
The Insomnia Severity Index: Factor Structure and Measurement and Structural Invariance across Perinatal Time Points

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
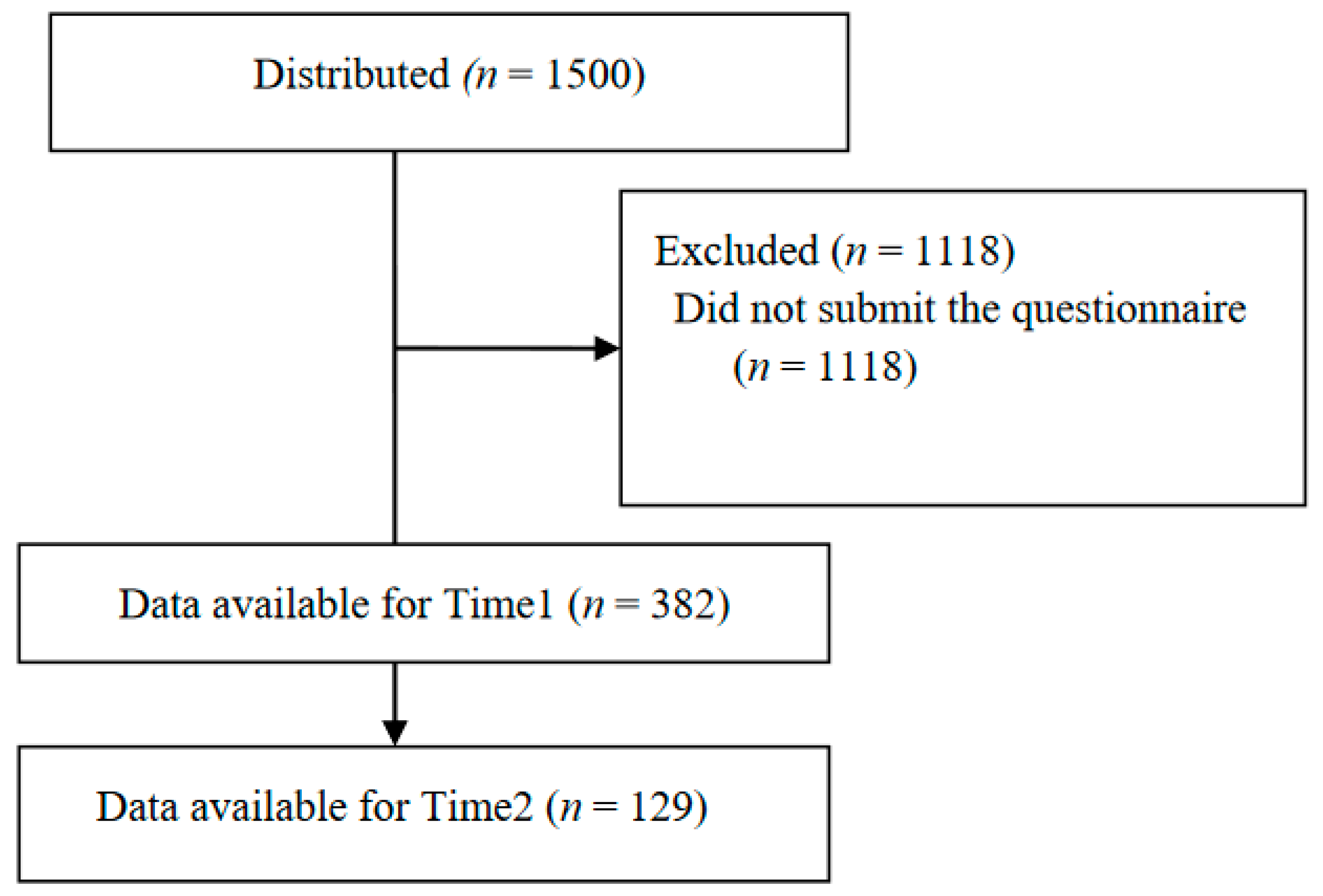
2.1. Procedures and Participants
2.2. Measurements
2.3. Data Analysis
2.3.1. EFA and CFA
2.3.2. Measurement Invariance and Structure Invariance
2.4. Ethical Considerations
3. Results
3.1. EFAs
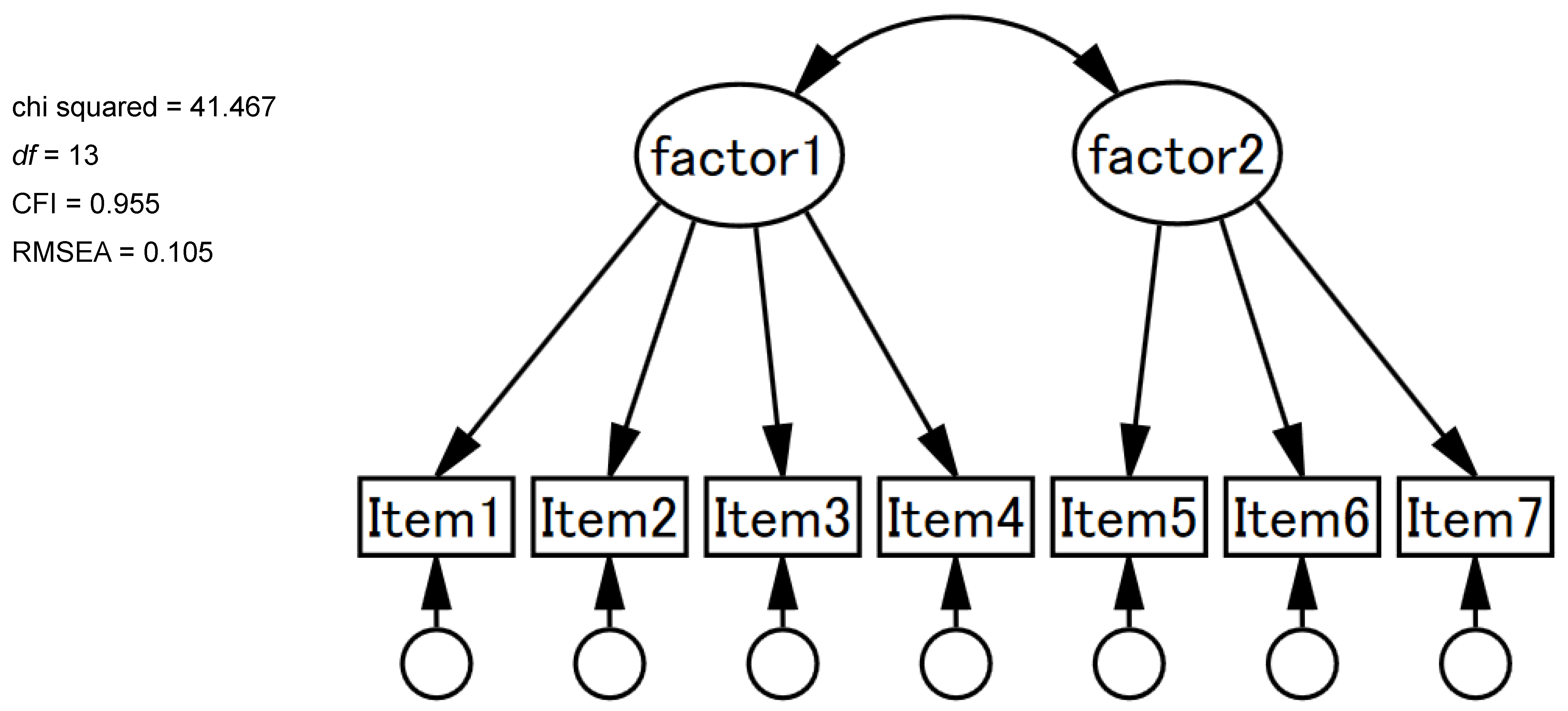
3.2. CFAs, Measurement Invariance, and Structure Invariance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morin, C.M.; Jarrin, D.C. Epidemiology of insomnia: Prevalence, course, risk factors, and public health burden. Sleep Med. Clin. 2022, 17, 173–191. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Satirical Manual of Mental Disorders, 5th ed.; (DSM-5); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Naud, K.; Ouellet, A.; Brown, C.; Pasquier, J.C.; Moutquin, J.M. Is sleep disturbed in pregnancy? J. Obstet. Gynaecol. Can. 2010, 32, 28–34. [Google Scholar] [CrossRef]
- Nodine, P.M.; Matthews, E.E. Common sleep disorders: Management strategies and pregnancy outcomes. J. Midwifery Womens Health 2013, 58, 368–377. [Google Scholar] [CrossRef]
- Hashmi, A.M.; Bhatia, S.K.; Bhatia, S.K.; Khawaja, I.S. Insomnia during pregnancy: Diagnosis and rational interventions. Pak. J. Med. Sci. 2016, 32, 1030–1037. [Google Scholar] [CrossRef]
- Hertz, G.; Fast, A.; Feinsilver, S.H.; Albertario, C.L.; Schulman, H.; Fein, A.M. Sleep in normal late pregnancy. Sleep 1992, 15, 246–251. [Google Scholar] [CrossRef]
- Wilson, D.L.; Barnes, M.; Ellett, L.; Permezel, M.; Jackson, M.; Crowe, S.F. Decreased sleep efficiency, increased wake after sleep onset and increased cortical arousals in late pregnancy. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 38–46. [Google Scholar] [CrossRef]
- Sedov, I.D.; Cameron, E.E.; Madigan, S.; Tomfohr-Madsen, L.M. Sleep quality during pregnancy: A meta-analysis. Sleep Med. Rev. 2018, 38, 168–176. [Google Scholar] [CrossRef]
- Fernández-Alonso, A.M.; Trabalón-Pastor, M.; Chedraui, P.; Pérez-López, F.R. Factors related to insomnia and sleepiness in the late third trimester of pregnancy. Arch. Gynecol. Obstet. 2012, 286, 55–61. [Google Scholar] [CrossRef]
- Mindell, J.A.; Cook, R.A.; Nikolovski, J. Sleep patterns and sleep disturbances across pregnancy. Sleep Med. 2015, 16, 483–488. [Google Scholar] [CrossRef]
- Okun, M.L.; Schetter, C.D.; Glynn, L.M. Poor sleep quality is associated with preterm birth. Sleep 2011, 34, 1493–1498. [Google Scholar] [CrossRef]
- Strange, L.B.; Parker, K.P.; Moore, M.L.; Strickland, O.L.; Bliwise, D.L. Disturbed sleep and preterm birth: A potential relationship? Clin. Exp. Obstet. Gynecol. 2009, 36, 166–168. [Google Scholar] [PubMed]
- Naghi, I.; Keypour, F.; Ahari, S.B.; Tavalai, S.A.; Khak, M. Sleep disturbance in late pregnancy and type and duration of labour. J. Obstet. Gynaecol. 2011, 31, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Jomeen, J.; Martin, C.R. Assessment and relationship of sleep quality to depression in early pregnancy. J. Reprod. Infant. Psychol. 2007, 25, 87–99. [Google Scholar] [CrossRef]
- Okun, M.L. Sleep and postpartum depression. Curr. Opin. Psychiatry 2015, 28, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Spielman, A.J.; Saskin, P.; Thorpy, M.J. Treatment of chronic insomnia by restriction of time in bed. Sleep 1987, 10, 45–56. [Google Scholar]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Kalmbach, D.A.; Cheng, P.; Roth, A.; Roth, T.; Swanson, L.M.; O’Brien, L.M.; Fresco, D.M.; Harb, N.C.; Cuamatzi-Castelan, A.S.; Reffi, A.N.; et al. DSM-5 insomnia disorder in pregnancy: Associations with depression, suicidal ideation, and cognitive and somatic arousal, and identifying clinical cutoffs for detection. Sleep Adv. 2022, 3, zpac006. [Google Scholar] [CrossRef]
- Sadeghniiat-Haghighi, K.; Montazeri, A.; Khajeh-Mehrizi, A.; Nedjat, S.; Aminian, O. The Insomnia Severity Index: Cross-cultural adaptation and psychometric evaluation of a Persian version. Qual. Life Res. 2014, 23, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Castronovo, V.; Galbiati, A.; Marelli, S.; Brombin, C.; Cugnata, F.; Giarolli, L.; Anelli, M.M.; Rinaldi, F.; Ferini-Strambi, L. Validation study of the Italian version of the Insomnia Severity Index (ISI). Neurol. Sci. 2016, 37, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Dragioti, E.; Wiklund, T.; Alföldi, P.; Gerdle, B. The Swedish version of the Insomnia Severity Index: Factor structure analysis and psychometric properties in chronic pain patients. Scand. J. Pain 2015, 9, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Kan, K.K.; Yeung, W.F. Assessing insomnia in adolescents: Comparison of Insomnia Severity Index, Athens Insomnia Scale and Sleep Quality Index. Sleep Med. 2011, 12, 463–470. [Google Scholar] [CrossRef]
- Gerber, M.; Lang, C.; Lemola, S.; Colledge, F.; Kalak, N.; Holsboer-Trachsler, E.; Pühse, U.; Brand, S. Validation of the German version of the insomnia severity index in adolescents, young adults and adult workers: Results from three cross-sectional studies. BMC Psychiatry 2016, 16, 174. [Google Scholar] [CrossRef]
- Otte, J.L.; Bakoyannis, G.; Rand, K.L.; Ensrud, K.E.; Guthrie, K.A.; Joffe, H.; McCurry, S.M.; Newton, K.M.; Carpenter, J.S. Confirmatory factor analysis of the Insomnia Severity Index (ISI) and invariance across race: A pooled analysis of MsFLASH data. Menopause 2019, 26, 850–855. [Google Scholar] [CrossRef]
- Chen, P.Y.; Yang, C.M.; Morin, C.M. Validating the cross-cultural factor structure and invariance property of the Insomnia Severity Index: Evidence based on ordinal EFA and CFA. Sleep Med. 2015, 16, 598–603. [Google Scholar] [CrossRef]
- Fernandez-Mendoza, J.; Rodriguez-Muñoz, A.; Vela-Bueno, A.; Olavarrieta-Bernardino, S.; Calhoun, S.L.; Bixler, E.O.; Vgontzas, A.N. The Spanish version of the Insomnia Severity Index: A confirmatory factor analysis. Sleep Med. 2012, 13, 207–210. [Google Scholar] [CrossRef]
- van de Vijver, F.J.R.; Leung, K. Methodological issues in psychological research on culture. J. Cross Cult. Psychol. 2000, 31, 33–51. [Google Scholar] [CrossRef]
- Vandenberg, R.J.; Lance, C.E. A review and synthesis of the measurement invariance literature: Suggestions, practices, and recommendations for organizational research. Organ. Res. Methods 2000, 3, 4–70. [Google Scholar] [CrossRef]
- Munezawa, T.; Morin, C.M.; Inoue, Y.; Nedate, K. Development of the Japanese version of Insomnia Severity Index (ISI-J). Jpn. J. Psychiatr. Treat. 2009, 24, 219–225. (In Japanese) [Google Scholar]
- Okajima, I.; Nakajima, S.; Kobayashi, M. Which Insomnia Severity Rating Scale is most appropriate for Screening? A comparative study of the; PSIQ, AIS, and ISI. In Proceedings of the Japanese Association of Behavior Therapy Academic Conference, Tokyo, Japan, 26 November 2011; Volume 37, pp. 146–147. [Google Scholar]
- Schermelleh-Engell, K.; Moosbrugger, H.; Muller, H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Chen, F.F. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equ. Model. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Manzar, M.D.; Jahrami, H.A.; Bahammam, A.S. Structural validity of the Insomnia Severity Index: A systematic review and meta-analysis. Sleep Med. Rev. 2021, 60, 101531. [Google Scholar] [CrossRef]
- Mindell, J.A.; Jacobson, B.J. Sleep disturbances during pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2000, 29, 590–597. [Google Scholar] [CrossRef]
- Hada, A.; Minatani, M.; Wakamatsu, M.; Kitamura, T. Disability during early pregnancy: Using the Sheehan Disability Scale during the first trimester in Japan. Healthcare 2022, 10, 2514. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Item No. | n | Contents | Mean (SD) | Skewness | Kurtosis |
|---|---|---|---|---|---|
| 1 | 378 | Severity of sleep onset | 1.9 (1.0) | 0.80 | −0.27 |
| 2 | 379 | Sleep maintenance | 2.2 (1.1) | 0.40 | −0.78 |
| 3 | 378 | Early morning awakening problems | 2.0 (1.1) | 0.80 | −0.33 |
| 4 | 379 | Sleep satisfaction | 3.1 (0.9) | −0.22 | 0.03 |
| 5 | 379 | Interference of sleep difficulties with daytime functioning | 2.2 (1.0) | 0.45 | −0.40 |
| 6 | 372 | Noticeability of sleep problems by others | 1.9 (1.0) | 0.73 | −0.31 |
| 7 | 379 | Distress caused by the sleep difficulties | 1.8 (0.9) | 0.82 | −0.20 |
| Item | Communality | 1-Factor | 2-Factor | 3-Factor | |||
|---|---|---|---|---|---|---|---|
| I | I | II | I | II | III | ||
| 1 | 0.49 | 0.70 | 0.26 | 0.56 | 0.22 | 0.50 | 0.13 |
| 2 | 0.39 | 0.62 | −0.08 | 0.93 | −0.05 | 0.91 | 0.01 |
| 3 | 0.30 | 0.54 | −0.06 | 0.78 | −0.02 | 0.79 | −0.06 |
| 4 | 0.43 | 0.65 | 0.36 | 0.38 | −0.02 | 0.00 | 0.94 |
| 5 | 0.69 | 0.83 | 0.83 | 0.03 | 0.78 | 0.01 | 0.09 |
| 6 | 0.59 | 0.77 | 0.84 | −0.04 | 0.91 | 0.03 | −0.15 |
| 7 | 0.63 | 0.80 | 0.87 | −0.04 | 0.82 | −0.05 | 0.08 |
| χ2 | df | χ2/df | Δχ2(df) | CFI | ΔCFI | RMSEA | ΔRMSEA | Judgement | |
|---|---|---|---|---|---|---|---|---|---|
| Primiparas (n = 168) vs. multiparas (n = 210) | |||||||||
| Configural | 76.948 | 26 | 2.960 | Ref | 0.958 | Ref | 0.072 | Ref | Accept |
| Metric | 83.150 | 31 | 2.682 | 6.202(5) | 0.957 | 0.001 | 0.067 | +0.005 | Accept |
| Scalar | 84.534 | 38 | 2.225 | 1.384(7) | 0.962 | +0.005 | 0.057 | +0.010 | Accept |
| Residual | 90.016 | 45 | 2.000 | 5.483(7) | 0.963 | +0.001 | 0.052 | +0.005 | Accept |
| Factor variance | 91.764 | 47 | 1.952 | 1.748(2) | 0.963 | 0.000 | 0.050 | +0.002 | Accept |
| Factor covariance | 91.862 | 48 | 1.914 | 0.098(1) | 0.964 | +0.001 | 0.049 | +0.003 | Accept |
| Time 1 (n = 382) vs. Time 2 (n = 129) | |||||||||
| Configural | 85.441 | 26 | 3.286 | Ref | 0.967 | Ref | 0.067 | Ref | Accept |
| Metric | 93.034 | 31 | 3.001 | 2.701(5) | 0.966 | 0.001 | 0.063 | +0.004 | Accept |
| Scalar | 106.893 | 38 | 2.813 | 13.651(7) | 0.962 | 0.004 | 0.060 | +0.003 | Accept |
| Residual | 128.468 | 45 | 2.855 | 22.591(7) | 0.954 | 0.008 | 0.060 | 0.000 | Accept |
| Factor variance | 128.742 | 47 | 2.739 | 0.324(2) | 0.955 | +0.001 | 0.058 | +0.002 | Accept |
| Factor covariance | 130.616 | 48 | 2.721 | 0.042(1) | 0.954 | 0.001 | 0.058 | 0.000 | Accept |
| Factor | Factor Mean Differences | SE |
|---|---|---|
| Multipara compared with nullipara | ||
| Severity | 0.023 NS | 0.087 |
| Impact | −0.014 NS | 0.075 |
| Time 2 compared with Time 1 | ||
| Severity | −0.047 NS | 0.073 |
| Impact | 0.078 NS | 0.086 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shinohara, E.; Hada, A.; Minatani, M.; Wakamatsu, M.; Kitamura, T. The Insomnia Severity Index: Factor Structure and Measurement and Structural Invariance across Perinatal Time Points. Healthcare 2023, 11, 1194. https://doi.org/10.3390/healthcare11081194
Shinohara E, Hada A, Minatani M, Wakamatsu M, Kitamura T. The Insomnia Severity Index: Factor Structure and Measurement and Structural Invariance across Perinatal Time Points. Healthcare. 2023; 11(8):1194. https://doi.org/10.3390/healthcare11081194
Chicago/Turabian StyleShinohara, Eriko, Ayako Hada, Mariko Minatani, Mikiyo Wakamatsu, and Toshinori Kitamura. 2023. "The Insomnia Severity Index: Factor Structure and Measurement and Structural Invariance across Perinatal Time Points" Healthcare 11, no. 8: 1194. https://doi.org/10.3390/healthcare11081194
APA StyleShinohara, E., Hada, A., Minatani, M., Wakamatsu, M., & Kitamura, T. (2023). The Insomnia Severity Index: Factor Structure and Measurement and Structural Invariance across Perinatal Time Points. Healthcare, 11(8), 1194. https://doi.org/10.3390/healthcare11081194