
Accelerating UN Sustainable Development Goals with AI-Driven Technologies: A Systematic Literature Review of Women’s Healthcare



Abstract
1. Introduction
2. Methodology
3. Results
3.1. Cluster 1: Gender Equality
3.2. Cluster 2: Health AI
3.3. Cluster 3: Sustainable Development Goals
3.4. Cluster 4: Research Approaches
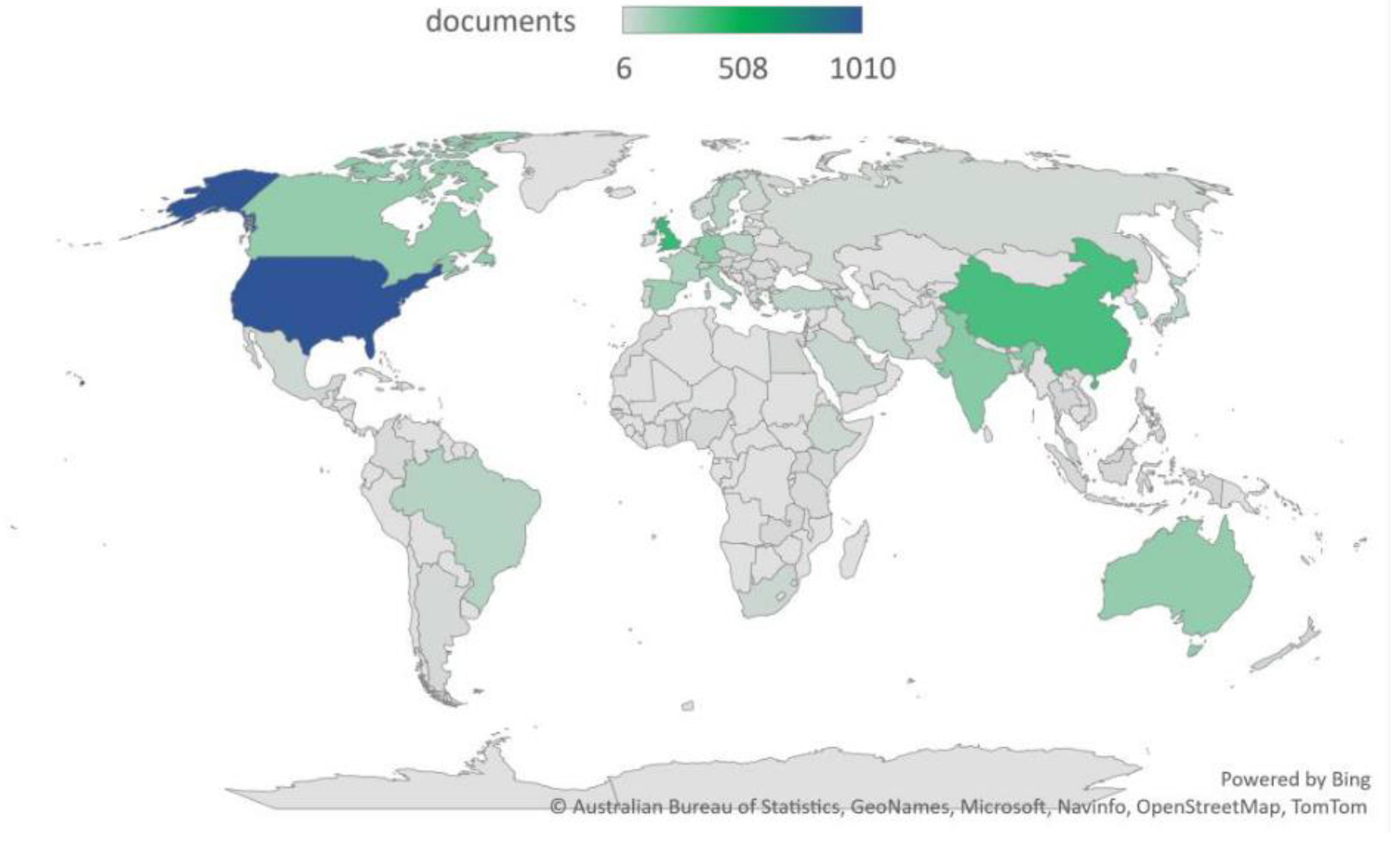
3.5. Cluster 5: Geographical Focus
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Transforming our World: The 2030 Agenda for Sustainable Development. United Nations Department of Economic and Social Affairs. 2015. Available online: https://sdgs.un.org/publications/transforming-our-world-2030-agenda-sustainable-development-17981 (accessed on 11 July 2022).
- Jha, A.; Kickbusch, I.; Taylor, P.; Abbasi, K. Accelerating achievement of the sustainable development goals. BMJ 2016, 352, i409. [Google Scholar] [CrossRef] [PubMed]
- Cleghorn, E. Unwell Women: Misdiagnosis and Myth in a Man-Made World; Dutton, Penguin Random House LLC: New York, NY, USA, 2021. [Google Scholar]
- Deziel, S. How Medical Research Has Failed Women. Chatelaine 2016. Available online: https://www.chatelaine.com/health/women-medical-research-bias/ (accessed on 17 January 2023).
- Davenport, T.; Kalakota, R. The potential for artificial intelligence in healthcare. Future Healthc. J. 2019, 6, 94. [Google Scholar] [CrossRef]
- Colombo, R.; Sanguineti, V. (Eds.) Rehabilitation Robotics, 1st ed.; Academic press: Cambridge, MA, USA, 2018. [Google Scholar]
- Vlamos, P.; Lefkimmiatis, K.; Cocianu, C.; State, L.; Luo, Z. Artificial Intelligence Applications in Biomedicine. Adv. Artif. Intell. 2013, 2013, 219137. [Google Scholar] [CrossRef]
- Lau, Y.S.A.; Staccini, P. Artificial intelligence in health: New opportunities, challenges and practical implication. Yearb. Med. Inform. 2019, 28, 174. [Google Scholar] [CrossRef]
- Vinuesa, R.; Azizpour, H.; Leite, I.; Balaam, M.; Dignum, V.; Domisch, S.; Felländer, A.; Langhans, S.D.; Tegmark, M.; Nerini, F.F. The role of artificial intelligence in achieving the Sustainable Development Goals. Nat. Commun. 2020, 11, 233. [Google Scholar] [CrossRef] [PubMed]
- Sawers, N.; Bolstar, N.; Bastewrous, A. The contribution of artificial intelligence in achieving sustainable development goals (SDG): What can eye health can learn from commercial industry and early lessons from the application of machine learning in eye health programme. Front. Public Health 2021, 9, 752049. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, K. On Intersectionality: Essential Writings; The New Press: New York, NY, USA, 2017; Available online: https://scholarship.law.columbia.edu/books/255 (accessed on 6 January 2023).
- Mustafa, F.; Lodh, S.; Nandy, M.; Kumar, V. Coupling of cryptocurrency trading with the sustainable environment goals: Is it on the cards? Bus. Strategy Environ. 2021, 31, 1152–1168. [Google Scholar] [CrossRef]
- Tomas, B.A.; Christopher, P.; Cavanillas, A.B.; Solvas, J.G.; Pool, R.; Roura, M. Tuberculosis in Migrant Population. A systematic review of the qualitative literature. PLoS ONE 2013, 8, e82440. [Google Scholar] [CrossRef]
- Schaap, R.; Wind, A.D.; Coenen, P.; Proper, K.; Boot, C. The effects of exit from work on health across different socioeconomic groups: A systematic literature review. Soc. Sci. Med. 2018, 198, 36–45. [Google Scholar] [CrossRef]
- King, T.L.; Kavanagh, A.; Scovelle, A.J.; Milner, A. Associations between gender equality and health: A systematic review. Health Promot. Int. 2020, 35, 27–41. [Google Scholar] [CrossRef]
- Gupta, G.R.; Oomman, N.; Grown, C.; Conn, K.; Hawkes, S.; Shawar, Y.R.; Shiffman, J.; Buse, K.; Mehra, R.; Bah, C.A.; et al. Gender Equality, Norms, and Health Steering Committee. Gender equality and gender norms: Framing the opportunities for health. Lancet 2019, 393, 2550–2562. [Google Scholar] [CrossRef] [PubMed]
- Greene, M.E.; Patton, G. Adolescence and Gender Equality in Health. J. Adolesc. Health 2019, 66, S1–S2. [Google Scholar] [CrossRef] [PubMed]
- Heise, P.L.; Green, M.E.; Opper, N.; Stavropoulou, M.; Harper, C.; Nascimento, M.; Zewdie, D. Gender inequality and restrictive gender norms: Framing the challenges to health. Lancet 2019, 393, 2440–2454. [Google Scholar] [CrossRef] [PubMed]
- Benyamini, Y.; Todorova, I. Women’s Reproductive Health in Sociocultural Context. Int. J. Behav. Med. 2017, 24, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Mustanski, B.; Van Wagenen, A.; Birkett, M.; Eyster, S.; Corliss, H.L. Identifying sexual orientation health disparities in adolescents: Analysis of pooled data from the Youth Risk Behavior Survey, 2005 and 2007. Am. J. Public Health 2014, 104, 211–217. [Google Scholar] [CrossRef]
- Leonardi, M.; Frecker, H.; Scheim, A.I.; Kives, S. Reproductive Health Considerations in Sexual and/or Gender Minority Adolescents. J. Pediatr. Adolesc. Gynecol. 2018, 32, 15–20. [Google Scholar] [CrossRef]
- Denno, D.M.; Hoopes, A.J.; Chandra-Mouli, V. Effective strategies to provide adolescent sexual and reproductive health services and to increase demand and community support. J. Adolesc. Health 2015, 56 (Suppl. S1), S22–S41. [Google Scholar] [CrossRef] [PubMed]
- Oram, S.; Khalifeh, H.; Howard, L.M. Violence against women and mental health. Lancet Psychiatry 2017, 4, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Barker, L.C.; Stewart, D.E.; Vigod, S.N. Intimate Partner Sexual Violence: An Often-Overlooked Problem. J. Womens Health 2019, 28, 363–374. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report—2000. Health Systems: Improving Performance. Available online: https://www.who.int/whr/2000/en/whr00_en.pdf (accessed on 20 August 2022).
- Waechter, R. Prevention of Sexual Violence in America: Where Do We Stand? Am. J. Public Health 2021, 111, 339–341. [Google Scholar] [CrossRef]
- Malmusi, D.; Vives, A.; Benach, J.; Borrell, C. Gender inequalities in health: Exploring the contribution of living conditions in the intersection of social class. Glob. Health Action 2014, 7, 23189. [Google Scholar] [CrossRef] [PubMed]
- Suls, J.; Rothman, A. Evolution of the biopsychosocial model: Prospects and challenges for health psychology. Health Psychol. 2004, 23, 119. [Google Scholar] [CrossRef] [PubMed]
- Sánchez–López, M.D.P.; Cuellar–Flores, I.; Dresch, V. The impact of gender roles on health. Women Health 2012, 52, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Gonzalo, S.; Aparicio, M.; Estaban-Gonzalo, L. Employment status, gender and health in Spanish women. Women Health 2018, 58, 744–758. [Google Scholar] [CrossRef] [PubMed]
- Banda, P.C.; Odimegwu, C.O.; Ntoimo, L.F.; Muchiri, E. Women at risk: Gender inequality and maternal health. Women Health 2017, 57, 405–429. [Google Scholar] [CrossRef] [PubMed]
- Stenberg, K.; Axelson, H.; Sheehan, P.; Anderson, I.; Gülmezoglu, A.M.; Temmerman, M.; Jamison, D.; Bustreo, F. Study Group for the Global Investment Framework for Women’s Children’s Health. Advancing social and economic development by investing in women’s and children’s health: A new Global Investment Framework. Lancet 2014, 383, 1333–1354. [Google Scholar] [CrossRef]
- United Nation’s International Children’s Emergency Fund. The UNICEF Health System Strengthening Approach 2016. Available online: http://www.unicef.org (accessed on 11 December 2022).
- Sumner, A. Global Poverty and the ‘New Bottom Billion’ Revisited: Why Are Some People Poor? Working paper; King’s College: Hong Kong, China, 2016. [Google Scholar]
- United Nation’s International Children’s Emergency Fund. UNICEF Data: Monitoring the Situation of Children and Women 2019; United Nations Children’s Fund: New York, NY, USA, 2019; Available online: https://data.unicef.org/ (accessed on 8 January 2023).
- Costello, A.; Naimy, Z. Maternal, newborn, child and adolescent health: Challenges for the next decade. Int. Health 2019, 11, 349–352. [Google Scholar] [CrossRef]
- Blanchet, K.; Ramesh, A.; Frison, S.; Warren, E.; Hossain, M.; Smith, J.; Knight, A.; Post, N.; Lewis, C.; Woodward, A.; et al. Evidence on public health interventions in humanitarian crises. Lancet 2017, 309, 2287–2296. [Google Scholar] [CrossRef]
- World Health Organization. Quality, Equity, Dignity: The Network to Improve Quality of Care for Maternal, Newborn and Child Health—Strategic Objectives; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/maternal_child_adolescent/documents/quality-care-network-objectives/en/ (accessed on 7 January 2023).
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Viner, R.M. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef]
- World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to Support Country Implementation. 2017. Available online: https://www.who.int/maternal_child_adolescent/topics/adolescence/framework-accelerated-action/en/ (accessed on 7 January 2023).
- Cazottes, I.; Costello, A.; Davis, J.; George, A.; Houeto, D.; Howard-Grabman, L.; Soerachman, R. WHO Recommendation on Community Mobilization through Facilitated Participatory Learning and Action Cycles with Women’s Groups for Maternal and Newborn Health; WHO: Geneva, Switzerland, 2014; ISBN 978 92 4 150727 1. Available online: http://www.who.int (accessed on 12 December 2022).
- More, N.S.; Das, S.; Bapat, U.; Alcock, G.; Manjrekar, S.; Kamble, V.; Osrin, D. Community resource centres to improve the health of women and children in informal settlements in Mumbai: A cluster-randomised, controlled trial. Lancet Glob. Health 2017, 5, e335–e349. [Google Scholar] [CrossRef]
- Fottrell, E.; Ahmed, N.; Morrison, J.; Kuddus, A.; Shaha, S.K.; King, C.; Jennings, H.; Akter, K.; Nahar, T.; Haghparast-Bidgoli, H.; et al. Community groups or mobile phone messaging to prevent and control type 2 diabetes and intermediate hyperglycaemia in Bangladesh (DMagic): A cluster-randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Yousafzai, A.K.; Rasheed, M.A.; Rizvi, A.; Armstrong, R.; Bhutta, Z.A. Effect of integrated responsive stimulation and nutrition interventions in the Lady Health Worker programme in Pakistan on child development, growth, and health outcomes: A cluster-randomised factorial effectiveness trial. Lancet 2014, 384, 1282–1293. [Google Scholar] [CrossRef] [PubMed]
- Pickering, A.J.; Djebbari, H.; Lopez, C.; Coulibaly, M.; Alzua, M.L. Effect of a community-led sanitation intervention on child diarrhoea and child growth in rural Mali: A cluster-randomised controlled trial. Lancet Glob. Health 2015, 3, e701–e711. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.S.; Goswami, R.; Raval, Y.J.; Marawi, S. Challenges and opportunities of big data in health care: A systematic review. JMIP Med. Inf. 2016, 4, E38. [Google Scholar] [CrossRef]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.; Guo, X.; Peng, Z.; Ye, Q.; Lai, K.-H. Trust and elderly user’s continuance intention regarding mobile health services: The contingent role of health and technology anxieties. Inf. Technol. People 2021, 35, 259–280. Available online: http://doi.org/10.1108/ITP-11-2019-0602 (accessed on 12 January 2023). [CrossRef]
- Gertrudes, J.C.; Maltarollo, V.G.; Silva, R.A.; Oliveira, P.R.; Honorio, K.M.; Da Silva, A.B.F. Machine learning techniques and drug design. Curr. Med. Chem. 2012, 19, 4289–4297. [Google Scholar] [CrossRef] [PubMed]
- Alimadadi, A.; Aryal, S.; Manandhar, I.; Munroe, P.B.; Joe, B.; Cheng, X. Artificial intelligence and machine learning to fight COVID-19. Physiol. Genom. 2020, 52, 200–202. [Google Scholar] [CrossRef]
- Gerke, S.; Minssen, T.; Cohen, G. Ethical and legal challenges of artificial intelligence-driven healthcare. In Artificial Intelligence in Healthcare, 1st ed.; Bohr, A., Memarzad, K., Eds.; Academic Press: Cambridge, MA, USA, 2020; eBook ISBN: 978012818439, Paperback ISBN: 9780128184387. [Google Scholar]
- van Kolfschooten, H. EU Regulation of Artificial Intelligence: Challenges for Patients ‘Rights’, EU regulation of artificial intelligence: Challenges for patients ‘rights’. Common Mark. Law Rev. 2022, 59, 81–112. [Google Scholar] [CrossRef]
- Lee, L.S.; Chan, P.K.; Wen, C.; Fung, W.C.; Cheung, A.; Chan, V.W.K.; Cheung, M.H.; Fu, H.; Yan, C.H.; Chiu, K.Y. Artificial intelligence in diagnosis of knee osteoarthritis and prediction of arthroplasty outcomes: A review. Arthroplasty 2022, 4, 16. [Google Scholar] [CrossRef]
- Manandhar, M.; Hawkes, S.; Buse, K.; Nosrati, E.; Magar, V. Gender, health and the 2030 agenda for sustainable development. Bull. World Health Organ. 2018, 96, 644–653. [Google Scholar] [CrossRef] [PubMed]
- WHO. Fact Sheet No. 31 on the Right to Health; The Office of the United Nations High Commissioner for Human Rights; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Blundell, R.; Dias, M.C.; Joyce, R.; Xu, X. COVID-19 and inequalities. J. Appl. Public Econ. 2020, 41, 291–319. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.D.; Morrison, R.S. Study design, precision, and validity in observational studies. J. Palliat. Med. 2009, 12, 77–82. [Google Scholar] [CrossRef]
- Kabisch, M.; Ruckes, C.; Seibert-Grafe, M.; Blettner, M. Randomized controlled trials: Part 17 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2011, 108, 663–668. [Google Scholar] [CrossRef]
- ICH E6. London UK: International Conference on Harmonization 1996. Guideline for Good Clinical Practice. CPMP/ICH/135/95, European Medicines Agency. Available online: http://www.ema.europe.eu (accessed on 4 January 2023).
- Patsopoulos, N.A.; Analatos, A.A.; Ioannidis, J.P. Relative citation impact of various study designs in the health sciences. J. Am. Med. Assoc. 2005, 293, 2362–2366. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Sackett, D.L.; Sinclair, J.C.; Hayward, R.; Cook, R.J.; Bass, E.; Gerstein, H.; Haynes, B.; Holbrook, A.; Jaeschke, R.; et al. Users’ guides to the medical literature: IX. A method for grading health care recommendations. J. Am. Assoc. 1995, 274, 1800–1804. [Google Scholar] [CrossRef]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.J.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial intelligence in cancer imaging: Clinical challenges and applications. CA A Cancer J. Clin. 2019, 69, 127–157. [Google Scholar] [CrossRef] [PubMed]
- Madan, N.; Lucas, J.; Akhter, N.; Collier, P.; Cheng, F.; Guha, A.; Zhang, L.; Sharma, A.; Hamid, A.; Ndiokho, I.; et al. Artificial intelligence and imaging: Opportunities in cardio-oncology. Am. Heart J. Plus Cardiol. Res. Pract. 2022, 15, 100126. [Google Scholar] [CrossRef]
- Danesi, C.C. The Impact of Artificial Intelligence on Women’s Rights: A Legal Point of View. In The Fourth Industrial Revolution and Its Impact on Ethics; Miller, K., Wendt, K., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 267–282. [Google Scholar] [CrossRef]
- Food and Drug Administration. FDA releases Artificial Intelligence/Machine Learning Action Plan. U.S. Food & Drug Administration. 2021. Available online: https://www.fda.gov/news-events/press-announcements/fda-releases-artificial-intelligencemachine-learning-action-plan (accessed on 13 July 2022).
- Salaffi, F.; Cimmino, M.A.; Malavolta, N.; Carotti, M.; Di Matteo, L.; Scendoni, P.; Grassi, W. Italian multicentre osteoporotic fracture study group. The burden of prevelent fracture on health-related quality of life in postmenoausal women with osteoporosis: The IMOF study. J. Rheumatol. 2007, 34, 1551–15601. [Google Scholar]
- Stahl, B.C.; Rodrigues, R.; Santiago, N.; Macnish, K. A European Agency for Artificial Intelligence: Protecting fundamental rights and ethical values. Comput. Law Secur. Rev. 2022, 45, 105661. [Google Scholar] [CrossRef]
- Tachmazidis, I.; Chen, T.; Adamou, M.; Antoniou, G. A hybrid AI approach for supporting clinical diagnosis of attention deficit hyperactivity disorder (ADHD) in adults. Health Inf. Sci. Syst. 2021, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Teji, J.S.; Jain, S.; Gupta, S.K.; Suri, J.S. NeoAI 1.0: Machine learning-based paradigm for prediction of neonatal and infant risk of death. Comput. Biol. Med. 2022, 147, 105639. [Google Scholar] [CrossRef] [PubMed]
- Kaur, P.; Singh, A.; Chana, I. BSense: A parallel Bayesian hyperparameter optimized Stacked ensemble model for breast cancer survival prediction. J. Comput. Sci. 2022, 60, 101570. [Google Scholar] [CrossRef]
- Xu, Y.; Liu, X.; Pan, L.; Mao, X.; Liang, H.; Wang, G.; Chen, T. Explainable Dynamic Multimodal Variational Autoencoder for the prediction of patients with suspected central precocious puberty. IEEE J. Biomed. Health Inform. 2022, 26, 1362–1373. [Google Scholar] [CrossRef] [PubMed]
- O’meara, S. The robot recruits in China’s healthcare system. Nature 2022, 582, S49–S51. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greenland, S.; Lash, T.L. Modern Epidemiology; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; Volume 3. [Google Scholar]
- Davidson, L.; Boland, M.R. Enabling pregnant women and their physicians to make informed medication decisions using artificial intelligence. J. Pharmacokinet. Pharmacodyn. 2020, 47, 305–318. [Google Scholar] [CrossRef]
- Balsamo, A. Technologies of the Gendered Body: Reading Cyborg Women; Duke University Press: Durham, NC, USA, 1995. [Google Scholar]
- World Health Organisation. Universal Health Coverage for Sexual and Reproductive Health in Ghana 2021, Available in Universal Health Coverage for Sexual and Reproductive Health in Ghana: Evidence Brief, WHO. Available online: http://www.who.int (accessed on 1 January 2023).
- Richardson, S.S.; Reiches, M.W.; Bruch, J.; Boulicault, M.; Noll, N.E.; Shattuck-Heidorn, H. Is There a Gender-Equality Paradox in Science, Technology, Engineering, and Math (STEM)? Commentary on the Study by Stoet and Geary. Psychol. Sci. 2020, 31, 338–341. [Google Scholar] [CrossRef]
- OECD. The OECD Artificial Intelligence (AI) Principles 2021. Available online: https://oecd.ai/en/ai-principles (accessed on 13 July 2022).
- Singapore Model Artificial Intelligence Governance Framework Second Edition, 2020, Personal Data Protection Commission Singapore. Available online: http://www.pdpc.gov.sg/help-and-resource (accessed on 2 January 2023).




{kind=link}
{kind=link}
{kind=link}
| Cluster | Thematic Marker | Keywords |
|---|---|---|
| 1. Gender Equality | Women Other gender Age Socioeconomic factors | Female adults, health care personnel, empowerment, child health, maternal mortality, childhood mortality, sexual orientation, newborn, infant, child, adolescent, young adults, middle-aged, very elderly, mortality, prenatal care, healthcare cost, nursing, workforce, quality of life, health insurance and health promotion, social support, government, poverty, leadership, patient care, social policy |
| 2. Health AI | Types of AI in health Gender Techniques of AI | Epidemiology, mental health, COVID-19, pregnancy, depression, prenatal care, cancer, artificial intelligence, female, prevention and control, retrospective study, machine learning, gender disparity |
| 3. Sustainable Development Goals | SDG 3 SDG 5 | Public health, health care delivery, healthcare services, healthcare policy, WHO, well-being, global health, quality of life, occupational health, equal participation; female adult, female, human rights |
| 4. Research Approaches | Medical science Social science Other | Controlled study, major clinical study, cross-sectional study, qualitative research, health survey, outcome assessment, randomized controlled trial, quantitative analysis, thematic analysis, clinical trial, statistics and numerical data, cohort study, meta- analysis. |
| 5. Geographical Focus | Developed countries Developing and emerging countries | United States of America, China, United Kingdom, India, Ghana, rural population, middle-income country, Nigeria, Africa |
| Keywords | Total Documents | Total Citation | % Document | % Citation |
|---|---|---|---|---|
| Equal participation | 45 | 97 | 27.27 | 24.12 |
| Empowerment | 32 | 82 | 19.39 | 20.39 |
| Violence and sexual exploitation | 28 | 101 | 16.69 | 25.12 |
| Public policy | 60 | 122 | 36.36 | 14.92 |
| Keywords | Total Documents | Total Citation | % Document | % Citation |
|---|---|---|---|---|
| Newborns and infants | 23 | 143 | 17.69 | 24.69 |
| Child | 11 | 89 | 8.46 | 15.37 |
| Adolescent | 35 | 159 | 26.92 | 27.46 |
| Young adults | 39 | 111 | 30 | 5.18 |
| Middle age | 9 | 56 | 6.92 | 9.67 |
| Very elderly | 13 | 21 | 16.15 | 3.62 |
| Keywords | Total Documents | Total Citation | % Documents | % Citation |
|---|---|---|---|---|
| Global health | 62 | 111 | 34.44 | 25.28 |
| Quality of life | 53 | 130 | 29.44 | 29.61 |
| Artificial intelligence | 35 | 97 | 19.45 | 22.09 |
| Machine learning | 30 | 101 | 16.66 | 6.83 |
| Keywords | Total Documents | Total Citation | % Documents | % Citation |
|---|---|---|---|---|
| Public health | 82 | 187 | 57.74 | 41.09 |
| Equal participation | 62 | 124 | 43.63 | 27.25 |
| Human rights | 59 | 144 | 29.35 | 31.64 |
| Keywords | Total Documents | Total Citation | % Document | % Citation |
|---|---|---|---|---|
| Cohort study | 43 | 111 | 45.26 | 27.07 |
| Meta-analysis | 17 | 131 | 17.89 | 31.56 |
| Randomized controlled trial (RCT) | 35 | 168 | 36.84 | 37.25 |
| Keywords | % Document | % Citation | Total Link Strength |
|---|---|---|---|
| United States of America (USA) | 23.31 | 28.11 | 61,101 |
| Canada | 8.21 | 13.33 | 42,759 |
| United Kingdom (UK) | 14.83 | 11.11 | 45,297 |
| East Asia | 9.01 | 7.22 | 42,115 |
| South East Asia | 27.15 | 25.79 | 21,479 |
| Scandinavian, Central, and South European countries | 4.83 | 3.22 | 10,433 |
| Australia and New Zealand | 3.78 | 3.77 | 17,837 |
| Central Asia | 6.44 | 4.13 | 25,357 |
| Latin America | 3.18 | 2.49 | 20,033 |
| Africa | 3.21 | 1.01 | 20,071 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, P.L.; Nandy, M.; Chakraborty, S. Accelerating UN Sustainable Development Goals with AI-Driven Technologies: A Systematic Literature Review of Women’s Healthcare. Healthcare 2023, 11, 401. https://doi.org/10.3390/healthcare11030401
Lau PL, Nandy M, Chakraborty S. Accelerating UN Sustainable Development Goals with AI-Driven Technologies: A Systematic Literature Review of Women’s Healthcare. Healthcare. 2023; 11(3):401. https://doi.org/10.3390/healthcare11030401
Chicago/Turabian StyleLau, Pin Lean, Monomita Nandy, and Sushmita Chakraborty. 2023. "Accelerating UN Sustainable Development Goals with AI-Driven Technologies: A Systematic Literature Review of Women’s Healthcare" Healthcare 11, no. 3: 401. https://doi.org/10.3390/healthcare11030401
APA StyleLau, P. L., Nandy, M., & Chakraborty, S. (2023). Accelerating UN Sustainable Development Goals with AI-Driven Technologies: A Systematic Literature Review of Women’s Healthcare. Healthcare, 11(3), 401. https://doi.org/10.3390/healthcare11030401