
The Potential of Digital Screening Tools for Childhood ADHD in School Environments: A Preliminary Study

 , ,
, ,  , and
, and
Abstract
1. Introduction
1.1. Background
1.1.1. ADHD and ENFEN Tests
1.1.2. ADHD and e-Health
1.2. Goal of This Study
2. Materials and Methods
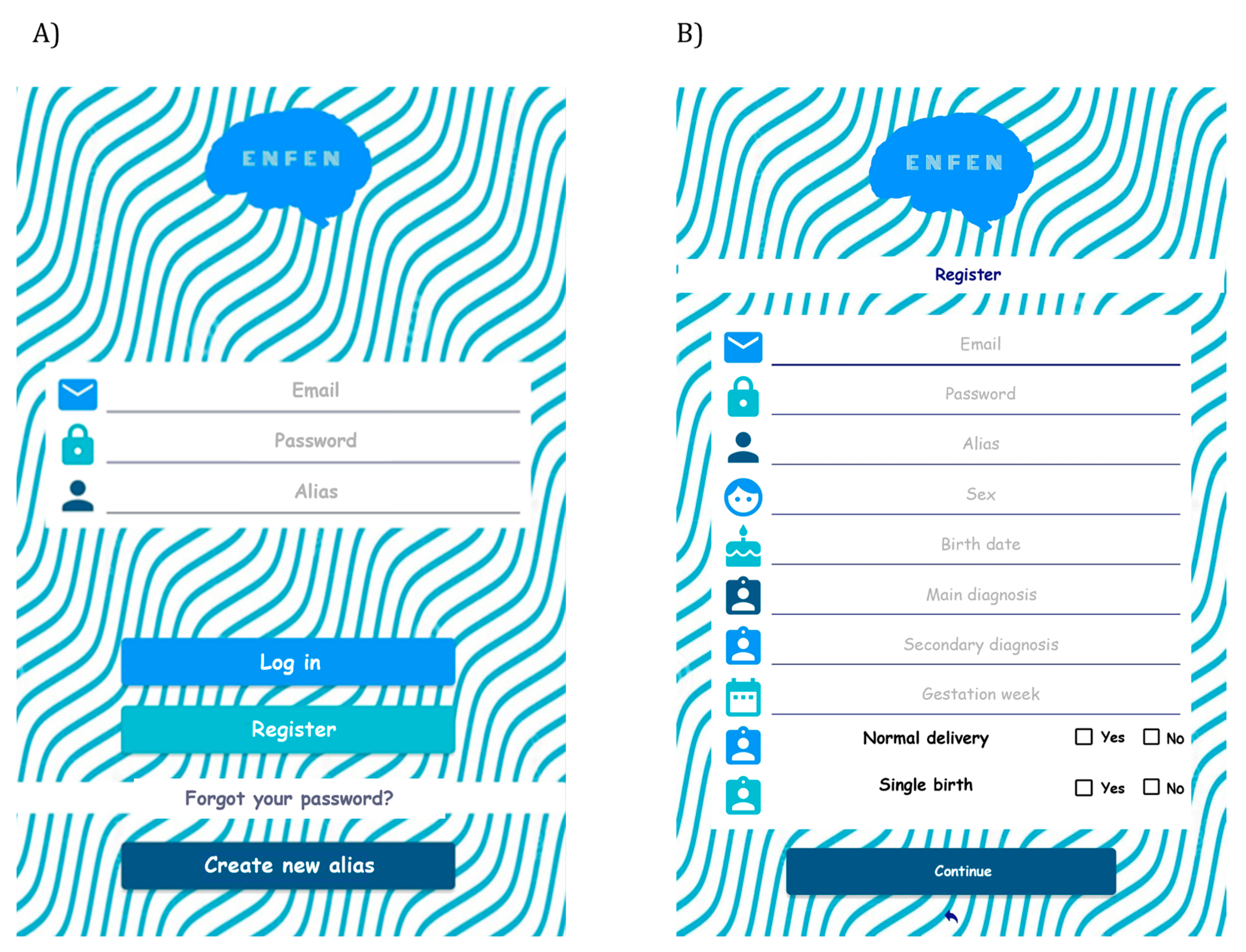
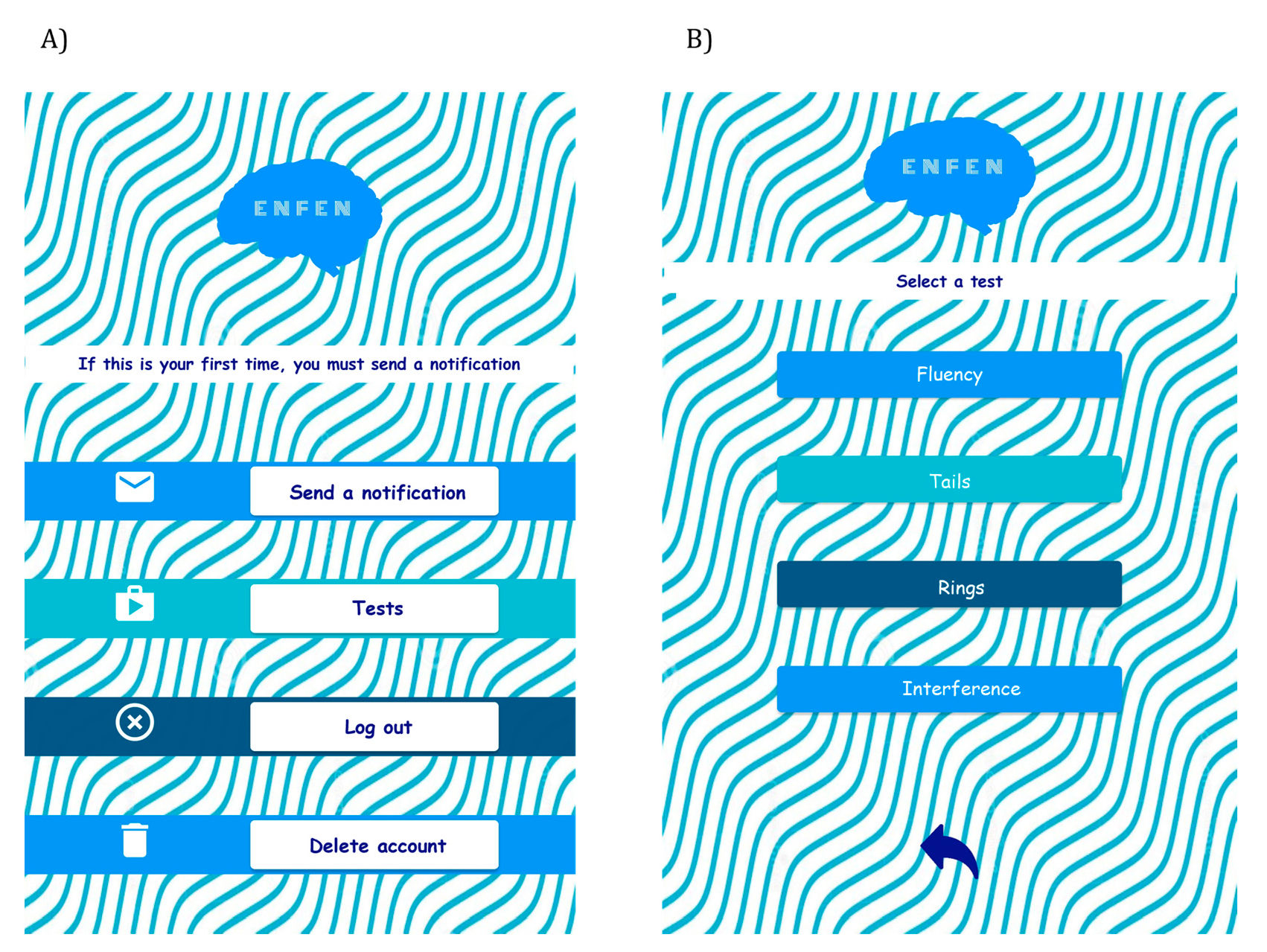
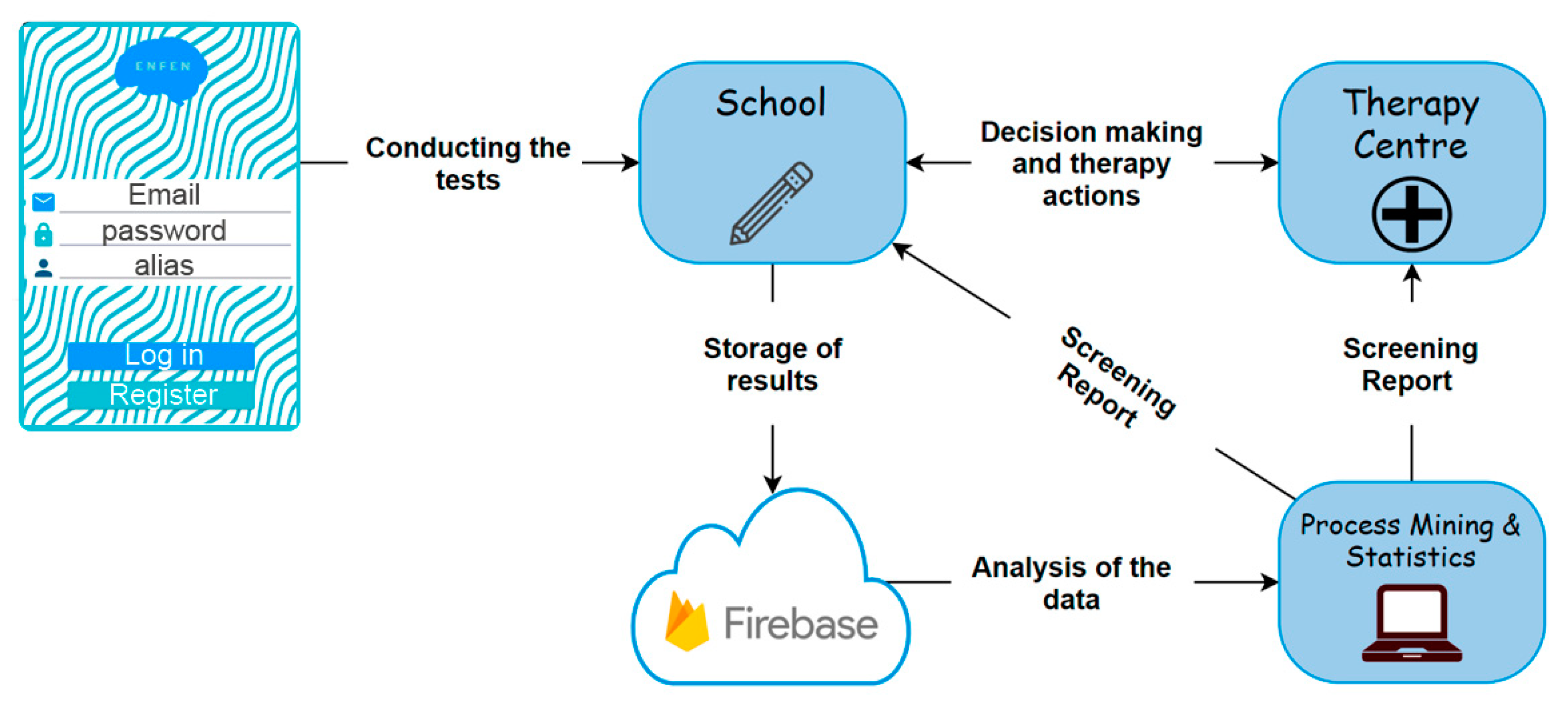
2.1. Application Framework
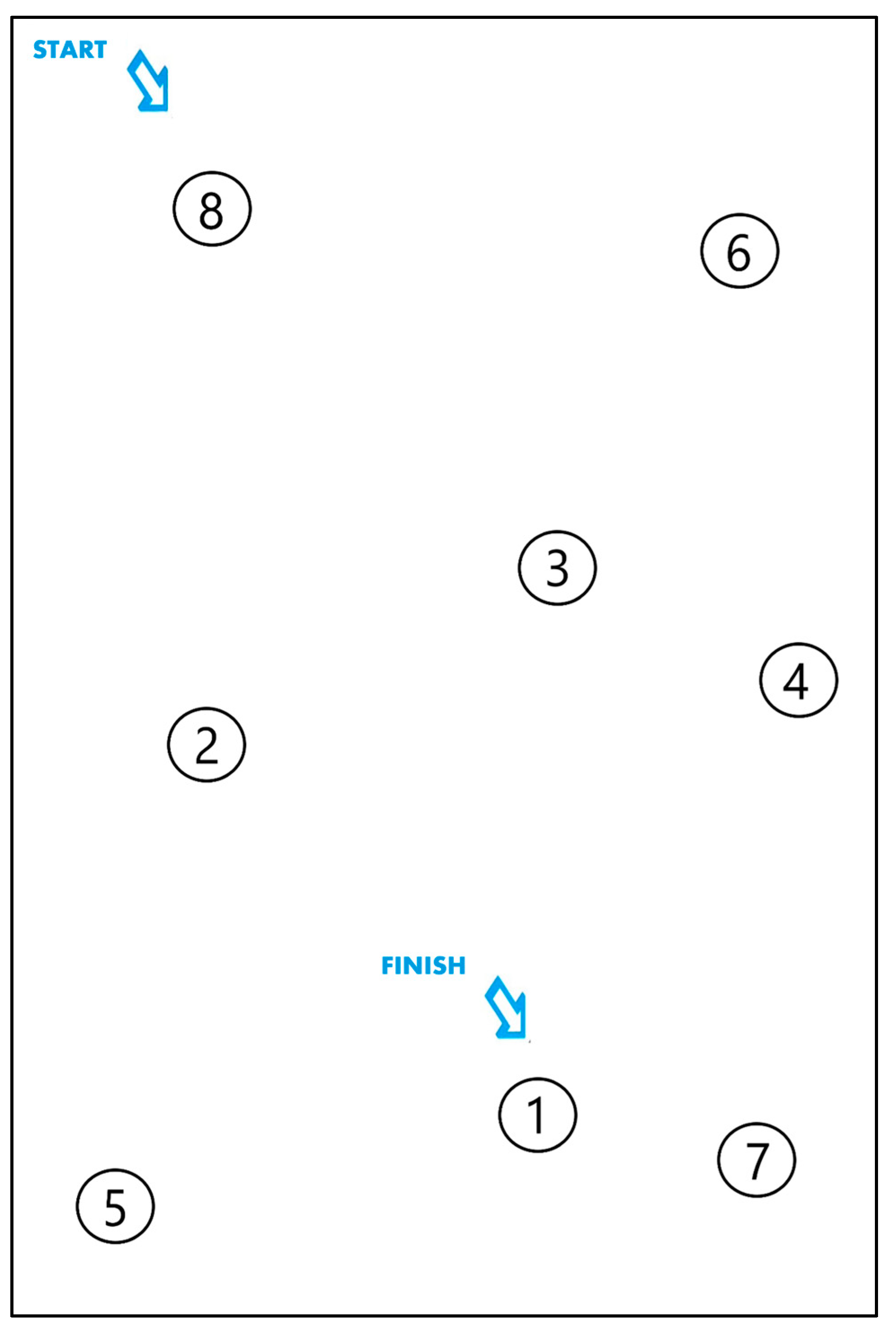
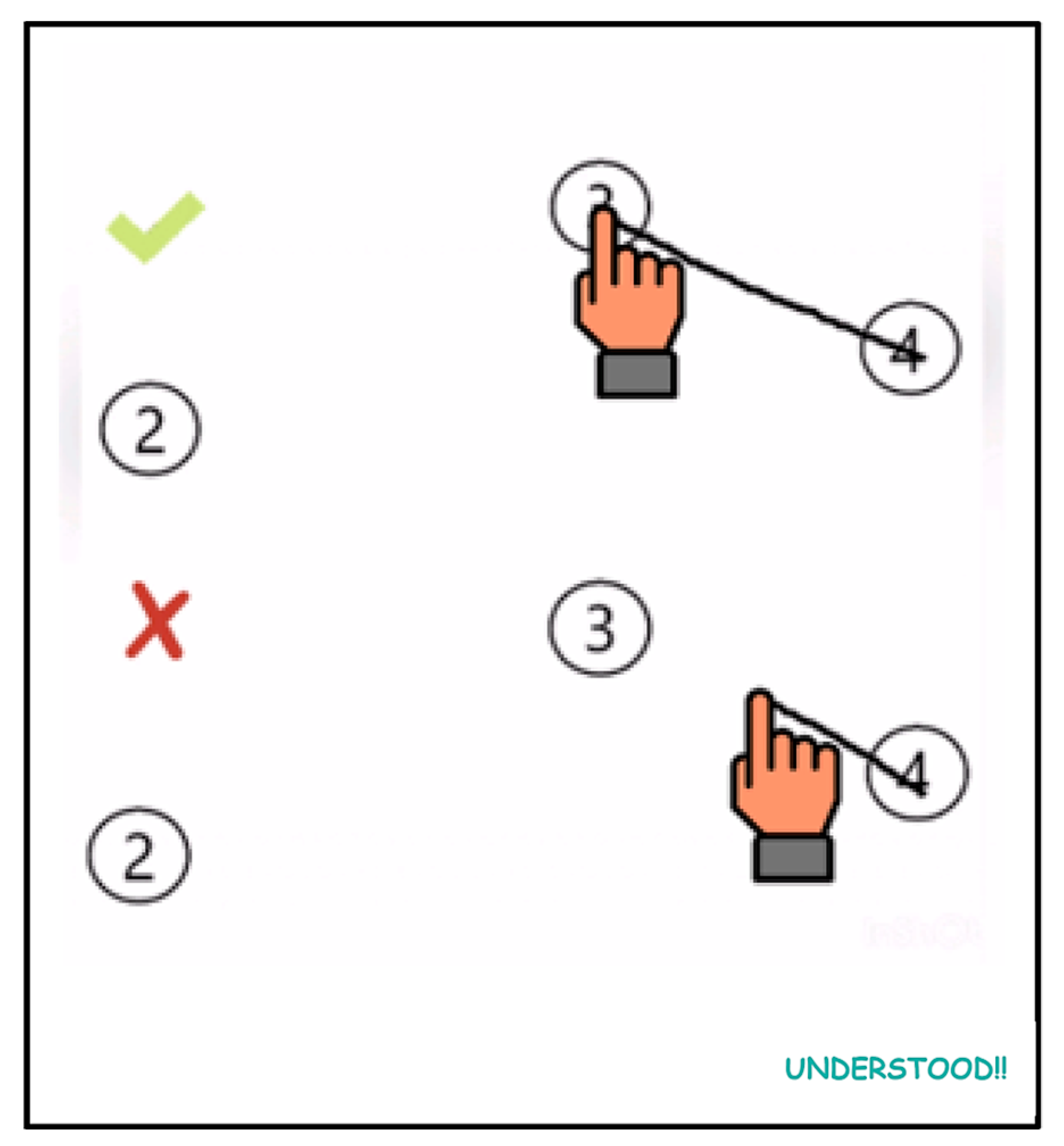
2.2. Test Design
- Start node: the node number from which the path is initiated.
- Target node: the node intentionally chosen as the next step in the path.
- Pressed nodes: the set of nodes collected by the application and considered for calculating the player’s final score.
- Final node: the node that contains the number 1. Once this node is considered a pressed node, the test is completed.
2.3. Hypothesis and Experimental Protocol
2.4. Sample Summary
2.5. Statistical Method
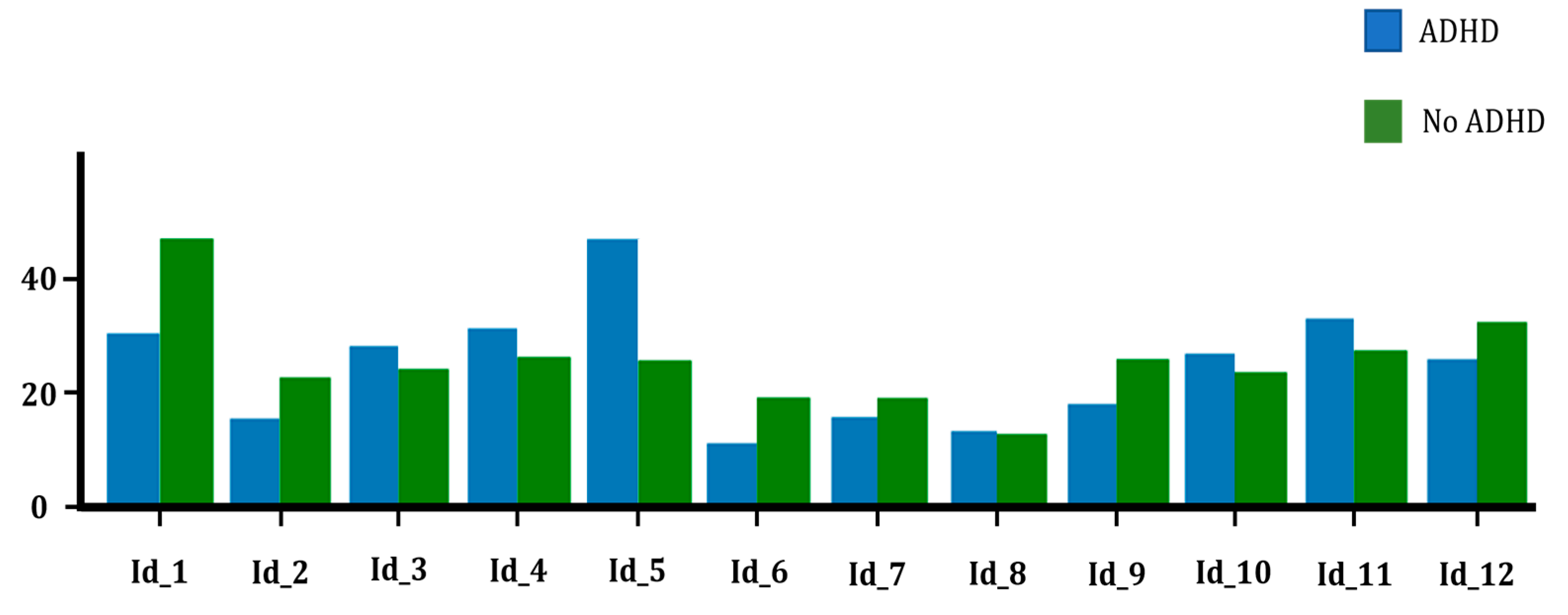
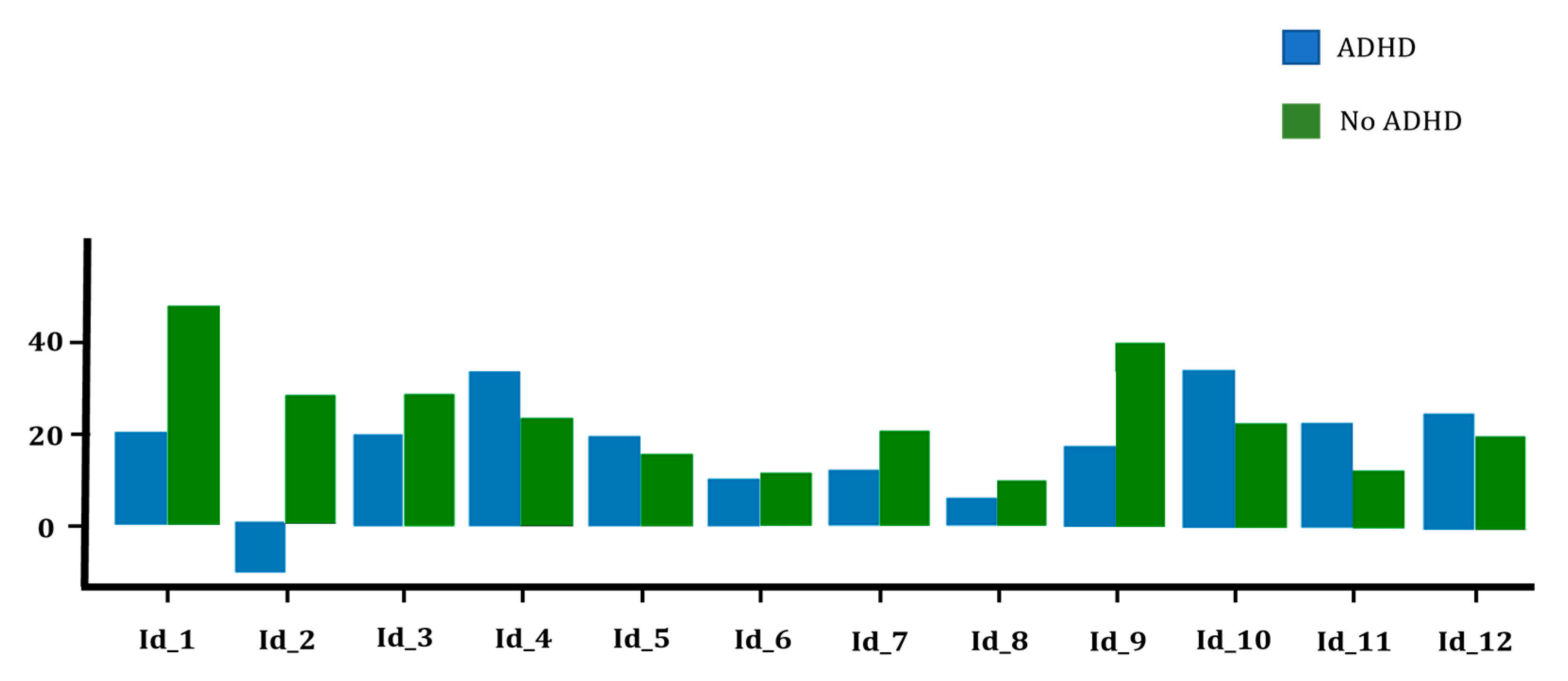
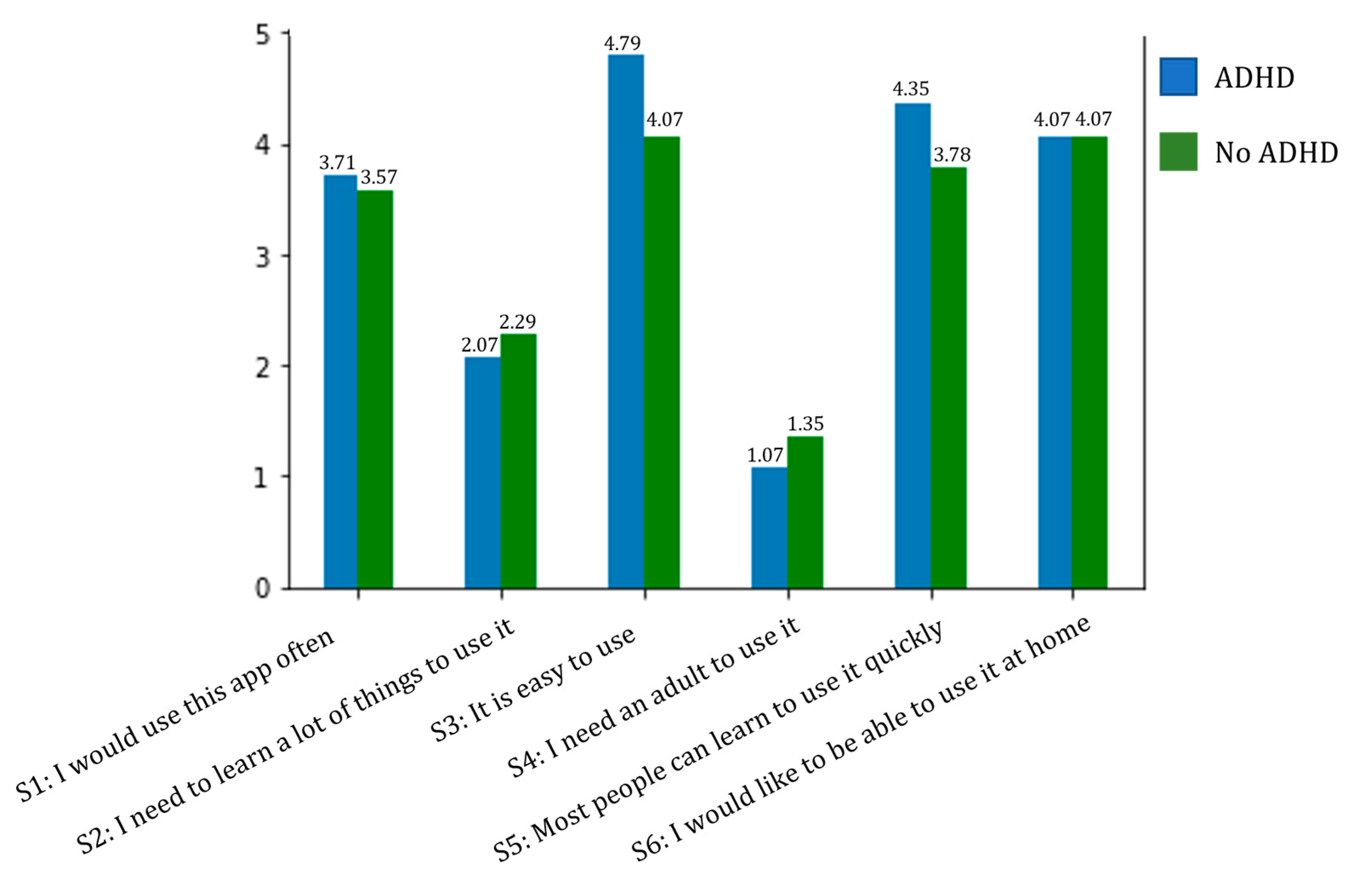
3. Results
Obtained Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tchang, A.; Falcó, D.; Peris, J. Todo lo Que Necesitas Saber Sobre el TDAH en la Etapa de Aprendizaje: Introducción al Trastorno por Déficit de Atención e Hiperactividad; Wolters Kluver: Madrid, Spain, 2020. [Google Scholar]
- Felt, B.T.; Biermann, B.; Christner, J.G.; Kochhar, P.; Van Harrison, R. Diagnosis and management of ADHD in children. Am. Fam. Phys. 2014, 90, 456–464. [Google Scholar]
- Austerman, J. ADHD and behavioral disorders: Assessment, management, and an update from DSM-5. Clevel. Clin. J. Med. 2015, 82 (Suppl. S1), S2–S7. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Han, D.; Luo, H. A virtual reality application for assessment for attention deficit hyperactivity disorder in school-aged children. Neuropsychiatr. Dis. Treat. 2019, 15, 1517–1523. [Google Scholar] [CrossRef]
- Tripp, G.; Wickens, J.R. Neurobiology of ADHD. Neuropharmacology 2009, 57, 579–589. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.J.; Sergeant, J.A.; Nigg, J.; Willcutt, E. Executive dysfunction and delay aversion in attention deficit hyperactivity disorder: Nosologic and diagnostic implications. Child Adolesc. Psychiatr. Clin. N. Am. 2008, 17, 367–384. [Google Scholar] [CrossRef]
- Ramos-Galarza, C.A.; Pérez-Salas, C. Relación entre el modelo híbrido de las funciones ejecutivas y el trastorno por déficit de atención con hiperactividad. Psicol. Caribe 2015, 32, 299–314. [Google Scholar] [CrossRef]
- Navarro-Soria, I.; de Mier, R.J.-R.; García-Fernández, J.M.; González-Gómez, C.; Real-Fernández, M.; de León, M.S.-M.; Lavigne-Cervan, R. Detection of executive performance profiles using the ENFEN battery in children diagnosed with attention-deficit hyperactivity disorder. Front. Psychol. 2020, 11, 552322. [Google Scholar] [CrossRef]
- Benzing, V.; Schmidt, M. The effect of exergaming on executive functions in children with ADHD: A randomized clinical trial. Scand. J. Med. Sci. Sports 2019, 29, 1243–1253. [Google Scholar] [CrossRef]
- Tamm, L.; Nakonezny, P.A. Metacognitive executive function training for young children with ADHD: A proof-of-concept study. Atten. Deficit Hyperact. Disord. 2015, 7, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Shuai, L.; Daley, D.; Wang, Y.F.; Zhang, J.S.; Kong, Y.T.; Tan, X.; Ji, N. Executive Function Training for Children with Attention Deficit Hyperactivity Disorder. Chin. Med. J. 2017, 130, 549–558. [Google Scholar] [CrossRef]
- Portellano, J.A.; Martínez, R.; Zumárraga, L. Manual ENFEN: Evaluación Neuropsicológica de las Funciones Ejecutivas en Niños; Hogrefe TEA Edicones: Madrid, Spain, 2009. [Google Scholar]
- Bowie, C.R.; Harvey, P.D. Administration and interpretation of the Trail Making Test. Nat. Protoc. 2006, 1, 2277–2281. [Google Scholar] [CrossRef]
- Oh, H.; Jadad, A.; Rizo, C.; Enkin, M.; Powell, J.; Pagliari, C. What is eHealth (3): A systematic review of Published Definitions. J. Med. Internet Res. 2005, 7, e110. [Google Scholar] [CrossRef] [PubMed]
- Pandria, N.; Spachos, D.; Bamidis, P.D. The future of mobile health: ADHD applications. In Proceedings of the International Conference on Interactive Mobile Communication Technologies and Learning (IMCL), Thessaloniki, Greece, 19–20 November 2015. [Google Scholar] [CrossRef]
- Istepanian, R.; Laxminarayan, S.; Pattiches, C.S. M-Health: Emerging Mobile Health System; Springer Science & Business Media: Berlin, Germany, 2006. [Google Scholar]
- Ryan, G.S.; Haroon, M.; Melvin, G. Evaluation of an educational website for parents of children with ADHD. Int. J. Med. Inform. 2015, 84, 974–991. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, E.J.; Dewald-Kaufmann, J.F.; Oort, F.J.; Bögels, S.M.; Meijer, A.M. Differential effects of online insomnia treatment on executive functions in adolescents. Sleep Med. 2015, 16, 510–520. [Google Scholar] [CrossRef]
- Olsen, M.R.; Casado-Lumbreras, C.; Colombo-Palacios, R. ADHD in eHealth—A Systematic literature review. Procedia Comput. Sci. 2016, 100, 207–214. [Google Scholar] [CrossRef][Green Version]
- Myers, K.; Vander Stoep, A.; Zhou, C.; McCarty, C.A.; Katon, W. Effectiveness of a telehealth service delivery model for treating Attention-Deficit Hyperactivity Disorder: A community-based randomized controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 263–274. [Google Scholar] [CrossRef]
- Baum, R.A.; Epstein, J.N.; Kelleher, K. Healthcare reform, quality, and technology: ADHD as a case study. Curr. Psychiatry Rep. 2003, 15, 369. [Google Scholar] [CrossRef]
- Silva, B.M.C.; Rodrigues, J.J.P.C.; de la Torre Díez, I.; López-Coronado, M.; Saleem, K. Mobile-health: A review of current state in 2015. J. Biomed. Inform. 2015, 56, 265–272. [Google Scholar] [CrossRef]
- Wu, L.-T.; Gersing, K.; Burchett, B.; Woody, G.E.; Blazer, D.G. Substance use disorders and comobird Axis I and II psychiatric disorders among young psychiatric patients: Findings from a large electronic health records database. J. Psychiatr. Res. 2011, 45, 1453–1462. [Google Scholar] [CrossRef]
- Geissbuhler, A.; Safran, C.; Buchan, I.; Bellazzi, R.; Labkoff, S.; Eilenberg, K.; Leese, A.; Richardson, C.; Mantas, J.; Murray, P.; et al. Trustworthy reuse of health data: A transnational perspective. Int. J. Med. Inform. 2013, 82, 1–9. [Google Scholar] [CrossRef]
- Van Allen, J.; Davis, A.M.; Lassen, S. The use of telemedicine in pediatric psychology: Research review and current applications. Child Adolesc. Psychiatr. Clin. N. Am. 2011, 20, 55–66. [Google Scholar] [CrossRef][Green Version]
- Bashiri, A.; Ghazisaeedi, M. The effectiveness of mHealth apps in the rehabilitation of children with Attention-Deficit Hyperactivity Disorder. Iran. J. Public Health 2018, 47, 140–142. Available online: https://ijph.tums.ac.ir/index.php/ijph/article/view/12060 (accessed on 9 May 2023).
- Reese, R.M.; Jamison, R.; Wendland, M.; Fleming, K.; Braun, M.J.; Turek, J. Evaluating interactive videoconferencing for assessing symptoms of autism. Telemed. J. E Health 2013, 19, 671–677. [Google Scholar] [CrossRef]
- Elford, R.; White, H.; Bowering, R.; Ghandi, A.; Maddiggan, B.; John, K.S. A randomized, controlled trial of child psychiatric assessments conducted using videoconferencing. J. Telemed. Telecare 2000, 6, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Kemppinen, J.; Korpela, J.; Partners, R.; Elfvengren, K.; Salmisaari, T.; Polkko, J.; Tuominen, M. A clinical decision support system for adult ADHD diagnosis process. In Proceedings of the Hawaii International Conference on System Sciences, Wailea, HI, USA, 7–10 January 2013. [Google Scholar] [CrossRef]
- Abdelnour, E.; Jansen, M.O.; Gold, J.A. ADHD Diagnostic Trends: Increased Recognition or Overdiagnosis? Mo. Med. 2022, 119, 467–473. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual for Mental Disorders (DSM-5), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013; ISBN 978-0-89042-576-3. [Google Scholar]
- Regier, D.A.; Narrow, W.E.; Kuhl, E.A.; Kupfer, D.J. The conceptual development of DSM-V. Am. J. Psychiatry 2009, 166, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.S. A critical review of ADHD diagnostic criteria: What to address in the DSM-V. J. Atten. Disord. 2010, 15, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Buñuel Álvarez, J.C. Diagnostico del trastorno de déficit de atención con/sin hiperactividad. Una visión desde la evidencia científica. Rev. Pediatría Atención Primaria 2006, 3, 25–37. Available online: https://pap.es/files/1116-591-pdf/616.pdf (accessed on 25 August 2023).
- Chen, Y.; Zhang, Y.; Jiang, X.; Zeng, X.; Sun, R.; Yu, H. COSA: Contextualized and objective system to support ADHD diagnosis. In Proceedings of the IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Madrid, Spain, 3–6 December 2018. [Google Scholar]
- Frank, M.C.; Sugarman, E.; Horowitz, A.C.; Lewis, M.L.; Yurovsky, D. Using tablets to collect data from young children. J. Cogn. Dev. 2016, 17, 1–17. [Google Scholar] [CrossRef]
- Kodular: Much More Than a Modern App Creator without Coding. Kodular. Available online: https://www.kodular.io/ (accessed on 21 September 2023).
- Firebase: Make Your App the Best It Can, Be. Google. Available online: https://firebase.google.com/?hl=es (accessed on 21 March 2023).
- Woolson, R.F. Wilcoxon signed-rank test. In Wiley Encyclopaedia of Clinical Trials; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2008. [Google Scholar] [CrossRef]
- Gu, D.; Lin, A.; Lin, G. Detection of Attention Deficit Hyperactivity Disorder in children using CEEMDAN-based cross frequency symbolic convergent cross mapping. Expert Syst. Appl. 2023, 226, 120105. [Google Scholar] [CrossRef]
- Kooij, S.J.; Bejerot, S.; Blackwell, A.; Caci, H.; Casas-Brugué, M.; Carpentier, P.J.; Edvinsson, D.; Fayyad, J.; Foeken, K.; Fitzgerald, M.; et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD. BMC Psychiatry 2010, 10, 67. [Google Scholar] [CrossRef] [PubMed]
- De la Peña Olvera, F.; Palacio Ortiz, J.D.; Barragán Pérez, E. Declaración de Cartagena para el trastorno por déficit de atención con hiperactividad (TDAH): Rompiendo el estigma. Rev. Cienc. De La Salud 2010, 8, 95–100. [Google Scholar]
- Cardo, E.; Ros-Cervera, G.; Eiris-Punal, J.; Escofet-Soteras, C.; Fernandez-Jaen, A.; Mulas, F.; Sanchez-Carpintero, R.; Sans, A. Current state of the attention deficit hyperactivity disorder approach in neuropediatrics. Rev. Neurol. 2017, 64, S105–S109. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Implementation Aspects | Description |
|---|---|
| Area of the nodes | The node area should be adequately adjusted. Therefore, if a child is moving towards the target node and happens to pass close to another node while defining their path, the latter should not appear as pressed |
| Pass over a node | Among the rules, it is possible to pass over other nodes on the screen while moving towards the target node. In such cases, those numbers should not be considered as pressed nodes and therefore should not be included in the final result |
| Total time required | The time elapsed from when the player presses the “understood” button until they reach the final node |
| Test rules | The method for explaining the rules must be agreed upon with the specialist, as it is a crucial requirement |
| Measurement of inactivity | The test implementation aims to redirect the individual’s attention in case it detects a period of inactivity |
| Age (Years) | ||||||||
|---|---|---|---|---|---|---|---|---|
| 6 | 7 | 8 | 9 | 10 | 11 | 12 | Total | |
| Female | 2 | 2 | 1 | 1 | 3 | 1 | 2 | 12 |
| Male | 1 | 3 | 1 | 3 | 2 | 4 | 2 | 16 |
| Total | 3 | 5 | 2 | 4 | 5 | 5 | 4 | 28 |
| ADHD Diagnosis | |||
|---|---|---|---|
| Yes | No | Total | |
| Female | 4 | 8 | 12 |
| Male | 10 | 6 | 16 |
| Total | 14 | 14 | 28 |
| Age Avg. | Gestation Weeks Avg. | Normal Birth | ||||
|---|---|---|---|---|---|---|
| ADHD | No ADHD | ADHD | No ADHD | ADHD | No ADHD | |
| Female | 9.25 | 8.87 | 39.25 | 39.25 | 3 | 7 |
| Male | 9.8 | 8.67 | 39.5 | 39.5 | 5 | 3 |
| Hits Avg. | Substitutions Avg. | Omissions Avg. | Time Spent Avg. (s) | Final Score Avg. | |
|---|---|---|---|---|---|
| ADHD | 18.69 | 0.23 | 0.38 | 92.69 | 19.50 |
| No ADHD | 18.91 | 0.08 | 0.25 | 87.83 | 21.15 |
| Hits Avg. | Substitutions Avg. | Omissions Avg. | Time Spent Avg. (s) | Final Score Avg. | |
|---|---|---|---|---|---|
| ADHD | 16.84 | 2 | 0 | 108.76 | 13.64 |
| No ADHD | 18.75 | 0.17 | 0.08 | 100.83 | 18.34 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabaldón-Pérez, A.-M.; Martín-Ruiz, M.-L.; Díez-Muñoz, F.; Dolón-Poza, M.; Máximo-Bocanegra, N.; Pau de la Cruz, I. The Potential of Digital Screening Tools for Childhood ADHD in School Environments: A Preliminary Study. Healthcare 2023, 11, 2795. https://doi.org/10.3390/healthcare11202795
Gabaldón-Pérez A-M, Martín-Ruiz M-L, Díez-Muñoz F, Dolón-Poza M, Máximo-Bocanegra N, Pau de la Cruz I. The Potential of Digital Screening Tools for Childhood ADHD in School Environments: A Preliminary Study. Healthcare. 2023; 11(20):2795. https://doi.org/10.3390/healthcare11202795
Chicago/Turabian StyleGabaldón-Pérez, Ana-Marta, María-Luisa Martín-Ruiz, Fernando Díez-Muñoz, María Dolón-Poza, Nuria Máximo-Bocanegra, and Iván Pau de la Cruz. 2023. "The Potential of Digital Screening Tools for Childhood ADHD in School Environments: A Preliminary Study" Healthcare 11, no. 20: 2795. https://doi.org/10.3390/healthcare11202795
APA StyleGabaldón-Pérez, A.-M., Martín-Ruiz, M.-L., Díez-Muñoz, F., Dolón-Poza, M., Máximo-Bocanegra, N., & Pau de la Cruz, I. (2023). The Potential of Digital Screening Tools for Childhood ADHD in School Environments: A Preliminary Study. Healthcare, 11(20), 2795. https://doi.org/10.3390/healthcare11202795