
Depression, Anxiety and Antidepressants and Anxiolytics Use in Spanish Informal Caregivers according to the Physical Activity Frequency: EHSS 2014–2020

 ,
,  ,
,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Data Source
2.2. Variables
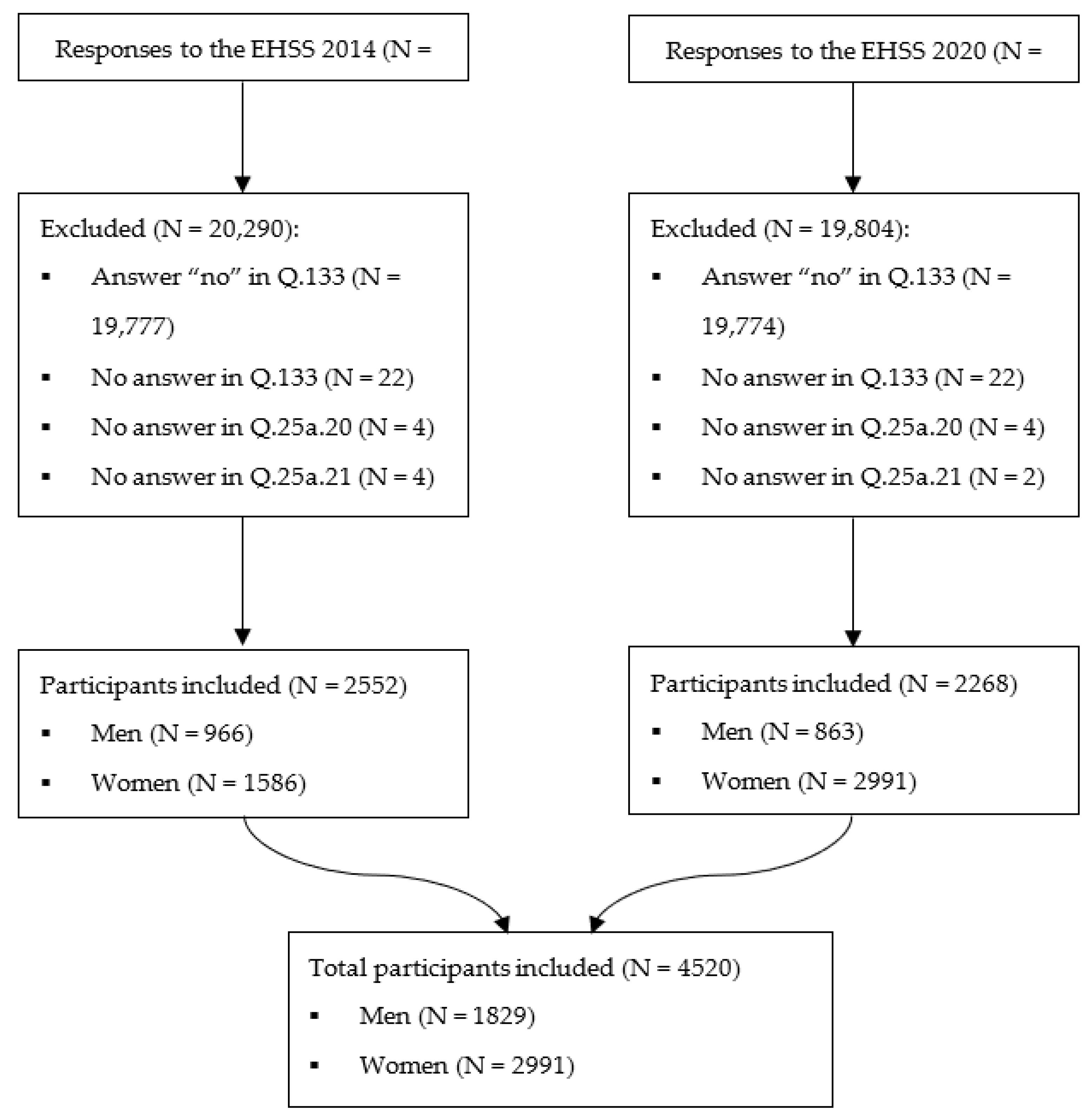
2.3. Participants
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization—Regional Office for Europe. The European Mental Health Action Plan 2013–2020; WHO: Geneva, Switzerland, 2015; p. 19. [Google Scholar]
- Litin, S.C. Mayo Clinic Family Health Book, 5th ed.; Litin, S.C., Ed.; Mayo Clinic Press: Rochester, MI, USA, 2018; p. 1392. ISBN 978-1-945564-02-4. [Google Scholar]
- Ministerio de Sanidad; Servicios Sociales e Igualdad; Instituto Nacional de Estadística Encuesta Nacional de Salud España 2017. Informe Monográfico de Salud Mental. SG Información Sanitaria Ministerio de Sanidad, Consumo y Bienestar Social 2017, 21–25. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/SALUD_MENTAL.pdf (accessed on 8 November 2022).
- Organización Mundial de la Salud Depresión. Available online: https://www.who.int/es/news-room/fact-sheets/detail/depression (accessed on 29 November 2022).
- Melhem, N.M.; Porta, G.; Oquendo, M.A.; Zelazny, J.; Keilp, J.G.; Iyengar, S.; Burke, A.; Birmaher, B.; Stanley, B.; Mann, J.J.; et al. Severity and Variability of Depression Symptoms Predicting Suicide Attempt in High-Risk Individuals. JAMA Psychiatry 2019, 76, 603–613. [Google Scholar] [CrossRef]
- Romero-Acosta, K.; Penelo, E.; Noorian, Z.; Ferreira, E.; Domènech-Llaberia, E. Racial/Ethnic Differences in the Prevalence of Internalizing Symptoms: Do Latin-American Immigrant Show More Symptomatology than Spanish Native-Born Adolescents? J. Health Psychol. 2014, 19, 381–392. [Google Scholar] [CrossRef]
- Sanchez-Garcia, M.; De La Rosa-Caceres, A.; Stasik-O’Brien, S.; Mancheno-Barba, J.J.; Lozano, O.M.; Diaz-Batanero, C. Norms According to Age and Gender for the Spanish Version of the Inventory of Depression and Anxiety Symptoms (IDAS-II). Front. Psychol. 2021, 12, 748025. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation Global Health Data Exchange (GHDx). Available online: https://ghdx.healthdata.org/ (accessed on 29 November 2022).
- Organización Mundial de la Salud Trastornos Mentales. Available online: https://www.who.int/es/news-room/fact-sheets/detail/mental-disorders (accessed on 29 November 2022).
- Córdoba, A.M.C.; Aparicio, M.J.G. Efectos de cuidar personas con Alzheimer: Un estudio sobre cuidadores formales e informales. Pensam. Psicológico 2014, 12, 149–167. [Google Scholar]
- Artaza Artabe, I.; Primitivo Ramos, C.; González Nuñez, J.; Martínez Hernández, D. Estudio de Investigación Sociosanitaria Sobre Cuidadores de Personas Mayores Dependientes; Sociedad Española de Geriatría y Gerontología; IMC—International Marketing & Communication S.A.: Madrid, Spain. Available online: http://envejecimiento.csic.es/documentos/documentos/Estudio-Cuidadores-segg.pdf (accessed on 8 November 2022).
- Hermida, E.; Vázquez, F.L.; Blanco, V.; Otero, P.; Torres, Á. El Malestar Emocional en los Cuidadores No Profesionales. In Proceedings of the 6th International and 11th National Congress of Clinical Psychology, Santiago de Compostela, Spain, 6–8 June 2013. [Google Scholar]
- Pérez Peñaranda, A.; García Ortiz, L.; Rodríguez Sánchez, E.; Losada Baltar, A.; Porras Santos, N.; Gómez Marcos, M.Á. Función familiar y salud mental del cuidador de familiares con dependencia. Aten. Primaria 2009, 41, 621–628. [Google Scholar] [CrossRef]
- Baltar, A.L. Estudio e Intervención sobre el Malestar Psicológico de los Cuidadores de Personas con Demencia; El Papel de los Pensamientos Disfuncionales; Imserso: Madrid, Spain, 2006. [Google Scholar]
- Awan, M.; Qureshi, S.; Tariq, H.; Siddiqi, F. Effects of Cardiopulmonary Conditioning on Body Mass Index, Physical Activity and General Psychological Health of Young Adults. Pak. Heart J. 2019, 52, 258–261. [Google Scholar]
- Ohrnberger, J.; Fichera, E.; Sutton, M. The Relationship between Physical and Mental Health: A Mediation Analysis. Soc. Sci. Med. 2017, 195, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.H.; Asare, M. Physical Activity and Mental Health in Children and Adolescents: A Review of Reviews. Br. J. Sport. Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [PubMed]
- Dinas, P.C.; Koutedakis, Y.; Flouris, A.D. Effects of Exercise and Physical Activity on Depression. Ir. J. Med. Sci. 2011, 180, 319–325. [Google Scholar] [CrossRef]
- Dishman, R.K.; O’Connor, P.J. Lessons in Exercise Neurobiology: The Case of Endorphins. Ment. Health Phys. Act. 2009, 2, 4–9. [Google Scholar] [CrossRef]
- Grisel, J.E.; Bartels, J.L.; Allen, S.A.; Turgeon, V.L. Influence of β-Endorphin on Anxious Behavior in Mice: Interaction with EtOH. Psychopharmacology 2008, 200, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Sloan, R.A.; Sawada, S.S.; Martin, C.K.; Church, T.; Blair, S.N. Associations between Cardiorespiratory Fitness and Health-Related Quality of Life. Health Qual. Life Outcomes 2009, 7, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Denche-Zamorano, Á.; Muñoz-Bermejo, L.; Carlos-Vivas, J.; Mendoza-Muñoz, M.; Franco-García, J.M.; Rojo-Ramos, J.; Vega-Muñoz, A.; Contreras-Barraza, N.; Barrios-Fernandez, S. A Cross-Sectional Study about the Associations between Physical Activity Level, Self-Perceived Health Perception and Mental Health in Informal Caregivers of Elderly or People with Chronic Conditions in Spain. Int. J. Environ. Res. Public. Health 2022, 19, 5320. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Bermejo, L.; Villafaina, S.; Collado-Mateo, D.; Postigo-Mota, S.; Adsuar, J.C. Physical Strength Perception of Older Caregivers in Rural Areas. Medicina 2019, 55, 692. [Google Scholar] [CrossRef] [PubMed]
- Egan, K.J.; Hodgson, W.; Dunlop, M.D.; Imperatore, G.; Kirk, A.; Maguire, R. A Novel Mobile App (“CareFit”) to Support Informal Caregivers to Undertake Regular Physical Activity from Home During and Beyond COVID-19 Restrictions: Co-Design and Prototype Development Study. JMIR Form. Res. 2021, 5, e27358. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística Metodología de La Encuesta Europea de Salud En España 2014 2014. Ministerio de Sanidad, Consumo y Bienestar Social Encuesta Nacional de Salud de España 2017. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm (accessed on 8 November 2022).
- Instituto Nacional de Estadística Metodología de La Encuesta Europea de Salud En España 2020 2020. Sanidad Consumo, M.; Social, B. Encuesta Nacional de Salud 2017 ENSE 2017: Metodología. Available online: https://www.ine.es/metodologia/t15/t153041917.pdf (accessed on 8 November 2022).
- Shfiezadeh, A.; Mirzaee, A.; Heravi-Karimooi, M.; Rejeh, N.; Sharif Nia, H.; Montazeri, A. Anxiety and Depression in Caregivers of Elderly with Alzheimer. Payesh Health Monit. 2019, 18, 579–587. [Google Scholar]
- Ketcher, D.; Trettevik, R.; Vadaparampil, S.T.; Heyman, R.E.; Ellington, L.; Reblin, M. Caring for a Spouse with Advanced Cancer: Similarities and Differences for Male and Female Caregivers. J. Behav. Med. 2020, 43, 817–828. [Google Scholar] [CrossRef]
- Oechsle, K.; Ullrich, A.; Marx, G.; Benze, G.; Wowretzko, F.; Zhang, Y.; Dickel, L.-M.; Heine, J.; Wendt, K.N.; Nauck, F.; et al. Prevalence and Predictors of Distress, Anxiety, Depression, and Quality of Life in Bereaved Family Caregivers of Patients With Advanced Cancer. Am. J. Hosp. Palliat. Care 2020, 37, 201–213. [Google Scholar] [CrossRef]
- Unsar, S.; Erol, O.; Ozdemir, O. Caregiving Burden, Depression, and Anxiety in Family Caregivers of Patients with Cancer. Eur. J. Oncol. Nurs. Off. J. Eur. Oncol. Nurs. Soc. 2021, 50, 101882. [Google Scholar] [CrossRef]
- Thomann, P.; Rousseau, A.; Valette, S.; Martin-Hunyadi, C.; Vogel, T.; Michel, B. Psychotropic Medication Use by Informal Caregivers of Elderly Patients with Dementia: A French Observational Study. NPG Neurol. Psychiatr. Gériatrie 2022, 22, 107–112. [Google Scholar] [CrossRef]
- Wolf, S.; Seiffer, B.; Zeibig, J.-M.; Welkerling, J.; Brokmeier, L.; Atrott, B.; Ehring, T.; Schuch, F.B. Is Physical Activity Associated with Less Depression and Anxiety During the COVID-19 Pandemic? A Rapid Systematic Review. Sport. Med. 2021, 51, 1771–1783. [Google Scholar] [CrossRef] [PubMed]
- McDowell, C.P.; Dishman, R.K.; Gordon, B.R.; Herring, M.P. Physical Activity and Anxiety: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Am. J. Prev. Med. 2019, 57, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Baik, D.; Song, J.; Tark, A.; Coats, H.; Shive, N.; Jankowski, C. Effects of Physical Activity Programs on Health Outcomes of Family Caregivers of Older Adults with Chronic Diseases: A Systematic Review. Geriatr. Nurs. 2021, 42, 1056–1069. [Google Scholar] [CrossRef] [PubMed]
- Montero-Cuadrado, F.; Galán-Martín, M.Á.; Sánchez-Sánchez, J.; Lluch, E.; Mayo-Iscar, A.; Cuesta-Vargas, Á. Effectiveness of a Physical Therapeutic Exercise Programme for Caregivers of Dependent Patients: A Pragmatic Randomised Controlled Trial from Spanish Primary Care. Int. J. Environ. Res. Public. Health 2020, 17, 7359. [Google Scholar] [CrossRef]
- Doyle, K.L.; Toepfer, M.; Bradfield, A.F.; Noffke, A.; Ausderau, K.K.; Andreae, S.; Pickett, K.A. Systematic Review of Exercise for Caregiver-Care Recipient Dyads: What Is Best for Spousal Caregivers-Exercising Together or Not at All? Gerontologist 2021, 61, e283–e301. [Google Scholar] [CrossRef] [PubMed]
- Valero-Cantero, I.; Casals, C.; Corral-Pérez, J.; Barón-López, F.J.; Wärnberg, J.; Vázquez-Sánchez, M.Á. Accelerometer-Measured Physical Activity, Inactivity, and Related Factors in Family Caregivers of Patients with Terminal Cancer. Int. J. Environ. Res. Public. Health 2023, 20, 179. [Google Scholar] [CrossRef]
- McAuley, E.; Elavsky, S.; Jerome, G.J.; Konopack, J.F.; Marquez, D.X. Physical Activity-Related Well-Being in Older Adults: Social Cognitive Influences. Psychol. Aging 2005, 20, 295–302. [Google Scholar] [CrossRef]
- Elavsky, S.; McAuley, E.; Motl, R.W.; Konopack, J.F.; Marquez, D.X.; Hu, L.; Jerome, G.J.; Diener, E. Physical Activity Enhances Long-Term Quality of Life in Older Adults: Efficacy, Esteem, and Affective Influences. Ann. Behav. Med. Publ. Soc. Behav. Med. 2005, 30, 138–145. [Google Scholar] [CrossRef]
- Marshall, E.; LaCaille, R.A.; LaCaille, L.J.; Lee, J.E.; Peterson, E. Effects of Physical Activity Interventions for Caregivers of Adults: A Meta-Analysis. Health Psychol. 2022, 41, 585–598. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| EHSS 2014 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | Men | Women | ||||||||
| N = 2552 | (%) | n = 966 | (%) | n = 1586 | (%) | x2 | df | p | CC | |
| Depression | 383 | (15.0) | 88 | (9.1) | 295 | (18.6) * | 42.4 | 1 | <0.001 | 0.128 |
| No depression | 2169 | (85.0) | 878 | (90.9) | 1291 | (81.4) * | ||||
| Anxiety | 352 | (13.8) | 75 | (7.8) | 277 | (17.5) * | 47.5 | 1 | <0.001 | 0.135 |
| No anxiety | 2200 | (86.2) | 891 | (92.2) | 1309 | (82.5) * | ||||
| Antidepressant | 195 | (7.6) | 39 | (4.0) | 156 | (9.8) * | 28.6 | 1 | <0.001 | 0.105 |
| No antidepressant | 2357 | (92.4) | 927 | (96.0) | 1430 | (90.2) * | ||||
| Anxiolytics | 419 | (16.4) | 94 | (9.7) | 325 | (20.5) * | 50.7 | 1 | <0.001 | 0.140 |
| No anxiolytics | 2133 | (83.6) | 872 | (90.3) | 1261 | (79.5) * | ||||
| EHSS 2020 | ||||||||||
| Total | Men | Women | ||||||||
| n = 2268 | (%) | n = 863 | (%) | n = 1405 | (%) | x2 | df | p | CC | |
| Depression | 268 | (11.8) | 72 | (8.3) | 196 | (14.0) * | 16.1 | 1 | <0.001 | 0.084 |
| No depression | 2000 | (88.2) | 791 | (91.7) | 1209 | (86.0) * | ||||
| Anxiety | 258 | (11.4) | 60 | (7.0) | 198 | (14.1) * | 27.0 | 1 | <0.001 | 0.109 |
| No anxiety | 2010 | (88.6) | 803 | (93.0) | 1207 | (85.9) * | ||||
| Antidepressant | 151 | (6.7) | 32 | (3.7) | 119 | (8.5) * | 19.5 | 1 | <0.001 | 0.092 |
| No antidepressants | 2117 | (93.3) | 831 | (96.3) | 1286 | (91.5) * | ||||
| Anxiolytics | 306 | (13.5) | 82 | (9.5) | 224 | (15.9) * | 19.0 | 1 | <0.001 | 0.091 |
| No anxiolytics | 1962 | (86.5) | 781 | (90.5) | 1181 | (84.1) * | ||||
| EHSS 2014 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Inactive | Occasional | Active | Very Active | |||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |||||
| Depression | Ref. | 0.65 * | 0.52 | 0.83 | 0.27 * | 0.16 | 0.46 | 0.40 * | 0.26 | 0.61 |
| Anxiety | Ref. | 0.68 | 0.32 | 1.47 | 0.22 * | 0.08 | 0.63 | 0.37 * | 0.15 | 0.90 |
| Antidepressants | Ref. | 0.64 | 0.24 | 1.72 | 0.34 | 0.11 | 1.12 | 0.20 * | 0.05 | 0.85 |
| Anxiolytics | Ref. | 0.69 | 0.34 | 1.42 | 0.50 | 0.23 | 1.09 | 0.30 * | 0.12 | 0.73 |
| EHSS 2020 | ||||||||||
| Inactive | Occasional | Active | Very Active | |||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |||||
| Depression | Ref. | 0.63 * | 0.47 | 0.84 | 0.48 * | 0.29 | 0.77 | 0.44 * | 0.29 | 0.67 |
| Anxiety | Ref. | 0.74 * | 0.55 | 0.99 | 0.56 * | 0.35 | 0.91 | 0.42 * | 0.27 | 0.66 |
| Antidepressants | Ref. | 0.65 * | 0.45 | 0.93 | 0.39 * | 0.20 | 0.76 | 0.26 * | 0.13 | 0.51 |
| Anxiolytics | Ref. | 0.72 * | 0.55 | 0.94 | 0.35 * | 0.21 | 0.58 | 0.34 * | 0.22 | 0.52 |
| EHSS2014 | |||||||
|---|---|---|---|---|---|---|---|
| PAF | Depression | Anxiety | Antidepressants | Anxiolytics | Age | Sex | |
| rho | rho | rho | rho | rho | rho | rho | |
| PAF | 1.000 | −0.125 ** | −0.124 ** | −0.107 ** | −0.119 ** | −0.153 ** | −0.087 |
| Depression | −0.125 ** | 1.000 | 0.554 ** | 0.523 ** | 0.385 ** | 0.100 ** | −0.129 ** |
| Anxiety | −0.124 ** | 0.554 ** | 1.000 | 0.480 ** | 0.433 ** | 0.075 ** | −0.136 ** |
| Antidepressants | −0.107 ** | 0.523 ** | 0.480 ** | 1.000 | 0.474 ** | 0.068 | −0.106 ** |
| Anxiolytics | −0.119 ** | 0.385 ** | 0.433 ** | 0.474 ** | 1.000 | 0.152 ** | −0.141 ** |
| Age | −0.153 ** | 0.100 ** | 0.075 ** | 0.068 | 0.152 ** | 1.000 | 0.026 |
| Sex | −0.087 ** | −0.129 ** | −0.136 ** | −0.106 ** | −0.141 ** | 0.026 | 1.000 |
| EHSS2020 | |||||||
| PAF | Depression | Anxiety | Antidepressants | Anxiolytics | Age | Sex | |
| PAF | 1.000 | −0.099 ** | −0.088 ** | −0.101 ** | −0.125 ** | −0.110 ** | −0.057 |
| Depression | −0.099 ** | 1.000 | 0.463 ** | 0.549 ** | 0.367 ** | 0.084 ** | −0.084 ** |
| Anxiety | −0.088 ** | 0.463 ** | 1.000 | 0.411 ** | 0.375 ** | 0.014 | −0.109 ** |
| Antidepressants | −0.101 ** | 0.549 ** | 0.411 ** | 1.000 | 0.417 ** | 0.054 | −0.093 ** |
| Anxiolytics | −0.125 ** | 0.367 ** | 0.375 ** | 0.417 ** | 1.000 | 0.119 ** | −0.092 ** |
| Age | −0.11 0 ** | 0.084 ** | 0.014 | 0.054 | 0.119 ** | 1.000 | 0.026 |
| Sex | −0.057 | −0.084 ** | −0.109 ** | −0.093 ** | −0.092 ** | 0.026 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denche-Zamorano, A.; Rodriguez-Redondo, Y.; Barrios-Fernandez, S.; Mendoza-Muñoz, M.; Rojo-Ramos, J.; Garcia-Gordillo, M.A.; Adsuar, J.C.; Muñoz-Bermejo, L. Depression, Anxiety and Antidepressants and Anxiolytics Use in Spanish Informal Caregivers according to the Physical Activity Frequency: EHSS 2014–2020. Healthcare 2023, 11, 990. https://doi.org/10.3390/healthcare11070990
Denche-Zamorano A, Rodriguez-Redondo Y, Barrios-Fernandez S, Mendoza-Muñoz M, Rojo-Ramos J, Garcia-Gordillo MA, Adsuar JC, Muñoz-Bermejo L. Depression, Anxiety and Antidepressants and Anxiolytics Use in Spanish Informal Caregivers according to the Physical Activity Frequency: EHSS 2014–2020. Healthcare. 2023; 11(7):990. https://doi.org/10.3390/healthcare11070990
Chicago/Turabian StyleDenche-Zamorano, Angel, Yeray Rodriguez-Redondo, Sabina Barrios-Fernandez, María Mendoza-Muñoz, Jorge Rojo-Ramos, Miguel Angel Garcia-Gordillo, Jose C. Adsuar, and Laura Muñoz-Bermejo. 2023. "Depression, Anxiety and Antidepressants and Anxiolytics Use in Spanish Informal Caregivers according to the Physical Activity Frequency: EHSS 2014–2020" Healthcare 11, no. 7: 990. https://doi.org/10.3390/healthcare11070990
APA StyleDenche-Zamorano, A., Rodriguez-Redondo, Y., Barrios-Fernandez, S., Mendoza-Muñoz, M., Rojo-Ramos, J., Garcia-Gordillo, M. A., Adsuar, J. C., & Muñoz-Bermejo, L. (2023). Depression, Anxiety and Antidepressants and Anxiolytics Use in Spanish Informal Caregivers according to the Physical Activity Frequency: EHSS 2014–2020. Healthcare, 11(7), 990. https://doi.org/10.3390/healthcare11070990