
Factors Impacting Retention of Aged Care Workers: A Systematic Review

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility and Screening
2.3. Methodological Quality
2.4. Data Extraction and Analysis
3. Results
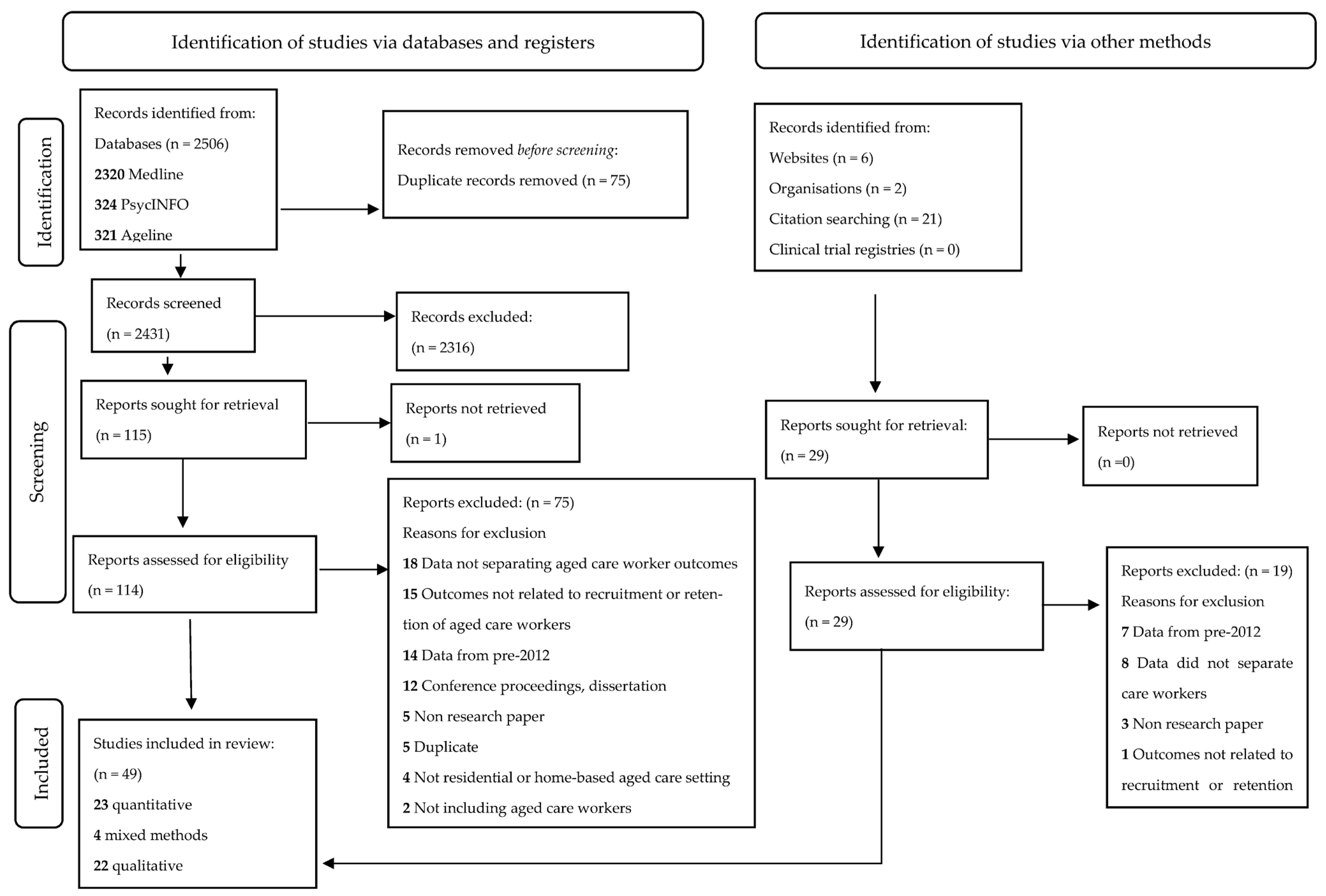
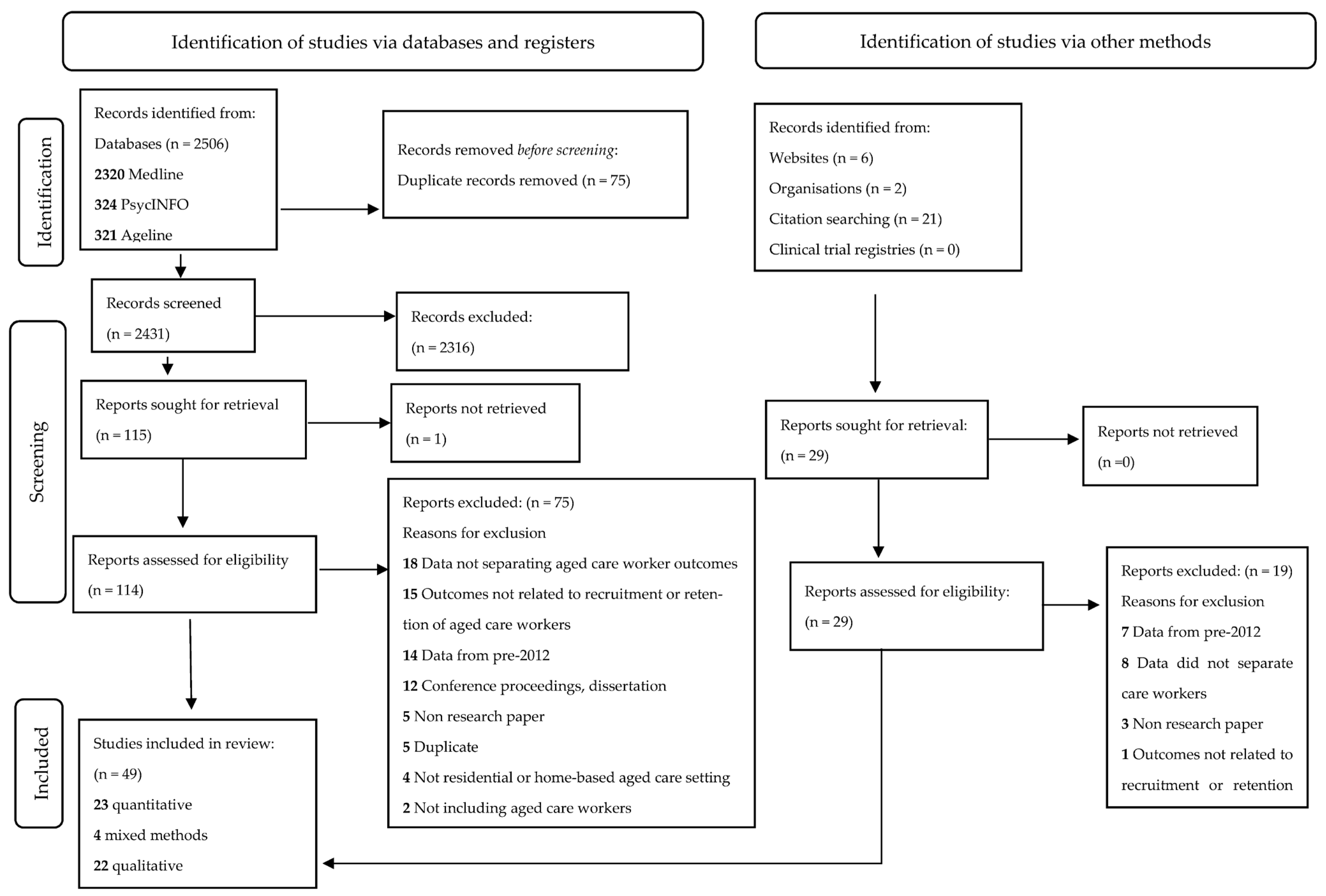
3.1. Identified Studies
3.2. Study Characteristics
3.3. Quality Assessment
3.4. Convergent Qualitative Synthesis
3.5. Individual Influences on Staff Retention
3.6. Organisational Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Economic Forum. Jobs of Tomorrow: Mapping Opportunity in the New Economy; World Economic Forum: Geneva, Switzerland, 2020; Available online: https://www3.weforum.org/docs/WEF_Jobs_of_Tomorrow_2020.pdf (accessed on 1 August 2023).
- Roser, M.; Ortiz-Ospina, E.; Ritchie, H. Life Expectancy. 2013. Available online: https://ourworldindata.org/life-expectancy (accessed on 1 August 2023).
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing populations: The challenges ahead. Lancet 2009, 374, 1196–1208. [Google Scholar] [CrossRef] [PubMed]
- Bloom, D.E.; Canning, D.; Fink, G. Implications of population ageing for economic growth. Oxf. Rev. Econ. Policy 2010, 26, 583–612. [Google Scholar] [CrossRef]
- Productivity Commission. Caring for Older Australians; Australian Government: Canberra, Australia, 2011. [Google Scholar]
- Siegel, E.O.; Bettega, K.; Bakerjian, D.; Sikma, S. Leadership in Nursing Homes: Directors of Nursing Aligning Practice With Regulations. J. Gerontol. Nurs. 2018, 44, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Huglin, J.; Whelan, L.; McLean, S.; Greer, K.; Mitchell, D.; Downie, S.; Farlie, M.K. Exploring utilisation of the allied health assistant workforce in the Victorian health, aged care and disability sectors. BMC Health Serv. Res. 2021, 21, 1144. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.J.; Maziarz, L.; Wagner, J.; Bell, J.; Burek, M. Nursing assistant turnover in nursing homes: A scoping review of the literature. Geriatr. Nurs. 2023, 51, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Eagar, K.; Westera, A.B.; Snoek, M.; Kobel, C.; Loggie, C.L.; Gordon, R. How Australian Residential Aged Care Staffing Levels Compare with International and National Benchmarks; University of Wollongong: Wollongong, Australia, 2019. [Google Scholar]
- Howe, A.L.; King, D.S.; Ellis, J.M.; Wells, Y.D.; Wei, Z.; Teshuva, K.A. Stabilising the aged care workforce: An analysis of worker retention and intention. Aust. Health Rev. 2012, 36, 83–91. [Google Scholar] [CrossRef]
- Hussein, S.; Ismail, M.; Manthorpe, J. Changes in turnover and vacancy rates of care workers in England from 2008 to 2010: Panel analysis of national workforce data. Health Soc. Care Community 2016, 24, 547–556. [Google Scholar] [CrossRef]
- Skills for Care. The State of the Adult Social Care Sector and Workforce in England; Leeds. 2022. Available online: https://www.skillsforcare.org.uk/Adult-Social-Care-Workforce-Data/Workforce-intelligence/documents/State-of-the-adult-social-care-sector/The-State-of-the-Adult-Social-Care-Sector-and-Workforce-2023.pdf (accessed on 1 August 2023).
- Gandhi, A.; Yu, H.; Grabowski, D.C. High Nursing Staff Turnover in Nursing Homes Offers Important Quality Information: Study examines high turnover of nursing staff at US nursing homes. Health Aff. 2021, 40, 384–391. [Google Scholar] [CrossRef]
- Zheng, Q.; Williams, C.S.; Shulman, E.T.; White, A.J. Association between staff turnover and nursing home quality–evidence from payroll-based journal data. J. Am. Geriatr. Soc. 2022, 70, 2508–2516. [Google Scholar] [CrossRef]
- Shin, J.H. Nursing Staff Characteristics on Resident Outcomes in Nursing Homes. J. Nurs. Res. 2019, 27, e7. [Google Scholar] [CrossRef]
- Loomer, L.; Grabowski, D.C.; Yu, H.; Gandhi, A. Association between nursing home staff turnover and infection control citations. Health Serv. Res. 2022, 57, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Squires, J.E.; Hoben, M.; Linklater, S.; Carleton, H.L.; Graham, N.; Estabrooks, C.A. Job Satisfaction among Care Aides in Residential Long-Term Care: A Systematic Review of Contributing Factors, Both Individual and Organizational. Nurs. Res. Pract. 2015, 2015, 157924. [Google Scholar] [CrossRef]
- Brownie, S.; Nancarrow, S. Effects of person-centered care on residents and staff in aged-care facilities: A systematic review. Clin. Interv. Aging 2013, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Marć, M.; Bartosiewicz, A.; Burzyńska, J.; Chmiel, Z.; Januszewicz, P. A nursing shortage–a prospect of global and local policies. Int. Nurs. Rev. 2019, 66, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.J.; Hamler, T.; Beltran, S.J.; Burns, J. Nursing home social services: A systematic review of the literature from 2010 to 2020. Soc. Work. Health Care 2021, 60, 387–409. [Google Scholar] [CrossRef]
- Rees, C.S.; Eley, R.; Osseiran-Moisson, R.; Francis, K.; Cusack, L.; Heritage, B.; Hegney, D. Individual and environmental determinants of burnout among nurses. J. Health Serv. Res. Policy 2019, 24, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Hoben, M.; Norton, P.; Estabrooks, C.A. Association of Work Environment with Missed and Rushed Care Tasks Among Care Aides in Nursing Homes. JAMA Netw. Open 2020, 3, e1920092. [Google Scholar] [CrossRef] [PubMed]
- Hodgkin, S.; Warburton, J.; Savy, P.; Moore, M. Workforce crisis in residential aged care: Insights from rural, older workers. Aust. J. Public Adm. 2017, 76, 93–105. [Google Scholar] [CrossRef]
- Gao, F.; Tilse, C.; Wilson, J.; Tuckett, A.; Newcombe, P. Perceptions and employment intentions among aged care nurses and nursing assistants from diverse cultural backgrounds: A qualitative interview study. J. Aging Stud. 2015, 35, 111–122. [Google Scholar] [CrossRef]
- Hegeman, C.; Hoskinson, D.; Munro, H.; Maiden, P.; Pillemer, K. Peer mentoring in long-term care: Rationale, design, and retention. Gerontol. Geriatr. Educ. 2007, 28, 77–90. [Google Scholar] [CrossRef]
- Weale, V.P.; Wells, Y.D.; Oakman, J. Flexible working arrangements in residential aged care: Applying a person–environment fit model. Asia Pac. J. Hum. Resour. 2017, 55, 356–374. [Google Scholar] [CrossRef]
- Dhakal, S.; Nankervis, A.; Connell, J.; Fitzgerald, S.; Burgess, J. Attracting and retaining personal care assistants into the Western Australia (WA) residential aged care sector. Labour Ind. 2017, 27, 333–349. [Google Scholar] [CrossRef]
- Brook, J.; Aitken, L.; Webb, R.; MacLaren, J.; Salmon, D. Characteristics of successful interventions to reduce turnover and increase retention of early career nurses: A systematic review. Int. J. Nurs. Stud. 2019, 91, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.M.Z. JBI Manual for Evidence Synthesis. 2020. Available online: https://synthesismanual.jbi.global (accessed on 1 August 2023).
- Stern, C.; Lizarondo, L.; Carrier, J.; Godfrey, C.; Rieger, K.; Salmond, S.; Apóstolo, J.; Kirkpatrick, P.; Loveday, H. Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evid. Synth. 2020, 18, 2108–2118. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2022. Available online: www.covidence.org (accessed on 1 August 2023).
- Davies, S.; Keenan, C.M.; Redley, B. Health Assistant in Nursing: A Victorian health service pilot. Asia Pac. J. Health Manag. 2017, 12, 17–24. [Google Scholar] [CrossRef]
- United Nations. World Population Ageing 2019: Highlights; Contract No.: (ST/ESA/SER.A/430); United Nations: New York City, NY, USA, 2019. [Google Scholar]
- Australian Government. Royal Commission into Aged Care Quality and Safety: Care, Dignity and Respect; Australian Government: Canberra, Australia, 2021. [Google Scholar]
- Morris, M.E.; Brusco, N.; McAleer, R.; Billett, S.; Brophy, L.; Bryant, R.; Carey, L.; Wright, A.C.; East, C.; Eckert, M. Care workforce: A rapid review of evidence supporting methods of recruitment, retention, safety and education. Hum. Resour. Health 2023. [Google Scholar] [CrossRef]
- Moore, C.B. Consumer directed care aged care reforms in Australia since 2009: A retrospective policy analysis. Health Policy 2021, 125, 577–581. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; et al. Improving the content validity of the mixed methods appraisal tool: A modified e-Delphi study. J. Clin. Epidemiol. 2019, 111, 49–59.e41. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Edhlund, B.; McDougall, A. NVivo 12 Essentials; Lulu: Denver, CO, USA, 2019. [Google Scholar]
- Thompson Burdine, J.; Thorne, S.; Sandhu, G. Interpretive description: A flexible qualitative methodology for medical education research. Med. Educ. 2021, 55, 336–343. [Google Scholar] [CrossRef]
- Moser, A.; Korstjens, I. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. Eur. J. Gen. Pract. 2018, 24, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.H.; Simpson, J.M.; Li, Z.; Cunich, M.M.; Thomas, T.H.; Chenoweth, L.; Kendig, H.L. Cluster Randomized Controlled Trial of An Aged Care Specific Leadership and Management Program to Improve Work Environment, Staff Turnover, and Care Quality. J. Am. Med. Dir. Assoc. 2015, 16, 629.e19–629.e28. [Google Scholar] [CrossRef]
- Ericson-Lidman, E.; Åhlin, J. Assessments of Stress of Conscience, Perceptions of Conscience, Burnout, and Social Support Before and After Implementation of a Participatory Action-Research-Based Intervention. Clin. Nurs. Res. 2017, 26, 205–223. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, W.H.; Singh, R.S.; Horan, K.; Moeller, M.T.; Wasson, R.; Jex, S.M. Group-Based Acceptance and Commitment Therapy for Nurses and Nurse Aides Working in Long-Term Care Residential Settings. J. Altern. Complement. Med. 2019, 25, 753–761. [Google Scholar] [CrossRef]
- Sharma, H.; Xu, L. Association Between Wages and Nursing Staff Turnover in Iowa Nursing Homes. Innov. Aging 2022, 6, igac004. [Google Scholar] [CrossRef]
- Berridge, C.; Lima, J.; Schwartz, M.; Bishop, C.; Miller, S.C. Leadership, Staff Empowerment, and the Retention of Nursing Assistants: Findings from a Survey of U.S. Nursing Homes. J. Am. Med. Dir. Assoc. 2020, 21, 1254–1259.e1252. [Google Scholar] [CrossRef]
- Brown, P.B.; Hudak, S.L.; Horn, S.D.; Cohen, L.W.; Reed, D.A.; Zimmerman, S. Workforce Characteristics, Perceptions, Stress, and Satisfaction among Staff in Green House and Other Nursing Homes. Health Serv. Res. 2016, 51 (Suppl. 1), 418–432. [Google Scholar] [CrossRef]
- Chang, Y.C.; Yeh, T.F.; Lai, I.J.; Yang, C.C. Job Competency and Intention to Stay among Nursing Assistants: The Mediating Effects of Intrinsic and Extrinsic Job Satisfaction. Int. J. Environ. Res. Public Health 2021, 18, 6436. [Google Scholar] [CrossRef]
- Chao, S.F.; Lu, P.C. Differences in determinants of intention to stay and retention between younger and older nursing assistants in long-term care facilities: A longitudinal perspective. J. Nurs. Manag. 2020, 28, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Charlesworth, S.; Isherwood, L. Migrant aged-care workers in Australia: Do they have poorer-quality jobs than their locally born counterparts? Ageing Soc. 2021, 41, 2702–2722. [Google Scholar] [CrossRef]
- Cheung, K.; Szeto, G.; Lai, G.K.B.; Ching, S.S.Y. Prevalence of and Factors Associated with Work-Related Musculoskeletal Symptoms in Nursing Assistants Working in Nursing Homes. Int. J. Environ. Res. Public Health 2018, 15, 265. [Google Scholar] [CrossRef]
- Dys, S.; Tunalilar, O.; Hasworth, S.; Winfree, J.; White, D.L. Person-centered care practices in nursing homes: Staff perceptions and the organizational environment. Geriatr. Nurs. 2022, 43, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Isherwood, L.; King, D. Targeting workforce strategies: Understanding intra-group differences between Asian migrants in the Australian aged care workforce. Int. J. Care Caring 2017, 1, 191–207. [Google Scholar] [CrossRef]
- Keisu, B.I.; Öhman, A.; Enberg, B. Employee effort—Reward balance and first-level manager transformational leadership within elderly care. Scand. J. Caring Sci. 2018, 32, 407–416. [Google Scholar] [CrossRef]
- Kennedy, K.A.; Applebaum, R.; Bowblis, J.R. Facility-Level Factors Associated With CNA Turnover and Retention: Lessons for the Long-Term Services Industry. Gerontologist 2020, 60, 1436–1444. [Google Scholar] [CrossRef]
- Liang, Y.W.; Hsieh, Y.; Lin, Y.H.; Chen, W.Y. The impact of job stressors on health-related quality of life of nursing assistants in long-term care settings. Geriatr. Nurs. 2014, 35, 114–119. [Google Scholar] [CrossRef]
- Lin, L.; Liu, X.; McGilton, K.S.; Yuan, Y.; Li, H.; Dong, B.; Xie, C.; Wang, H.; Li, H.; Tian, L. Level of nurse supportive supervision and its influencing factors in long-term care facilities. Geriatr. Nurs. 2021, 42, 1316–1322. [Google Scholar] [CrossRef]
- Matthews, M.; Carsten, M.K.; Ayers, D.J.; Menachemi, N. Determinants of turnover among low wage earners in long term care: The role of manager-employee relationships. Geriatr. Nurs. 2018, 39, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Monforte, M.; Bethell, J.; Stewart, S.; Chu, C.H.; Escrig-Pinol, A.; Gea-Sánchez, M.; McGilton, K.S. The influence of supervisory support, work effectiveness, work empowerment and stress secondary to residents’ responsive behaviours on job satisfaction of nursing staff: A multisite cross-sectional study. J. Nurs. Manag. 2021, 29, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Rodwell, J.; Demir, D.; Gulyas, A. Individual and contextual antecedents of workplace aggression in aged care nurses and certified nursing assistants. Int. J. Nurs. Pract. 2015, 21, 367–375. [Google Scholar] [CrossRef]
- Stevens, M.L.; Karstad, K.; Januario, L.B.; Mathiassen, S.E.; Rugulies, R.; Hallman, D.M.; Holtermann, A. Nursing Home, Ward and Worker Level Determinants of Perceived Quantitative Work Demands: A Multi-Level Cross-Sectional Analysis in Eldercare. Ann. Work Expo. Health 2022, 66, 1033–1043. [Google Scholar] [CrossRef]
- Wallin, A.O.; Jakobsson, U.; Edberg, A.K. Job satisfaction and associated variables among nurse assistants working in residential care. Int. Psychogeriatr. 2012, 24, 1904–1918. [Google Scholar] [CrossRef]
- Yang, M.H.; Jhan, C.J.; Hsieh, P.C.; Kao, C.C. A Study on the Correlations between Musculoskeletal Disorders and Work-Related Psychosocial Factors among Nursing Aides in Long-Term Care Facilities. Int. J. Environ. Res. Public Health 2021, 19, 255. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Punnett, L.; McEnany, G.P.; Gore, R. Contributing influences of work environment on sleep quantity and quality of nursing assistants in long-term care facilities: A cross-sectional study. Geriatr. Nurs. 2016, 37, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Beynon, C.; Supiano, K.; Siegel, E.O.; Edelman, L.S.; Hart, S.E.; Madden, C. Collaboration Between Licensed Nurses and Certified Nurse Aides in the Nursing Home: A Mixed Methods Study. Res. Gerontol. Nurs. 2022, 15, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Dhakal, S.P.; Nankervis, A.; Connell, J.; Burgess, J. Challenges of caring for the aged: Attracting and retaining aged care assistants in Western Australia. Australas. J. Ageing 2020, 39, e573–e577. [Google Scholar] [CrossRef]
- Graham, P.; Dougherty, J.P. Oh, their aching backs! occupational injuries in nursing assistants. Orthop. Nurs. 2012, 31, 218–223. [Google Scholar] [CrossRef]
- Leskovic, L.; Erjavec, K.; Leskovar, R.; Vukovič, G. Burnout and job satisfaction of healthcare workers in Slovenian nursing homes in rural areas during the COVID-19 pandemic. Ann. Agric. Environ. Med. 2020, 27, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Adebayo, B.; Nichols, P.; Heslop, K.; Brijnath, B. Migrant Care Workers’ Perceptions of Their Working Conditions in Australian Residential Aged Care Facilities. J. Transcult. Nurs. 2023, 34, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Amateau, G.; Gendron, T.L.; Rhodes, A. Stress, strength, and respect: Viewing direct care staff experiences through a trauma-informed lens. Gerontol. Geriatr. Educ. 2023, 44, 380–395. [Google Scholar] [CrossRef] [PubMed]
- Bergqvist, M.; Bastholm-Rahmner, P.; Gustafsson, L.L.; Holmgren, K.; Veg, A.; Wachtler, C.; Schmidt-Mende, K. How much are we worth? Experiences of nursing assistants in Swedish nursing homes during the first wave of COVID-19. Int. J. Older People Nurs. 2023, 18, e12498. [Google Scholar] [CrossRef]
- Booi, L.; Sixsmith, J.; Chaudhury, H.; O’Connor, D.; Young, M.; Sixsmith, A. ‘I wouldn’t choose this work again’: Perspectives and experiences of care aides in long-term residential care. J. Adv. Nurs. 2021, 77, 3842–3852. [Google Scholar] [CrossRef]
- Cooke, H.A.; Baumbusch, J. Not Just How Many but Who Is on Shift: The Impact of Workplace Incivility and Bullying on Care Delivery in Nursing Homes. Gerontologist 2021, 61, 563–572. [Google Scholar] [CrossRef]
- Creapeau, L.J.G.; Johs-Artisensi, J.L.; Lauver, K.J. Leadership and Staff Perceptions on Long-term Care Staffing Challenges Related to Certified Nursing Assistant Retention. J. Nurs. Adm. 2022, 52, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Dijxhoorn, A.-F.Q.; Heijnen, Y.; van der Linden, Y.M.; Leget, C.; Raijmakers, N.J.H.; Brom, L. Nursing assistants’ perceptions and experiences with the emotional impact of providing palliative care: A qualitative interview study in nursing homes. J. Adv. Nurs. 2023. [Google Scholar] [CrossRef] [PubMed]
- Franzosa, E.; Mak, W.; Burack, R.O.; Hokenstad, A.; Wiggins, F.; Boockvar, K.S.; Reinhardt, J.P. Perspectives of certified nursing assistants and administrators on staffing the nursing home frontline during the COVID-19 pandemic. Health Serv. Res. 2022, 57, 905–913. [Google Scholar] [CrossRef]
- Gleason, H.P.; Boerner, K.; Barooah, A. Supporting home health aides through a client’s death: The role of supervisors and coworkers. Geriatr. Nurs. 2016, 37, 278–283. [Google Scholar] [CrossRef]
- Goel, K.; Penman, J. Employment experiences of immigrant workers in aged care in regional South Australia. Rural Remote Health 2015, 15, 2693. [Google Scholar] [CrossRef]
- Gray, J.A.; Lukyanova, V. Examining Certified Nursing Assistants’ Perceptions of Work-Related Identity. Creat. Nurs. 2017, 23, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Hoedl, M.; Thonhofer, N.; Schoberer, D. COVID-19 pandemic: Burdens on and consequences for nursing home staff. J. Adv. Nurs. 2022, 78, 2495–2506. [Google Scholar] [CrossRef]
- Holmberg, M.D.; Flum, M.; West, C.; Zhang, Y.; Qamili, S.; Punnett, L. Nursing Assistants’ Dilemma: Caregiver Versus Caretaker. Hosp. Top. 2013, 91, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Krein, S.L.; Turnwald, M.; Anderson, B.; Maust, D.T. “Sometimes it’s not about the money... it’s the way you treat people...”: A Qualitative Study of Nursing Home Staff Turnover. J. Am. Med. Dir. Assoc. 2022, 23, 1178–1184. [Google Scholar] [CrossRef]
- Lim, J. Characteristics of Elderly Care Work That Influence Care Workers’ Turnover Intentions. Healthcare 2021, 9, 259. [Google Scholar] [CrossRef] [PubMed]
- Marziali, E.; Mackenzie, C.S.; Tchernikov, I. Acceptability of an e-learning program to help nursing assistants manage relationship conflict in nursing homes. Am. J. Alzheimer’s Dis. Other Dement. 2015, 30, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Nichols, P.; Horner, B.; Fyfe, K. Understanding and improving communication processes in an increasingly multicultural aged care workforce. J. Aging Stud. 2015, 32, 23–31. [Google Scholar] [CrossRef]
- Roussillon Soyer, C.; St-Onge, S.; Igalens, J.; Balkin, D.B. The demotivating impact of absenteeism in nursing homes. J. Nurs. Manag. 2021, 29, 1679–1690. [Google Scholar] [CrossRef]
- Senecal, M.B.; McBride, K.; Steiner, V.; Pierce, L.; Saltzman, B. State Tested Nursing Assistants’ Workplace Experiences That Threaten or Support Intent to Stay. Rehabil. Nurs. 2020, 45, 323–331. [Google Scholar] [CrossRef]
- Sousa-Ribeiro, M.; Persson, L.; Sverke, M.; Lindfors, P. Approaching retirement: A qualitative study of older nursing assistants’ experiences of work in residential care and late-career planning. J. Aging Stud. 2022, 60, 100994. [Google Scholar] [CrossRef] [PubMed]
- Titley, H.K.; Young, S.; Savage, A.; Thorne, T.; Spiers, J.; Estabrooks, C.A. Cracks in the foundation: The experience of care aides in long-term care homes during the COVID-19 pandemic. J. Am. Geriatr. Soc. 2023, 71, 198–205. [Google Scholar] [CrossRef]
- Winarnita, M.; Higo, M.; Klassen, T.; Blackberry, I. Asian female migrant aged care workers in regional Australia and social resilience. Rev. Reg. Res. 2022. [Google Scholar] [CrossRef]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- McCallum, J. Australia’s New Aged: Issues for Young and Old; Taylor & Francis: London, UK, 2023. [Google Scholar]
- Lee, Y.K.; Fried, T.R.; Costello, D.M.; Hajduk, A.M.; O’Leary, J.R.; Cohen, A.B. Perceived dementia risk and advance care planning among older adults. J. Am. Geriatr. Soc. 2022, 70, 1481–1486. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Johnson, C.E.; Auret, K.; Ritson, D.; Masarei, C.; Chua, D.; Licqurish, S.; Mitchell, G.; Cook, A. Comparison of end-of-life care for people living in home settings versus residential aged care facilities: A nationwide study among Australian general practitioners. Health Soc. Care Community 2022, 30, 91–101. [Google Scholar] [CrossRef]
- McMaughan, D.J.; Oloruntoba, O.; Smith, M.L. Socioeconomic Status and Access to Healthcare: Interrelated Drivers for Healthy Aging. Front. Public Health 2020, 8, 231. [Google Scholar] [CrossRef]
- Zimmer, Z.; Jagger, C.; Chiu, C.-T.; Ofstedal, M.B.; Rojo, F.; Saito, Y. Spirituality, religiosity, aging and health in global perspective: A review. SSM-Popul. Health 2016, 2, 373–381. [Google Scholar] [CrossRef]
- Shrestha, S.; Alharbi, R.J.; Wells, Y.; While, C.; Rahman, M.A. Caring self-efficacy of direct care workers in residential aged care settings: A mixed methods scoping review. Geriatr. Nurs. 2021, 42, 1429–1445. [Google Scholar] [CrossRef]
- Australian Commission of Safety and Quality in Health Care. National Safety and Quality Health Service (NSQHS) Standards; Australian Government: Canberra, Australia, 2023. Available online: https://www.safetyandquality.gov.au/standards/nsqhs-standards/clinical-governance/clinical-governance-standard (accessed on 1 August 2023).
- Australian Government. Respect, care dignity. A generational plan for aged care in Australia. In Health Do; Australian Government: Canberra, Australia, 2021. [Google Scholar]
- Teisberg, E.; Wallace, S.; O’Hara, S. Defining and Implementing Value-Based Health Care: A Strategic Framework. Acad. Med. 2020, 95, 682–685. [Google Scholar] [CrossRef]
- Koopmans, L.; Damen, N.; Wagner, C. Does diverse staff and skill mix of teams impact quality of care in long-term elderly health care? An exploratory case study. BMC Health Serv. Res. 2018, 18, 988. [Google Scholar] [CrossRef]
- Polacsek, M.; Goh, A.; Malta, S.; Hallam, B.; Gahan, L.; Cooper, C.; Low, L.-F.; Livingston, G.; Panayiotou, A.; Loi, S.; et al. ‘I know they are not trained in dementia’: Addressing the need for specialist dementia training for home care workers. Health Soc. Care Community 2020, 28, 475–484. [Google Scholar] [CrossRef]
- Anderson, K.; Blair, A. What have staff got to do with it? Untangling complex relationships between residential aged care staff, the quality of care they provide, and the quality of life of people with dementia. Arch. Gerontol. Geriatr. 2021, 94, 104378. [Google Scholar] [CrossRef]
- Spilsbury, K.; Charlwood, A.; Valizade, D.; Haunch, K. Relationship between care home staffing and quality of care: A mixed-methods approach. Innov. Aging 2019, 3 (Suppl. 1), S242. [Google Scholar] [CrossRef]
- Colic-Peisker, V.; Fozdar, F. Employment Niches for Recent Refugees: Segmented Labour Market in Twenty-first Century Australia. J. Refug. Stud. 2006, 19, 203–229. [Google Scholar] [CrossRef]
- Overgaard, C.; Withers, M.; Mcdermott, J. What do we know about the experiences of migrant care workers in Australia? A scoping study. Aust. J. Soc. Issues 2022, 57, 663–686. [Google Scholar] [CrossRef]
- Crasii, O.; Nawar, Y.S. Exploring the Effect of Business Strategy on Employees’ Retention During Pandemic and After Brexit: The case Home Care Sector in UK. Bus. Manag. Rev. 2022, 13, 134–144. [Google Scholar] [CrossRef]
- King-Dejardin, A. The Social Construction of Migrant Care Work. At the Intersection of Care, Migration and Gender; International Labour Organization Report; International Labour Organization: Geneva, Switzerland, 2019; pp. 978–992. [Google Scholar]
- Theobald, H. Care workers with migration backgrounds in formal care services in Germany: A multi-level intersectional analysis. Int. J. Care Caring 2017, 1, 209–226. [Google Scholar] [CrossRef]
- Mulliner, E.; Riley, M.; Maliene, V. Older People’s Preferences for Housing and Environment Characteristics. Sustainability 2020, 12, 5723. [Google Scholar] [CrossRef]
- Horner, B.; Boldy, D.P. The benefit and burden of “ageing-in-place” in an aged care community. Aust. Health Rev. 2008, 32, 356–365. [Google Scholar] [CrossRef]

{kind=link}
| Inclusion | Exclusion |
|---|---|
|
|
| Author (Year) Country | Study Aims | Study Design, Data Collection | Participants | Key Findings | MMAT |
|---|---|---|---|---|---|
| Quantitative interventional studies | |||||
| Jeon (2015) [45] Australia | Evaluate the effectiveness of a clinical leadership training program (CLiAC) for middle managers in RACFs | RCT (double-blind cluster), questionnaires, human resource records | n = 589 IG: 191 AIN/PCAs, 26 nurses; CG: 276 AIN/PCAs, 46 nurses. 12 RACFs, 12 community | Positive influence on perceptions of supervisor support, management leadership styles, behaviours; passive avoidance behaviour of managers; overall satisfaction with leadership. No effect on care worker stress, turnover, intention to leave. | High |
| Ericson-Lindman (2017) [46] Sweden | Assess conscience, burnout, and social support of health care professionals following participatory action research | Pre–post intervention, questionnaires | n = 29 5 RNs and 24 CNAs from single RACF | Minor increase in perception of conscience and work-related social support. No effect on stress of conscience or burnout. | Mod |
| O’Brien (2019) [47] USA | Process evaluation of a group-based cognitive behavioural treatment program for care staff working in aged care | RCT with waitlist control, questionnaires | n = 71 Intervention 37, control group 34, nurses and NAs from NHs | Significant reduction in staff absences and mental health symptoms. No change in number of workplace injuries reported. | High |
| Quantitative descriptive studies | |||||
| Berridge (2020) [49] USA | Examine the relationship between NA retention and factors considered important to NH culture change at a facility level | Cross-sectional, questionnaire | n = 1368 NH administrators | Associations between high (vs low) retention rates of NAs and greater leadership/staff empowerment scores; low NH administrator turnover; high NH occupancy rates; presence of a union; greater hours per day allocated to residents. | High |
| Brown (2016) [50] USA | Identify differences in staffing hours, turnover, staff experiences, and perceptions between NHs and “Green House” NHs | Cross-sectional (two groups), questionnaires, human resource records | n = 502 (226 Green House, 276 NH), 47% CNAs | Green House NH CNAs reported increased ability to do their job in the event of staff absences. Nonsignificant trend towards lower CNA turnover in Green House NHs. | High |
| Chang (2021) [51] Taiwan | Investigate the influence of CNA job competency, satisfaction, and intention to stay | Cross-sectional, questionnaires | n = 333 236 CNAs from NHs, 97 CNAs from 26 NHs and 15 elderly welfare institutions | Job satisfaction related to higher job competency and salary, mediating a positive effect on intention to stay. Positively influenced by internal factors, i.e., self-esteem. | High |
| Chao (2020) [52] Taiwan | Assess determinants of intention to stay and actual retention rates between younger and older NAs | Longitudinal, questionnaires | n = 595 258 “Younger” and 337 “Older” CNAs from 137 LTCFs | Younger NA retention significantly influenced by gender and marital status. Older NAs retention significantly influenced by high work latitude and utilisation strategies; low burnout rates. | High |
| Charlesworth (2020) [53] Australia | Investigate the differences in migrant status amongst PCAs and HCWs against casual status and underemployment | Cross-sectional, questionnaires | n = 7114 2759 PCAs from RACFs, 4355 HCW | Migrant HCW and PCAs significantly more likely to be male and hold high levels of formal qualifications than locally born workers. Migrant workers much more likely to be underemployed and on casual contracts, with higher rates of multiple jobholding. | High |
| Cheung (2018) [54] Hong Kong | Determine prevalence of, and factors related to, workplace-related musculoskeletal injuries in Nas | Cross-sectional, questionnaires | n = 440 NAs from 47 NHs | Musculoskeletal injuries found to be experienced at high rates by NAs working in NHs; in mainly older, female workers who perceive work to be more stressful; associated with an increased intention to leave and a perceived health status of “not good”. | High |
| Dys (2022) [55] USA | Investigate staff perceptions of person-centred practices, organisational culture, and relationship to staff outcomes | Cross-sectional, questionnaire | n = 340 266 DCWs and 74 nurses from 23 NHs | No significant difference between DCWs or nurse perceptions of person-centred care; intention to leave; affective commitment. | High |
| Isherwood (2017) [56] Australia | To understand the difference between groups of Asian migrant care workers | Cross-sectional, questionnaire | n = 4530 PCAs from RACFs | Asian-born migrant PCAs had significantly higher levels of post-high school education compared to locally born PCAs. Asian PCAs were more likely to be employed on a casual basis, working fewer hours than desired, be expected to work longer shifts than scheduled and holding multiple jobs. Asian PCAs were more satisfied than locally born PCAs with the job role and wage. | High |
| Keisu (2018) [57] Sweden | Assess the relationship between care worker perceptions of management styles and ratings of effort and reward in aged care work | Cross-sectional, questionnaire | n = 159 80 nurses and allied health staff, 73 NAs, and 4 administrators from 9 RACFs | Association between professionals and greater reward for effort; professionals and identification of managers as having positive transformational leadership styles; higher transformational leadership style of managers and employee reward for effort. | High |
| Kennedy (2020) [58] USA | Examine facility-level factors associated with CNA turnover and retention in LTCF | Cross-sectional, questionnaire, certification reporting, human resources | n = 835 LTCFs | Associations between high turnover and lower retention of CNAs; for-profit status of facilities; turnover of DON staff; low empowerment of CNAs; greater proportion of residents with psychiatric illness (not dementia); low local unemployment rates. | High |
| Liang (2014) [59] Taiwan | Investigate the relationship between health-related quality of life and job stressors in NH care workers | Cross-sectional, questionnaire | n = 443 NAs from 64 LTCFs | Greater physical quality of life associated with staff with longer shift lengths; psychological job demands. Greater mental health quality of life associated with older staff age, working in smaller NHs. | High |
| Lin (2021) [60] China | Assess the level of supportive supervision and factors influencing this from RNs to PSWs in LTCFs | Cross-sectional, questionnaire | n = 643 PSWs from 12 LTCFs | Factors increasing supportive supervision included nurses with higher education levels; female nurses; completion of management training; increased years of experience; higher RN/PSW ratios. PSWs reported moderate levels of supportive supervision. | Mod |
| Matthews (2018) [61] | Examine the impact of manager-employee relationship quality on turnover in “low-wage earners” working in LTCFs | Longitudinal, questionnaire | n = 337 69 CNAs, 98 NAs, and 23 medical technicians | Turnover associated with reporting lower levels of affect, respect, or contribution towards supervisors; experience of lower levels of loyalty from supervisors than retained staff. Most significant factor irrespective of age, gender, or job satisfaction was loyalty experienced by the employee. | High |
| Rodríguez-Monforte (2020) [62] Canada | Analyse the association between work-related stress and job satisfaction of care staff in NHs and factors that may confound this relationship | Cross-sectional, questionnaire | n = 272 191 CNAs and 81 nurses from 5 NHs | Reduced job satisfaction related to stress resulting from resident behaviour; lower levels of supervisory support; less work effectiveness; less empowerment. | High |
| Rodwell (2015) [63] Australia | Examine the relationship between the job-demands resource model, negative affect, demographics workplace aggression | Cross-sectional, questionnaire | n = 291 208 nurses and 83 NAs from RACFs | CNAs reported high rates of threats of assault, physical assault, bullying, and emotional abuse from residents’ families. Increased emotional abuse was related to higher workloads, younger age of staff and lower levels of workplace support. | High |
| Sharma (2022) [48] USA | Assess the relationship between wages and nursing home staff turnover | Cross-sectional, human resource records | n = 439 NHs with turnover data from 2013 to 2017 | Factors associated with lower turnover were higher wages, with small increases not effective. Factors not associated with lower turnover included resident demographics; staff hours; facility location; local unemployment rates. | High |
| Stevens (2022) [64] Denmark | Investigate the determinants of perceived quantitative work demands and at what organisational levels they occur in NHs | Cross-sectional survey and observational, questionnaire, observations, step rate | n = 383 185 CAs, 162 care helpers and 33 professional health care workers | Lower perceived quantitative work demands associated with least qualified staff (care helpers); migrants; working fixed night or evening/night shifts; lower work-related emotional demands; lower influence levels at work. Not associated with resident-related physical tasks or step counts. | High |
| Wallin (2012) [65] Sweden | Examine factors associated with job satisfaction in NAs working RACF | Cross-sectional, questionnaire | n = 225 Nas from specialised dementia care and general RACFs | Higher general job satisfaction associated with a caring climate and personalised care provision. Higher nursing care satisfaction associated with general work climate, environmental and organisational support. Low job satisfaction associated with NA health complaints. | High |
| Yang (2021) [66] Taiwan | Investigate the relationship between musculoskeletal disorders and psychosocial factors in NAs | Cross-sectional, questionnaire | n = 308 NAs from 15 LTCFs | Increased reporting of musculoskeletal injury related to lower social support; higher psychological job demands; older age of NAs; migrants; those not using assistive devices for manual handling tasks. | High |
| Zhang (2016) [67] USA | Explore psychological and organisational work-related factors that impact sleep in NAs working in LTCFs | Cross-sectional, questionnaires | n = 744 NAs from 15 LTCFs | Lower mental health scores related to work–family conflict; working night shifts; poor sleep quality, but not sleep quantity. | High |
| Author (Year) Country | Study Aims | Study Design, Data Collection | Participants | Key Findings | MMAT |
|---|---|---|---|---|---|
| Beynon (2022) [68] USA | Assess the perception (Aim 1) and explore the experience (Aim 2) of workplace collaboration amongst LNs and CNAs in RACFs | Cross-sectional, questionnaires, interviews | n = 116 (Aim 1). n = 36 (Aim 2) 68 CNAs and 48 LNs from 4 RACFs (Aim 1); 12 CNAs and 12 RNs from 4 RACFs (Aim 2) | Agreement between nurses and CNAs regarding moderate levels of collaboration and teamwork across facilities; belief that collaboration improved quality of care through a shared interest of resident wellbeing. LNs identified that due to hierarchy they were more likely to determine level of co-worker connection. | High |
| Dhakal (2020) [69] Australia | Explore factors related to attraction and retention of ACAs | Cross-sectional, questionnaire | n = 79 ACAs from 11 RACFs | Intention to leave associated with casual roles, younger age of workers, metropolitan location, heavy workloads, lack of teamwork, low staff-to-resident ratios. Retention associated with payrates; job security; promotional opportunities; available working hours. | High |
| Graham (2012) [70] USA | Investigate the prevalence of work-related back injuries in CNAs | Cross-sectional, questionnaire | n = 35 CNAs from NHs | Work related injuries were experienced by almost 50% of respondents. Majority back injuries incurred via patient manual handling. Low staff ratios and poor relationships with supervising nurses reported to be most difficult aspects of jobs. | Mod |
| Leskovic (2020) [71] Slovenia | Assess any change in job satisfaction and burnout of care worker staff in NHs from pre-pandemic to during a pandemic | Recurrent cross-sectional, questionnaire | n = 1188 1079 NAs, 109 nurses from 98 NHs | Burnout syndromes increased prevalence from 2013 to 2020; related to an increase in emotional exhaustion and lowered job satisfaction. Lower job satisfaction in 2020 associated with changes in shift length; lack of breaks worsened job satisfaction. Greater cooperation between staff was noted during the pandemic. | High |
| Author (Year) Country | Study Aims | Study Design, Data Collection | Participants | Key Findings | MMAT |
|---|---|---|---|---|---|
| Adebayo (2023) [72] Australia | Explore the perceptions of migrant care workers regarding job demands coping strategies and intention to stay | Interpretative descriptive, interviews | n = 20 Migrant care workers from RACFs | Motivators to working in aged care included employment availability, attraction to care role. Stressors included resettlement, communication difficulties with residents and co-workers, lack of familiarity with workplace routines, and experience of discrimination. Enablers of retention included flexibility and organisational support. | High |
| Amateau (2023) [73] USA | Explore trauma and resilience related concepts from CNAs experiences in RACF | Grounded theory, focus groups | n = 18 16 current CNAs and 2 former CNAs from 4 RACFs | Stress, strength, and resilience related to identity; relationships with residents; workplace culture and values; personal wellness. | High |
| Bergqvist (2022) [74] Sweden | Understand experiences of CNAs working in RACF during a pandemic | Interpretative descriptive, focus groups | n = 20 NAs from 4 RACFs | Major themes arising from work-related experiences included feelings of abandonment, disrespect, and fear; development of routines and strategies to cope; stress related to irregular staffing and management guidance. | High |
| Booi (2021) [75] Canada | Provide insight into the working conditions and perceptions of CAs working in a RACF | Long qualitative ethnographic study, observations, interviews | n = 31 CAs from 1 RACF | Main views of workers feeling unprepared, insufficient onsite training and stress related to staffing; powerlessness with relation to care decisions; a lack of respect and experience of stigmatisation; feeling overwhelmed and expressing an intention to leave, compelled to stay for resident wellbeing. | High |
| Cooke (2021) [76] Canada | Explore the impact of workplace incivility and bullying on residential CA relationships | Long qualitative ethnographic study, observations, interviews | n = 38 21 CAs, 6 LPNs, 5 administrative, and 6 support staff from 2 LTCFs | Exposure to incivility and bullying found to impact reluctance to request assistance or trust co-workers; sense of judgement around work ethic, with resentment towards staff receiving help from others; reinforcement of declining offers of assistance, leading to unsafe manual handling behaviours amongst newer staff. | High |
| Creapeau (2022) [77] USA | Explore SNF leadership and CNA staff perceptions of challenges related to CNA retention | Interpretative descriptive, interviews | n = 413 295 CNAs, 59 NH administrators, 59 DONs from 59 NHs | Key responses from stakeholder groups identified wages, shortage of candidates with appropriate qualifications, and nature of the job main causes of staffing challenges. NHAs also citing competition/low unemployment rates. All stakeholder groups agreed wages, working relationships, and appreciation the most important things for CNA retention. | Mod |
| Dijxhoorn (2023) [78] Netherlands | Understand NA experiences of providing end-of-life care in NHs | Interpretative descriptive, interviews | n = 17 NAs | Elements impacting care provision included suffering, grief, feelings of unfairness, accumulation of deaths; relationships and interactions with residents and families, receiving gratitude; feelings of fulfilment, powerlessness, and inadequacy. | High |
| Franzosa (2022) [79] USA | Understand the perspectives of staff working in NHs during a pandemic | Interpretative descriptive, interviews, focus groups | n = 62 56 CNAs and 6 administrators from 6 NHs | Identified challenges were staffing shortages, pressure to work when unwell or fatigued. Strategies to improve working conditions included teamwork and communication across direct care staff and management to ensure confidence and safety; accessibility of leadership, mentors, and ongoing training; recognition of work–life balance and mental health impact of working in pandemic conditions. | High |
| Gleason (2016) [80] USA | Understand the experience of HHAs following the death of a client | Interpretative descriptive, interviews | n = 80 HHAs working in community service for eldercare | Over 1/3 felt they could “very much” turn to supervisors for support; less than 1/5 felt they could turn to a co-worker. Low rates (less than 20%) sought support before or after client’s death from either supervisors or co-workers. Most common types of support sought were opportunity to talk; training related to death/dying; being allowed time off; consideration of notification methods to staff. | High |
| Goel (2015) [81] Australia | Understand the experience of migrant aged care workers in a regional area | Interpretative descriptive, focus groups | n = 7 5 PCAs, 1 HCW, 1 AHA | Flexibility of hours, care role, socialisation, and receiving wages improved satisfaction with employment. Time constraints, work demands, poor inter-collegial relationships, and lack of supervision and organisational support reduced satisfaction with employment. | Mod |
| Gray (2017) [82] USA | Explore CNA perceptions of work identity within context of relationships with other staff and residents in SNF | Interpretative descriptive, focus groups | n = 45 CNAs from 4 SNFs | Work-related identity categories were connector (communicating information about residents to supervisors). Provided CNAs with sense of control; advocate (CNAs felt to be in a strong position to detail any needs of residents); overloaded worker (impacted by limited or conflicting direction and emotional/physical exhaustion); companion (sense of importance to residents, compliments, and appreciation increased satisfaction). | High |
| Hoedl (2022) [83] Austria | Understand the experience of working during a pandemic for NH staff | Interpretative descriptive, interviews | n = 18 8 NA, 2 CA, 8 nurses from 5 NHs | Work-related consequences of the pandemic included increase in quantitative and qualitative workload—time resources for PPE, pressure to fill social needs of residents; changes to work organisation—positive communication from multidisciplinary team and organisation, negative aspect inability to take planned leave; physical—wearing PPE, tiredness, and exhaustion; psychological—uncertainty of the situation, stress, fear of infection for self and the residents; social—reduction in contacts outside of NH. | High |
| Holmberg (2013) [84] USA | Explore CNAs perceptions of work roles and work environment on care provision and mental health impacts | Interpretative descriptive, focus groups | n >150 CNAs from 7 NHs | Individual level themes were caregiver as both an identity and holistic practice, with experience of stress when quality care not achieved, concern about resident autonomy and dignity. Organisational level themes included issues with working for large companies, staffing shortages, and relationships with supervisors; perceived lack of respect from resident families or supervisors regarding CNA knowledge/skills or importance of their role. | High |
| Krein (2022) [85] USA | Understand the experience of NH staff and families of residents and perceptions of factors related to turnover | Interpretative descriptive, interviews | n = 42 16 CNA, 9 nurses, 17 family members of residents from 5 NHs | All stakeholder groups reported negative aspects including disruption to care, difference in quality of care, risk of errors. Minimal experience of turnover was reported within some family and NH administrators and noted positive aspects of high retention including consistency of care and increased teamwork. Proposed ways to reduce turnover included increases in wage potentially useful however, direct care staff and families felt this would need to be significantly high to make a difference; administrators and direct care staff identified rapport development, showing staff appreciation, and supporting teamwork. | High |
| Lim (2021) [86] Korea | Explore the influence of work-related care of the elderly on intention to stay and turnover in NH staff | Interpretative descriptive, interviews | n = 10 Care workers from 5 NHs and 5 home care providers | Factors influencing turnover intentions found to be low status of care work within society; employment instability, unprotected labour rights, and safety with absence of training and supervision; low wages and no regulation of wages; emotional/mental health stress. | High |
| Marziali (2015) [87] Canada | Explore the responses of NAs to a self-efficacy educational intervention | Interpretative descriptive, focus groups | n = 164 147 NAs and 17 nurses from 17 LTCFs | CNAs felt training provided novel ways to handle interactions with residents, but not necessarily reflective of complex work situations. Well-functioning teams reported CNA autonomy and feelings of respect for their role; poorly functioning teams reported more stress, little autonomy, and unsatisfactory relationships with supervisors. | High |
| Nichols (2015) [88] Australia | Investigate how multiculturalism shapes and is supported in aged care settings | Interpretative descriptive, interviews | n = 58 30 PCAs, 16 nurses, 5 management, and 5 family members from 6 RACFs | CaLD staff were more likely to have post-high school qualifications than non-CaLD with the majority obtained overseas. Opportunities for employment and aspirational lifestyle were drivers for migration. Migrant staff reported culture shock and limited understanding of dementia. CaLD staff reported experiences of discrimination and mistrust from non-CaLD colleagues. | High |
| Roussillon-Soyer (2021) [89] France | Investigate the psychological impact of absenteeism on nurse and NAs working in NHs | Interpretative descriptive, interviews | n = 42 11 nurses and 31 certified caregivers or noncertified caregivers from 7 NHs | Short-term or last-minute absences placed additional pressure on staff, reducing feelings of control, trust, and stability. Lack of training of recruits and substitutes increases safety risks to staff and residents. Lack of recognition of heavy workload, salaries not representative of contribution, reduction in quality of life due to often increased work hours. Work overload impacting satisfaction with job, pressured to neglect residents due to time constraints. | High |
| Senecal (2019) [90] USA | Understand factors influencing intention to stay in NAs working in SNFs | Interpretative descriptive, interviews | n = 10 NAs from 6 SNFs | Intention to stay supportive factors included work-related self-confidence; positive relationships with residents and appreciation; teamwork and consideration of others in own actions. Intention to stay threatening factors reported as seeking career advancement; difficulty with providing person-centred care due to resources; limited supervisory support and teamwork. | High |
| Sousa-Ribeiro (2022) [91] Sweden | Investigate the experience of older NAs employed in NH as they near retirement | Phenomenology, interviews | n = 8 NAs from 1 NH | Major themes included late-career plans with societal expected retirement age, openness to continue working with more flexibility in selected hours; personal health, work ability, and ageing; perception of work as a health risk due to physical and emotional stress; motives to continue working including financial considerations and meaningfulness of work. | High |
| Titley (2022) [92] Canada | Explore the impact on CAs working in LTCFs during a pandemic | Interpretative descriptive, interviews | n = 52 CAs from 8 LTCFs | Major themes arising included compounding stress associated with enforcing isolation; grief and loss—untimely death of residents; fear of infection for themselves and residents; significant staff shortages and limited direct communication with managers; increased feelings of resilience and optimism. | High |
| Winarnita (2022) [93] Australia | Understand the experience of Asian female migrant aged care workers in regional areas | Interpretative descriptive, interviews, observations | n = 7 PCAs from 7 RACFs | Major themes included overcoming prejudice from residents and locally born peers; the importance of peers with a similar cultural background; the benefits of working within an in-demand sector; the cost-effectiveness of working and living in a regional community; and the challenges of communication being an essential part of the role but coming from an English as a second language background. | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thwaites, C.; McKercher, J.P.; Fetherstonhaugh, D.; Blackberry, I.; Gilmartin-Thomas, J.F.-M.; Taylor, N.F.; Bourke, S.L.; Fowler-Davis, S.; Hammond, S.; Morris, M.E. Factors Impacting Retention of Aged Care Workers: A Systematic Review. Healthcare 2023, 11, 3008. https://doi.org/10.3390/healthcare11233008
Thwaites C, McKercher JP, Fetherstonhaugh D, Blackberry I, Gilmartin-Thomas JF-M, Taylor NF, Bourke SL, Fowler-Davis S, Hammond S, Morris ME. Factors Impacting Retention of Aged Care Workers: A Systematic Review. Healthcare. 2023; 11(23):3008. https://doi.org/10.3390/healthcare11233008
Chicago/Turabian StyleThwaites, Claire, Jonathan P. McKercher, Deirdre Fetherstonhaugh, Irene Blackberry, Julia F-M. Gilmartin-Thomas, Nicholas F. Taylor, Sharon L. Bourke, Sally Fowler-Davis, Susan Hammond, and Meg E. Morris. 2023. "Factors Impacting Retention of Aged Care Workers: A Systematic Review" Healthcare 11, no. 23: 3008. https://doi.org/10.3390/healthcare11233008
APA StyleThwaites, C., McKercher, J. P., Fetherstonhaugh, D., Blackberry, I., Gilmartin-Thomas, J. F.-M., Taylor, N. F., Bourke, S. L., Fowler-Davis, S., Hammond, S., & Morris, M. E. (2023). Factors Impacting Retention of Aged Care Workers: A Systematic Review. Healthcare, 11(23), 3008. https://doi.org/10.3390/healthcare11233008