Abstract
Objectives: The objectives of this scoping review are to estimate the prevalence of obesity and overweight in the Saudi community and in different age groups, genders, and geographical location, in addition to the change in prevalence over time. Methods: This scoping review of evidence was conducted in accordance with the Joanna Briggs Institute methodology for scoping reviews and was reported following the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. The population of this review was categorized into four age groups: young adults (18–25 years), adults (26–45), (mid-life adults) (46–60) and old people (60+). Each group was then categorized by gender into males and females. We included studies of adults aged 18 years and above. The pooled prevalence of obesity and overweight of the population, based on BMI, was estimated after stratification based on the age, gender, and geographical area. In addition, the change in the prevalence of obesity/overweight over time from 2011 to 2021 was investigated from the pooled data. The Metaprop program in Stata was used for statistical analysis. Results: A total of 39 studies with 640,952 participants were included in this review. The pooled prevalence of obesity and overweight in the age group of ≤25 years old, including both genders, was 30%. However, it was higher in young males (40%) compared to young females (25%). The prevalence of obesity and overweight among young adults has dropped by over 40% between 2012 and 2021. The overall pooled prevalence rate of obesity and overweight in the age groups >25 years old (adults, mid-life, and old people), including both genders, was 66%, with similar prevalence among males (68%) and females (71%). In addition, a similar prevalence was observed among both adult and old people (62% and 65%, respectively), but was higher in the mid-life group (76%). Furthermore, mid-life women had the highest prevalence among all groups (87%), compared to 77% among males in the same age group. The same difference in prevalence between the gender persisted in older females compared to older males (79% vs. 65%, respectively). There is a noticeable drop in the pooled prevalence of overweight and obesity among adults > 25 years old of over 28% between 2011 and 2021. There was no difference in the prevalence of obesity/overweight by geographical region. Conclusions: Despite the noticeable drop in the prevalence of obesity in the Saudi community, the prevalence of high BMI is high in Saudi Arabia irrespective of age, gender, or geographical location. Mid-life women have the highest prevalence of high BMI, which makes them the focus of a tailored strategy for intervention. Further research is needed to investigate which are the most effective interventions to address obesity in the country.
1. Introduction
Obesity has emerged as a global public health problem. The prevalence of obesity has increased significantly to a pandemic level during the last 50 years [1]. Recent reports showed that over 670 million adults worldwide were obese, in addition to 1.3 billion who were considered overweight in 2016 [1,2].
The prevalence of obesity and overweight in the Middle East was 21% and 33%, respectively, as estimated by a recently published systematic review [3]. Al-Quwaidhi et al. reported that the prevalence of obesity among adults in Saudi Arabia had increased from 22% in 1990 to 36% in 2005. The same study projected that there will be a considerable increase in obesity prevalence both in adult men and women by the year 2022 [4].
Similar to other high-income countries, 83% of the Saudi population lives in cities [5]. Rapid urbanization has had a negative impact on the prevalence of obesity and overweight in the country mainly due to limited physical activity with heavy traffic, and a lack of sport and gymnasium facilities and of sidewalks [6]. Many studies have reported a significant association between overweight and obesity and physical inactivity in Saudi Arabia [7,8,9]. Furthermore, there is a noticeable change in the pattern of diet in the Saudi community, with minimal consumption of fruits, vegetables, and fiber, and a high intake of sugar, saturated fat, and salt [10]. Published studies have demonstrated a significant association between overweight and obesity and unhealthy diet in the Saudi population [9,11,12]. In addition, socioeconomic determinants play a considerable role in the progressive increase in the prevalence of obesity in Saudi Arabia [5]. Apart from genetic predisposition, family size was found to be inversely associated with obesity in Saudi adolescents, along with parents’ level of education and employment [7].
Analysis of the recent Global Burden of Disease 2019 showed that a high BMI is one of the main risk factors for premature mortality and morbidity worldwide, including in the Middle East and Saudi Arabia [13]. High BMI is strongly linked to cardiovascular diseases, a leading cause of morbidity and preterm death both globally and in Saudi Arabia [14,15].
Obesity is a modifiable risk factor, which has the potential to be reversed or prevented. However, the prevalence of overweight and obesity in the Saudi Arabian population remains high, indicating ineffectiveness or lack of preventive measures and interventions [16,17]. Recently, many national programs and interventions have been implemented to reduce the prevalence of high BMI, however, the effectiveness of these programs has yet to be proven [18].
Different sectors of the community will respond to different types of interventions which are tailored according to the demographic characteristics of that group of the population, including gender and age [19,20]. Hence, the main objectives of this scoping review are to estimate the prevalence of obesity and overweight in the Saudi community among different age groups, genders, and geographical locations. This information will contribute to the framing of this health problem in its real perspective, so policy makers can set policies for proper allocation of resources to contain a long-standing and growing health problem.
2. Materials and Methods
2.1. Protocol and Registration
This scoping review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews [21]. The Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines were followed for reporting [22]. The scoping review protocol is registered in The Open Science Framework (OSF) [23].
2.2. This Scoping Review Addresses the following Research Questions
- What is the prevalence rate of overweight and obesity among adults in the Saudi Arabian community in general and among subgroups of the population?
- What is the overall prevalence of obesity and overweight in the Saudi Arabian community?
- What is the distribution of obesity and overweight according to age?
- What is the distribution of obesity and overweight according to gender?
- What is the distribution of obesity and overweight according to geographical regions?
- What is the temporality of obesity and overweight over the last 10 years?
- What are the research gaps in the published literature on the prevalence of obesity and overweight in Saudi Arabia?
2.3. Information Sources and Search
The search strategy aimed to locate published studies. A medical librarian conducted an electronic literature search in six databases—MEDLINE (Ovid), Embase (Ovid), PyscINFO (Ovid), Cochrane CENTRAL (Ovid), Cochrane Database of Systematic Reviews (Ovid), and CINAHL (Ebsco)—from January 2011 till December 2021. A search strategy including all keywords and terms was adapted for each included database (Supplementary Materials). The reference lists of all included articles were screened for additional studies. There was no language limitation. The search keywords were: overweight, obesity, prevalence, incidence, obesity in adults, obesity in adolescence, obesity in pregnancy, obesity in geriatrics, cohort studies, cross sectional studies, systematic review, scoping review, and review.
2.4. Selection of Sources of Evidence
Once the search of the six databases was completed, the medical librarian uploaded the search results into EndNote reference manager and removed the duplicates. Two authors independently conducted title/abstract and full-text article screenings. Reasons for exclusion of articles that did not meet the inclusion criteria were reported. Any discrepancies regarding selection of included articles were reviewed by a third reviewer or resolved by discussion with additional reviewers.
2.5. Eligibility (Inclusion) Criteria
- The population was limited to the Saudi Arabian community including both male and female adults, in addition to a subgroup of participants including pregnant and postpartum women and geriatrics;
- Studies of the adult population (18 years and above). However, studies which included a sample starting from a minimum age of 15 years in which this age group could not be separated from adults were also included in the analysis;
- Populations in the community, educational institutions, or health institutions (e.g., hospital, health center);
- All quantitative observational research designs (descriptive, cohort, cross-sectional, case, and case series) and surveys with the primary objective of quantifying the prevalence of obesity and overweight;
- Obesity and overweight were reported as BMI;
- Published data were collected between January 2011 and December 2021.
2.6. Exclusion Criteria
- Studies on populations with conditions that may not be generalizable to the general population (e.g., chronic kidney disease, cancer);
- Studies on children and adolescents < 15 years old;
- Abstracts, conference proceedings, and grey literature.
2.7. Data Charting Process
Prevalence of obesity and overweight was reported for the total population and each subgroup from the included articles. However, when the age distribution reported in the article differed from the age distribution adopted in this review, re-calculation of the prevalence was performed for each age subgroup. Data was exported from EndNote to Google Sheets. Reviewers manually extracted data using the same sheet. Charting was done independently by two reviewers. Any disagreements between the reviewers were resolved by discussion with other reviewers.
2.8. Data Items
For the included studies, the following information was extracted into Google Sheets: study ID (author, publication year), study design, setting (hospital, school, etc.), geographical region and city, population type (students, workers, etc.), sample size, age range of the population (mean ± SD), and prevalence of obesity and overweight as percentages of the study population and gender.
2.9. Outcome Measures
For the analysis in this review, we combined overweight and obesity as high BMI due to the similar effect as a risk factor for other non-communicable diseases. On the basis of BMI, subjects were classified as either normal weight (<25 kg/m2), overweight (25–29.9 kg/m2), or obese (≥30 kg/m2) [24].
2.10. Data Synthesis
The extracted data was presented in tabular, forest plot, and map forms. In addition, a descriptive summary accompanied the tabulated and charted results to describe how the results relate to the research questions of this scoping review. To answer the research questions, we performed meta-analysis of proportions of overweight and obesity to pool the prevalence among different age groups and genders, trends over time, and across geographical regions. We used Metaprop program in Stata (StataCorp. 2019. Stata Statistical Software: Release 16.1 College Station, TX, USA: StataCorp LLC) that facilitates the pooling of proportions to report a summary of prevalence at different levels. The population of this review was categorized into four age groups: young adults (18–25 years), adults (26–45), mid-life adults (46–60), and old people (60+). Each group was then categorized by gender into males and females. We included studies of adults’ population 18 years and above. Studies which included a population with a minimum age of 15 years in which this age group could not be separated from adults were included in the analysis. In addition, each group of studies from the same geographical region (there are five geographical regions in Saudi Arabia), were analyzed together.
3. Results
The published literature search identified a total of 9293 publications (Figure 1). After removal of duplicates (n = 3135), articles published before 2011 (2004), ineligible articles identified by automation tools (n = 204), and those excluded for other reasons (n = 115), a total of 3781 records remained. Screening by title and abstract led to the exclusion of 3715 records. Full text was sought for 66 records, of which seven could not be retrieved. From the 59 eligible studies, a total of 20 studies were excluded following full-text review. Reasons for exclusion included: the absence of reported prevalence (n = 2) [25,26]; data collected before 2011 (n = 2) [27,28]; the study’s participants being restricted to a specific age group and not being representative of a whole population (n = 1) [29]; the population were children (n = 3) [30,31,32]; population was mixed and data could not be separated for the included population i.e., including Saudis and non-Saudis (n = 3) [33,34,35] or adults and children (n = 1) [36]; and studies with a scope irrelevant to the objectives of this review (n = 4) [37,38,39,40] or presenting findings that have been reported more than once (n = 4) [34,38,41,42]. Finally, 39 studies were included in this review (Figure 1 and Table 1).
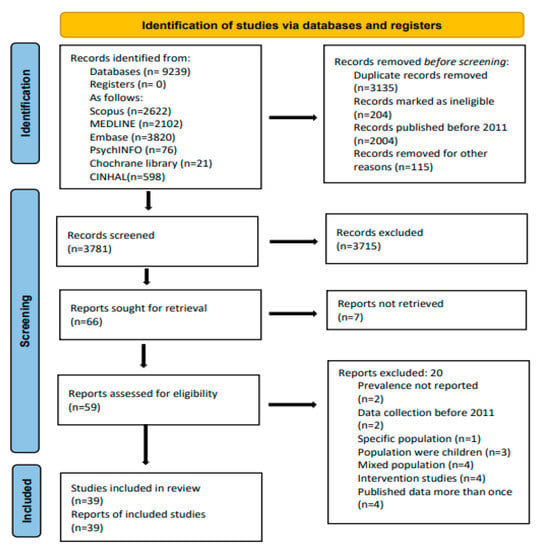
Figure 1.
Prisma Flow Chart.
3.1. Age, Gender, and Temporal Influences on the Prevalence of Obesity and Overweight among Young Adults
The pooled prevalence of obesity and overweight in the age group of ≤25 years old, including both genders, was 30% (Figure 2 and Table 1). However, it was higher among males (40%) compared to young females (25%). Furthermore, there is obvious temporal variation in the prevalence of obesity and overweight among young adults, which dropped from 41% in 2012 to 24% in 2021 (Figure 3).
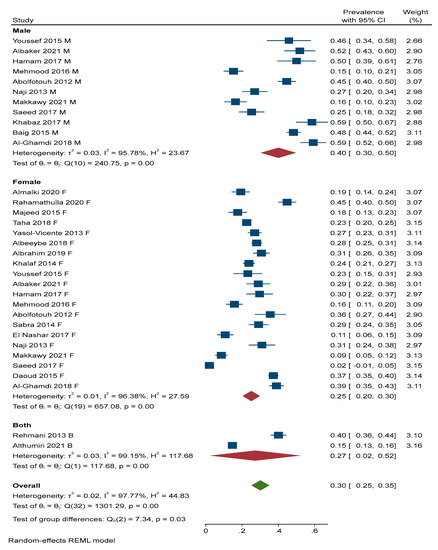
Figure 2.
Prevalence of obesity among young adults by gender. M = Male, F = Female, B = Both (male and female) [41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63].
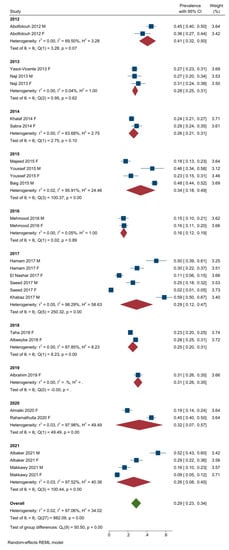
Figure 3.
Prevalence of obesity among young adults by year. M = Male, F = Female, B = Both (male and female) [41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64].
3.2. Age, Gender, and Temporal Influences on the Prevalence of Obesity and Overweight among Adults, Mid-Life, and Old People
The overall pooled prevalence rate of obesity and overweight in the age groups older than 25 years (adults, mid-life, and old people) including both genders was 66%, with nearly similar prevalence among males (68%) and females (71%) (Figure 4 and Table 1). Considering specific age groups, similar rates were observed among both adults and old people (62% and 65%, respectively). However, the pooled prevalence was highest among adults in the mid-life group (76%), showing an increase of nearly 10% from other age categories (Figure 5). Further analysis of the prevalence in this group by gender (Figure 6 and Figure 7 and Table 1) showed that mid-life women had the highest prevalence among all groups (87%), compared to 77% among males in the same age group. The same difference in prevalence between both genders persisted in old females compared to old males (79% vs. 65%, respectively) (Figure 6 and Figure 7). There is a noticeable drop in the pooled prevalence of overweight and obesity among adults aged over 25 years of 28% in the year 2021 compared to that reported in the year 2011 (Figure 8 and Table 1).
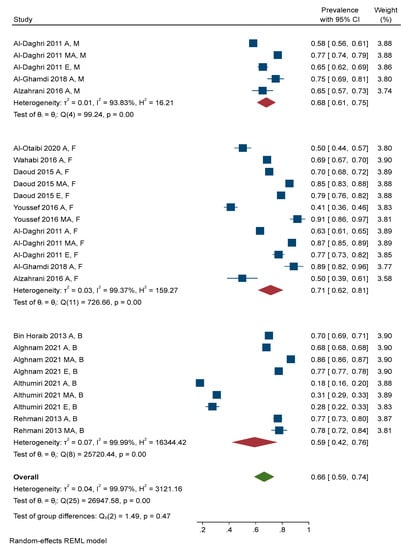
Figure 4.
Prevalence of obesity for all groups, excluding young adults, by gender. A M = Adult males, AF = Adult females, AB = Adult males and females, MA M = middle-aged males, MA F = Middle-aged females, MA B = Middle-aged males and females, EM = Old males, EF = Old females, EB = Old males and females [52,62,63,64,65,66,67,68,69,70,71].
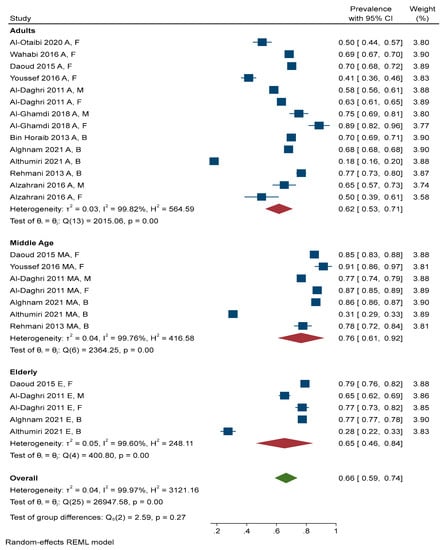
Figure 5.
Prevalence of obesity for all participants excluding young adults by age group. A M = Adult males, AF = Adult females, AB = Adult males and females, MA M = middle-aged males, MA F = Middle-aged females, MA B = Middle-aged males and females, EM = Old males, EF = Old females, EB = Old males and females [52,62,63,64,65,66,67,68,69,70,71].
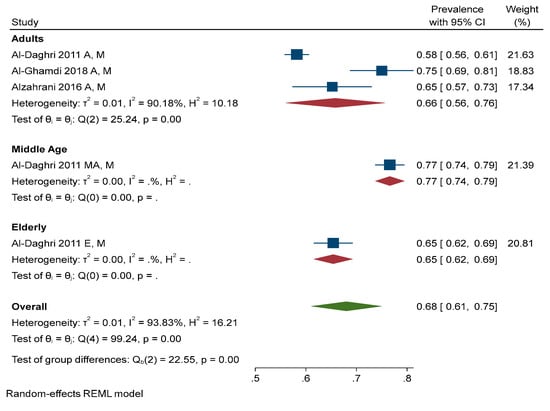
Figure 6.
Prevalence of obesity for all participants excluding young adults by age group among males. AM = Adult males, MA M = Middle-Aged males, EM = Old males [52,65,66].
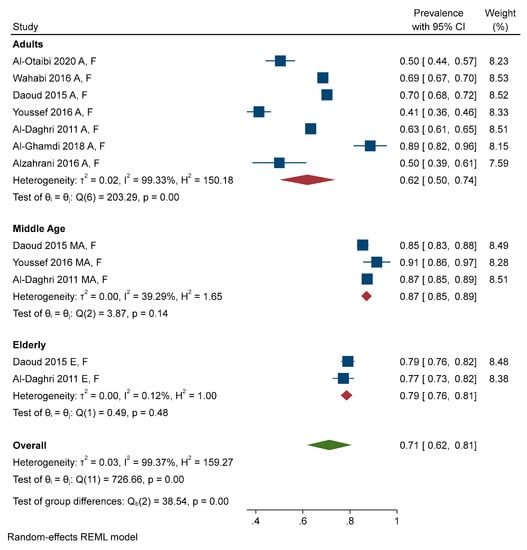
Figure 7.
Prevalence of obesity for all participants excluding young adults by age group among females. AF = Adult females, MA F = Middle-aged females, EF = Old females [52,62,65,66,67,68,69].
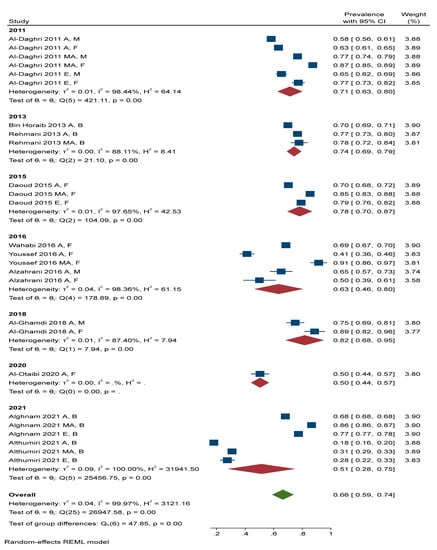
Figure 8.
Prevalence of obesity for all participants excluding young adults by year of publication. A M = Adult males, AF = Adult females, AB = Adult males and females, MA M = middle-aged males, MA F = Middle-aged females, MA B = Middle-aged males and females, EM = Old males, EF = Old females, EB = Old males and females [52,62,63,64,65,66,67,68,69,70,71].
3.3. Prevalence of Obesity and Overweight by Geographic Area
Two studies were excluded from this analysis because the prevalence was reported at the national level and data could not be separated [62,70]. The group differences among the five geographical regions were non-significant (X2 = 2.71, p-value = 0.607). The central region had the highest prevalence (50%), followed by the eastern region (45%), southern region (42%), western region (40%), and northern region (39%) (Figure 9 and Figure 10 and Table 1).
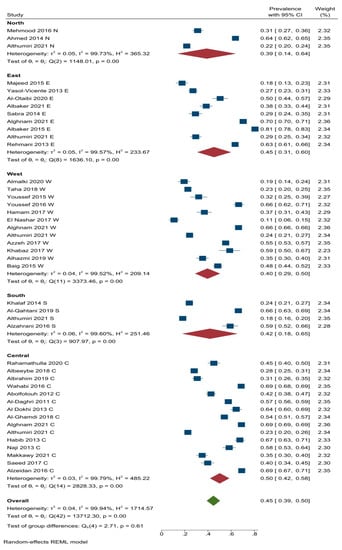
Figure 9.
Prevalence of obesity and overweight by geographic area. N = North, E = East, W = West, S = South, C = Central [41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,63,64,65,66,67,68,69,71,72,73,74,75,76,77,78,79].
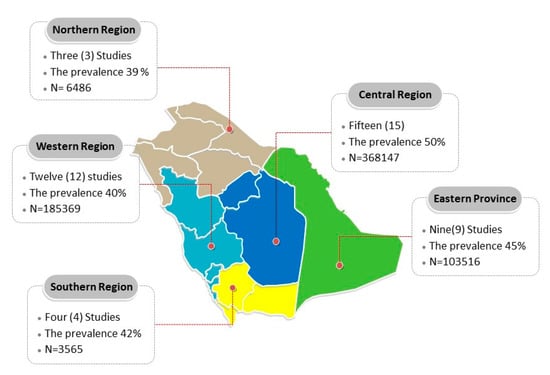
Figure 10.
Prevalence of obesity and overweight across the five geographic areas.

Table 1.
Summary of the Included Studies.
Table 1.
Summary of the Included Studies.
| No | Study ID | Design | Setting | Region/City | Population | Sample Size | Age (Years) Range (Mean ± SD) | Prevalence |
|---|---|---|---|---|---|---|---|---|
| 1 | Almalki 2020 [53] | Cross-sectional | University | Western/Jeddah | Female university students | Total = 232 | 18–27 (20.98 ± 1.48) | Overall (19.3%) |
| 2 | Abolfotouh 2012 [46] | Cross-sectional | University | Central/Riyadh | University students | Total = 501 F = 118 (23.5%) | 18–26 | Overall (42.5%) M (44.7%) F (35.6%) |
| 3 | Ahmed 2014 [72] | Cross-sectional | Primary health care centers | Northern/Hail | General population | Total = 5000 | <25–71+ (43.5 ± 18.7) M (44.6 ± 20.2) F (42.3 ± 16.9) | Overall (63.6%) M (56.2%) F (71%) |
| 4 | Al Dokhi 2013 [73] | Cross-sectional | Population-based | Central | Healthy adults | Total = 411 F = 111 (27%) | 18–72 (36.91 ± 15.22) | Overall (64.2%) M (57.4%) F (71%) |
| 5 | Albaker 2015 [74] | Cross-sectional | University Hospital | Eastern | General population | Total = 711 F = 356 (50.1%) | 18–60 (40 ± 12.9) | Overall (80.5%) |
| 6 | Albaker 2021 [43] | Cross-sectional | University | Eastern/Dammam | University students | Total = 310 F = 183 (59%) | 18.45 ± 0.8 | Overall (38.4%) M (51.9%) F (29%) |
| 7 | Albeeybe 2018 [57] | Cross-sectional | University | Central/Riyadh | Female university students | Total = 907 | (20.9 ± 1.8) | Overall (28.1%) |
| 8 | Albrahim 2019 [58] | Cross-sectional | University | Central/Riyadh | Female university students | Total = 396 | 18–24 (20.1 ± 1.55) | Overall (30.7%) |
| 9 | Al-Daghri 2011 [65] | Cohort study | Primary healthcare centers | Central/Riyadh | General population | Total = 6630 F = 3640 (54.9%) | 18–80 | Overall (57.4%) By age and gender: 18–45 [M (58.2%), F (63.3%)] 46–60 [M (67.6%), F (78.3%)] 61–80 [M (65.4%), F (77.2%)] |
| 10 | Al-Ghamdi 2018 [52] | Cross-sectional | Population-based | Central/Al Kharj | General population | Total = 1019 F = 638 (63%) | 18–67 | Overall (54.3%) By age and gender: 18–29: [M (59%), F (39%)] 30–67: [M (75%), F (89%)] |
| 11 | Alghnam 2021 [71] | Cross-sectional | Population-based | Central, western, and eastern | Patients | Total = 573,698 | 17 years and older | Overall (68.6%) By age: 17–25 (38.5%) 26–45 (68%) 46–64 (86.4%) ≥65 (77.6%) |
| 12 | Alhazmi 2019 [75] | Cross-sectional | University | Western/AL Madinah Al Monawarah | University students | Total = 342 F = 171 (50%) | ≤22 years (64.6%) > 22 years (35.4%) | Overall (35.3%) |
| 13 | Al-Otaibi 2020 [67] | Cross-sectional | Hospital | Eastern/Al-Ahsa | Pregnant women | Total = 238 | 20–40 (29.2 ± 5.1) | Overall (50.4%) |
| 14 | Al-Qahtani 2019 [76] | Cross-sectional | Primary health care centers | Southwestern | Healthy adults | Total = 1238 F = 410 (34%) | Not reported | Overall (66%) |
| 15 | Althumiri 2021 [64] | Cross-sectional | Population-based | National 13 Regions | Healthy adults | Total = 4709 F = 2358 (50.1%) | 18–90 (36.4 ± 13.5) | Overall (24.7%) By age: 18–19 (14.1%) 20–29 (14.8%) 30–39 (18.1%) 40–49 (29.8%) 50–59 (32.8%) 60–(27.6%) |
| 16 | Alzahrani 2016 [66] | Cross-sectional | Hospitals and family medicine centers | Southern/Aseer | Resident physicians | Total = 211 F = 33.2% | ≤25–>30 (27.9 ± 2.6) | Overall (59%) M (65.2%) F (50%) |
| 17 | Alzeidan 2016 [77] | Cross-sectional | University | Central/Riyadh | University employees and families | Total = 3063 F = 1907 (62.3%) | 18–≥60 (38.58 ± 14.09) | Overall (69%) |
| 18 | Azzeh 2017 [78] | Cross-sectional | Population-based | Western/Mecca, Jeddah, and Altaif | Healthy adults | Total = 2548 F = 1125 (44.2%) | Overall 18–60 (29.1 ± 8.5) F (28.3 ± 9.1) M (29.7 ± 8) | Overall (55.1%) M (62.8%) F (45.3%) |
| 19 | Baig 2015 [51] | Cross-sectional | University | Western/Jeddah | Male University Students | Total = 610 | 22.40 ± 3.90 | Overall (48.4%) |
| 20 | Bin Horaib 2013 [70] | Cross-sectional | Population based | Nationwide five regions of KSA (Eastern, northern, southern, western, and central) | Healthy adult (Military personnel) | Total = 10500 | <30–50 (34.12 ± 7.25) | Overall (62.4%) |
| 21 | Daoud 2015 [62] | Cross-sectional | National Households and primary healthcare clinics | All regions (13 health regions) | Adult women | Total = 5482 | 15–≥65 | Overall (61.5%) By age: 15 –24 (37.3%) 25–44 (70%) 45–60 (85%) >60 (79%) |
| 22 | El Nashar 2017 [61] | Cross-sectional | University | Western/AL Madinah Al Monawarah | Female students | Total = 186 | Preparatory university students | Overall (10.7%) |
| 23 | Habib 2013 [79] | Cross-sectional | Population-based | Central | Healthy adults | Total = 530 F = 167 (31.5%) | 18–72 (36.9 ± 15.2) F = 36.7 ± 9.5 M = 38.8 ± 15.6 | Overall (67.4%) |
| 24 | Hamam 2017 [44] | Cross-sectional | University | Western/Taif | University students | Total = 228 F = 148 (64.9%) | 1st–6th years of university | Overall (36.8%) M (50.1%) F (29.7%) |
| 25 | Khabaz 2017 [50] | Cross-sectional | University, | Western/Jeddah | University Students | Total = 116 | 18–26 years | Overall (58.6%) |
| 26 | Khalaf 2014 [59] | Cross-sectional | University | Southwestern | Female university students | Total = 663 | 18–25 (20.4 ± 1.5) | Overall (23.8%) |
| 27 | Majeed 2015 [41] | Cross-sectional | University | Eastern/Dammam | Female university students | Total = 215 | (19.27 ± 0.95) | Overall (17.6%) |
| 28 | Makkawy 2021 [48] | Cross-sectional | University | Central/Riyadh | University Students | Total = 401 F = 267 (66.6%) | (22.2 ± 2.9) | Overall (34.9%) M (16.4%) F (8.6%) |
| 29 | Mehmood 2016 [45] | Cross-sectional | University | Northern/Ar’ar | University students | Total = 405 F = 236 (58.3%) | 19–25 (21.49 ±1.59) | Overall (31.1%) M (15.3%) F (15.8%) |
| 30 | Naji 2013 [47] | Cross-sectional | University | Central/Al-Majmaah | University students | Total = 303 F = 151 (49.8%) | Not reported | Overall (58.1%) M (27%) F (31%) |
| 31 | Rahamathulla 2020 [54] | Cross-sectional | University | Central/Wadi Al Dawaser | Female university students | Total = 374 | (20.6 ± 1.26) | Overall (44.9%) |
| 32 | Rehmani 2013 [63] | Cross-sectional | Population-based | Eastern | Healthy adolescents and adults | Total = 1339 F = 570 (42.6%) | ≥15 (30.7 ± 12.7) | Overall (63.3%) M (67.9%) F (57%) By age categories: 15–24 (40.1%) 25–34 (78.3%) 35–44 (76.7%) 45–54 (80.1%) ≥55 (60.9%) |
| 33 | Sabra 2014 [60] | Cross-sectional | University | Eastern/Dammam | Female university students | Total = 260 | 18–≥22 | Overall = (29.2%) |
| 34 | Saeed 2017 [49] | Cross-sectional | University | Central/Riyadh | University students | Total = 281 | 21.26 ± 1.21 | Overall (39.7%) M (25.3%) F (2.1%) |
| 35 | Taha 2018 [55] | Cross-sectional | University | Western/Taif | Female university students | Total = 1200 | 17–33 Median = 21 | Overall (22.6%) |
| 36 | Wahabi 2016 [68] | Cohort study | Hospitals | Central/Riyadh | Pregnant women and maternity population | Total = 14568 | (29 ± 5.9) | Overall (68.5%) |
| 37 | Yasol-Vicente 2013 [56] | Cross-sectional | University | Eastern/Jubail | Female university students | Total = 514 | Preparatory + Bachelor students | Overall (27%) |
| 38 | Youssef 2015 [42] | Cross-sectional | University | Western/AL-Madina Al-Monawarah | University students | Total = 165 F = 104 (63%) | (20.5 ± 0.1) | Overall (31.9%) M (45.9%) F (23.2%) |
| 39 | Youssef 2016 [69] | Cross-sectional | Population-based | Western/AL-Madina Al-Monawarah | Adult women | Total = 448 | 18–60 | By age categories: 18–39 (41.3%) 40–60 (91.4%) |
M: Male, F: Female.
4. Discussion
The current study investigated the influences of age, gender, temporality, and geographical area on the prevalence of obesity and overweight among Saudi Arabian adults. The findings revealed that the pooled prevalence among adults aged over 25 years was more than double that of young adults (66% vs. 30%). While the pooled prevalence of obesity and overweight was higher in males compared to females in the young adults’ group, it was higher in females than in males in the mid-life and old age groups. In addition, the mid-life group was associated with the highest prevalence rates for both genders, but there was a higher prevalence among females than males in this age group. However, there was a noticeable drop in the prevalence of obesity and overweight among all age groups between the year 2011 and 2021. This study did not show a difference in the prevalence of overweight/obesity between the five geographical areas of the Kingdom.
The pooled prevalence of obesity among young adults in this study was 30%, which is in line with the findings of other studies in both developed and developing countries [80]. Similar trends in the prevalence of overweight and obesity by gender and age have been reported in other countries of the Eastern Mediterranean Region [3,81]. Estimates of the prevalence of obesity and overweight in USA and UK were 22% to 35%, respectively, among the 18–23 years old age group [82,83]. Peltzer et al. investigated the rate of obesity among university students from 22 low- and middle-income countries and reported a similar overall rate of obesity of 22% [84]. In agreement with several studies, mainly from Asia [85,86,87], young adult males showed higher prevalence rates of overweight/obesity compared to females. However, this finding is not consistent all over the world, as reported by other investigators [84].
Several factors may contribute to such gender differences in this age group. Taking into consideration that the majority of young adults are university students, as well as the conservative culture in Saudi Arabia, males are more likely than females to live away from their families to pursue their undergraduate study in different universities, which renders them more likely to gain weight by depending mainly on fast food and soft drinks for their diet [88,89].
Another explanation comes from gender discrepancy of body image perception. Several studies have found that males underestimate their weights compared to females, and that overweight/obese males perceive being overweight to be the ideal body image, whereas females perceive a normal weight to be the ideal body image [90,91]. This may lead young men to gain weight in order to reach their ‘ideal’ buff image, while young women will desire to lose weight and maintain a thin body image [80].
Similar to other reports in the literature, this study showed an increase in the prevalence of overweight/obesity with age [92]. Changes in lifestyle which have already started during young adulthood, such as increased consumption of fast food, skipping breakfast, and snacking, all increase the risk of being overweight/obese later during adult and mid-life [93,94,95]. In addition, the shift from active to sedentary lifestyles inside and outside the workplace, the lack of time to practice physical activity due to work or social and family responsibilities, together with decreased metabolism with age all contribute to less activity and more obesity.
Females in adult and mid-life age experience more physiological changes due to pregnancy and childbearing, which, along with the above-mentioned factors, makes women in their reproductive age more obese than men in the same age groups. Alotibi et al. examined the pre-pregnancy weight of nulliparous women and found that the prevalence of obesity in this group of women was only 14.7% compared to 64% in women who had two or more children [67]. Wahabi et al. 2019 investigated postpartum weight retention in Saudi Arabian women and showed that 35% of the investigated population had ≥7 kg of extra weight retained one year following delivery [96].
Moreover, although more than 40% of Saudi Arabian women are university graduates, they have higher unemployment rates at 80–86% [67,68], which contributes to physical inactivity following completion of their education [77]. These factors can explain the dominance of obesity in females during the adult, mid-life, and old age stages compared to males in the current study.
We were rather surprised by the decreased prevalence of overweight/obesity we observed in this study between the years 2011 and 2021. Studies that link the reduction of the prevalence of obesity and overweight in Saudi Arabia to certain interventions on a national scale, are scarce [64]. Nevertheless, many new regulations that promote a healthier lifestyle have been introduced to Saudi Arabia on a national level, which may have contributed to the current reduction in obesity/overweight found in this study. Example of these changes include new regulations that allowed female fitness centers to open in the country, and physical activity classes in female schools which were introduced in 2017 [97,98]. Furthermore, as part of the Vision 2030 plan, the government initiated quality of life programs and resources to encourage community participation in exercise as well as healthy lifestyles [99]. The introduction of legislation requiring printing a meal’s calories on restaurant menus at the beginning of 2019, with the intention to increase awareness of the importance of the amount of calories each type of food contains in the Saudi Arabian community, is another pertinent intervention [100]. Excise taxes of 50% and 100% were introduced on sugar-sweetened and carbonated drinks and energy drinks, respectively, in early 2019 [101].
The increase in the treatment of obesity, including bariatric surgery, may have increased the awareness of the community at large about obesity as a chronic disease and a risk factor for other chronic diseases, especially with coverage by press and social media [102,103].
In this study there was no significant difference in the pooled prevalence of obesity/overweight between the regions of Saudi Arabia, and an overall prevalence of 45%. This may be due to the balanced distribution of health care and social facilities in the Kingdom. However, most of the studies in this review were conducted in urban cities, rather than in rural areas, which share the same standard of living, lifestyle and availability of restaurants that provide fast food and high-calorie drinks. In addition, the new large geographical regions we used in this study may have obscured the small variations in prevalence of obesity/overweight that were noticed in other studies using smaller geographical regions [10].
One of the many programs and interventions the Kingdom has initiated to address the problem of obesity among the different sectors of the community was the approval of national clinical practice guidelines for the management of overweight and obesity, which were published in 2016 [64,104]. However, the ACTION International Observation Study (ACTION-IO), which included healthcare professionals and individuals with obesity from many countries around the world, including Saudi Arabia, found several barriers to effective obesity healthcare, which needs a set of tailored interventions, such as education and training [18,105]. Many of the barriers identified in the ACTION-IO study were related to a lack of communication and trust between healthcare providers and people living with obesity, which delayed timely effective interventions [18]. In addition, the study documented many misconceptions among both groups, including that people with obesity believe they should accept complete responsibility for their own weight loss, and that fewer than 50% of healthcare providers believed genetics were barriers to obesity management [18].
4.1. Implications for Research (Research Gaps) and Practice
In line with the national promotion of public health and preventive medicine in Saudi Arabia, more studies are required to further explore the epidemiology and determinants of overweight and obesity and propose strategies to address the challenges and barriers for obesity prevention and management [106].
Future epidemiological studies should stratify epidemiological findings based on gender and age to tailor effective intervention for each group of the population based on their characteristics and specific platforms for communication. Such stratification will help in the detection of the group mostly in need of interventions (e.g., women at reproductive age, postpartum women).
Further studies are needed to explore the viewpoints of the Saudi Arabian community at large and the individuals living with obesity regarding the social, economic, and medical aspects of overweight/obesity. Such information will facilitate designing and implementing effective educational programs pertaining to obesity prevention and management with partnership between the community and healthcare providers [104,107].
Obesity varies with socioeconomic, ethnic, and other factors, and the findings of this review indicate the need for studies to assess whether obesity prevalence has a different distribution at a smaller geographic level than the regional level, for instance, between urban and rural areas. Such knowledge will advise better allocation of resources and targeted interventions [108].
Social media and the press should be employed to increase the awareness of the community about obesity as a chronic disease and as a risk factor for other disease, and channels for seeking medical attention and advice should be established and made available and easily accessible [109].
All the implemented and the proposed programs for obesity in Saudi Arabia should include surveillance systems and evaluation plans to monitor the progress of effective interventions and facilitate audits for maximum cost-effectiveness [104].
Similar to other medical conditions and chronic diseases, individuals with obesity should be the center of care [110].
Undergraduate and graduate medical curricula should include updated and evidence-based information on the epidemiology, etiology, risk factors, management, and prevention of obesity at the individual and national levels [111].
4.2. Strength and Limitation of this Study
This review is the first report to provide data on the prevalence of obesity by age and gender and geographical region in Saudi Arabia. It provides valuable information on specific sectors of the populations to be targeted with tailored effective interventions [20,112]. Despite implementing several promising policies in Saudi Arabia, it is not yet clear how and to what extent they have impacted each group of the population [113]. This scoping review is the first step in planning age-and-gender-specific strategies.
However, the results of this review should be approached with caution due to the high heterogeneity associated with pooling the data. This may be due to differences in the study designs, but performance bias cannot be excluded, especially considering that we did not conduct critical appraisal for any of the included studies.
5. Conclusions
Despite the noticeable drop in the prevalence of obesity in the Saudi community the prevalence of high BMI is high in Saudi Arabia irrespective of age, gender, or geographical location. Mid-life women have the highest prevalence of high BMI, which should make them the focus of a tailored strategy for intervention. Further research is needed to investigate which are the most effective interventions to address obesity in the country.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare11081143/s1, Table S1: Search strategies title.
Author Contributions
Conceptualization: H.W. and A.A.F., Data curation: H.W., S.E., M.T., Y.A., R.A., E.S., K.B., Z.S. and L.H.; Formal analysis: H.W., A.A.F., S.E., M.T., Y.A., R.A., E.S., K.B. and Z.S.; Methodology: H.W., A.A.F., S.E., M.T., Y.A., R.A., E.S., K.B. and Z.S.; Project administration: H.W., S.E. and E.S.; Resources: L.H., Y.A. and S.E. Software: A.A.F., Y.A., R.A., E.S., K.B., Z.S. and L.H.; Writing—original draft: H.W., A.A.F., S.E., M.T., Y.A., R.A., E.S., K.B. and Z.S.; Writing—review and editing: H.W., A.A.F., S.E., M.T., Y.A., R.A., E.S., K.B. and Z.S. All authors have read and agreed to the published version of the manuscript.
Funding
This project was funded by Princess Nourah bint Abdulrahman university researchers supporting project (number PNURSP2022R21) Princess Nourah bint Abdulrahman university, Riyadh, Saudi Arabia.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All relevant data are within the manuscript and its supporting information files.
Conflicts of Interest
The authors have declared that no competing interest exist.
References
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Okati-Aliabad, H.; Ansari-Moghaddam, A.; Kargar, S.; Jabbari, N. Prevalence of Obesity and Overweight among Adults in the Middle East Countries from 2000 to 2020: A Systematic Review and Meta-Analysis. J. Obes. 2022, 2022, 8074837. [Google Scholar] [CrossRef] [PubMed]
- Al Quwaidhi, A.; Pearce, M.; Critchley, J.; Sobngwi, E.; O’Flaherty, M. Trends and future projections of the prevalence of adult obesity in Saudi Arabia, 1992–2022. East. Mediterr. Health J. 2014, 20, 589–595. [Google Scholar] [CrossRef]
- Habbab, R.M.; Bhutta, Z.A. Prevalence and social determinants of overweight and obesity in adolescents in Saudi Arabia: A systematic review. Clin. Obes. 2020, 10, e12400. [Google Scholar] [CrossRef]
- Sobal, J. Commentary: Globalization and the epidemiology of obesity. Int. J. Epidemiol. 2001, 30, 1136–1137. [Google Scholar] [CrossRef]
- Alazzeh, A.Y.; AlShammari, E.M.; Smadi, M.M.; Azzeh, F.S.; AlShammari, B.T.; Epuru, S.; Banu, S.; Bano, R.; Sulaiman, S.; Alcantara, J.C.; et al. Some Socioeconomic Factors and Lifestyle Habits Influencing the Prevalence of Obesity among Adolescent Male Students in the Hail Region of Saudi Arabia. Children 2018, 5, 39. [Google Scholar] [CrossRef]
- Adaili, M.; Mohamed, A.; Alkhashan, H. Association of overweight and obesity with decline in academic performance among female high-school students, Riyadh, Saudi Arabia. East. Mediterr. Health J. 2016, 22, 887–893. [Google Scholar] [CrossRef]
- Koura, H.M.; A Alenazi, S.; Zaki, S.; Mohamed, A.H. Prevalence of obesity among male adolescents in Arar Saudi Arabia: Future risk of cardiovascular disease. Indian J. Community Med. 2015, 40, 182–187. [Google Scholar] [CrossRef]
- I Al-Othaimeen, A.; Al-Nozha, M.; Osman, A.K. Obesity: An emerging problem in Saudi Arabia. Analysis of data from the National Nutrition Survey. East. Mediterr. Health J. 2007, 13, 441–448. [Google Scholar]
- Al-Hazzaa, H.M.; A Abahussain, N.; I Al-Sobayel, H.; Qahwaji, D.M.; O Musaiger, A. Lifestyle factors associated with overweight and obesity among Saudi adolescents. BMC Public Health 2012, 12, 354. [Google Scholar] [CrossRef]
- Al Dahi, S.K.; Rofayda, M.A.; Eman, G.Y.; Rami, M.A.; Sanna, H.E.; Malak, M.E.; Fatma, A.A. Adolescents’ overweight and obesity among Alabnaa schools in Tabuk, Saudi Arabia. Saudi J. Obes. 2017, 5, 3. [Google Scholar]
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Khalil, C.A.; Sulaiman, K.; Singh, R.; Jayyousi, A.; Asaad, N.; AlHabib, K.F.; Alsheikh-Ali, A.; Al-Jarallah, M.; Bulbanat, B.; AlMahmeed, W.; et al. BMI is inversely correlated to the risk of mortality in patients with type 2 diabetes hospitalized for acute heart failure: Findings from the Gulf aCute heArt failuRE (Gulf-CARE) registry. Int. J. Cardiol. 2017, 241, 262–269. [Google Scholar] [CrossRef]
- Al-Raddadi, R.; Bahijri, S.M.; Jambi, H.A.; Ferns, G.; Tuomilehto, J. The prevalence of obesity and overweight, associated demographic and lifestyle factors, and health status in the adult population of Jeddah, Saudi Arabia. Ther. Adv. Chronic Dis. 2019, 10, 2040622319878997. [Google Scholar] [CrossRef]
- Hazazi, A.; Wilson, A. Noncommunicable diseases and health system responses in Saudi Arabia: Focus on policies and strategies. A qualitative study. Health Res. Policy Syst. 2022, 20, 63. [Google Scholar] [CrossRef]
- Caterson, I.D.; Alfadda, A.A.; Auerbach, P.; Coutinho, W.; Cuevas, A.; Dicker, D.; Hughes, C.; Iwabu, M.; Kang, J.H.; Nawar, R. Gaps to bridge: Misalignment between perception, reality and actions in obesity. Diabetes Obes. Metab. 2019, 21, 1914–1924. [Google Scholar] [CrossRef]
- Taylor, J.; Walsh, S.; Kwok, W.; Pinheiro, M.B.; De Oliveira, J.S.; Hassett, L.; Bauman, A.; Bull, F.; Tiedemann, A.; Sherrington, C. A scoping review of physical activity interventions for older adults. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 82. [Google Scholar] [CrossRef]
- Lozano-Chacon, B.; Suarez-Lledo, V.; Alvarez-Galvez, J. Use and Effectiveness of Social-Media-Delivered Weight Loss Interventions among Teenagers and Young Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8493. [Google Scholar] [CrossRef]
- Peters, M.; Godfrey, C.; McInerney, P. JBI Manual for Evidence Synthesis Chapter 11: Scoping Reviews. 2020. Available online: https://jbi-global-wiki.refined.site/space/MANUAL/4687342/Chapter+11%3A+Scoping+reviews (accessed on 16 October 2022).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Wahabi, H.A.; Fayed, A.; Shata, N.Z.; Esmaeil, S.; Alzeidan, R.; Saeed, E.; Amer, Y.S.; Titi, M.A.; Bahkali, K.; Hneiny, H.; et al. The Impact of Age, Gender, Temporality and Geographical Region on the Prevalence of Obesity in Saudi Arabia: The Scope of Evidence. Available online: https://osf.io/yuef2/#! (accessed on 16 October 2022).
- WHO. Global Database on Body Mass Index: BMI Classification. Available online: http://www.assessmentpsychology.com/icbmi.htm (accessed on 20 November 2022).
- Al-Hanawi, M.K.; Chirwa, G.C.; Kamninga, T.M. Decomposition of Gender Differences in Body Mass Index in Saudi Arabia using Unconditional Quantile Regression: Analysis of National-Level Survey Data. Int. J. Environ. Res. Public Health 2020, 17, 2330. [Google Scholar] [CrossRef] [PubMed]
- Aldossari, K. Prevalence and determinants of overweight/obesity among the medical students. In Proceedings of the Obesity Surgery, Riyadh, Saudi Arabia; August 2015; p. 1330. [Google Scholar]
- Warsy, A.; El-Hazmi, M.; Al-Hazmi³, A. Prevalence of Co-existing Hypertension and Obesity in Saudis. Biomed. Pharmacol. J. 2015, 4, 269–274. [Google Scholar] [CrossRef]
- Garawi, F.; Ploubidis, G.B.; Devries, K.; Al-Hamdan, N.; Uauy, R. Do routinely measured risk factors for obesity explain the sex gap in its prevalence? Observations from Saudi Arabia. BMC Public Health 2015, 15, 254. [Google Scholar] [CrossRef] [PubMed]
- Albakr, R.B.; Saad, H.A.; Pharaon, M.G.; Nasse, A. Association of Abdominal Adiposity with Diabetes and Cardiovascular Diseases in Adult Saudi. Exp. Clin. Cardiol. 2014, 20, 3745–3760. [Google Scholar]
- Al-Mohaimeed, A.; Ahmed, S.; Dandash, K.; Ismail, M.S.; Saquib, N. Concordance of obesity classification between body mass index and percent body fat among school children in Saudi Arabia. BMC Pediatr. 2015, 15, 16. [Google Scholar] [CrossRef]
- Alsaleem, M.A. Depression, Anxiety, Stress, and Obesity among Male Adolescents at Abha City, Southwestern Saudi Arabia. J. Genet. Psychol. 2021, 182, 488–494. [Google Scholar] [CrossRef]
- Al-Hazzaa, H.M.; Abahussain, N.A.; Al-Sobayel, H.I.; Qahwaji, D.M.; Alsulaiman, N.A.; Musaiger, A.O. Prevalence of Overweight, Obesity, and Abdominal Obesity among Urban Saudi Adolescents: Gender and Regional Variations. J. Health Popul. Nutr. 2014, 32, 634–645. [Google Scholar]
- Amin, T.T.; Al Sultan, A.I.; Mostafa, O.A.; Darwish, A.A.; Al-Naboli, M.R. Profile of Non-Communicable Disease Risk Factors Among Employees at a Saudi University. Asian Pac. J. Cancer Prev. 2014, 15, 7897–7907. [Google Scholar] [CrossRef]
- Shereen, M.; Al-Maflehi, N.; Al Husaini, N.; Al Selga, R.; Jaber, T.A. Preference of food intake among dental students in relation to exercise and body mass index: A cross-sectional study. Int. Food Res. J. 2014, 21, 685–691. [Google Scholar]
- Mosli, H.H.; Kutbi, H.A.; Alhasan, A.H.; Mosli, R.H. Understanding the Interrelationship between Education, Income, and Obesity among Adults in Saudi Arabia. Obes. Facts 2020, 13, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; El Bcheraoui, C.; Tuffaha, M.; Robinson, M.; Daoud, F.; Jaber, S.; Mikhitarian, S.; Al Saeedi, M.; AlMazroa, M.A.; Mokdad, A.H.; et al. Obesity and Associated Factors—Kingdom of Saudi Arabia, 2013. Prev. Chronic Dis. 2014, 11, E174. [Google Scholar] [CrossRef] [PubMed]
- Al-Otaibi, H.H. Measuring Stages of Change, Perceived Barriers and Self efficacy for Physical Activity in Saudi Arabia. Asian Pac. J. Cancer Prev. 2013, 14, 1009–1016. [Google Scholar] [CrossRef]
- Alruwaili, M.; Hamad, I.; Selim, S. Distribution of Obesity among Male in Aljouf Population, Saudi Arabia. J. Pure Appl. Microbiol. 2015, 9, 617–622. [Google Scholar]
- Alqahtani, B.A. Association between Physical Frailty and Sleep Quality among Saudi Older Adults: A Community-Based, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12741. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, A.; Berggren, V.; Al-Hazzaa, H.; Bergström, S.; Westergren, A. Undernutrition risk, overweight/obesity, and nutritional care in relation to undernutrition risk among inpatients in southwestern Saudi Arabia: A hospital-based point prevalence study. J. Nutr. Disord. Ther. 2011, 1, 104. [Google Scholar] [CrossRef]
- Majeed, F. Association of BMI with diet and physical activity of female medical students at the University of Dammam, Kingdom of Saudi Arabia. J. Taibah Univ. Med. Sci. 2015, 10, 188–196. [Google Scholar] [CrossRef]
- Youssef, M.H.; Mojaddidi, M.; El Bab, M.F.; El Nabi, W.; Salem, M. Gender differences in body composition, respiratory functions, life style among medical students. Biomed. Res. 2015, 26, 567–574. [Google Scholar]
- Albaker, W.; El-Ashker, S.; Baraka, M.A.; El-Tanahi, N.; Ahsan, M.; Al-Hariri, M. Adiposity and cardiometabolic risk assessment among university students in Saudi Arabia. Science Progress. 2021, 104, 0036850421998532. [Google Scholar] [CrossRef]
- Hamam, F.A.; Eldalo, A.; Alnofeie, A.A.; Alghamdi, W.Y.; Almutairi, S.S.; Badyan, F.S. The association of eating habits and lifestyle with overweight and obesity among health sciences students in Taif University, KSA. J. Taibah Univ. Med. Sci. 2017, 12, 249–260. [Google Scholar] [CrossRef]
- Mehmood, Y.; Al-Swailmi, F.K.; Al-Enazi, S.A. Frequency of obesity and comorbidities in medical students. Pak. J. Med. Sci. 2016, 32, 1528–1532. [Google Scholar] [CrossRef] [PubMed]
- Abolfotouh, M.A.; Al-Alwan, I.A.; Al-Rowaily, M.A. Prevalence of Metabolic Abnormalities and Association with Obesity among Saudi College Students. Int. J. Hypertens. 2012, 2012, 819726. [Google Scholar] [CrossRef] [PubMed]
- Naji, E.; Kashoo, F.Z.; Kashoo, M. Prevalence of Obesity and Overweight among Majmaah University Students. Indian J. Physiother. Occup. Ther. Int. J. 2013, 7, 41. [Google Scholar] [CrossRef]
- Makkawy, E.; Alrakha, A.M.; Al-Mubarak, A.F.; Alotaibi, H.T.; Alotaibi, N.T.; A Alasmari, A.; Altamimi, T. Prevalence of overweight and obesity and their associated factors among health sciences college students, Saudi Arabia. J. Fam. Med. Prim. Care 2021, 10, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Saeed, E.; Assiri, A.M.; AwadEljack, I.; AlJasser, A.S.; Alhuzimi, A.M.; Assiri, A.A.; Alqahtani, N.A.; Alshahrani, S.A.; A Al-Ammar, Y. Obesity and associated risk factors among students of health colleges of King Saud University, Saudi Arabia: A cross-sectional study. J. Pak. Med. Assoc. 2017, 67, 355–359. [Google Scholar] [PubMed]
- Khabaz, M.N.; Bakarman, M.A.; Baig, M.; Ghabrah, T.M.; Gari, M.A.; Butt, N.S.; Alghanmi, F.; Balubaid, A.; Alzahrani, A.; Hamouh, S. Dietary habits, lifestyle pattern and obesity among young Saudi university students. J. Pak. Med. Assoc. 2017, 67, 1541–1546. [Google Scholar]
- Baig, M.; Gazzaz, Z.J.; A Gari, M.; Al-Attallah, H.G.; Al-Jedaani, K.S.; Mesawa, A.T.; A Al-Hazmi, A. Prevalence of obesity and hypertension among University students’ and their knowledge and attitude towards risk factors of Cardiovascular Disease (CVD) in Jeddah, Saudi Arabia. Pak. J. Med. Sci. 2015, 31, 816. [Google Scholar] [CrossRef]
- Al-Ghamdi, S.; Shubair, M.M.; Aldiab, A.; Al-Zahrani, J.M.; Aldossari, K.K.; Househ, M.; Nooruddin, S.; Razzak, H.A.; El-Metwally, A. Prevalence of overweight and obesity based on the body mass index; a cross-sectional study in Alkharj, Saudi Arabia. Lipids Health Dis. 2018, 17, 1–8. [Google Scholar] [CrossRef]
- Almalki, A.H.; Saad, M.S.; Alzahrani, S.S.; A Moalim, M.; Nahdi, S.O.; Sonbol, H.S.; Sunbol, A.H. Association Study between Different Anthropometric Measures and other Clinical Markers in Saudi Female Students at King Abdulaziz University. Am. J. Biochem. Biotechnol. 2020, 16, 32–39. [Google Scholar] [CrossRef]
- Rahamathulla, M.P.; Sha M, M. Frequency and Awareness of Risk Factors of Non-Communicable Diseases among University Students in Saudi Arabia. Pak. J. Med. Sci. 2020, 36, 740–745. [Google Scholar] [CrossRef]
- Taha, A.A.A.E.-A.; Abu-Zaid, H.A.; Desouky, D.E.-S. Eating Disorders Among Female Students of Taif University, Saudi Arabia. Arch. Iran. Med. 2018, 21, 111–117. [Google Scholar]
- Yasol-Vicente, J.L. Prevalence of overweight and obesity among the constituents of Jubail University College-Female Branch. J. Phys. Educ. Sport 2013, 13, 409. [Google Scholar]
- Albeeybe, J.; Alomer, A.; AlAhmari, T.; Asiri, N.; Alajaji, R.; Almassoud, R.; Al-Hazzaa, H.M. Body Size Misperception and Overweight or Obesity among Saudi College-Aged Females. J. Obes. 2018, 2018, 5246915. [Google Scholar] [CrossRef] [PubMed]
- Albrahim, T.; Alrubaish, A.A.; Alfadhliah, J.T.S.; Alaskar, M.K.; Alatawi, M.A.; Aldekhayyil, S.A. The Spectrum of Disordered Eating Attitudes Among Female University Students: A Cross-Sectional Study. Curr. Res. Nutr. Food Sci. J. 2019, 7, 698–707. [Google Scholar] [CrossRef]
- Khalaf, A.; Westergren, A.; Berggren, V.; Ekblom, Ö.; Al-Hazzaa, H.M. Prevalence and association of female weight status and dietary habits with sociodemographic factors: A cross-sectional study in Saudi Arabia. Public Health Nutr. 2015, 18, 784–796. [Google Scholar] [CrossRef]
- Sabra, A. Obesity among female intermediate nursing students of health science collage in Dammam city, Saudi Arabia: Prevalence and associated factors. Can. J. Clin. Nutr. 2014, 2, 29–45. [Google Scholar] [CrossRef]
- El Nashar, D.E.; Alananbeh, K.M.; Al Hassan, N. Genetic, dietary, and non-dietary risk factors of obesity among preparatory-year female students at Taibah University, Saudi Arabia. J. Taibah Univ. Sci. 2017, 11, 408–421. [Google Scholar] [CrossRef]
- Daoud, F.; El Bcheraoui, C.; Tuffaha, M.; AlMazroa, M.A.; Al Saeedi, M.; Nooh, R.M.; Al Rayess, Z.; Al-Raddadi, R.M.; Memish, Z.A.; Basulaiman, M.; et al. The health status of Saudi women: Findings from a national survey. J. Public Health 2016, 38, 660–672. [Google Scholar] [CrossRef]
- Rehmani, R.; Elzubair, A.; Al Maani, M.; Chaudary, I.; Al Qarni, A.; Khasshogi, T.; Al Shuaibi, A. Population-based health survey in eastern region of Saudi Arabia. East. Mediterr. Health J. 2013, 19, 417–425. [Google Scholar] [CrossRef]
- Althumiri, N.A.; Basyouni, M.H.; AlMousa, N.; AlJuwaysim, M.F.; Almubark, R.A.; BinDhim, N.F.; Alkhamaali, Z.; Alqahtani, S.A. Obesity in Saudi Arabia in 2020: Prevalence, Distribution, and Its Current Association with Various Health Conditions. Healthcare 2021, 9, 311. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.S.; Alkharfy, K.M.; Yousef, M.; Sabico, S.L.; Chrousos, G.P. Diabetes mellitus type 2 and other chronic non-communicable diseases in the central region, Saudi Arabia (riyadh cohort 2): A decade of an epidemic. BMC Med. 2011, 9, 76. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, A.A.; Al-Khaldi, Y.M.; Alsamghan, A.S. Prevalence of obesity among Saudi board residents in Aseer Region, Saudi Arabia. Saudi J. Obes. 2016, 4, 13. [Google Scholar] [CrossRef]
- Al-Otaibi, H.; Hussein, N.; Mustafa, H.; Al-Mudaires, N. Obesity, gestational weight gain, and polyunsaturated fatty acids profile in pregnant Saudi women. Bioinformation 2020, 16, 493. [Google Scholar] [CrossRef] [PubMed]
- Wahabi, H.; Fayed, A.; Esmaeil, S.; Alzeidan, R.; Elawad, M.; Tabassum, R.; Hansoti, S.; Magzoup, M.E.; Al-Kadri, H.; Elsherif, E. Riyadh mother and baby multicenter cohort study: The cohort profile. PLoS ONE 2016, 11, e0150297. [Google Scholar]
- Youssef, M.H.; Hifnawy, T.H.; Tarhony, S.; El Fadhly, E. The Relationship Between Age, BMI, Fat Percentage and Body Composition Among Women in Al Madina, Saudi Arabia. Atheroscler. Suppl. 2018, 32, 68. [Google Scholar] [CrossRef]
- Bin Horaib, G.; I Al-Khashan, H.; Mishriky, A.; A Selim, M.; Alnowaiser, N.; A BinSaeed, A.; Alawad, A.D.; Al-Asmari, A.K.; Alqumaizi, K. Prevalence of obesity among military personnel in Saudi Arabia and associated risk factors. Saudi Med. J. 2013, 34, 401–407. [Google Scholar] [PubMed]
- Alghnam, S.; Alessy, S.A.; Bosaad, M.; Alzahrani, S.; Al Alwan, I.I.; Alqarni, A.; Alshammari, R.; Al Dubayee, M.; Alfadhel, M. The Association between Obesity and Chronic Conditions: Results from a Large Electronic Health Records System in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 12361. [Google Scholar] [CrossRef]
- Ahmed, H.G.; Ginawi, I.A.; Elasbali, A.M.; Ashankyty, I.M.; Al-Hazimi, A.M. Prevalence of Obesity in Hail Region, KSA: In a Comprehensive Survey. J. Obes. 2014, 2014, 961861. [Google Scholar] [CrossRef]
- Al Dokhi, L.; Habib, S.S. Assessment of gender differences in body composition and physical fitness scoring in Saudi adults by bioelectrical impedance analysis. Acta Clin. Croat. 2013, 52, 189–194. [Google Scholar]
- Albaker, W.I. Assessment of Body Mass Index versus Body Fat Percentage in Detecting Obesity and Related Comorbidity. Bahrain Med. Bull. 2015, 158, 1–4. [Google Scholar] [CrossRef]
- Alhazmi, A.H.; Al Johani, A. Prevalence and associated factors of eating disorders among students in Taiba University, Saudi Arabia: A cross-sectional study. Malays. J. Public Health Med. 2019, 19, 172–176. [Google Scholar] [CrossRef]
- Al-Qahtani, A.M. Prevalence and predictors of obesity and overweight among adults visiting primary care settings in the southwestern region, Saudi Arabia. BioMed Res. Int. 2020, 2020, 3796923. [Google Scholar] [CrossRef] [PubMed]
- Alzeidan, R.; Rabiee, F.; Mandil, A.; Hersi, A.; Fayed, A. Non-Communicable Disease Risk Factors among Employees and Their Families of a Saudi University: An Epidemiological Study. PLoS ONE 2016, 11, e0165036. [Google Scholar] [CrossRef]
- Azzeh, F.S.; Bukhari, H.M.; Header, E.A.; Ghabashi, M.A.; Al-Mashi, S.S.; Noorwali, N.M. Trends in overweight or obesity and other anthropometric indices in adults aged 18–60 years in western Saudi Arabia. Ann. Saudi Med. 2017, 37, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Habib, S.S. Body mass index and body fat percentage in assessment of obesity prevalence in saudi adults. Biomed. Environ. Sci. 2013, 26, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Poobalan, A.; Aucott, L. Obesity Among Young Adults in Developing Countries: A Systematic Overview. Curr. Obes. Rep. 2016, 5, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef]
- Mirmiran, P.; Mirbolooki, M.; Azizi, F. Familial clustering of obesity and the role of nutrition: Tehran Lipid and Glucose Study. Int. J. Obes. 2002, 26, 1617–1622. [Google Scholar] [CrossRef]
- Lowry, R.; Galuska, D.A.; Fulton, J.E.; Wechsler, H.; Kann, L.; Collins, J.L. Physical activity, food choice, and weight management goals and practices among US college students. Am. J. Prev. Med. 2000, 18, 18–27. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S.; Samuels, T.A.; Özcan, N.K.; Mantilla, C.; Rahamefy, O.H.; Wong, M.L.; Gasparishvili, A. Prevalence of Overweight/Obesity and Its Associated Factors among University Students from 22 Countries. Int. J. Environ. Res. Public Health 2014, 11, 7425–7441. [Google Scholar] [CrossRef]
- Boo, N.Y.; Chia, G.J.Q.; Wong, L.C.; Chew, R.M.; Chong, W.; Loo, R.C.N. The prevalence of obesity among clinical students in a Malaysian medical school. Singap. Med. J. 2010, 51, 126. [Google Scholar]
- Banwell, C.; Lim, L.; Seubsman, S.A.; Bain, C.; Dixon, J.; Sleigh, A. Body mass index and health-related behaviours in a national cohort of 87 134 Thai open university students. J. Epidemiol. Community Health 2009, 63, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Zárate, M.; Becerra-Bulla, F.; Prieto-Suárez, E. Anthropometric evaluation of university students in Bogotá, Colombia. Rev. De Salud Pública 2008, 10, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Butler, S.M.; Black, D.R.; Blue, C.L.; Gretebeck, R.J. Change in Diet, Physical Activity, and Body Weight in Female College Freshman. Am. J. Health Behav. 2004, 28, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Pengpid, S.; Peltzer, K. Prevalence of overweight/obesity and central obesity and its associated factors among a sample of university students in India. Obes. Res. Clin. Pract. 2014, 8, e558–e570. [Google Scholar] [CrossRef] [PubMed]
- Saleem, M.D.; Ahmed, G.; Mulla, J.; Haider, S.S.; Abbas, M. Weight misperception amongst youth of a developing country: Pakistan -a cross-sectional study. BMC Public Health 2013, 13, 707. [Google Scholar] [CrossRef]
- A Maruf, F.; O Akinpelu, A.; Nwankwo, M.J. Perceived body image and weight: Discrepancies and gender differences among University undergraduates. Afr. Health Sci. 2012, 12, 464–472. [Google Scholar] [CrossRef]
- Gregory, C.; Martorell, R.; Narayan, K.V.; Ramirez-Zea, M.; Stein, A.D. Five-year changes in adiposity and cardio-metabolic risk factors among Guatemalan young adults. Public Health Nutr. 2009, 12, 228–235. [Google Scholar] [CrossRef]
- Olusanya, J.; Omotayo, O. Prevalence of obesity among undergraduate students of tai Solarin University of Education, Ijagun, Ijebu-ode. Pak. J. Nutr. 2011, 10, 940–946. [Google Scholar] [CrossRef]
- Dhruv, S.; Iyer, U.; Bhatt, K. Assessment of Cardio-Metabolic Risk Factors among Young Adult Females. Am. J. Infect. Dis. 2012, 8, 34–40. [Google Scholar] [CrossRef]
- Niemeier, H.M.; Raynor, H.; Lloyd-Richardson, E.E.; Rogers, M.L.; Wing, R.R. Fast Food Consumption and Breakfast Skipping: Predictors of Weight Gain from Adolescence to Adulthood in a Nationally Representative Sample. J. Adolesc. Health 2006, 39, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Wahabi, H.A.; Fayed, A.A.; Tharkar, S.; Esmaeil, S.A.; Bakhsh, H. Postpartum Weight Retention and Cardiometabolic Risk among Saudi Women: A Follow-Up Study of RAHMA Subcohort. BioMed Res. Int. 2019, 2019, 2957429. [Google Scholar] [CrossRef] [PubMed]
- Saudi Arabia to Start Granting Female Gym Licenses This Month. Arabnews, 12 February 2017.
- Paul, K. Saudi Arabia to Introduce Physical Education For Schoolgirls. Reuters, 11 July 2017. [Google Scholar]
- Saudi Vision 2030, Quality of Life Program. Available online: https://www.vision2030.gov.sa/v2030/vrps/qol/ (accessed on 2 November 2022).
- Restaurants in Saudi Arabia Must List Calories on Menus by End of 2018. Available online: https://english.alarabiya.net/life-style/healthy-living/2017/10/03/Restaurant-menus-to-list-calories-in-Saudi-Arabia#:~:text=Restaurants%20and%20cafes%20will%20now,and%20Drug%20Authority%20(SFDA) (accessed on 2 November 2022).
- East, P.M. KSA: Inclusion of Sugar Sweetened Beverages and Other Tobacco Products in the Excise Tax System. Available online: https://www.pwc.com/m1/en/services/tax/me-tax-legal-news/2019/ksa-inclusion-of-sugar-beverages-and-tobacco-products-in-the-ets.html (accessed on 2 November 2022).
- Williamson, J.M.L.; Rink, J.A.; Hewin, D.H. The Portrayal of Bariatric Surgery in the UK Print Media. Obes. Surg. 2012, 22, 1690–1694. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.P.S.; Martinino, A.; Manicone, F.; Pereira, M.L.S.; Puzas, Á.I.; Pouwels, S.; Martínez, J.M. Bariatric surgery on social media: A cross-sectional study. Obes. Res. Clin. Pract. 2022, 16, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Alfadda, A.A.; Al-Dhwayan, M.M.; Alharbi, A.A.; Al Khudhair, B.K.; Al Nozha, O.M.; Al-Qahtani, N.M.; Alzahrani, S.H.; Bardisi, W.M.; Sallam, R.M.; Riva, J.J.; et al. The Saudi clinical practice guideline for the management of overweight and obesity in adults. Saudi Med. J. 2016, 37, 1151–1162. [Google Scholar] [CrossRef] [PubMed]
- Alfadda, A.A.; Al Qarni, A.; Alamri, K.; Ahamed, S.S.; Abo’ouf, S.M.; Shams, M.; Abdelfattah, W.; Al Shaikh, A. Perceptions, attitudes, and barriers toward obesity management in Saudi Arabia: Data from the ACTION-IO study. Saudi J. Gastroenterol. 2021, 27, 166. [Google Scholar] [CrossRef] [PubMed]
- Tyrovolas, S.; El Bcheraoui, C.; A Alghnam, S.; Alhabib, K.F.; Almadi, M.A.H.; Al-Raddadi, R.M.; Bedi, N.; El Tantawi, M.; Krish, V.S.; A Memish, Z.; et al. The burden of disease in Saudi Arabia 1990–2017: Results from the Global Burden of Disease Study 2017. Lancet Planet. Health 2020, 4, e195–e208. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guideline on Self-Care Interventions for Health and Well-Being, 2022 Revision; World Health Organization: Geneva, Switzerland, 2022; p. 181. [Google Scholar]
- Sepúlveda-Peñaloza, A.; Cumsille, F.; Garrido, M.; Matus, P.; Vera-Concha, G.; Urquidi, C. Geographical disparities in obesity prevalence: Small-area analysis of the Chilean National Health Surveys. BMC Public Health 2022, 22, 1443. [Google Scholar] [CrossRef]
- Li, C.; Ademiluyi, A.; Ge, Y.; Park, A. Using Social Media to Understand Web-Based Social Factors Concerning Obesity: Systematic Review. JMIR Public Health Surveill. 2022, 8, e25552. [Google Scholar] [CrossRef]
- Kalra, S.; Kapoor, N.; Kota, S.; Das, S. Person-centred obesity care–techniques, thresholds, tools and targets. Eur. Endocrinol. 2020, 16, 11. [Google Scholar] [CrossRef]
- Vitolins, M.Z.; Crandall, S.; Miller, D.; Ip, E.; Marion, G.; Spangler, J.G. Obesity Educational Interventions in U.S. Medical Schools: A Systematic Review and Identified Gaps. Teach. Learn. Med. 2012, 24, 267–272. [Google Scholar] [CrossRef] [PubMed]
- DeCaria, J.E.; Sharp, C.; Petrella, R.J. Scoping review report: Obesity in older adults. Int. J. Obes. 2012, 36, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Alsukait, R.F.; Alfawaz, R.; Alamri, A.; Alghaith, T.; Alghodaier, H.; Hamza, M.M.; Sunaid, F.b.; El-Saharty, S.; Alkhalaf, M.; Alluhidan, M.; et al. Obesity-Prevention Strategies and Policies for Saudi Arabia. In Overweight and Obesity in Saudi Arabia: Consequences and Solutions; World Bank Group: Washington, DC, USA, 2022; pp. 105–133. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).