
Management of Bilateral Quadriceps Tendon Ruptures Post Total Knee Arthroplasty by Kesler Technique Using Fiber Tape

 ,
,  and
and
Abstract
1. Introduction
2. Case Description
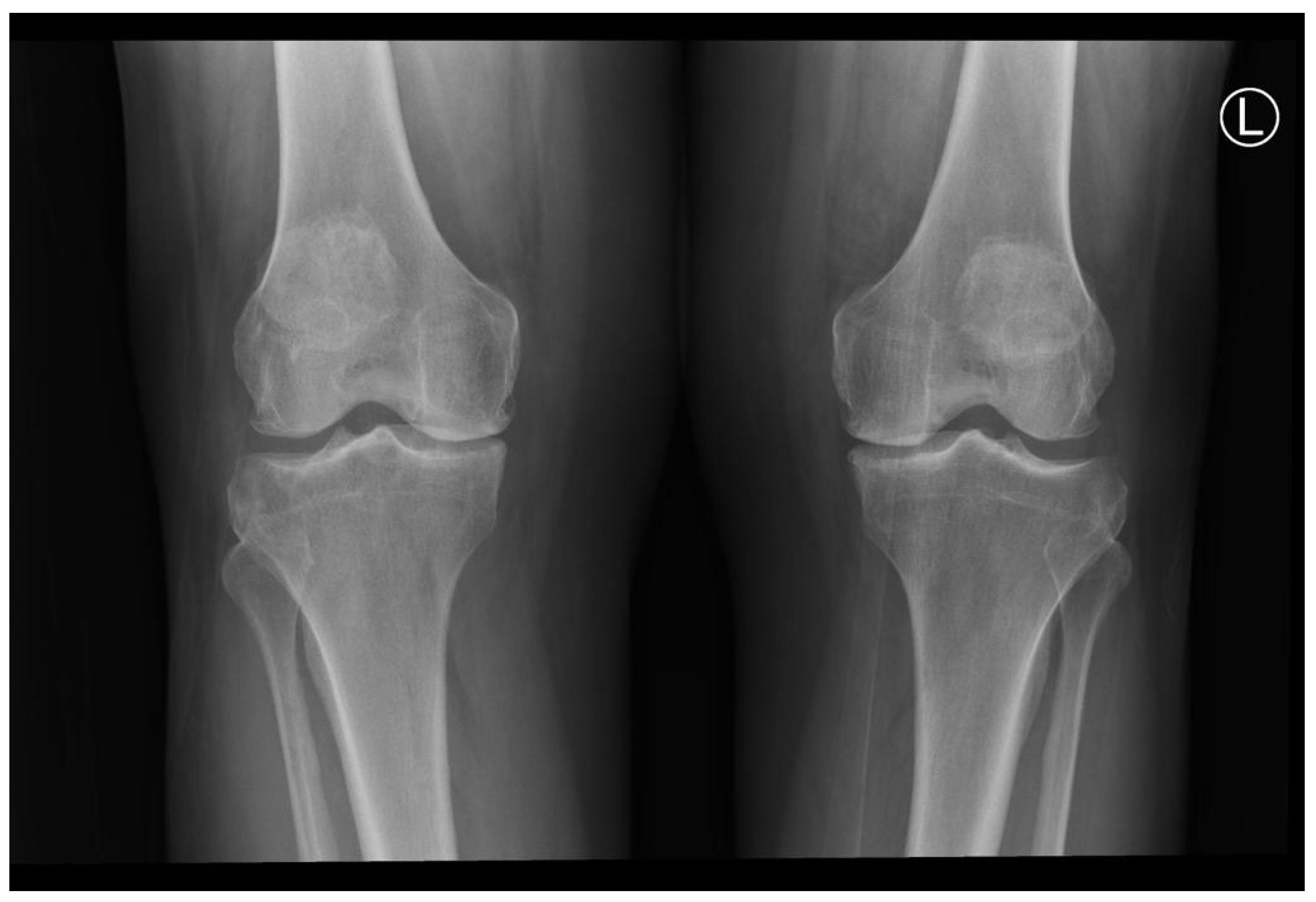
2.1. Pre-Intervention Phase
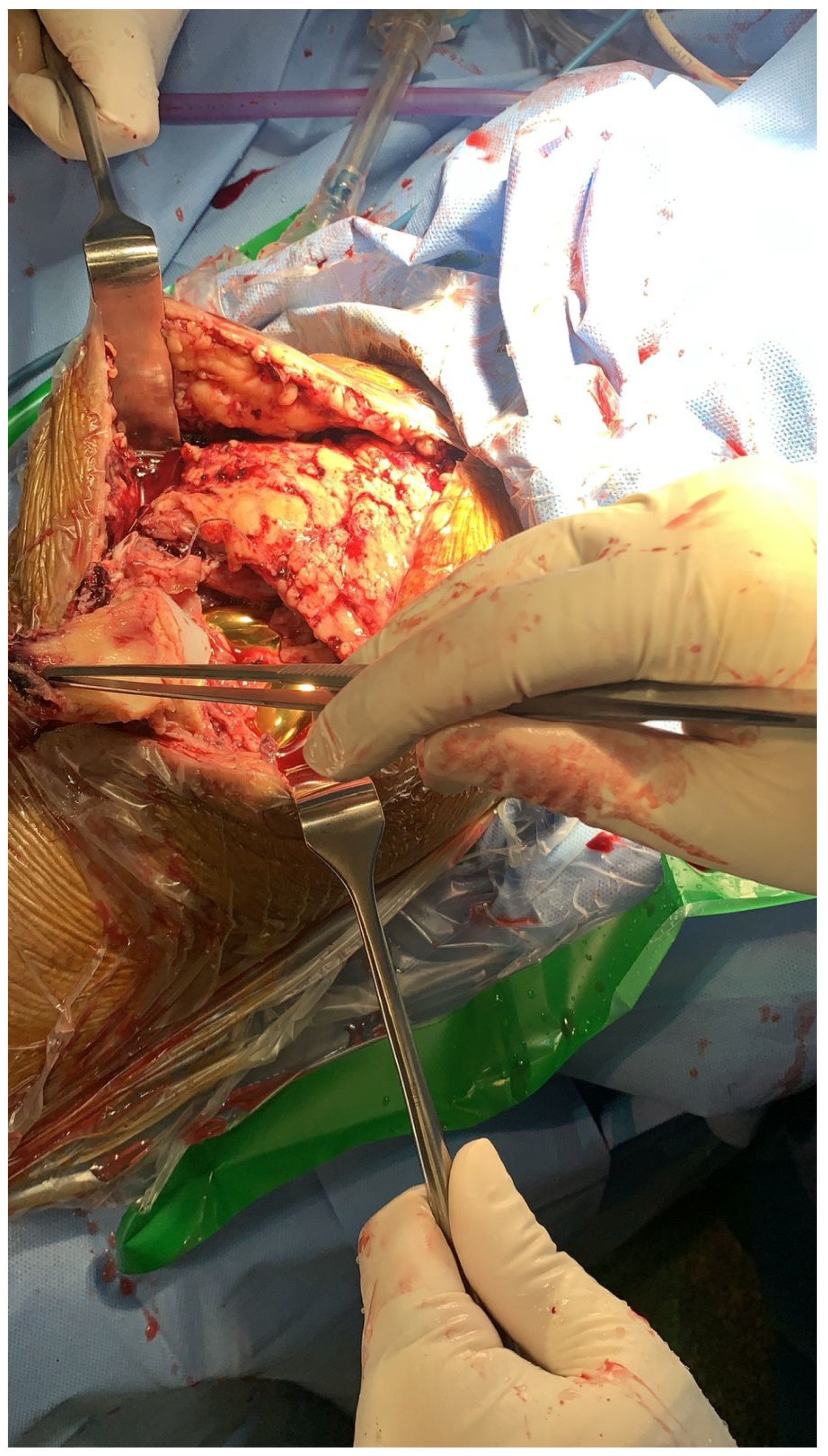
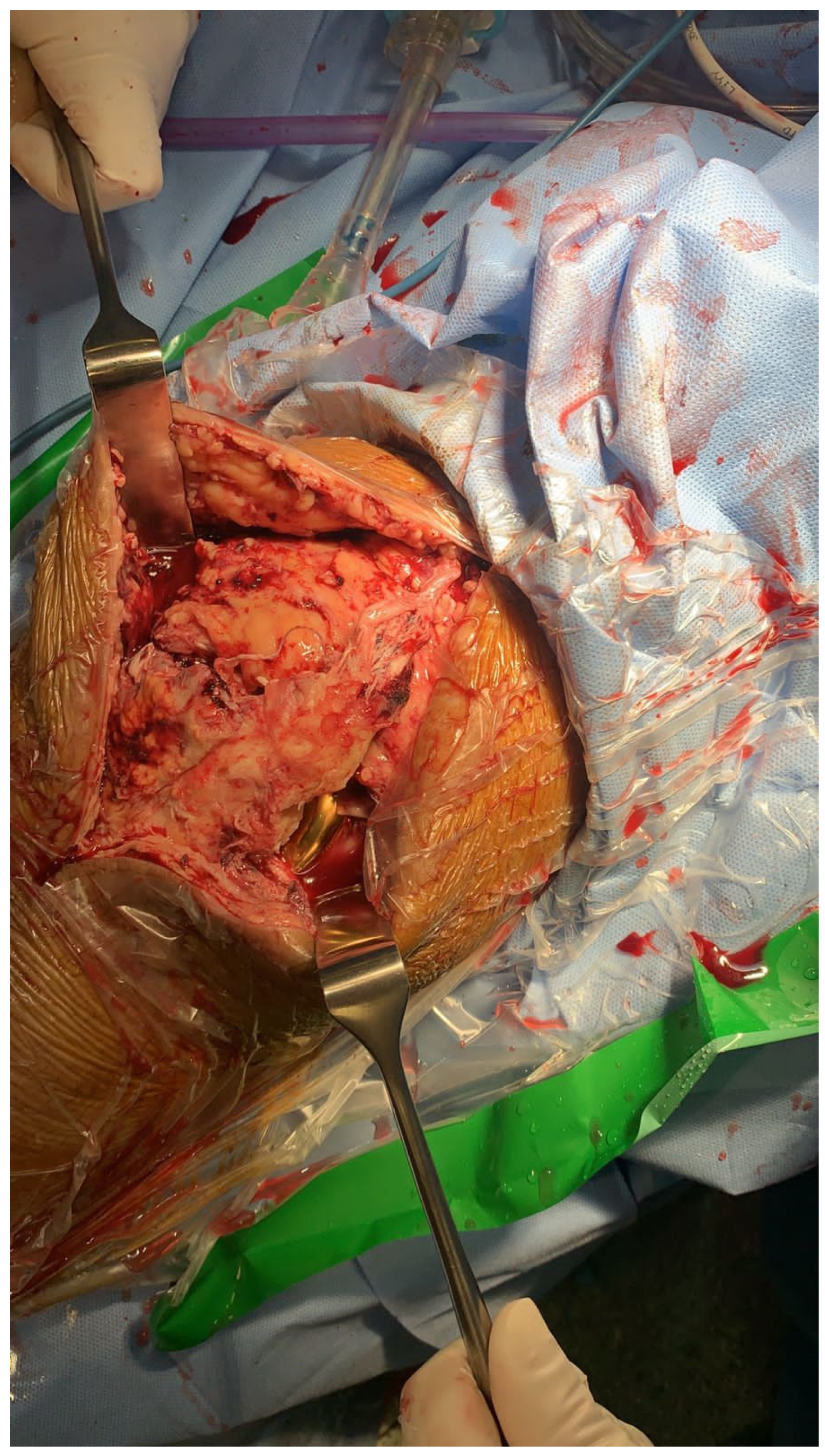
2.2. Intervention Phase
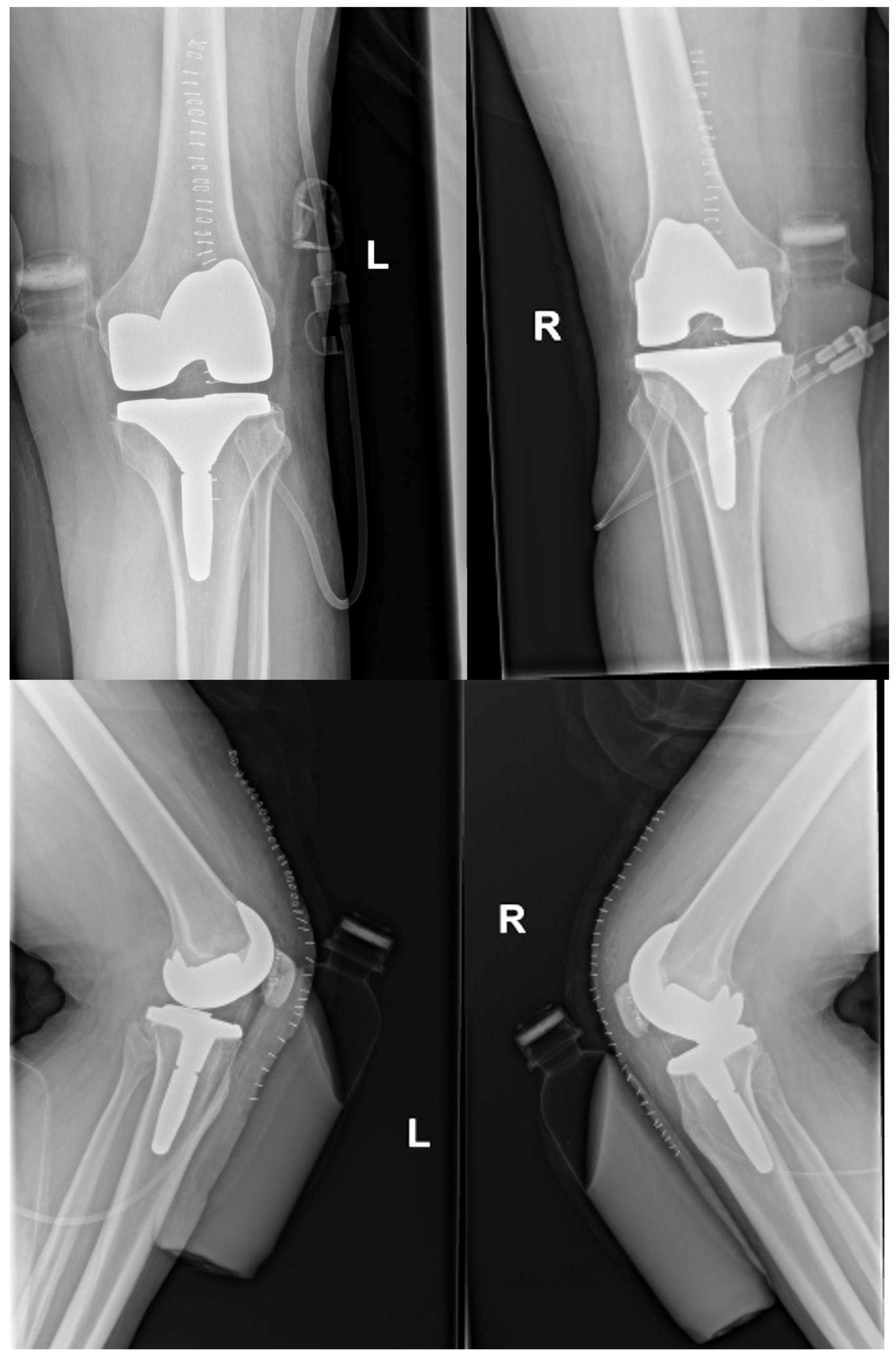
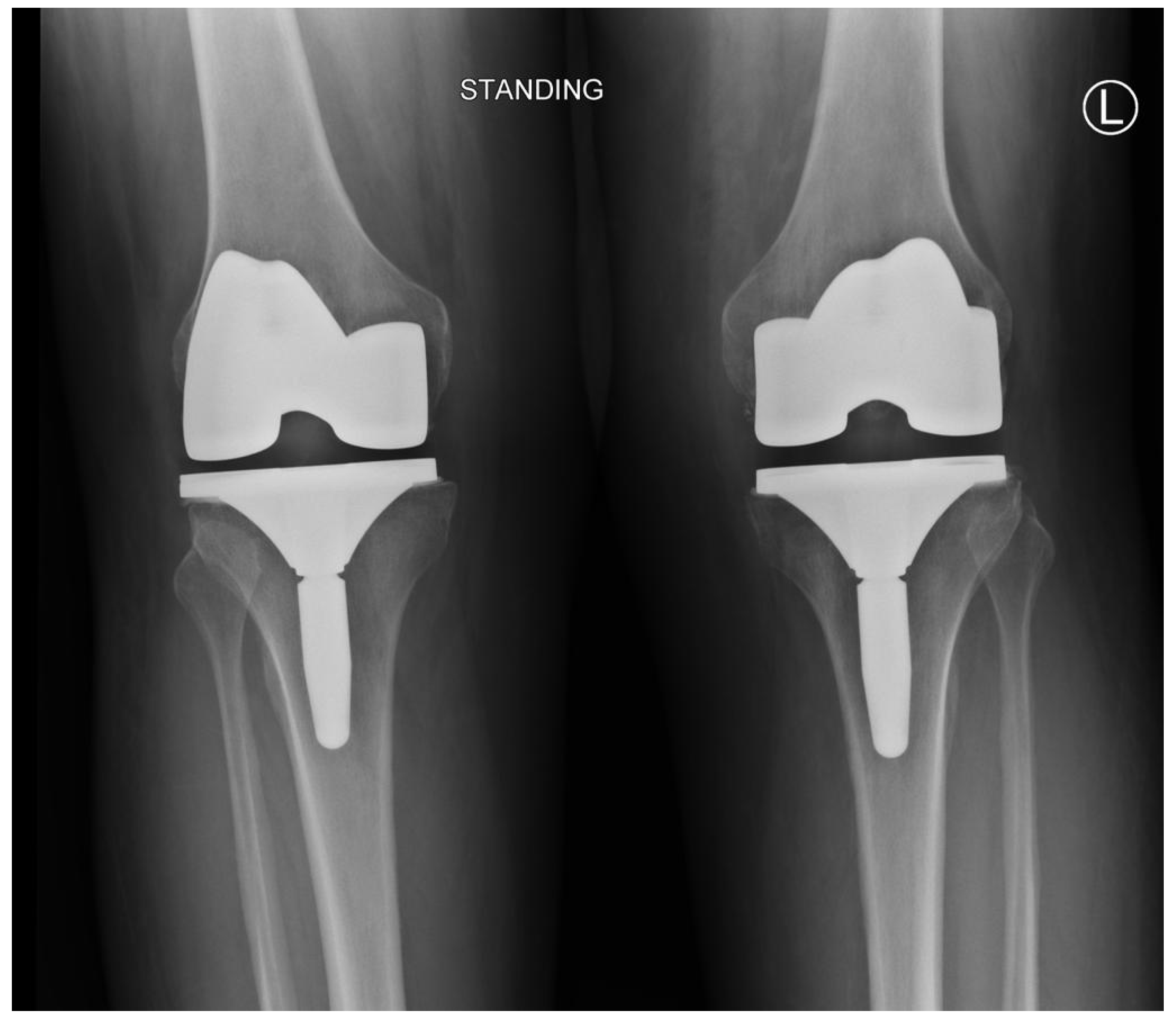
2.3. Post-Intervention Phase and the Results
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kanamoto, T.; Mae, T.; Yokoyama, T.; Tanaka, H.; Ebina, K.; Nakata, K. Significance and definition of early knee osteoarthritis. Ann. Jt. 2020, 5, 4. [Google Scholar] [CrossRef]
- Pereira, D.; Peleteiro, B.; Araujo, J.; Branco, J.; Santos, R.A.; Ramos, E. The effect of osteoarthritis definition on prevalence and incidence estimates: A systematic review. Osteoarthr. Cartil. 2011, 19, 1270–1285. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudian, A.; Lohmander, L.S.; Mobasheri, A.; Englund, M.; Luyten, F.P. Early-stage symptomatic osteoarthritis of the knee—Time for action. Nat. Rev. Rheumatol. 2021, 17, 621–632. [Google Scholar] [CrossRef] [PubMed]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- Skou, S.T.; Roos, E.M.; Laursen, M.B.; Rathleff, M.S.; Arendt-Nielsen, L.; Rasmussen, S.; Simonsen, O. Total knee replacement and non-surgical treatment of knee osteoarthritis: 2-year outcome from two parallel randomized controlled trials. Osteoarthr. Cartil. 2018, 26, 1170–1180. [Google Scholar] [CrossRef]
- Burn, E.; Weaver, J.; Morales, D.; Prats-Uribe, A.; Delmestri, A.; Strauss, V.Y.; He, Y.; Robinson, D.E.; Pinedo-Villanueva, R.; Kolovos, S.; et al. Opioid use, postoperative complications, and implant survival after unicompartmental versus total knee replacement: A population-based network study. Lancet Rheumatol. 2019, 1, e229–e236. [Google Scholar] [CrossRef]
- Ormaza, A.; Moreta, J.; Mosquera, J.; de Ugarte, O.S.; Mozos, J.L.M.D.L. Chronic quadriceps tendon rupture after total knee arthroplasty augmented with synthetic mesh. Orthopedics 2017, 40, 38–42. [Google Scholar] [CrossRef]
- Tucker, J.E.; Jones, C.R. Bilateral Quadriceps Tendon Repair with Suture Anchors: Case Series. Perm J. 2020, 24, 19.098. [Google Scholar] [CrossRef]
- Tuong, B.; White, J.; Louis, L.; Cairns, R.; Andrews, G.; Forster, B.B. Get a kick out of this: The spectrum of knee extensor mechanism injuries. Br. J. Sports Med. 2011, 45, 140–146. [Google Scholar] [CrossRef]
- Seng, C.; Lim, Y.-J.; Pang, H.N. Spontaneous disruption of the bilateral knee extensor mechanism: A report of two cases. J. Orthop. Surg. 2015, 23, 262–266. [Google Scholar] [CrossRef]
- Wu, W.; Wang, C.; Ruan, J.; Wang, H.; Huang, Y.; Zheng, W.; Chen, F. Simultaneous spontaneous bilateral quadriceps tendon rupture with secondary hyperparathyroidism in a patient receiving hemodialysis: A case report. Medicine 2019, 98, e14809. [Google Scholar] [CrossRef]
- Mine, T.; Tanaka, H.; Taguchi, T.; Ihara, K.; Moriwaki, T.; Kawai, S. Patellar tendon rupture and marked joint instability after total knee arthroplasty. Arch. Orthop. Trauma Surg. 2004, 124, 267–271. [Google Scholar] [CrossRef]
- Sharma, G.; Bagaria, V.; Nadange, S.; Waghchoure, C.; Shah, S.; Tangirala, R.; Wadia, F. Quadriceps Tendon Rupture and Contralateral Patella Tendon Avulsion Post Primary Bilateral Total Knee Arthroplasty: A Case Report. Reconstr. Rev. 2016, 6, 31–36. [Google Scholar] [CrossRef]
- Vyas, P.; Cui, Q. Management Options for Extensor Mechanism Discontinuity in Patients with Total Knee Arthroplasty. Cureus 2020, 12, e9225. [Google Scholar] [CrossRef]
- Matava, M.J. Patellar tendon ruptures. JAAOS-J. Am. Acad. Orthop. Surg. 1996, 4, 287–296. [Google Scholar] [CrossRef]
- Meyer, Z.; Ricci, W.M. Knee extensor mechanism repairs: Standard suture repair and novel augmentation technique. J. Orthop. Trauma. 2016, 30, S30–S31. [Google Scholar] [CrossRef]
- Sebastin, S.J.; Ho, A.; Karjalainen, T.; Chung, K.C. History and evolution of the Kessler repair. J. Hand. Surg. Am. 2013, 38, 552–561. [Google Scholar] [CrossRef]
- Piskin, A.; Yuceturk, A.; Tomak, Y.; Mete, O.Z.E.R.; Gulman, B.; Ataman, A.; Kangal, M.; Sahin, Y.; Desteli, E.; Taner, A.L.İ.C. Tendon repair with the strengthened modified Kessler, modified Kessler, and Savage suture techniques: A biomechanical comparison. Acta Orthop. Traumatol. Turc. 2007, 41, 238–243. [Google Scholar]
- Yoneda, S.; Okubo, H.; Linderman, S.W.; Kusano, N.; Silva, M.J.; Thomopoulos, S.; Kanaya, F.; Gelberman, R.H. The effect of modified locking methods and suture materials on Zone II flexor tendon repair—An ex vivo study. PLoS ONE 2018, 13, e0205121. [Google Scholar] [CrossRef]
- Rehman, H.; Kovacs, P. Quadriceps tendon repair using hamstring, prolene mesh and autologous conditioned plasma augmentation. A novel technique for repair of chronic quadriceps tendon rupture. Knee 2015, 22, 664–668. [Google Scholar] [CrossRef]
- Yun, A.G.; Rubash, H.E.; Scott, R.D.; Laskin, R.S. Quadriceps rupture associated with a proximal quadriceps release in total knee arthroplasty: A report of three cases. JBJS 2003, 85, 1809–1811. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, R.E.; Hanssen, A.D.; Lewallen, D.G.; Pagnano, M.W. Quadriceps tendon rupture after total knee arthroplasty: Prevalence, complications, and outcomes. JBJS 2005, 87, 37–45. [Google Scholar]
- Soong, J.W.; Silva, A.N.; Andrew, T.H.C. Disruption of quadriceps tendon after total knee arthroplasty: Case report of four cases. J Orthop Surg. 2017, 25, 2309499017717206. [Google Scholar] [CrossRef] [PubMed]
- Lynch, A.F.; Rorabeck, C.H.; Bourne, R.B. Extensor mechanism complications following total knee arthroplasty. J. Arthroplast. 1987, 2, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.; Balcells-Nolla, P.; James, P.J.; Bloch, B.V. Extensor mechanism failure in total knee arthroplasty. EFORT Open Rev. 2021, 6, 181–188. [Google Scholar] [CrossRef]
- Carlson Strother, C.R.; LaPrade, M.D.; Keyt, L.K.; Wilbur, R.R.; Krych, A.J.; Stuart, M.J. A Strategy for Repair, Augmentation, and Reconstruction of Knee Extensor Mechanism Disruption: A Retrospective Review. Orthop. J. Sport Med. 2021, 9, 23259671211046624. [Google Scholar] [CrossRef]
- Gilmore, J.H.; Clayton-Smith, Z.J.; Aguilar, M.; Pneumaticos, S.G.; Giannoudis, P.V. Reconstruction techniques and clinical results of patellar tendon ruptures: Evidence today. Knee 2015, 22, 148–155. [Google Scholar] [CrossRef]
- Alshahrani, A.A.; Tedla, J.S.; Alshehri, A.A.; Abbas, Z.Y. Management of Neglected Patellar Tendon Rupture via the Ilizarov Apparatus and Patellar Transport Following Multistage Reconstruction using Contralateral Patella Tendon Bone Autograft: A Case Study. Indian J. Orthop. 2022, 56, 933–937. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Resistance Training Characteristics | 7th Week | 8th Week | 9th Week | 10th Week | 11th Week Re-Check 1RM and Assign a New Load | 12th Week |
|---|---|---|---|---|---|---|
| Load percentages of 1RM | 40 | 50 | 60 | 70 | 50 | 60 |
| Number of repetitions | 6–8 | 8–10 | 10–12 | 12–14 | 8–10 | 10–12 |
| Number of sets * | 3 | 3 | 3 | 3 | 3 | 3 |
| Number of sessions per week | 4 | 5 | 5 | 5 | 4 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlShaafi, W.A.; Alqahtani, M.H.; Assiri, A.H.; Alqhtani, A.A.; Tedla, J.S.; Motlag, D.S. Management of Bilateral Quadriceps Tendon Ruptures Post Total Knee Arthroplasty by Kesler Technique Using Fiber Tape. Healthcare 2023, 11, 631. https://doi.org/10.3390/healthcare11050631
AlShaafi WA, Alqahtani MH, Assiri AH, Alqhtani AA, Tedla JS, Motlag DS. Management of Bilateral Quadriceps Tendon Ruptures Post Total Knee Arthroplasty by Kesler Technique Using Fiber Tape. Healthcare. 2023; 11(5):631. https://doi.org/10.3390/healthcare11050631
Chicago/Turabian StyleAlShaafi, Waleed Ahmad, Mohammed Hassan Alqahtani, Abdullah Hassan Assiri, Abdulrhman Abdullah Alqhtani, Jaya Shanker Tedla, and Dhuha Saeed Motlag. 2023. "Management of Bilateral Quadriceps Tendon Ruptures Post Total Knee Arthroplasty by Kesler Technique Using Fiber Tape" Healthcare 11, no. 5: 631. https://doi.org/10.3390/healthcare11050631
APA StyleAlShaafi, W. A., Alqahtani, M. H., Assiri, A. H., Alqhtani, A. A., Tedla, J. S., & Motlag, D. S. (2023). Management of Bilateral Quadriceps Tendon Ruptures Post Total Knee Arthroplasty by Kesler Technique Using Fiber Tape. Healthcare, 11(5), 631. https://doi.org/10.3390/healthcare11050631