
Remote and Unsupervised Exercise Strategies for Improving the Physical Activity of Colorectal Cancer Patients: A Meta-Analysis
 , and
, and 
Abstract
1. Introduction
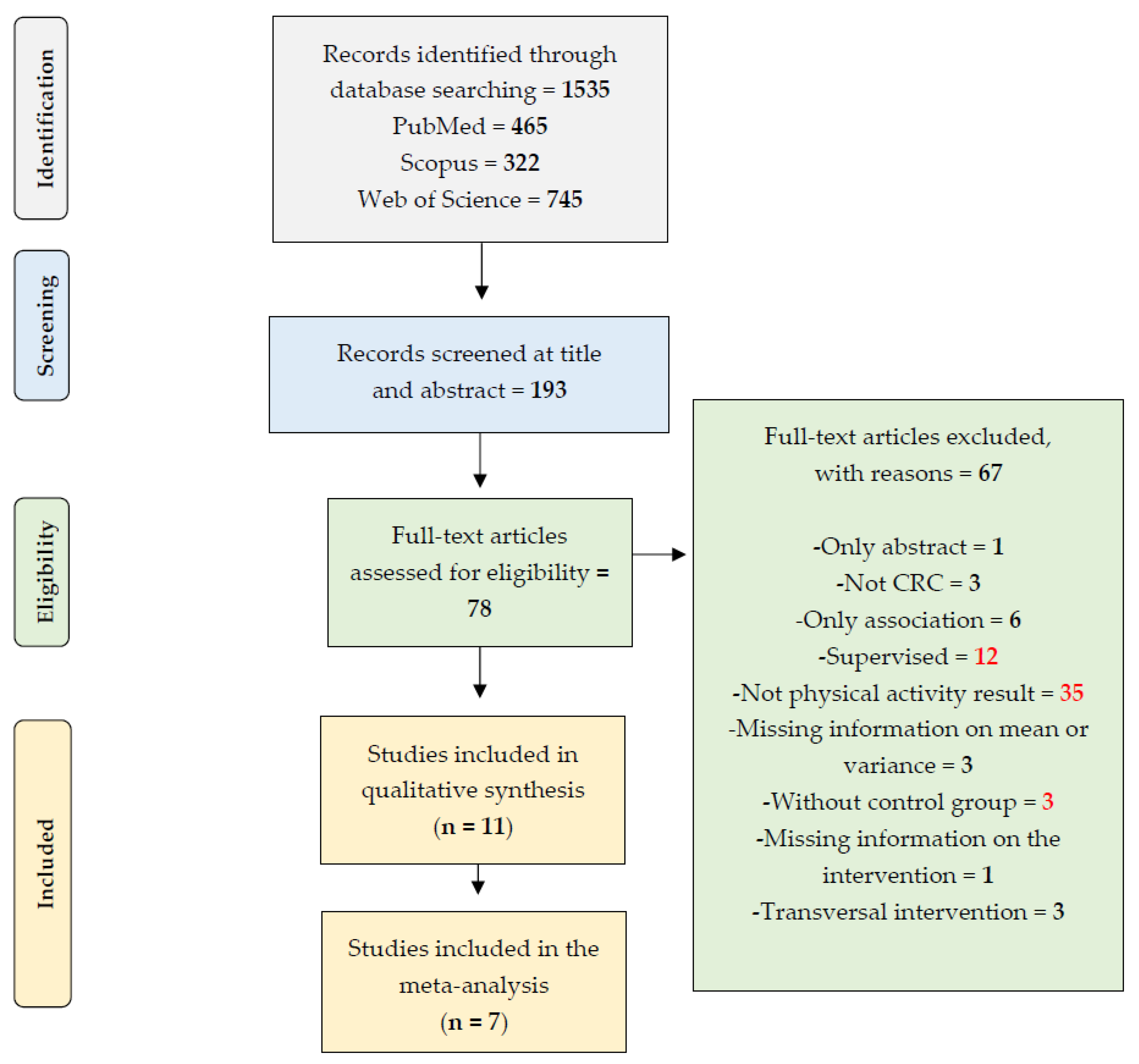
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment
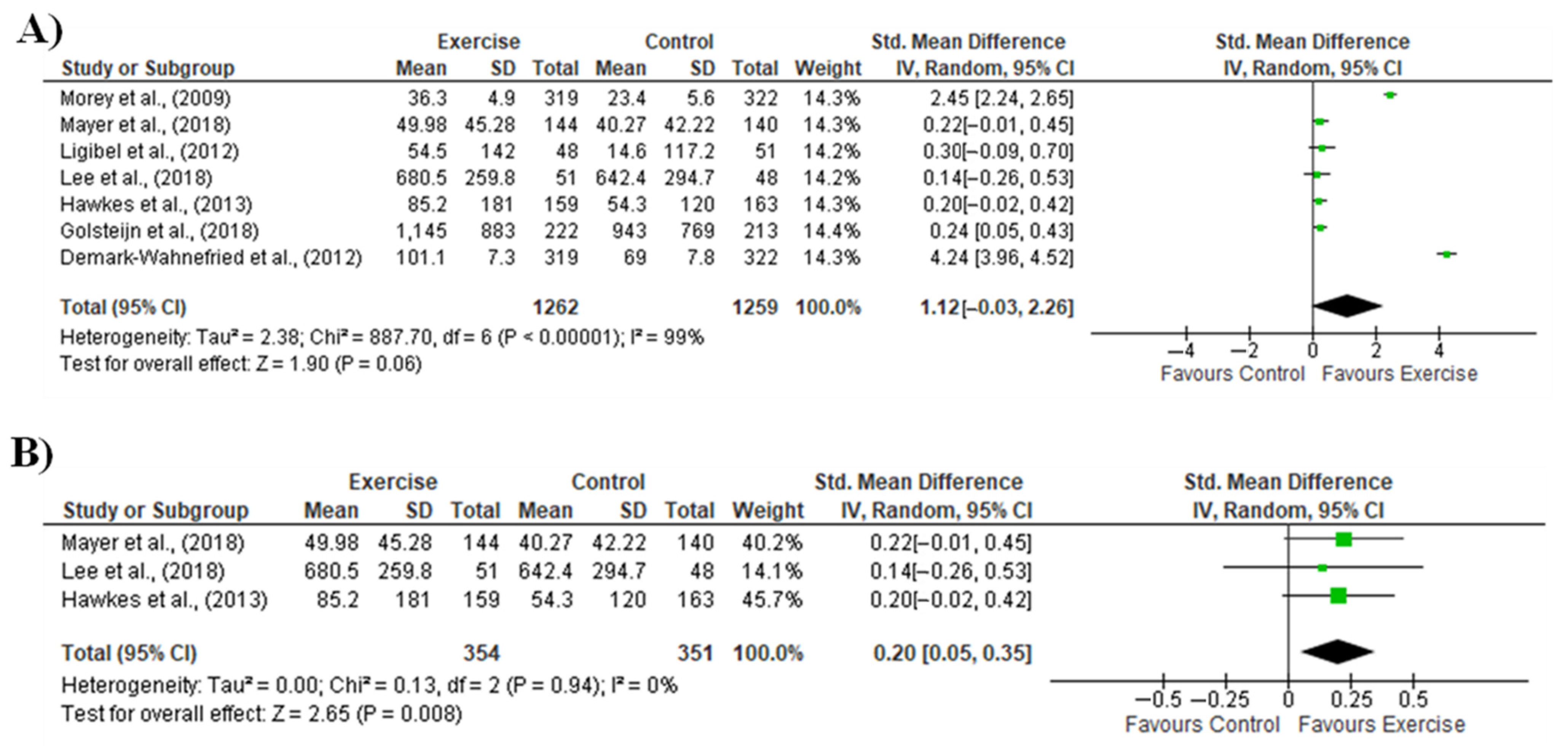
2.4. Meta-Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Morey et al., 2009 [34] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Ligibel et al., 2012 [32] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Demark-Wahnefried et al., 2012 [28] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Hawkes et al., 2013 [30] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Pinto et al., 2013 [38] | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes |
| Park et al., 2015 [37] | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Mayer et al., 2018 [33] | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
| Lee et al., 2018 [31] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Golsteijn et al., 2018 [29] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes |
| Maxwell-Smith et al., 2018 [40] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Moug et al., 2019 [36] | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes |
References
- Jung, Y.M.; Chung, J.P.; Son, H.P. Physical Activity Interventions for Colorectal Cancer Survivors: A Systematic Review and Meta- analysis of Randomized Controlled Trials. Cancer Nurs. 2021, 44, E414–E428. [Google Scholar] [CrossRef] [PubMed]
- Mbous, Y.P.; Patel, J.; Kelly, K.M. A systematic review and meta-analysis of physical activity interventions among colorectal cancer survivors. Transl. Behav. Med. 2020, 10, 1134–1143. [Google Scholar] [CrossRef] [PubMed]
- Schmid, D.; Leitzmann, M.F. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: A systematic review and meta-analysis. Ann. Oncol. 2014, 25, 1293–1311. [Google Scholar] [CrossRef] [PubMed]
- Walter, V.; Jansen, L.; Knebel, P.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H. Physical activity and survival of colorectal cancer patients: Population-based study from Germany. Int. J. Cancer 2017, 140, 1985–1997. [Google Scholar] [CrossRef]
- Wang, L.; Langlais, C.S.; Kenfield, S.A.; Chan, J.M.; Graff, R.E.; Allen, I.E.; Atreya, C.E.; Van Blarigan, E.L. mHealth Interventions to Promote a Healthy Diet and Physical Activity among Cancer Survivors: A Systematic Review of Randomized Controlled Trials. Cancers 2022, 14, 3816. [Google Scholar] [CrossRef]
- Wiltink, L.M.; White, K.; King, M.T.; Rutherford, C. Systematic review of clinical practice guidelines for colorectal and anal cancer: The extent of recommendations for managing long-term symptoms and functional impairments. Support. Care Cancer 2020, 28, 2523–2532. [Google Scholar] [CrossRef]
- Gao, R.; Yu, T.; Liu, L.; Bi, J.; Zhao, H.; Tao, Y.; Li, F.; Guo, L. Exercise intervention for post-treatment colorectal cancer survivors: A systematic review and meta-analysis. J. Cancer Surviv. 2020, 14, 878–893. [Google Scholar] [CrossRef]
- Kraemer, M.B.; Priolli, D.G.; Reis, I.G.M.; Pelosi, A.C.; Garbuio, A.L.P.; Messias, L.H.D. Home-based, supervised, and mixed exercise intervention on functional capacity and quality of life of colorectal cancer patients: A meta-analysis. Sci. Rep. 2022, 12, 2471. [Google Scholar] [CrossRef]
- Singh, B.; Hayes, S.C.; Spence, R.R.; Steele, M.L.; Millet, G.Y.; Gergele, L. Exercise and colorectal cancer: A systematic review and meta-analysis of exercise safety, feasibility and effectiveness. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–14. [Google Scholar] [CrossRef]
- Choy, K.T.; Lam, K.; Kong, J.C. Exercise and colorectal cancer survival: An updated systematic review and meta-analysis. Int. J. Color. Dis. 2022, 37, 1751–1758. [Google Scholar] [CrossRef]
- Eyl, R.E.; Xie, K.; Koch-Gallenkamp, L.; Brenner, H.; Arndt, V. Quality of life and physical activity in long-term (≥5 years post-diagnosis) colorectal cancer survivors—systematic review. Health Qual. Life Outcomes 2018, 16, 112. [Google Scholar] [CrossRef]
- Hirschey, R.; Nance, J.; Hoover, R.; Triglianos, T.; Coffman, E.; Horrell, L.N.; Walker, J.S.; Bryant, A.L.; Valle, C.G. Physical Activity: A Systematic Review to Inform Nurse Recommendations During Treatment for Colorectal Cancer. Clin. J. Oncol. Nurs. 2021, 25, 697–705. [Google Scholar] [CrossRef]
- Hong, J.; Park, J. Systematic Review: Recommendations of Levels of Physical Activity among Colorectal Cancer Patients (2010–2019). Int. J. Environ. Res. Public Health 2021, 18, 2896. [Google Scholar] [CrossRef] [PubMed]
- McGettigan, M.; Cardwell, C.R.; Cantwell, M.M.; Tully, M.A. Physical activity interventions for disease-related physical and mental health during and following treatment in people with non-advanced colorectal cancer. Cochrane Database Syst. Rev. 2020, 5, CD012864. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Jiang, C.; Zhou, L. Physical activity and mortality in patients with colorectal cancer: A meta-analysis of prospective cohort studies. Eur. J. Cancer Prev. 2020, 29, 15–26. [Google Scholar] [CrossRef] [PubMed]
- van Gestel, T.; Groen, L.; Puik, J.; van Rooijen, S.; van der Zaag-Loonen, H.; Schoonmade, L.; Danjoux, G.; Daams, F.; Schreurs, W.; Bruns, E. Fit4Surgery for cancer patients during covid-19 lockdown—A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2022, 48, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Brandenbarg, D.; Korsten, J.H.W.M.; Berger, M.Y.; Berendsen, A.J. The effect of physical activity on fatigue among survivors of colorectal cancer: A systematic review and meta-analysis. Support. Care Cancer 2018, 26, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Huizinga, F.; Westerink, N.-D.L.; Berendsen, A.J.; Walenkamp, A.M.E.; de Greef, M.H.G.; Nijeweeme, J.K.O.; de Bock, G.H.; Berger, M.Y.; Brandenbarg, D. Home-based Physical Activity to Alleviate Fatigue in Cancer Survivors: A Systematic Review and Meta-analysis. Med. Sci. Sports Exerc. 2021, 53, 2661. [Google Scholar] [CrossRef] [PubMed]
- Rezende, L.F.M.; Lee, D.H.; Ferrari, G.; Eluf-Neto, J.; Giovannucci, E.L. Physical activity for cancer patients during COVID-19 pandemic: A call to action. Cancer Causes Control. 2020, 32, 1–3. [Google Scholar] [CrossRef]
- Barakat, S.; Boehmer, K.; Abdelrahim, M.; Ahn, S.; Al-Khateeb, A.A.; Villalobos, N.; Prokop, L.; Erwin, P.J.; Fleming, K.; Serrano, V.; et al. Does Health Coaching Grow Capacity in Cancer Survivors? A Systematic Review. Popul. Health Manag. 2018, 21, 63–81. [Google Scholar] [CrossRef]
- Ayyoubzadeh, S.M.; Kalhori, S.R.N.; Shirkhoda, M.; Mohammadzadeh, N.; Esmaeili, M. Supporting colorectal cancer survivors using eHealth: A systematic review and framework suggestion. Support. Care Cancer 2020, 28, 3543–3555. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, K.H.D.S.; de Oliveira, M.V.L.; Nascimento, I.J.B.D.; Rocha, L.D.B.; Filho, L.E.C.D.S.; Rocha, R.S.B.; da Silva, M.L.; Cunha, K.D.C. Physical Exercise and Quality of Life of Patients Diagnosed with Colorectal Cancer: Systematic Literature Review. J. Gastrointest. Cancer 2021, 52, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Je, Y.; Jeon, J.Y.; Giovannucci, E.L.; Meyerhardt, J.A. Association between physical activity and mortality in colorectal cancer: A meta-analysis of prospective cohort studies. Int. J. Cancer 2013, 133, 1905–1913. [Google Scholar] [CrossRef] [PubMed]
- Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Systematica Reviews: CRD’s Guidance for Undertaking Reviews in Health Care. Available online: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf (accessed on 10 November 2022).
- Database PE. Available online: https://pedro.org.au/ (accessed on 10 November 2022).
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Morey, M.C.; Sloane, R.; Snyder, D.C.; Miller, P.E.; Hartman, T.J.; Cohen, H.J. Reach Out to Enhance Wellness Home-Based Diet-Exercise Intervention Promotes Reproducible and Sustainable Long-Term Improvements in Health Behaviors, Body Weight, and Physical Functioning in Older, Overweight/Obese Cancer Survivors. J. Clin. Oncol. 2012, 30, 2354–2361. [Google Scholar] [CrossRef]
- Golsteijn, R.H.J.; Bolman, C.; Volders, E.; Peels, D.A.; De Vries, H.; Lechner, L. Short-term efficacy of a computer-tailored physical activity intervention for prostate and colorectal cancer patients and survivors: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–14. [Google Scholar] [CrossRef]
- Hawkes, A.L.; Chambers, S.K.; Pakenham, K.I.; Patrao, T.A.; Baade, P.D.; Lynch, B.M.; Aitken, J.F.; Meng, X.; Courneya, K.S. Effects of a Telephone-Delivered Multiple Health Behavior Change Intervention (CanChange) on Health and Behavioral Outcomes in Survivors of Colorectal Cancer: A Randomized Controlled Trial. J. Clin. Oncol. 2013, 31, 2313–2321. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.F.; Ho, J.W.C.; Fong, D.Y.T.; Macfarlane, D.J.; Cerin, E.; Lee, A.M.; Leung, S.; Chan, W.Y.Y.; Leung, I.P.F.; Lam, S.H.S.; et al. Dietary and Physical Activity Interventions for Colorectal Cancer Survivors: A Randomized Controlled Trial. Sci. Rep. 2018, 8, 5731. [Google Scholar] [CrossRef] [PubMed]
- Ligibel, J.A.; Meyerhardt, J.; Pierce, J.P.; Najita, J.; Shockro, L.; Campbell, N.; Newman, V.A.; Barbier, L.; Hacker, E.; Wood, M.; et al. Impact of a telephone-based physical activity intervention upon exercise behaviors and fitness in cancer survivors enrolled in a cooperative group setting. Breast Cancer Res. Treat. 2012, 132, 205–213. [Google Scholar] [CrossRef]
- Mayer, D.K.; Landucci, G.; Awoyinka, L.; Atwood, A.K.; Carmack, C.L.; Demark-Wahnefried, W.; McTavish, F.; Gustafson, D.H. SurvivorCHESS to increase physical activity in colon cancer survivors: Can we get them moving? J. Cancer Surviv. 2017, 12, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Morey, M.C.; Snyder, D.C.; Sloane, R.; Cohen, H.J.; Peterson, B.; Hartman, T.J.; Miller, P.; Mitchell, D.C.; Demark-Wahnefried, W. Effects of Home-Based Diet and Exercise on Functional Outcomes Among Older, Overweight Long-term Cancer Survivors: RENEW: A randomized controlled trial. JAMA 2009, 301, 1883–1891. [Google Scholar] [CrossRef] [PubMed]
- Maxwell-Smith, C.; Hince, D.; Cohen, P.; Bulsara, M.K.; Boyle, T.; Platell, C.; Tan, P.; Levitt, M.; Salama, P.; Tan, J.; et al. A randomized controlled trial of WATAAP to promote physical activity in colorectal and endometrial cancer survivors. Psycho-Oncology 2019, 28, 1420–1429. [Google Scholar] [CrossRef] [PubMed]
- Moug, S.J.; Mutrie, N.; Barry, S.J.E.; Mackay, G.; Steele, R.J.C.; Boachie, C.; Buchan, C.; Anderson, A.S. Prehabilitation is feasible in patients with rectal cancer undergoing neoadjuvant chemoradiotherapy and may minimize physical deterioration: Results from the REx trial. Color. Dis. 2019, 21, 548–562. [Google Scholar] [CrossRef]
- Park, J.-H.; Lee, J.; Oh, M.; Park, H.; Chae, J.; Kim, D.-I.; Lee, M.K.; Yoon, Y.J.; Lee, C.W.; Park, S.; et al. The effect of oncologists’ exercise recommendations on the level of exercise and quality of life in survivors of breast and colorectal cancer: A randomized controlled trial. Cancer 2015, 121, 2740–2748. [Google Scholar] [CrossRef]
- Pinto, B.M.; Papandonatos, G.; Goldstein, M.G.; Marcus, B.H.; Farrell, N. Home-based physical activity intervention for colorectal cancer survivors. Psycho-Oncology 2013, 22, 54–64. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Comprehensive Meta-Analysis (Version 2.2. 027). Biostat: Englewood, NJ, USA, 2006. [Google Scholar]
- Hardcastle, S.J.; Maxwell-Smith, C.; Kamarova, S.; Lamb, S.; Millar, L.; Cohen, P.A. Factors influencing non-participation in an exercise program and attitudes towards physical activity amongst cancer survivors. Support. Care Cancer 2018, 26, 1289–1295. [Google Scholar] [CrossRef]
- Awasthi, R.; Minnella, E.M.; Ferreira, V.; Ramanakumar, A.V.; Scheede-Bergdahl, C.; Carli, F. Supervised exercise training with multimodal pre-habilitation leads to earlier functional recovery following colorectal cancer resection. Acta Anaesthesiol. Scand. 2019, 63, 461–467. [Google Scholar] [CrossRef]
- Hatlevoll, I.; Skolbekken, J.; Oldervoll, L.M.; Wibe, A.; Hofsli, E. Colorectal cancer patients’ experiences with supervised exercise during adjuvant chemotherapy—A qualitative study. Scand. J. Med. Sci. Sports 2021, 31, 2300–2309. [Google Scholar] [CrossRef]
- Lopez, C.; McGarragle, K.; Pritlove, C.; Jones, J.M.; Alibhai, S.M.H.; Lenton, E.; Mina, D.S. Variability and limitations in home-based exercise program descriptions in oncology: A scoping review. Support. Care Cancer 2020, 28, 4005–4017. [Google Scholar] [CrossRef]
- Fisher, A.; Williams, K.; Beeken, R.; Wardle, J. Recall of physical activity advice was associated with higher levels of physical activity in colorectal cancer patients. BMJ Open 2015, 5, e006853. [Google Scholar] [CrossRef] [PubMed]


| Study | Sample Size | Age | Only CRC Patients? Stage of Cancer or Condition |
|---|---|---|---|
| Morey et al., (2009) [34] | Control—n = 322 Female—n = 177 Male—n = 145 Intervention—n = 319 Female—n = 172 Male—n = 147 | Control = 73 ± 5 yrs Intervention = 73 ± 5 yrs | No Control Breast—n = 146 Prostate—n = 130 Colorectal—n = 46 Years since cancer diagnosis = 8 ± 2 Intervention Breast—n = 143 Prostate—n = 131 Colorectal—n = 45 Years since cancer diagnosis = 8 ± 2 |
| Ligibel et al., (2012) [32] | Control—n = 60 Female—n = 56 Male—n = 4 Intervention—n = 61 Female—n = 56 Male—n = 5 | Control = 55 ± 10 yrs Intervention = 53 ± 10 yrs | No Control Breast—n = 50 Colorectal—n = 10 Stage 1 = 21; Stage 2 = 23; Stage 3 = 16 Intervention Breast—n = 50 Colorectal—n = 11 Stage 1 = 20; Stage 2 = 19; Stage 3 = 22 |
| # Demark-Wahnefried et al., (2012) [28] | Control—n = 245 Female—n = 138 Male—n = 107 Intervention—n = 243 Female—n = 132 Male—n = 111 | Control = 72 ± 5 yrs Intervention = 73 ± 5 yrs | No Control Breast—n = 110 Prostate—n = 94 Colorectal—n = 41 Intervention Breast—n = 111 Prostate—n = 99 Colorectal—n = 33 ≥5 years from diagnosis |
| Hawkes et al., (2013) [30] | Control—n = 205 Female—n = 90 Male—n = 115 Intervention—n = 205 Female—n = 99 Male—n = 106 | Control = 67 ± 9 yrs Intervention = 64 ± 10 yrs | Yes Control—Dukes’ staging—A = 39; B = 53; C = 48; Unknown = 65; Intervention—Dukes’ staging—A = 36; B = 65; C = 45; Unknown = 59 |
| Pinto et al., (2013) [38] | Control—n = 26 Female—n = 14 Male—n = 12 Intervention—n = 20 Female—n = 12 Male—n = 8 | Control = 55 ± 8 yrs Intervention = 59 ± 11 yrs | Yes Stages 1, 2 or 3 |
| Park et al., (2015) [37] | Control—n = 59 Female—n = 50 Male—n = 9 Intervention—n = 50 Female—n = 45 Male—n = 5 | Control = 53 ± 8 yrs Intervention = 50 ± 8 yrs | No Control Breast—n = 41 Colorectal—n = 18 Stage 1 = 22; Stage 2 = 21; Stage 3 = 12 Intervention Breast—n = 39 Colorectal—n = 11 Stage 1 = 19; Stage 2 = 15; Stage 3 = 8 |
| Mayer et al., (2018) [33] | Control—n = 140 Female—n = 73 Male—n = 67 Intervention—n = 144 Female—n = 74 Male—n = 70 | Control = 57 ± 14 yrs (n = 104) Intervention = 59 ± 13 yrs (n = 115) | Yes Control—Stage 1 = 27; Stage 2 = 82; Stage 3 = 29 Intervention—Stage 1 = 39; Stage 2 = 63; Stage 3 = 41 |
| Lee et al., (2018) [31] | Control—n = 56 Female—n = 26 Male—n = 30 Intervention—n = 56 Female—n = 16 Male—n = 40 | Control = 64 ± 9 yrs Intervention =66 ± 9 yrs | Yes Control—Stage 1 = 12; Stage 2 = 24; Stage 3 or 4= 20 Intervention—Stage 1 = 8; Stage 2 = 27; Stage 3 or 4= 20 |
| Golsteijn et al., (2018) [29] | Control—n = 229 Female—n = 25 Male—n = 204 Intervention—n = 249 Female—n = 37 Male—n = 212 | Control = 66 ± 8 yrs Intervention = 66 ± 7 yrs | No Control Prostate—n = 143 Colorectal—n = 86 Intervention Prostate—n = 149 Colorectal—n = 100 At least 6 weeks post-surgery |
| Maxwell-Smith et al., (2018) [40] | Control—n = 34 Female—n = 13 Male—n = 21 Intervention—n = 34 Female—n = 21 Male—n = 13 | Control = 62 ± 8 yrs Intervention = 65 ± 7 yrs | No Control Gynaecologic—n = 4 Colorectal—n = 30 Intervention Gynaecologic—n = 11 Colorectal—n = 23 Stages 1 or 2 |
| Moug et al., (2019) [36] | Control—n = 24 Female—n = 11 Male—n = 13 Intervention—n = 24 Female—n = 6 Male—n = 18 | Control = 66 ± 9 yrs Intervention = 65 ± 11 yrs | Yes New diagnosis |
| Study | -Intervention Strategy -Control -Length | Physical Activity Parameter (Dependent Variable) and Results |
|---|---|---|
| Morey et al., (2009) [34] |
| Community Health Activities Model Program for Seniors questionnaire § Control Baseline = 28.7 ± 2.3 min/wk 48 wk = 23.4 ± 5.6 min/wk Intervention Baseline = 24.6 ± 2.1 min/wk 48 wk = 36.3 ± 4.9 min/wk |
| Ligibel et al., (2012) [32] |
| 7-Day Physical Activity Recall Control Baseline = 65.7 ± 84.1 min/wk 16 wk = 14.6 ± 117.2 min/wk Intervention Baseline = 44.9 ± 58.5 min/wk 16 wk = 54.5 ± 142.0 min/wk |
| Demark-Wahnefried et al., (2012) [28] |
| Community Health Activities Model Program for Seniors questionnaire Control Baseline = 37.5 ± 3.2 min/wk 48 wk = 69.0 ± 7.8 min/wk Intervention Baseline = 33.3 ± 2.9 min/wk 48 wk = 101.1 ± 7.3 min/wk |
| Hawkes et al., (2013) [30] |
| Godin Leisure-Time Exercise Questionnaire Control Baseline = 52.0 ± 112.5 min/wk 48 wk = 54.3 ± 120.0 min/wk Intervention Baseline = 58.9 ± 132.9 min/wk 48 wk = 85.2 ± 181.0 min/wk |
| Pinto et al., (2013) [38] |
| Seven-day Physical Activity Recall Control §§ Baseline = 30 min/wk 12 wk = 146 min/wk Intervention §§ Baseline = 30 min/wk 12 wk = 88 min/wk |
| Park et al., (2015) [37] |
| Godin Leisure-Time Exercise Questionnaire Control §§ Baseline = 254.56 min/wk 4 wk = −39.05 min/wk Intervention §§ Baseline = 187.85 min/wk 4 wk = +47.57 min/wk |
| Mayer et al., (2018) [33] |
| Godin Leisure-Time Exercise Questionnaire Control Baseline = 15.49 ± 27.6 min/wk 24 wk = 40.27 ± 42.22 min/wk Intervention Baseline = 19.43 ± 27.07 min/wk 24 wk = 49.98 ± 45.28 min/wk |
| Lee et al., (2018) [31] |
| Accelerometer §§§ Control Baseline = 473.3 ± 267.3 min/wk 96 wk = 642.4 ± 294.7 min/wk Intervention Baseline = 460.8 ± 239.6 min/wk 96 wk = 680.5 ± 259.8 min/wk |
| Golsteijn et al., (2018) [29] |
| Short Questionnaire to Assess Health Enhancing Physical Activity Control Baseline = 873 ± 764 min/wk 24 wk = 943 ± 769 min/wk Intervention Baseline = 780 ± 721 min/wk 24 wk = 1145 ± 883 min/wk |
| Maxwell-Smith et al., (2018) [40] |
| Accelerometer Control §§ Baseline = 158 min/wk 12 wk = 138 min/wk Intervention §§ Baseline = 170 min/wk 12 wk = 186 min/wk |
| Moug et al., (2019) [36] |
| Accelerometer Control Baseline = 7773 ± 3975 median steps/day 12 wk = 5920 ± 3152 median steps/day Intervention Baseline = 7779 ± 4045 steps/day §§§§ 12 wk = 6675 ± 3100 steps/day §§§§ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelosi, A.C.; Rostirola, G.C.; Pereira, J.S.; Silva, K.C.; Fontanari, M.E.R.; Oliveira, M.S.P.; Reis, I.G.M.d.; Messias, L.H.D. Remote and Unsupervised Exercise Strategies for Improving the Physical Activity of Colorectal Cancer Patients: A Meta-Analysis. Healthcare 2023, 11, 723. https://doi.org/10.3390/healthcare11050723
Pelosi AC, Rostirola GC, Pereira JS, Silva KC, Fontanari MER, Oliveira MSP, Reis IGMd, Messias LHD. Remote and Unsupervised Exercise Strategies for Improving the Physical Activity of Colorectal Cancer Patients: A Meta-Analysis. Healthcare. 2023; 11(5):723. https://doi.org/10.3390/healthcare11050723
Chicago/Turabian StylePelosi, Andrea Corazzi, Gabriela Cerávolo Rostirola, Juliana Silva Pereira, Karen Christine Silva, Maria Eduarda Ramos Fontanari, Manoela Stahl Parisotto Oliveira, Ivan Gustavo Masselli dos Reis, and Leonardo Henrique Dalcheco Messias. 2023. "Remote and Unsupervised Exercise Strategies for Improving the Physical Activity of Colorectal Cancer Patients: A Meta-Analysis" Healthcare 11, no. 5: 723. https://doi.org/10.3390/healthcare11050723
APA StylePelosi, A. C., Rostirola, G. C., Pereira, J. S., Silva, K. C., Fontanari, M. E. R., Oliveira, M. S. P., Reis, I. G. M. d., & Messias, L. H. D. (2023). Remote and Unsupervised Exercise Strategies for Improving the Physical Activity of Colorectal Cancer Patients: A Meta-Analysis. Healthcare, 11(5), 723. https://doi.org/10.3390/healthcare11050723