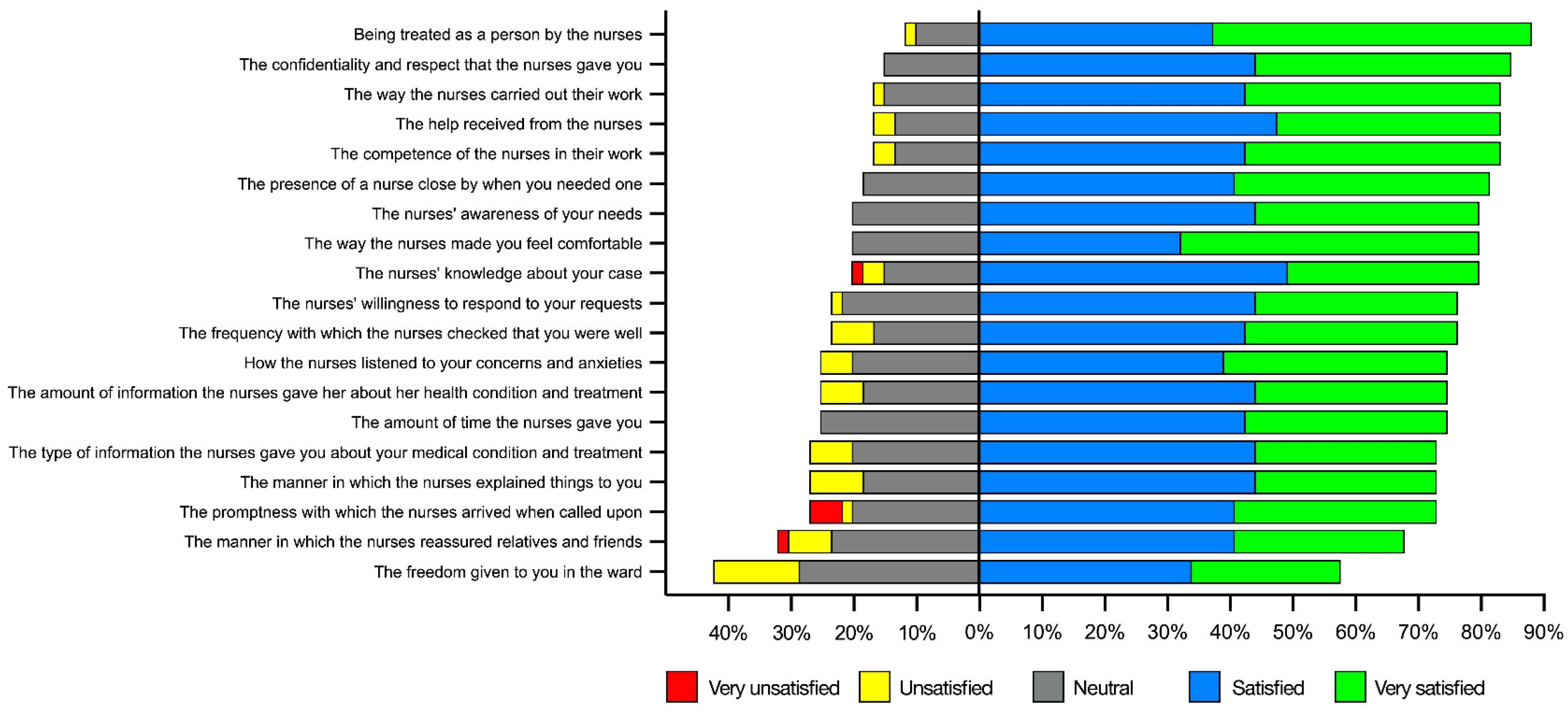
4.6. Patients’ Evaluation of Nursing Care: Data from Questionnaires and Patient Interviews
4.7. Patients’ Experiences with Respect to Their Needs: Data from Patient Interviews
4.8. Nursing Care (Data from Questionnaires and Interviews with Nurses and from Clinical Records)
4.9. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Weekly Epidemiological Update on COVID-19—24 November 2023. Available online: https://www.who.int/publications/m/item/covid-19-epidemiological-update---24-november-2023 (accessed on 24 November 2023).
- Cipriano, P.F. Influence: Nurses Can Change the World. Int. Nurs. Rev. 2022, 69, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Melnikov, S.; Kagan, I.; Felizardo, H.; Lynch, M.; Jakab-Hall, C.; Langan, L.; Vermeir, P.; Luiking-Martin, M.-L. Practices and Experiences of European Frontline Nurses under the Shadow of COVID-19. Nurs. Health Sci. 2022, 24, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Falcó-Pegueroles, A.; Rosa, D.; Tolotti, A.; Graffigna, G.; Bonetti, L. The Psychosocial Impact of Flu Influenza Pandemics on Healthcare Workers and Lessons Learnt for the COVID-19 Emergency: A Rapid Review. Int. J. Public Health 2020, 65, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Villa, M.; Balice-Bourgois, C.; Tolotti, A.; Falcó-Pegueroles, A.; Barello, S.; Luca, E.C.; Clivio, L.; Biegger, A.; Valcarenghi, D.; Bonetti, L. Ethical Conflict and Its Psychological Correlates among Hospital Nurses in the Pandemic: A Cross-Sectional Study within Swiss COVID-19 and Non-COVID-19 Wards. Int. J. Environ. Res. Public Health 2021, 18, 12012. [Google Scholar] [CrossRef] [PubMed]
- Stuijfzand, S.; Deforges, C.; Sandoz, V.; Sajin, C.-T.; Jaques, C.; Elmers, J.; Horsch, A. Psychological Impact of an Epidemic/Pandemic on the Mental Health of Healthcare Professionals: A Rapid Review. BMC Public Health 2020, 20, 1230. [Google Scholar] [CrossRef] [PubMed]
- Jubin, J.; Delmas, P.; Gilles, I.; Oulevey Bachmann, A.; Ortoleva Bucher, C. Protective Factors and Coping Styles Associated with Quality of Life during the COVID-19 Pandemic: A Comparison of Hospital or Care Institution and Private Practice Nurses. Int. J. Environ. Res. Public Health 2022, 19, 7112. [Google Scholar] [CrossRef] [PubMed]
- Pagnucci, N.; Fornili, M.; Pradal, M.; Uccelli, F.; Bovone, A.; Meini, M.; Scateni, M.; Baglietto, L.; Forfori, F. Reorganization of Intensive Care Units for the COVID-19 Pandemic: Effects on Nursing Sensitive Outcomes. J. Prev. Med. Hyg. 2022, 63, E383–E390. [Google Scholar] [CrossRef]
- International Council of Nurses (ICN). Nursing Definitions. Available online: https://www.icn.ch/resources/nursing-definitions (accessed on 24 November 2023).
- Barello, S.; Graffigna, G. Caring for Health Professionals in the COVID-19 Pandemic Emergency: Toward an “Epidemic of Empathy” in Healthcare. Front. Psychol. 2020, 11, 1431. [Google Scholar] [CrossRef]
- Sperling, D. Ethical Dilemmas, Perceived Risk, and Motivation among Nurses during the COVID-19 Pandemic. Nurs. Ethics 2021, 28, 9–22. [Google Scholar] [CrossRef]
- Cénat, J.M.; Blais-Rochette, C.; Kokou-Kpolou, C.K.; Noorishad, P.-G.; Mukunzi, J.N.; McIntee, S.-E.; Dalexis, R.D.; Goulet, M.-A.; Labelle, P.R. Prevalence of Symptoms of Depression, Anxiety, Insomnia, Posttraumatic Stress Disorder, and Psychological Distress among Populations Affected by the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Psychiatry Res. 2021, 295, 113599. [Google Scholar] [CrossRef]
- Cénat, J.M.; Dalexis, R.D.; Guerrier, M.; Noorishad, P.-G.; Derivois, D.; Bukaka, J.; Birangui, J.-P.; Adansikou, K.; Clorméus, L.A.; Kokou-Kpolou, C.K.; et al. Frequency and Correlates of Anxiety Symptoms during the COVID-19 Pandemic in Low- and Middle-Income Countries: A Multinational Study. J. Psychiatr. Res. 2021, 132, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Kola, L.; Kohrt, B.A.; Hanlon, C.; Naslund, J.A.; Sikander, S.; Balaji, M.; Benjet, C.; Cheung, E.Y.L.; Eaton, J.; Gonsalves, P.; et al. COVID-19 Mental Health Impact and Responses in Low-Income and Middle-Income Countries: Reimagining Global Mental Health. Lancet Psychiatry 2021, 8, 535–550. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.; Sheikh, T.L.; Gidado, S.; Poggensee, G.; Nguku, P.; Olayinka, A.; Ohuabunwo, C.; Waziri, N.; Shuaib, F.; Adeyemi, J.; et al. An Evaluation of Psychological Distress and Social Support of Survivors and Contacts of Ebola Virus Disease Infection and Their Relatives in Lagos, Nigeria: A Cross Sectional Study—2014. BMC Public Health 2015, 15, 824. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.R.; Shrivastava, P.S. COVID-19 and Impairment of Mental Health: Public Health Perspective. Afr. Health Sci. 2021, 21, 1527–1532. [Google Scholar] [CrossRef] [PubMed]
- D’Alvano, G.; Buonanno, D.; Passaniti, C.; De Stefano, M.; Lavorgna, L.; Tedeschi, G.; Siciliano, M.; Trojsi, F. Support Needs and Interventions for Family Caregivers of Patients with Amyotrophic Lateral Sclerosis (ALS): A Narrative Review with Report of Telemedicine Experiences at the Time of COVID-19 Pandemic. Brain Sci. 2021, 12, 49. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B. Revisiting health information technology ethical, legal, and social issues and evaluation: Telehealth/telemedicine and COVID-19. Int. J. Med. Inform. 2020, 143, 104239. [Google Scholar] [CrossRef]
- Chen, C.-S.; Wu, H.-Y.; Yang, P.; Yen, C.-F. Psychological Distress of Nurses in Taiwan Who Worked during the Outbreak of SARS. Psychiatr. Serv. 2005, 56, 76–79. [Google Scholar] [CrossRef]
- Falcó-Pegueroles, A.; Lluch-Canut, T.; Roldan-Merino, J.; Goberna-Tricas, J.; Guàrdia-Olmos, J. Ethical Conflict in Critical Care Nursing: Correlation between Exposure and Types. Nurs. Ethics 2015, 22, 594–607. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Hung, Y.-T.; Wang, H.-H.; Ma, S.-C.; Chang, S.-C. Factors of Resilience in Emergency Department Nurses Who Have Experienced Workplace Violence in Taiwan. J. Nurs. Scholarsh. 2016, 48, 23–30. [Google Scholar] [CrossRef]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.B.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-Term Psychological and Occupational Effects of Providing Hospital Healthcare during SARS Outbreak. Emerg. Infect. Dis. 2006, 12, 1924–1932. [Google Scholar] [CrossRef]
- Ortoleva Bucher, C.; Delmas, P.; Oulevey Bachmann, A.; Gilles, I. Stressors, Self-Reported Overall Health, Potential Protective Factors and the Workplace Well-Being of Nurses during the COVID-19 Pandemic in Switzerland: A Longitudinal Mixed-Methods Study Protocol. BMJ Open 2021, 11, e057021. [Google Scholar] [CrossRef] [PubMed]
- Feder, S.; Smith, D.; Griffin, H.; Shreve, S.T.; Kinder, D.; Kutney-Lee, A.; Ersek, M. “Why Couldn’t I Go in To See Him?” Bereaved Families’ Perceptions of End-of-Life Communication During COVID-19. J. Am. Geriatr. Soc. 2021, 69, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, C.S.; Magalhães, B.; Silva, S.; Edra, B. (Re)’Thinking’ Family in Nursing Care in Pandemic Times. Int. Nurs. Rev. 2022, 69, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Hugelius, K.; Harada, N.; Marutani, M. Consequences of Visiting Restrictions during the COVID-19 Pandemic: An Integrative Review. Int. J. Nurs. Stud. 2021, 121, 104000. [Google Scholar] [CrossRef] [PubMed]
- Keen, A.; George, A.; Stuck, B.T.; Snyder, C.; Fleck, K.; Azar, J.; Kara, A. Nurse Perceptions of a Nurse Family Liaison Implemented during the COVID-19 Pandemic: A Qualitative Thematic Analysis. Intensive Crit. Care Nurs. 2022, 70, 103185. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research; Sage: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Balice-Bourgois, C.; Bonetti, L.; Tolotti, A.; Liptrott, S.J.; Villa, M.; Luca, C.E.; Steiner, L.M.; Biegger, A.; Goncalves, S.; Moser, L.; et al. Experiences and Needs of Patients, Caregivers and Nurses during the COVID-19 Pandemic: Study Protocol for a Mixed-Methods Multicentre Study. Int. J. Environ. Res. Public Health 2022, 19, 12838. [Google Scholar] [CrossRef]
- Cantarelli, M. Il Modello Delle Prestazioni Infermieristiche; 3a Edizione; Casa Editrice Ambrosiana: Milano, Italy, 2003; ISBN 978-88-08-78000-3. [Google Scholar]
- Piredda, M.; Cossu, L.; Amato, S.; Alvaro, R.; Tartaglini, D.; Spiga, F.; Pascarella, M.; De Marinis, M.G. A Measure of Patient Satisfaction with Nursing Care: The Italian Version of “Newcastle Satisfaction with Nursing Scales” [Misura Della Soddisfazione Del Paziente per l’assistenza Infermieristica Ricevuta: Versione Del “Newcastle Satisfaction with Nursing Scales”]. Int. Nurs. Perspect. 2007, 7, 25–31. [Google Scholar]
- Piredda, M.; Vellone, E.; Piras, G.; Fida, R.; Latour, J.M.; Matarese, M.; Alvaro, R.; De Marinis, M.G. Psychometric Evaluation of the Newcastle Satisfaction with Nursing Scales. J. Nurs. Care Qual. 2015, 30, 84–92. [Google Scholar] [CrossRef][Green Version]
- Sandelowski, M. Sample Size in Qualitative Research. Res. Nurs. Health 1995, 18, 179–183. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Guba, E.G.; Lincoln, Y.S. Effective Evaluation: Improving the Usefulness of Evaluation Results through Responsive and Naturalistic Approaches; Jossey-Bass: Hoboken, NJ, USA, 1981; ISBN 0-87589-493-3. [Google Scholar]
- Carnevale, F.A. Authentic Qualitative Research and the Quest for Methodological Rigour. Can. J. Nurs. Res. 2002, 34, 121–128. [Google Scholar] [PubMed]
- Younas, A.; Pedersen, M.; Durante, A. Characteristics of Joint Displays Illustrating Data Integration in Mixed-methods Nursing Studies. J. Adv. Nurs. 2020, 76, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Younas, A.; Pedersen, M.; Tayaben, J.L. Review of Mixed-Methods Research in Nursing. Nurs. Res. 2019, 68, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Guetterman, T.C.; Fetters, M.D.; Creswell, J.W. Integrating Quantitative and Qualitative Results in Health Science Mixed Methods Research through Joint Displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Younas, A.; Rasheed, S.P.; Zeb, H. Using Legitimation Criteria to Establish Rigour in Sequential Mixed-Methods Research. Nurse Res. 2020, 28, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Ardakani, M.F.; Farajkhoda, T.; Mehrabbeik, A. Lived Experiences of Recovered COVID-19 Patients after Hospitalization: A Phenomenological Research. Iran. J. Nurs. Midwifery Res. 2022, 27, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Son, H.-M.; Choi, W.-H.; Hwang, Y.-H.; Yang, H.-R. The Lived Experiences of COVID-19 Patients in South Korea: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 7419. [Google Scholar] [CrossRef]
- Alkaissi, A.; Zaben, F.; Abu-Rajab, M.; Alkony, M. Lived Experiences of Palestinian Patients with COVID-19: A Multi-Center Descriptive Phenomenological Study of Recovery Journey. BMC Public Health 2022, 22, 470. [Google Scholar] [CrossRef]
- Falcó-Pegueroles, A.; Bosch-Alcaraz, A.; Terzoni, S.; Fanari, F.; Viola, E.; Via-Clavero, G.; Hoyo, S.G.-D.; Parini, A.M.; Poveda-Moral, S.; Parozzi, M.; et al. COVID-19 Pandemic Experiences, Ethical Conflict and Decision-Making Process in Critical Care Professionals (Quali-Ethics-COVID-19 Research Part 1): An International Qualitative Study. J. Clin. Nurs. 2023, 32, 5185–5200. [Google Scholar] [CrossRef]
- Firouzkouhi, M.; Abdollahimohammad, A.; Rezaie-Kheikhaie, K.; Mortazavi, H.; Farzi, J.; Masinaienezhad, N.; Hashemi-Bonjar, Z. Nurses’ Caring Experiences in COVID-19 Pandemic: A Systematic Review of Qualitative Research. Health Sci. Rev. 2022, 3, 100030. [Google Scholar] [CrossRef]
- Falcó-Pegueroles, A.; Viola, E.; Poveda-Moral, S.; Rodríguez-Martín, D.; Via-Clavero, G.; Barello, S.; Bosch-Alcaraz, A.; Bonetti, L. Protective Factors of Ethical Conflict during a Pandemic-Quali-Ethics-COVID-19 Research Part 2: An International Qualitative Study. J. Clin. Nurs. 2023, 32, 6677–6689. [Google Scholar] [CrossRef] [PubMed]
- Henderson, V. The Concept of Nursing. J. Adv. Nurs. 2006, 53, 21–31, discussion 32–34. [Google Scholar] [CrossRef] [PubMed]
- Gunawan, J.; Aungsuroch, Y.; Watson, J.; Marzilli, C. Nursing Administration: Watson’s Theory of Human Caring. Nurs. Sci. Q. 2022, 35, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Kitson, A. Fundamentals of Care: Methodologies, Metrics and Mobilisation. J. Clin. Nurs. 2020, 29, 1762–1764. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.; Prandi, C.; Bonetti, L. Experience of Middle Management Nurses during the COVID-19 Pandemic in Switzerland: A Qualitative Study. J. Nurs. Manag. 2021, 29, 1956–1964. [Google Scholar] [CrossRef] [PubMed]
- Förster, C.; Paparella, C.; Duchek, S.; Güttel, W.H. Leading in the Paradoxical World of Crises: How Leaders Navigate through Crises. Schmalenbachs Z. Betriebswirtschaftliche Forsch. 2022, 74, 631–657. [Google Scholar] [CrossRef] [PubMed]
- Kutney-Lee, A.; Stimpfel, A.W.; Sloane, D.M.; Cimiotti, J.P.; Quinn, L.W.; Aiken, L.H. Changes in Patient and Nurse Outcomes Associated with Magnet Hospital Recognition. Med. Care 2015, 53, 550. [Google Scholar] [CrossRef]
- Scott, J.G.; Sochalski, J.; Aiken, L. Review of Magnet Hospital Research: Findings and Implications for Professional Nursing Practice. J. Nurs. Adm. 1999, 29, 9–19. [Google Scholar] [CrossRef]
- Watson, J.; Woodward, T. Jean Watson’s Theory of Human Caring; SAGE Publications Limited: London, UK, 2020; ISBN 1-5297-2756-1. [Google Scholar]
- Valcarenghi, D.; Bagnasco, A.; Aleo, G.; Catania, G.; Zanini, M.; Cavaliere, B.; Carnevale, F.; Sasso, L. Exploring the Interaction between Nursing Decision Making and Patient Outcomes in 2 European Cancer Centers: A Qualitative Study. Cancer Nurs. 2018, 41, E40–E49. [Google Scholar] [CrossRef]
- Tolotti, A.; Bagnasco, A.; Catania, G.; Aleo, G.; Pagnucci, N.; Cadorin, L.; Zanini, M.; Rocco, G.; Stievano, A.; Carnevale, F.A.; et al. The Communication Experience of Tracheostomy Patients with Nurses in the Intensive Care Unit: A Phenomenological Study. Intensive Crit. Care Nurs. 2018, 46, 24–31. [Google Scholar] [CrossRef]
- Tolotti, A.; Cadorin, L.; Bonetti, L.; Valcarenghi, D.; Pagnucci, N. Communication Experiences of Tracheostomy Patients with Nurses in the ICU: A Scoping Review. J. Clin. Nurs. 2023, 32, 2361–2370. [Google Scholar] [CrossRef] [PubMed]
- Twigg, D.E.; Kutzer, Y.; Jacob, E.; Seaman, K. A Quantitative Systematic Review of the Association between Nurse Skill Mix and Nursing-Sensitive Patient Outcomes in the Acute Care Setting. J. Adv. Nurs. 2019, 75, 3404–3423. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Marisa Cantarelli’s Nursing Performance Model [30] |
|---|
| Fundamental nursing needs |
|
|
|
|
|
|
|
|
|
|
|
| Nurses’ Characteristics | All Nurses * | Patients’ Characteristics | All Patients | ||
|---|---|---|---|---|---|
| (n = 100) | (n = 57) | ||||
| Age | Age, mean years, ±SD | 69 | ±11.0 | ||
| 20 to 30 years | 33 | (34.4) | Female, gender | 18 | (31.5) |
| 31 to 50 years | 46 | (47.9) | BMI, mean kg/m2, ±SD | 27.4 | ±5.5 |
| 51 to 60 years | 17 | (17.7) | Autonomous/partially autonomous | 55 | (96.4) |
| Female, gender | 68 | (70.8) | Previous comorbidity | 32 | (56.1) |
| Years of experience as nurse | Hypertension | 17 | (29.8) | ||
| 0 to 5 | 24 | (25.0) | Diabetes mellitus | 9 | (15.7) |
| 6 to 20 | 47 | (49.0) | Renal impairment | 3 | (5.2) |
| over 20 | 25 | (26.0) | Heart diseases | 9 | (15.7) |
| Post-graduate education | 80 | (80.0) | Other | 7 | (12.2) |
| Intensive care employment during pandemic | 33 | (34.7) | High educational level | 19 | (33.3) |
| Hospital length of stay during COVID-19 pandemic, median (IQR) | 17 | (13–37) | |||
| Admission in ICU | 25 | (43.8) | |||
| NURSES (n = 100) Top Three Most Common Nursing Interventions Performed | PATIENTS (n = 57) Top Three Common Nursing Interventions Received | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Interventions | n. (%) | Degree of Usefulness | Interventions | n (%) | Degree of Usefulness | ||||
| Breathing | |||||||||
| Assessment/monitoring of respiratory parameters | 99 | (99.0) | 10 | (9–10) | Supply me with oxygen | 49 | (85.9) | 8 | (5–10) |
| Prevention of complications from devices used | 95 | (95.0) | 8 | (7–10) | Airing out the room | 37 | (64.9) | 6 | (4–7) |
| Support in cases of anxiety/dyspnoea | 91 | (91.0) | 9 | (8–10) | Getting me into a sitting position | 27 | (47.4) | 6.5 | (3–8) |
| Resting and sleeping | |||||||||
| Discretionary use of drugs in reserve | 85 | (85.0) | 8 | (6–10) | Promoting a peaceful and quiet environment | 32 | (56.1) | 8 | (5–9) |
| Communication and relationship for anxiety situations | 83 | (83.0) | 8 | (7–10) | Administering therapy | 28 | (49.1) | 7 | (4–10) |
| Promoting a comfortable sleeping environment | 83 | (83.0) | 8 | (5–10) | Switching off or dimming the light | 27 | (47.4) | 7 | (4–10) |
| Interacting in communication | |||||||||
| Maintaining a constant presence at the patient’s bedside | 94 | (94.0) | 8 | (6–10) | Provide me with clear information about my situation | 45 | (78.9) | 8 | (6.5–10) |
| Maintain appropriate communication | 92 | (92.0) | 9 | (8–10) | Answer my questions | 39 | (68.4) | 8 | (6–10) |
| Ensuring communication with relatives | 87 | (87.0) | 10 | (8–10) | Explain to me which interventions they were going to do | 38 | (66.7) | 8 | (7.5–10) |
| Movement | |||||||||
| Help with moving without aids | 85 | (85.0) | 7 | (5–9) | Getting me to exercise | 28 | (49.1) | 8 | (5–10) |
| Promotion of physiotherapy programme | 83 | (83.0) | 8 | (5–9) | Helping me get out of bed, sit in an armchair, and get back into bed | 21 | (36.8) | 8 | (4–10) |
| Maintaining motor skills | 80 | (80.0) | 8 | (6–10) | Helping me move in bed | 20 | (35.1) | 7 | (4.5–8.5) |
| Nutrition and hydration | |||||||||
| Monitoring of glycaemia (for diabetic patients) | 99 | (99.0) | 9 | (8–10) | Checking my glycaemia | 34 | (59.6) | 7 | (3–10) |
| Surveillance of nutritional status and hydration | 94 | (94.0) | 8 | (7–10) | Asking me what I preferred to eat | 33 | (57.9) | 8 | (6–10) |
| Surveillance and management of disorders such as nausea and vomiting | 89 | (89.0) | 8 | (7–10) | Giving me drips | 32 | (56.1) | 8 | (5–10) |
| Hygiene | |||||||||
| Skin surveillance and/or care | 95 | (95.0) | 9 | (8–10) | Provide me with hygiene care supplies | 37 | (64.9) | 7 | (3–9) |
| Oral cavity surveillance and/or care | 94 | (96.0) | 9 | (8–10) | Help me wash or shower | 26 | (45.6) | 6.5 | (4–10) |
| Partial or full help with hygiene | 91 | (91.0) | 8 | (7–10) | Accompany me to the bathroom | 24 | (42.1) | 7 | (4–10) |
| Urinary and bowel elimination | |||||||||
| Control on adequate elimination | 95 | (95.0) | 9 | (8–10) | Accompany me to the bathroom | 20 | (35.1) | 7 | (4–10) |
| Bladder catheter management | 93 | (93.0) | 8 | (7–10) | Bring me the bedpan or the urinal | 18 | (31.6) | 7.5 | (2–10) |
| Assisting in the use of elimination aids (urinal, bedpan, commode chair) | 80 | (80.0) | 8 | (7–10) | Placing me in the commode chair | 13 | (22.8) | 7 | (0–10) |
| Safe environment | |||||||||
| Correct use of protective equipment | 90 | (90.0) | 10 | (7–10) | Explain how to prevent the spread of COVID-19 | 38 | (66.7) | 8 | (7–10) |
| Preventing situations of disorientation and delirium | 88 | (88.8) | 8 | (7–10) | Maintain a clean environment | 35 | (61.4) | 8 | (7–10) |
| Preventing accidental falls by acting environment | 84 | (84.4) | 8 | (7–10) | Explain how to avoid falls and injuries | 19 | (33.4) | 8 | (5–10) |
| Maintaining cardiovascular function | |||||||||
| Surveillance of vital parameters | 95 | (95.0) | 10 | (9–10) | Take my blood pressure | 46 | (80.7) | 7 | (6–10) |
| Surveillance of states of consciousness | 95 | (95.0) | 10 | (8–10) | Take my body temperature | 45 | (78.9) | 7 | (6–10) |
| Maintaining an adequate body temperature | 95 | (95.0) | 8 | (8–10) | Administer my therapy | 39 | (68.4) | 8 | (6–10) |
| Therapeutic procedures * | |||||||||
| Therapy administration and monitoring | 96 | (96.0) | 9 | (8–10) | n.a. | ||||
| Administering oxygen therapy | 94 | (94.0) | 10 | (8–10) | n.a. | ||||
| Monitoring possible complications due to therapy | 94 | (94.0) | 10 | (8–10) | n.a. | ||||
| Diagnostic procedures * | |||||||||
| Collecting biological samples | 95 | (95.0) | 8 | (5–9) | n.a. | ||||
| Monitoring disease evolution | 93 | (93.0) | 9 | (8–10) | n.a. | ||||
| Supporting patients with anxieties and fears | 85 | (85.0) | 8 | (5–10) | n.a. | ||||
| NPM Nursing Needs | Novelty Nursing Interventions | n. (%) | |
|---|---|---|---|
| Breathing | Use of oxygen delivery devices (Venturi system, CPAP) | 7 | (7.0) |
| Resting and sleeping | Use of new medicines for analgesia-sedation due to depletion of usual medicine stocks | 4 | (4.0) |
| Interacting in communication | Ensuring communication with relatives (telephone, tablet, or other) | 10 | (10.0) |
| Movement | Implementing pronation | 13 | (13.0) |
| Nutrition and hydration | Feeding tracheostomised patients | 2 | (2.0) |
| Hygiene | Teaching about hygiene problems for home discharge | 2 | (2.0) |
| Urinary and bowel elimination | Handling fecal incontinence devices | 2 | (2.0) |
| Safe environment | Use of personal protective equipment | 5 | (5.0) |
| Maintaining cardiovascular function | Invasive monitoring of haemodynamic parameters | 3 | (3.0) |
| Therapeutic procedures | Artificial ventilation in patients with respiratory insufficiency | 2 | (2.0) |
| Diagnostic procedures | Monitoring of disease evolution COVID-19 | 4 | (4.0) |
| Nurses Interviews (n = 16) | |
|---|---|
| Macro Theme | Themes |
|
|
|
|
|
|
|
|
|
|
| Patient Interviews (n = 15) | |
|---|---|
| Macro Theme | Themes |
|
|
|
|
|
|
|
|
| Quantitative Results (Nurse Survey) | Clinical Records | Quantitative Results (Patient Survey) | Qualitative Results (Nurse Interviews) | Qualitative Results (Patient Interviews) | Agree | Disagree | Integration of Quantitative and Qualitative Data. |
|---|---|---|---|---|---|---|---|
| 78% of the nurses were aware of their needs. 80% of the patients were fully satisfied with the nursing care received. | Many patients were grateful for the care received, also because they realized the nurses’ high level of stress and dedication to ensure the best possible care. | Appreciation of the nurses’ technical and professional competence. | X | The nursing staff is fully committed to ensuring the highest quality of care and patients realize this. | |||
Needs considered important by nurses:
| Need to breathe reported in most clinical records. The need for sleep and rest was reported less frequently. Management of crisis conversations with patients and family members | Needs considered important by patients:
| Importance of the need to breathe, respiratory monitoring, and timely interventions. Importance of the need for sleep and rest (in relation to asthenia, disturbed sleep). Communication managed by nurses at different moments (admission, to reassure, support during respiratory weaning, reassurance during functional recovery). | Breathing difficulty made the person experience the fear of dying. Importance of the need for sleep and rest. Support and encouragement from nurses. Difficulty recognizing faces due to masks, making communication difficult. | X X X | The same perception of the main problems was identified both from the patients’ and nurses’ points of view. The need for breathing is not mentioned in the patient interviews. The need for sleep and rest was described as as being important, but appeared less in the clinical records. | |
| Implicit or rarely stated objectives | Generic objectives: generic objectives were pursued based on clinical evolution and changes in knowledge about the disease. | X | |||||
| 34% of nurses reported that they had implemented new actions to address the need to breathe (pronation, high flow oxygen therapy with Venturi mask) and for communication (video calls). | Interventions related to the need to breathe and communicate were present in most of the clinical records. | Giving me oxygen (Median 8 (5–10]) Letting me communicate with my family via mobile phone/tablet (Median 8 (6.5–9.5)). Explaining to me the interventions they were about to perform (Median 8 (5.75–10)). | New skills emerged in relation to breathing and communication needs. New actions: high flow oxygen therapy, pronation, use of new scores—early warning score, use of technology to facilitate communication. | Facilitating contacts with family members (mobile phones/video calls). Clear information about nursing interventions. | X | There is full agreement between different data sources about breathing and communication needs and the related interventions. | |
| Giving me clear information about my situation (Median 8 (6.5–10)). | Insufficient information about the clinical situation, intubation, and awakening. | X | There are differences between the quantitative and qualitative data of the patients. | ||||
| Seeing them all naked in these big rooms. Distorted faces. | Body image—seeing themselves unkempt caused embassment and suffering. | X | |||||
| For nurses, there was not enough time to provide care due to the workload. | Time that passes slowly causes suffering | X | |||||
| Continuous patient turnover. Nurses suffered seeing people die alone. | Hearing what happened to other patients increased the fear of death. | X | Anguish for death, even if experienced differently by nurses and patients. | ||||
| Sense of helplessness and fear of not doing the right thing. | Feeling helpless for not being able to do anything anymore. | X | Sense of helplessness for both stakeholders, but for different reasons. | ||||
| Fear of contagion. | |||||||
| Nurses had difficulty capturing sudden changes due to poor perception of patients’ respiratory deterioration. | They felt confused and surprised when they were unexpectedly and suddenly told that they would be intubated. | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tolotti, A.; Bonetti, L.; Luca, C.E.; Villa, M.; Liptrott, S.J.; Steiner, L.M.; Balice-Bourgois, C.; Biegger, A.; Valcarenghi, D. Nurses Response to the Physical and Psycho-Social Care Needs of Patients with COVID-19: A Mixed-Methods Study. Healthcare 2024, 12, 114. https://doi.org/10.3390/healthcare12010114
Tolotti A, Bonetti L, Luca CE, Villa M, Liptrott SJ, Steiner LM, Balice-Bourgois C, Biegger A, Valcarenghi D. Nurses Response to the Physical and Psycho-Social Care Needs of Patients with COVID-19: A Mixed-Methods Study. Healthcare. 2024; 12(1):114. https://doi.org/10.3390/healthcare12010114
Chicago/Turabian StyleTolotti, Angela, Loris Bonetti, Corina Elena Luca, Michele Villa, Sarah Jayne Liptrott, Laura Maria Steiner, Colette Balice-Bourgois, Annette Biegger, and Dario Valcarenghi. 2024. "Nurses Response to the Physical and Psycho-Social Care Needs of Patients with COVID-19: A Mixed-Methods Study" Healthcare 12, no. 1: 114. https://doi.org/10.3390/healthcare12010114
APA StyleTolotti, A., Bonetti, L., Luca, C. E., Villa, M., Liptrott, S. J., Steiner, L. M., Balice-Bourgois, C., Biegger, A., & Valcarenghi, D. (2024). Nurses Response to the Physical and Psycho-Social Care Needs of Patients with COVID-19: A Mixed-Methods Study. Healthcare, 12(1), 114. https://doi.org/10.3390/healthcare12010114