

Developing a Theory of Community Caring for Public Health Nursing

Abstract
1. Introduction
1.1. Valuing the Community Caring Nursing Theory
1.2. Caring in Nursing Communities and a Community of Caring
1.3. Purpose
2. Developing the Theory of CCPHN
2.1. Motivation to Develop the Theory
2.2. Review of the Literature for Developing the Theory of CCPHN

{kind=link}
{kind=link}
| Reference | Research Design | Aim of the Study | Key Findings |
|---|---|---|---|
| Pindus et al. [42] | Systematic review and meta-ethnography | To describe and explain stroke survivors’ and informal caregivers’ experiences of primary care and community healthcare services. To offer potential solutions for how negative experiences could be addressed by healthcare services. | Stroke survivors and caregivers feel abandoned because they have become marginalized by services, and they do not have the knowledge or skills to re-engage. This can be addressed by increasing stroke-specific health literacy through targeted and timely information provision and improving continuity of care between specialist and generalist services. |
| Gilmore et al. [43] | Rapid evidence review | To identify what approaches and community actors are involved, what interventions are conducted, who the target groups of community engagement are and how equity considerations are incorporated, what the linkages and relationship with other health system stakeholders are, and what the main implementation considerations for successful community engagement for infectious disease prevention and control are. | This rapid review highlights the main community engagement actors and approaches and the interventions that they conduct within the prevention and control of the infectious disease. This review also notes the lack of documented community engagement activities in high-income countries. Well-implemented community engagement strategies can support the design of interventions, building trust, and community entry, social and behavioral change communication, risk communication, surveillance and contract tracing, and logistical and administrative support during COVID-19 prevention and control responses. |
| Williams et al. [44] | These coalitions were randomized to one of two approaches (community resilience or preparedness) | To clarify a social network survey to measure the number, type, and quality of relationships among organizations participating in 16 coalitions brought together to address community resilience in the Los Angeles Community Disaster Resilience project. | The community resilience coalitions were initially larger and had lower trust among members than the preparedness communities. Over time, these trust differences dissipated. While both coalitions grew, the resilience community coalitions maintained their size difference throughout the project. We also found differences in the types of activities implemented by the resilience communities; these differences were directly related to the training provided. |
| Tsuruta et al. [45] | A cross-sectional study | To examine the relationship between social capital and happiness in a community with the lowest National Health Insurance expenditures in Japan. | A positive relationship between social capital and happiness concerning all three factors of social capital (trust, connections, interaction, and social participation). |
| Kawasaki et al. [47] | Qualitative descriptive research | To describe public health nurses’ (PHNs) experiences in caring for people in their communities during the recovery stage of the Fukushima nuclear accident. | The PHNs supported and cared for people in their communities, driven by their compelling sense of mission even in the absence of correct information and sufficient knowledge. They spoke of being heartbroken and barely able to face the reality of the impact of the accident. PHNs supported people because of a compelling sense of mission, yet it was a great burden. |
| Zerwekh [31] | Phenomenological approach | To learn anew the world of caring, not that previously encoded. | Fear and silencing keep us from “rising up” at all levels of organization and community; the truth is rarely spoken to power for fear of repercussions. As nurses, by strengthening individual clients, we enhance the possibility of them acting as empowered communities. Nurses can validate, explain, teach, and replicate fearless caring with clients subject to innumerable societal injustices and fears. As the gap between rich and poor widens, a unique group of outstanding nurse colleagues persistently struggles to affirm humanity and build the individual capacity of the most disadvantaged. They draw them into communities where there is strength in numbers. They see human possibilities where others see no hope. Thus, power is born when caring for others, valuing another, and believing in human potential. Experiencing concern and unconditional regard, the patient’s self-love and self-regard gradually increase. |
| Parker and Barry’s [23,47] | Theoretical paper | To describe the application of a community nursing practice model to school nursing. | The first concentric circle includes persons and groups in each school or community, such as parent/teacher organizations, who share their concern for the well-being of the persons being served. The categories of care that comprise the first circle are consultation and collaboration and appraisal and evaluation. The second circle includes structured and organized groups within a wider range or jurisdiction, such as a district- or county-level organization, which also share a concern for the well-being of persons being served. The categories of care include consultation and collaboration as research and evaluation. The third circle reaches out to state, regional, national, and international organization members from whom consultation, collaboration, appraisal, and evaluation are sought. |
| Pope et al. [33] | Theoretical paper | To explore ethics in community practice with the principles of caring, beneficence, autonomy, advocacy, and social justice. | The ethical principles of beneficence, autonomy, advocacy, and social justice in community nursing were discussed from the lens of caring. Caring in nursing practice must work to protect a community’s right to autonomy. Conscious participation by nursing policymakers on ethical questions related to healthcare decisions expands the scope of a caring nursing practice and benefits communities as well as individuals. The community discourse addressing issues directly related to patient autonomy, access to healthcare, and resource allocation is within the scope of this practice. |
| Falk-Rafael [49] | Theoretical paper | To examine and congruence of critical caring theory with public health nursing practice. | Congruence between expert public health nursing practice and the theory in terms of caring/social justice ethics that underpins practice and the relevance to their practice of the carative health-promoting process of contributing to the creation of supportive and sustainable physical, social, political, and economic environments. PHNs encountered many barriers to a practice underpinned by a caring/social justice ethic, some limiting their moral agency. |
| Chinn, P.L.; Falk-Rafael, A. [50] | Theoretical paper | To present a theoretical model that grounds teaching and learning in nursing on the focus, values, and ideals of nursing as a discipline. | The critical caring pedagogy model was formed by integrating Falk-Rafael’s theory of critical caring in public health nursing, Noddings’ philosophy of caring education, and Chinn’s theory of peace and power. This model of critical caring pedagogy was developed by a logical analysis of the three organizing constructs and the conceptual relationships between and among these constructs. When nurse educators ground teaching and learning practice in nursing’s own theoretical and philosophic foundation, they teach nursing in powerful ways that show nursing values and ideals through action, revealing deeper meanings of the words that form texts, lectures, and objectives set forth in a curriculum outline. |
| Falk-Rafael, A. [51] | Qualitative exploratory study | To identify their conceptualization of empowerment, the strategies they identified as empowering, and the outcomes of empowering strategies they observed in their practice. | Active participation of the client in their empowerment was essential; they asserted that they could only facilitate, not create, empowerment in others, yet they hinted at their responsibility to do so by referring to empowerment as a matter of social justice and equity. In addition to active participation, nurses identified increased awareness as being critical to the empowering process. That awareness was threefold and included awareness of one’s strengths and limitations, one’s rights to have control over personal/family health issues and a voice in decisions directly affecting their health, and social and political factors that influence health and healthcare. Interwoven and interacting with increased awareness and active participation, and increased knowledge and skills that made acting on informed choices not only more possible but also more likely to be successful in achieving clients’ desired outcomes and attaining their health goals. |
| Smith-Campbell B. [52] | Case study | To describe the concepts and relationships within caring, the Smith-Campbell Community Model was developed from a community case study. | The case study exemplifies a community that felt a moral obligation and empathy to assist members of their community who had special needs. After interacting with each other and gaining more information about those in need, this plurality of persons felt compelled to act by establishing an organization to meet the needs of the medically indigent. The caring action led to receptivity and positive outcomes or actual healthcare services for the medically indigent. This case study explicated the concepts of caring previously identified in the literature but was broadened to include an ontology of community and individuals. |
2.3. Concepts Relevant to Structuring Community Caring Practice
2.3.1. Assumptions of the Theory of CCPHN
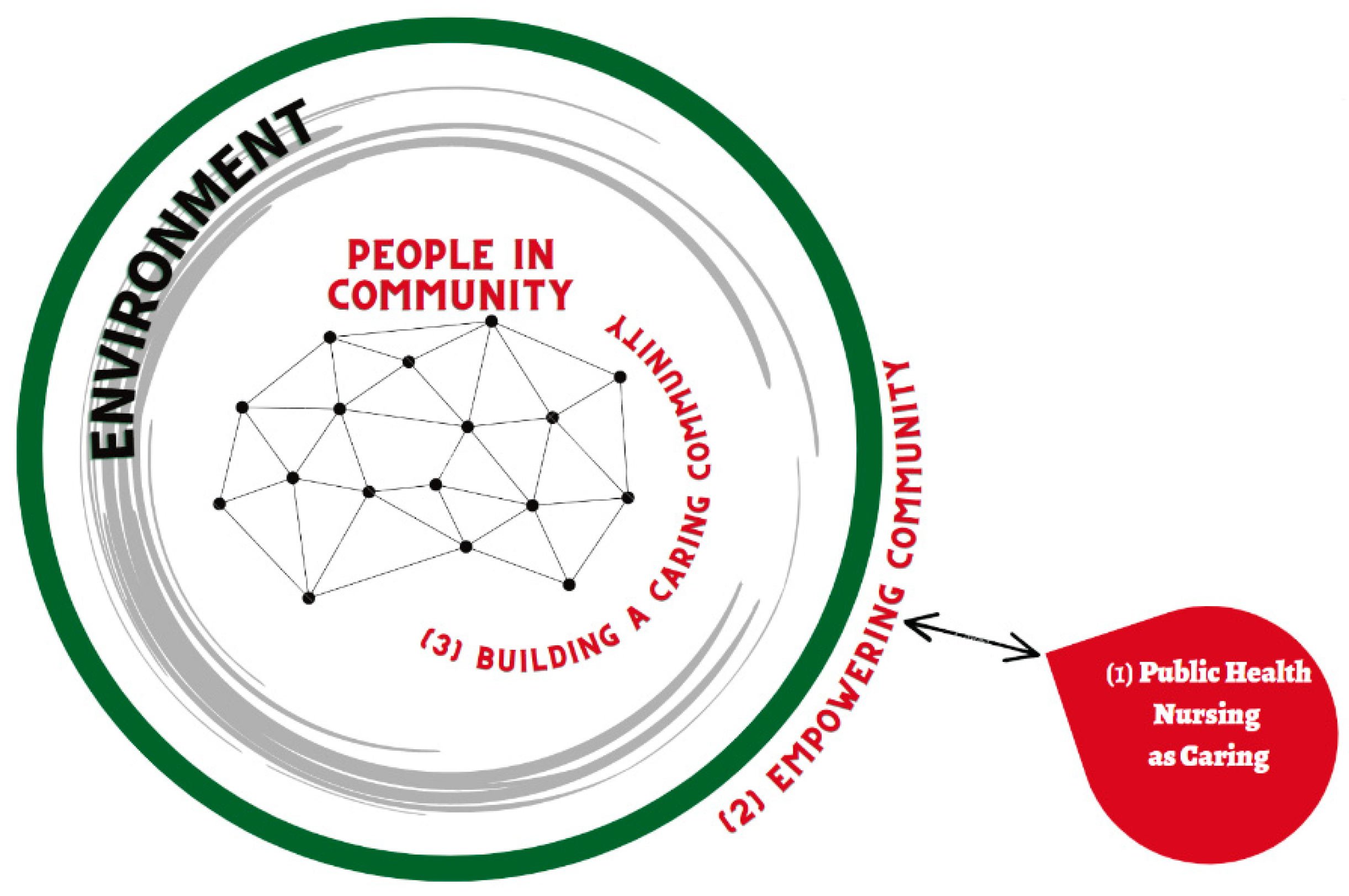
2.3.2. The Process of Nursing in the Theory of CCPHN [Figure 1]
- PHNs regard the community as an independent entity, aim to build a caring community, and facilitate the empowerment of community members.
- The caring community fostered by PHN creates a sense of solidarity from new values without being bound by old customs that are limiting. PHNs are partners with the community.
- Forming a caring community involves policymaking. To build a caring community that includes marginalized people, PHNs need to influence the entire community and create measures that meet regional challenges, including the development of new social resources. This will lead to an environment of enhanced health potential.

2.3.3. Metaparadigm Concepts of Nursing in Relation to the Theory of CCPHN
3. Community Caring in Nursing Transforming Communities
3.1. Caring Competencies and Outcomes of PHN
3.1.1. Public Health Nursing as Caring
3.1.2. Competency of PHN to Develop a Caring Community
- i.
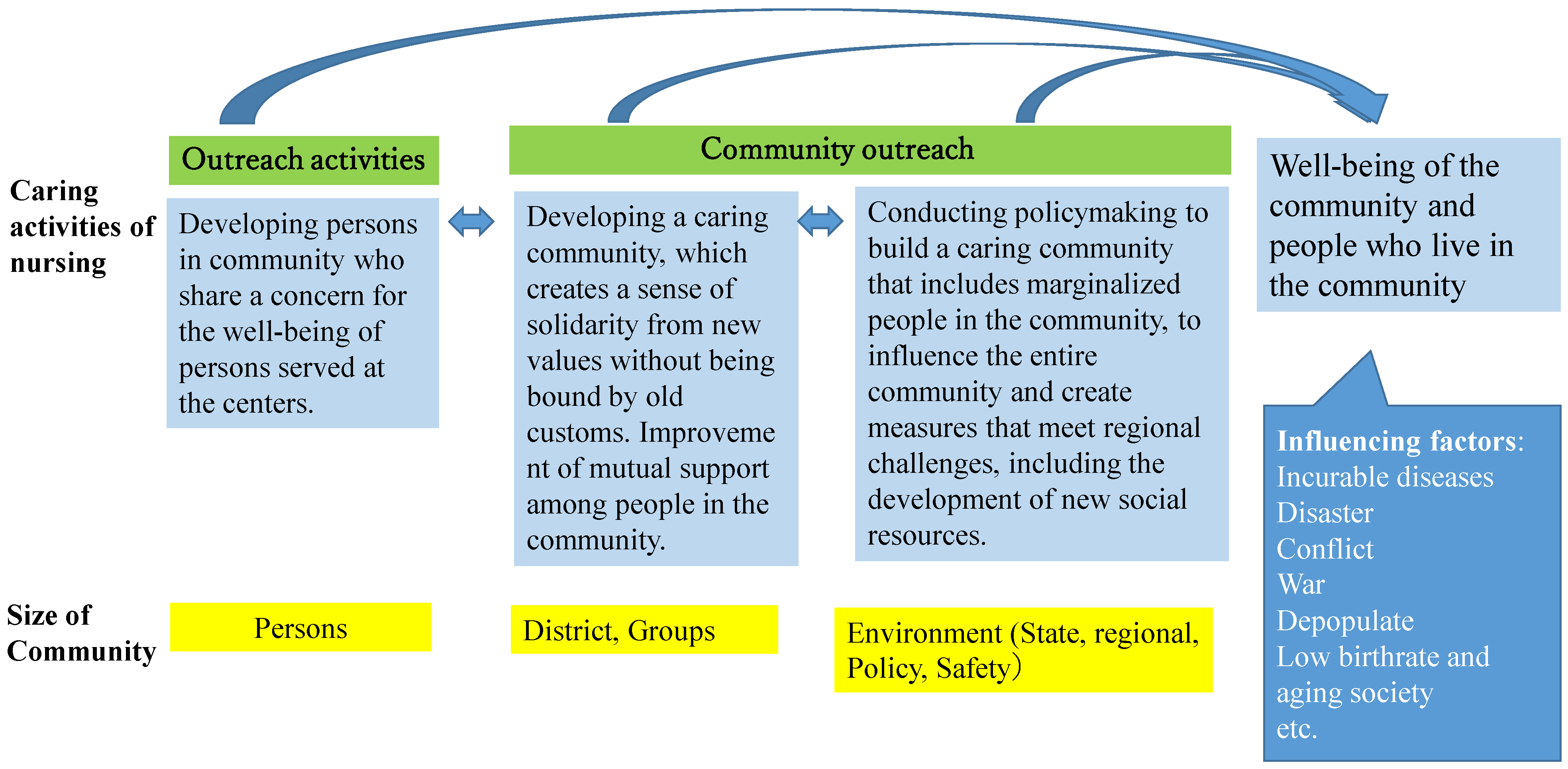
- Community Caring Targets and Activities [Figure 2]
3.1.3. The Expected Outcomes for a Caring Community
3.1.4. Factors Affecting Caring Communities

4. Clinical Applications of the Theory of Community Caring in Public Health Nursing
4.1. Use of this Theory in Practice in the Community
4.1.1. Community Use
4.1.2. Use of this Theory in Basic Education for PHNs and in-Service Education
4.2. Future Research
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Masaki, H.; Nagae, H.; Teshima, M.; Izumi, S. Nursing leadership in a rapidly aging society: Implications of “The Future of Nursing” report in Japan. Nurs. Res. Pract. 2012, 2012, 820345. [Google Scholar] [CrossRef] [PubMed]
- Muramatsu, N.; Akiyama, H. Japan: Super-aging society preparing for the future. Gerontologist 2011, 51, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Saito, E.; Ueki, S.; Yasuda, N.; Yamazaki, S.; Yasumura, S. Risk factors of functional disability among community-dwelling elderly people by household in Japan: A prospective cohort study. BMC Geriatr. 2014, 14, 93. [Google Scholar] [CrossRef]
- Mizuho, A. Elder abuse in Japan. Educ. Gerontol. 2006, 32, 13–23. [Google Scholar] [CrossRef]
- Melchiorre, M.G.; Chiatti, C.; Lamura, G.; Torres-Gonzales, F.; Stankunas, M.; Lindert, J.; Ioannidi-Kapolou, E.; Barros, H.; Macassa, G.; Soares, J.F.J. Social support, socio-economic status, health and abuse among older people in seven European countries. PLoS ONE 2013, 8, e54856. [Google Scholar] [CrossRef] [PubMed]
- Japan’s Ministry of Health, Labour, and Welfare. White Paper. Chapter 3: Toward the Construction of a Social Security System Supported by the Community. Available online: https://www.mhlw.go.jp/wp/hakusyo/kousei/05/dl/1-1d.pdf (accessed on 23 October 2022).
- Naylor, M.; Keating, S.A. Transitional care: Moving patients from one care setting to another. Am. J. Nurs. 2008, 108 (Suppl. 9), 58–63. [Google Scholar] [CrossRef]
- Salmond, S.W.; Echevarria, M. Healthcare transformation and changing roles for nursing. Orthop. Nurs. 2017, 36, 12–25. [Google Scholar] [CrossRef]
- Fujiwara, T.; Yamaoka, Y.; Kawachi, I. Neighborhood social capital and infant physical abuse: A population-based study in Japan. Int. J. Ment. Health Syst. 2016, 10, 13. [Google Scholar] [CrossRef]
- Leventhal, T.; Brooks-Gunn, J. The neighborhoods they live in: The effects of neighborhood residence on child and adolescent outcomes. Psychol. Bull. 2000, 126, 309–337. [Google Scholar] [CrossRef]
- Lette, M.; Baan, C.A.; van den Berg, M.; de Bruin, S.R. Initiatives on early detection and intervention to proactively identify health and social problems in older people: Experiences from the Netherlands. BMC Geriatr. 2015, 15, 143. [Google Scholar] [CrossRef]
- Simonds, V.W.; Wallerstein, N.; Duran, B.; Villegas, M. Community-based participatory research: Its role in future cancer research and public health practice. Prev. Chronic Dis. 2013, 10, 120205. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US); Roundtable on Health Disparities. Appendix D, Community Approaches to Addressing Health Disparities. In Challenges and Successes in Reducing Health Disparities: Workshop Summary; National Academies Press: Washington, DC, USA, 2008. Available online: https://www.ncbi.nlm.nih.gov/books/NBK215366/ (accessed on 22 December 2022).
- Japan Academy of Public Health Nursing, The Definition of Public Health Nursing. Available online: https://japhn.jp/wp/wp-content/uploads/2017/05/def_phn_en.pdf (accessed on 1 November 2022).
- Honda, H.; Kawaharada, M.; Shindo, Y.; Tanaka, R.; Nakajima, A.; Nimura, Y. Social capital in Japan: What characteristics do public health nurses see in their communities? Jpn. J. Nurs. Sci. 2018, 15, 135–145. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for South-East Asia. A Framework for Community Health Nursing Education. 2010. Available online: https://apps.who.int/iris/rest/bitstreams/909338/retrieve (accessed on 3 December 2021).
- Maass, R.; Kloeckner, C.A.; Lindstrøm, B.; Lillefjell, M. The impact of neighborhood social capital on life satisfaction and self-rated health: A possible pathway for health promotion? Health Place 2016, 42, 120–128. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Promotion. Available online: https://www.who.int/teams/health-promotion/enhanced-wellbeing/first-global-conference (accessed on 6 July 2022).
- Wilkinson, R.; Marmot, M. Social Determinants of Health: The Solid Facts, 2nd ed.; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- World Health Organization Regional Office for Europe Social Determinants of Health. The Solid Facts. Second Edition. Available online: https://apps.who.int/iris/bitstream/handle/10665/326568/9789289013710-eng.pdf?sequence=1&isAllowed=y (accessed on 6 July 2022).
- Institute of Medicine (US) Committee on Enhancing Environmental. 3 Nursing Practice. In Nursing Health, & Environment: Strengthening the Relationship to Improve the Public’s Health; Pope, A.M., Snyder, M.A., Mood, L.H., Eds.; National Academies Press: Washington, DC, USA, 1995. Available online: https://www.ncbi.nlm.nih.gov/books/NBK232401/ (accessed on 6 July 2022).
- Durant, A.F.; McDermott, S.; Kinney, G.; Triner, T. Caring science: Transforming the ethic of caring-healing practice, environment, and culture within an integrated care delivery system. Perm. J. 2015, 19, e136–e142. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.; Barry, C. Community practice guided by a nursing model. Nurs. Sci. Q. 1999, 12, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Peck, S. The Different Drum: Community Making and Peace; Simon & Schuster: New York, NY, USA, 1987. [Google Scholar]
- Davis, P. Caring and Competent Caregivers; University of Georgia: Athens, GA, USA, 1998. [Google Scholar]
- Hong, P.; Gumz, E.; Choi, S.; Crawley, B.; Ah Cho, J. Centering on structural and individual employment barriers for human–social development. Soc. Dev. Issues 2022, 43, 29–55. [Google Scholar] [CrossRef]
- Australian Institute of Family Studies. What Is Community Development? Available online: https://aifs.gov.au/cfca/expert-panel-project/what-community-development (accessed on 6 July 2022).
- Adeline, R.; Falk, R. Watson’s philosophy, science, and theory of human caring as a conceptual framework for guiding. Adv. Nurs. Sci. 2000, 23, 34–49. [Google Scholar]
- Watson, J. Nursing: Human Science and Human Care: A Theory of Nursing; National League for Nursing: New York, NY, USA, 1988. [Google Scholar]
- Bent, K.N. The ecologies of community caring. ANS Adv. Nurs. Sci. 1999, 21, 29–36. [Google Scholar] [CrossRef]
- Zerwekh, J.V. Caring on the ragged edge: Nursing persons who are disenfranchised. ANS Adv. Nurs. Sci. 2000, 22, 47–61. [Google Scholar] [CrossRef]
- Ventura, C.A.A.; Austin, W.; Carrara, B.S.; de Brito, E.S. Nursing care in mental health: Human rights and ethical issues. Nurs. Ethics 2021, 28, 463–480. [Google Scholar] [CrossRef]
- Yin, M.; Li, Z.; Zhou, C. Experience of stigma among family members of people with severe mental illness: A qualitative systematic review. Int. J. Ment. Health Nurs. 2020, 29, 141–160. [Google Scholar] [CrossRef] [PubMed]
- Gadow, S.; Schroeder, C.A. Ethics and community health: An advocacy approach. In Community as Partner: Theory and Practice in Nursing; Anderson, E., McFarlane, J., Eds.; JB Lippincott: Philadelphia, PA, USA, 1994. [Google Scholar]
- Pope, B.; Hough, M.C.; Chase, S. Ethics in community nursing. Online J. Health Ethics 2016, 12, 3. [Google Scholar] [CrossRef]
- Tulchinsky, T.H. Ethical issues in public health. In Case Studies in Public Health; Elsevier BV: Amsterdam, The Netherlands, 2018; pp. 277–316. [Google Scholar] [CrossRef]
- Postmortem Investigation Group. Morinaga Milk Arsenic Poisoning Incident. In Visit of the 14th Year—Records of the Follow-Up Investigation of Morinaga Milk Arsenic Poisoning Incident; Seseragi Publishing Co: Osaka, Japan, 1988. [Google Scholar]
- Learning from the Trajectory from Private Resentment to Public Resentment: The Starting Point of Public Health in the Morinaga Milk arsenic poisoning incident. In Proceedings of the 24th Gathering of Public Health Nurses Working for Local Governments Executive Committee; Seseragi Publishing Co.: Osaka, Japan, 1993.
- Iwamoto, S. Learning contents of the students in the class about the public health nurses’ activities for victimized child due to arsenic-laces dry milk by Morinaga. Bull. Kobe City Coll. Nurs. 2014, 18, 39–45. [Google Scholar]
- Ministry of Health, Labour and Welfare. Morinaga Milk Arsenic Poisoning Incident. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/shokuhin/kenkoukiki/morinaga/index.html (accessed on 6 July 2022).
- Tanaka, M.; Houjyou, H.; Yamashita, S. Morinaga Milk Arsenic Poisoning Incident; Minerva Shobo: Kyoto, Japan, 1973. [Google Scholar]
- Pindus, D.M.; Mullis, R.; Lim, L.; Wellwood, I.; Rundell, A.V.; Aziz, N.A.A.; Mant, J. Stroke survivors’ and informal caregivers’ experiences of primary care and community healthcare services—A systematic review and meta-ethnography. PLoS ONE 2018, 13, e0192533. [Google Scholar] [CrossRef]
- Gilmore, B.; Ndejjo, R.; Tchetchia, A.; de Claro, V.; Mago, E.; Diallo, A.A.; Lopes, C.; Bhattacharyya, S. Community engagement for COVID-19 prevention and control: A rapid evidence synthesis. BMJ Glob. Health 2020, 5, e003188. [Google Scholar] [CrossRef]
- Williams, M.V.; Chandra, A.; Spears, A.; Varda, D.; Wells, K.B.; Plough, A.L.; Eisenman, D.P. Evaluating community partnerships addressing community resilience in Los Angeles, California. Int. J. Environ. Res. Public Health 2018, 15, 610. [Google Scholar] [CrossRef]
- Tsuruta, K.; Shiomitsu, T.; Hombu, A.; Fujii, Y. Relationship between social capital and happiness in a Japanese community: A cross-sectional study. Nurs. Health Sci. 2019, 21, 245–252. [Google Scholar] [CrossRef]
- Kawasaki, C.; Omori, J.; Ono, W.; Konishi, E.; Asahara, K. Public health nurses’ experiences in caring for the Fukushima community in the wake of the 2011 Fukushima nuclear accident. Public Health Nurs. 2016, 33, 335–342. [Google Scholar] [CrossRef]
- Parker, M.; Barry, C. The Community Nursing Practice Model. Nursing Theories and Nursing Practice, 4th ed.; F.A. Davi: Philadelphia, PA, USA, 2015; pp. 435–437. [Google Scholar]
- Barry, C.D.; Gordon, S.C.; Lange, B. The usefulness of the community nursing practice model in grounding practice and research: Narratives from the United States and Africa. Res. Theory Nurs. Pract. 2007, 21, 174–184. [Google Scholar] [CrossRef]
- Falk-Rafael, A.; Betker, C. Witnessing social injustice downstream and advocating for health equity upstream: “the trombone slide” of nursing. Adv. Nurs. Sci. 2012, 35, 98–112. [Google Scholar] [CrossRef]
- Chinn, P.L.; Falk-Rafael, A. Embracing the focus of the discipline of nursing: Critical caring pedagogy. J. Nurs. Scholarsh. 2018, 50, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Falk-Rafael, A.R. Empowerment as a process of evolving consciousness: A model of empowered caring. ANS Adv. Nurs. Sci. 2001, 24, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Smith-Campbell, B. A case study on expanding the concept of caring from individuals to communities. Public Health Nurs. 1999, 16, 405–411. [Google Scholar] [CrossRef]
- Smith, M.C.; Turkell, M.; Wolf, Z. Caring in Nursing Classics; Springer: New York, NY, USA, 2013. [Google Scholar]
- Nightingale, F. Notes on nursing: What it is and what it is not. In Selected Writings of Florence Nightingale; Seymer, L.R., Ed.; MacMillan Book Co.: New York, NY, USA, 1954. [Google Scholar]
- Mayeroff, M. On Caring; The Harper Perennial: New York, NY, USA, 1971. [Google Scholar]
- Boykin, A.; Schoenhofer, S. Nursing as Caring, a Model for Transforming Practice; Jones and Bartlett Publishers: Burlington, MA, USA, 1993. [Google Scholar]
- Fawcett, J. The metaparadigm of nursing: Present status and future refinements. Image J. Nurs. Scholarsh. 1984, 16, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, J. Theory: Basis for the study and practice of nursing education. J. Nurs. Educ. 1985, 24, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, J. On the requirements for a metaparadigm: An invitation to dialogue. Nurs. Sci. Q. 1996, 9, 94–97. [Google Scholar] [CrossRef]
- Murayama, H.; Fujiwara, Y.; Kawachi, I. Social capital and health: A review of prospective multilevel studies. J. Epidemiol. 2012, 22, 179–187. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwamoto, S. Developing a Theory of Community Caring for Public Health Nursing. Healthcare 2023, 11, 349. https://doi.org/10.3390/healthcare11030349
Iwamoto S. Developing a Theory of Community Caring for Public Health Nursing. Healthcare. 2023; 11(3):349. https://doi.org/10.3390/healthcare11030349
Chicago/Turabian StyleIwamoto, Saori. 2023. "Developing a Theory of Community Caring for Public Health Nursing" Healthcare 11, no. 3: 349. https://doi.org/10.3390/healthcare11030349
APA StyleIwamoto, S. (2023). Developing a Theory of Community Caring for Public Health Nursing. Healthcare, 11(3), 349. https://doi.org/10.3390/healthcare11030349