


Effectiveness of mHealth Interventions for Monitoring Antenatal Care among Pregnant Women in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Studies for the Review
- Types of studies—All published randomised, quasi-experimental, and cluster randomised trials were included in this analysis. After making an unsuccessful effort to contact the study author for more information, studies reported in abstract form, without adequate information on study methods, or where the findings were ambiguous were excluded. This systematic analysis excluded studies involving case reports, case studies, editorials, perspectives, literature reviews, conference abstracts, observational studies, commentaries, and studies published in languages other than English.
- b.
- Types of participants—Pregnant women (from the first trimester to the third trimester) (up to delivery) in LMICs.
- -
- The pregnant women were followed by routine care with mHealth intervention and utilized a mobile application.
- c.
- Types of interventions—mHealth application for monitoring antenatal health intervention activities—short message service (SMS), voice calling, voice messaging, notification alerts through a mobile application, and IVRS (interactive voice response system).
- d.
- Types of outcome measures
- Primary outcomes for the mother: ANC attendance
2.2. Search Methods for the Identification of Studies
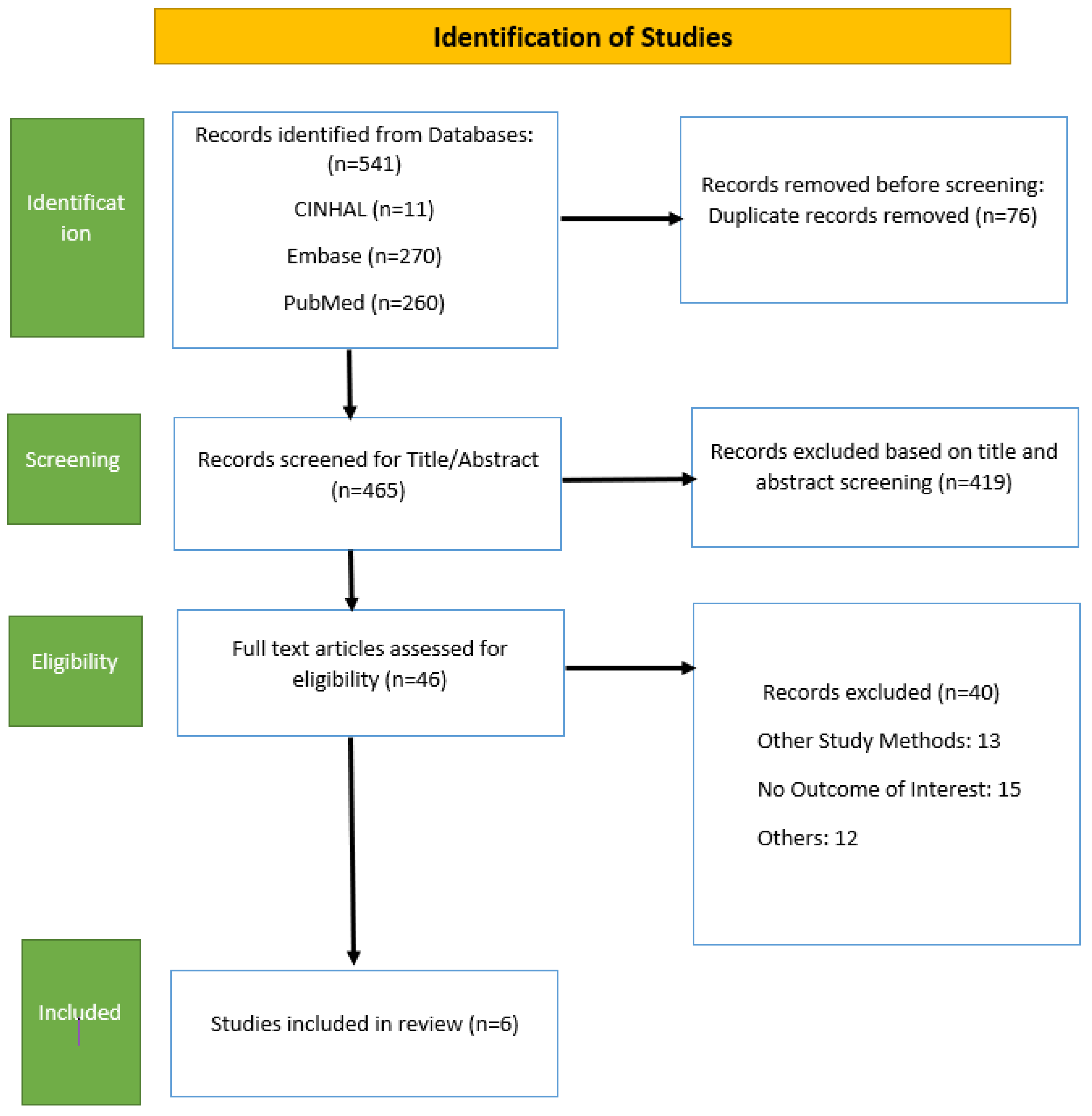
- Data sources and search strategy—This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines [21]. We comprehensively searched the MEDLINE, Embase, and CINAHL databases from inception from January to May 2022. Additional citations were sought from the references in articles retrieved through searches.
2.3. Data Collection and Analysis
- Selection of studies—The studies were selected independently by two reviewers (MM and DP) by reading their titles and abstracts through the use of Rayyan software, and disagreements were resolved through discussion with a third reviewer (JM). Full articles were retrieved for studies that did not provide a summary or had a scant abstract to determine their eligibility for inclusion. Two review authors (MM and DP) independently evaluated the full texts of the remaining papers for inclusion. Disagreements between them were solved through discussion and concord. A third review author was involved in deciding if no conclusion was reached. Details of the screening are provided below in the PRISMA flow chart.
- Data extraction and management—Using a predesigned data extraction form, two review authors individually retrieved the following information: (1) study information (study ID, date of extraction, title, authors, and source of study if not published); (2) study characteristics (study design, sample size, and inclusion/exclusion criteria used in the study, geographical location, and setting); (3) characteristics of the participants, including population type and mean age; (4) details of interventions; and (5) outcomes as described in the outcome measures above.
- Assessment of risk of bias in the included studies—We used the ‘Revman risk of bias’ assessment tool to assess the risk of bias for the included studies. Two review authors (JM and DS) independently evaluated the risk of bias in the included studies—the details are presented in Table 1 (risk of bias table). Disagreements were resolved through discussion or a conversation with a third review author.
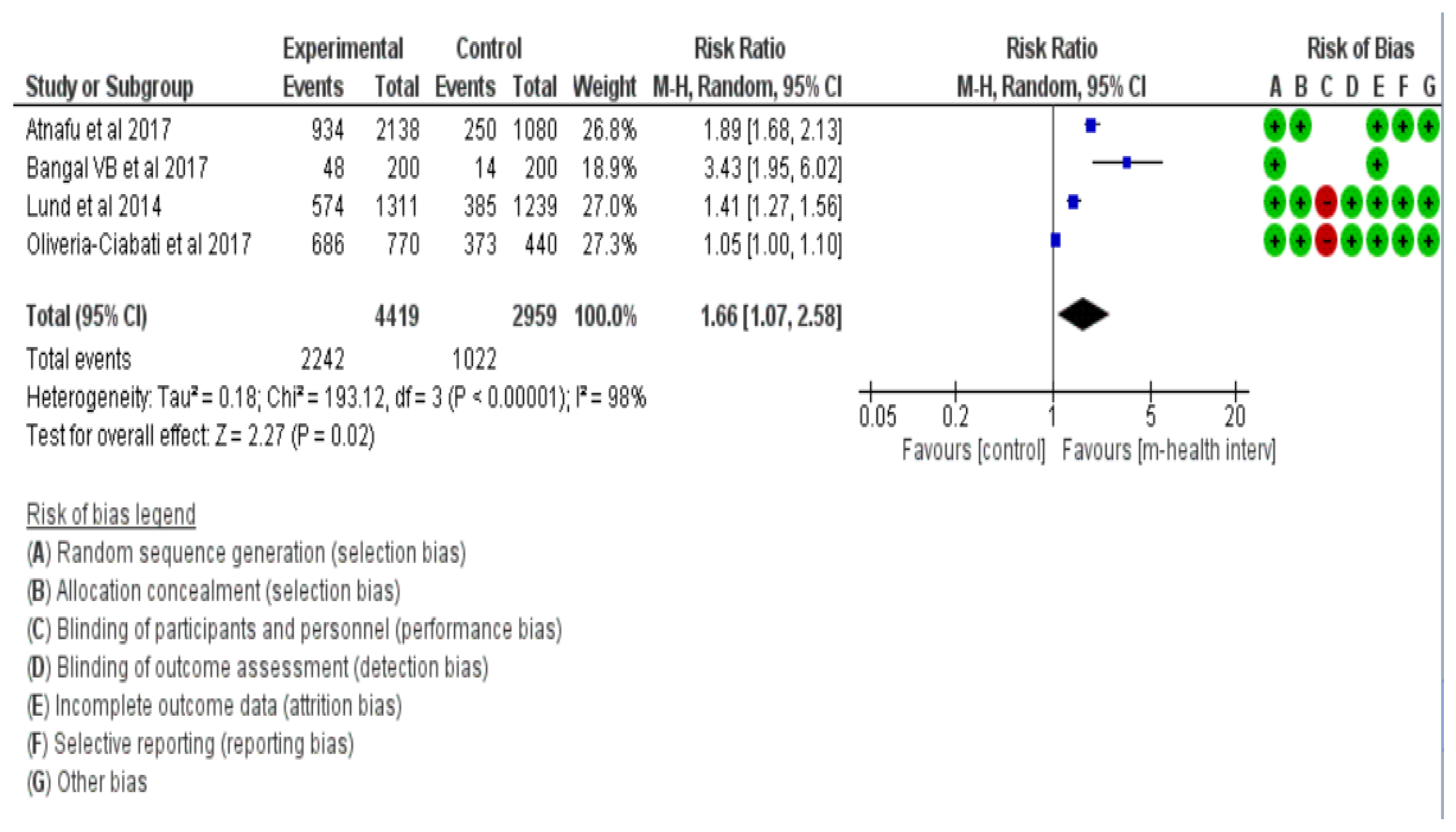
- Measurement of treatment effect—The statistical analysis was executed according to [22]. We expressed effect measures as risk ratios and risk differences with 95% confidence intervals in the case of dichotomous outcomes. Based on the numerator and denominator of the studies where the risk ratio was not reported, we calculated the risk ratio between mothers who used a mobile phone and those who did not in both the intervention and control arms.
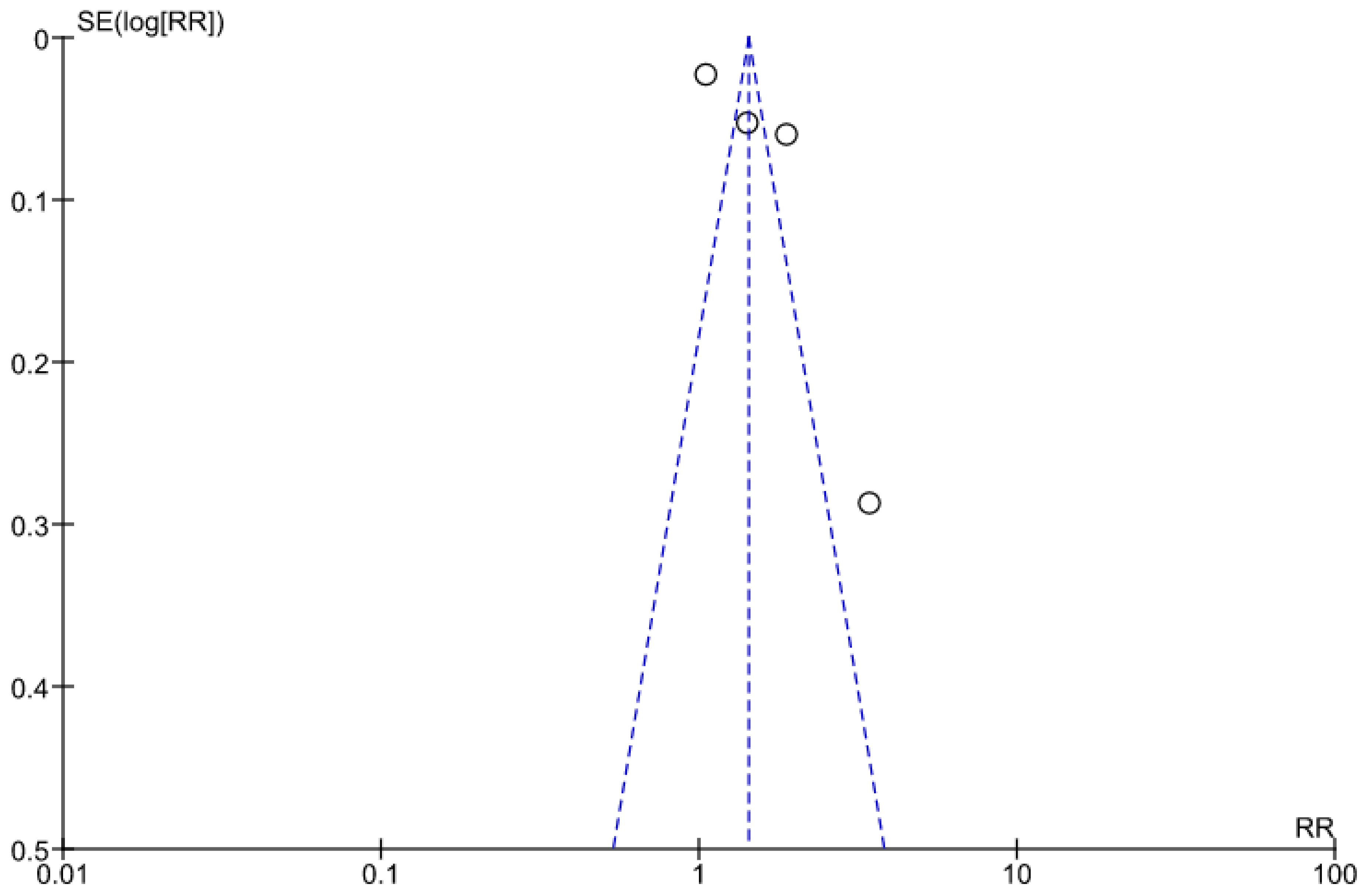
- Assessment of reporting bias—By determining whether the study was registered in a trial registry, a protocol was accessible, and an outcome was provided in the methods section, reporting bias was evaluated. The list of results from those sources was contrasted with the results mentioned in the paper that was published. An inverted funnel plot was used to assess potential publication bias.
- Data synthesis—We used Review Manager 5 software (version 5.4) to carry out the meta-analysis for this study. The meta-analysis was carried out by statistically combining the pregnancy outcomes of increased attendance at antenatal check-ups in various studies. The statistical analyses were carried out according to [22]. We conducted a random-effect meta-analysis where appropriate. We used funnel plots to assess publication bias in the meta-analysis with I2 value and heterogeneity.
- Quality of evidence—A quality check of the evidence was carried out by Review Manager 5 software (version 5.4) using the risk of bias tool depicting the included studies at high, low, or moderate risk. In all analyses, a p-value of less than 0.05 was considered statistically significant.
3. Results
3.1. Identification and Characteristics of Included Studies for SR and MA
3.2. Results for ANC Attendance
4. Discussion
4.1. Policy Implications
- Cost-effective interventions: When compared to traditional healthcare services, mHealth interventions have the potential to improve maternal health outcomes at a lower cost. When making decisions about maternal health care, policymakers should consider the cost-effectiveness of these interventions.
- Accessibility of technology: Policymakers should prioritise increasing access to mobile phones and Internet services, as these are essential for mHealth interventions to be effective. This may involve increasing investment in telecommunication infrastructure and making Internet and mobile phone services more affordable [38].
- Capacity building: India has launched various initiatives to improve public healthcare infrastructure, including the National Rural Health Mission (NRHM) and the Indian Public Health Standards (IPHS). Structural changes have been proposed to provide quality care to rural populations, and training and capacity building of healthcare personnel is critical. Policymakers must prioritise building the capacity of healthcare workers to deliver effective mHealth interventions, including training on the use of mHealth tools and ensuring access to necessary resources [39].
- Monitoring and evaluation: To ensure the effectiveness and sustainability of mHealth interventions for maternal health outcomes, policymakers should prioritise monitoring and evaluating their impact. In resource-limited settings, mHealth interventions should be considered by public health practitioners, policymakers, and researchers. This study’s findings and evidence-based recommendations could be useful in addressing maternal healthcare challenges in low- and middle-income countries (LMICs) through the use of various mHealth interventions, thereby contributing to the achievement of the Sustainable Development Goal of Maternal and Child Health [40,41].
4.2. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Masoi, T.J.; Kibusi, S.M. Improving pregnant women’s knowledge on danger signs and birth preparedness practices using an interactive mobile messaging alert system in Dodoma region, Tanzania: A controlled quasi experimental study. Reprod. Health 2019, 16, 177. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Sathi, N.J.; Abdullah, H.M.; Naime, J.; Butt, Z.A. Factors affecting the utilisation of antenatal care services during pregnancy in Bangladesh and 28 other low-and middle-income countries: A meta-analysis of demographic and health survey data. Dr. Sulaiman Al Habib Med. J. 2022, 4, 19–31. [Google Scholar] [CrossRef]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. 2016. Available online: https://www.who.int/publications/i/item/9789241549912 (accessed on 4 February 2023).
- National Health Mission. Guidelines for—Antenatal Care and Skilled Attendance at Birth. Available online: https://nhm.gov.in/images/pdf/programmes/maternal-health/guidelines/sba_guidelines_for_skilled_attendance_at_birth.pdf (accessed on 4 February 2023).
- Jinga, N.; Mongwenyana, C.; Moolla, A.; Malete, G.; Onoya, D. Reasons for late presentation for antenatal care, healthcare providers’ perspective. BMC Health Serv. Res. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.who.int/news/item/05-10-2021-new-global-targets-to-prevent-maternal-deaths (accessed on 4 February 2023).
- Available online: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (accessed on 4 February 2023).
- Available online: https://data.unicef.org/topic/maternal-health/antenatal-care/ (accessed on 4 February 2023).
- Kumar, G.; Choudhary, T.S.; Srivastava, A.; Upadhyay, R.P.; Taneja, S.; Bahl, R.; Martines, J.; Bhan, M.K.; Bhandari, N.; Mazumder, S. Utilisation, equity and determinants of full antenatal care in India: Analysis from the National Family Health Survey 4. BMC Pregnancy Childbirth 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Vallely, L.M.; Calvert, B.; De Silva, M.; Panisi, L.; Babona, D.; Bolnga, J.; Duro-Aina, T.; Noovao-Hill, A.; Naidu, S.; Leisher, S.; et al. Improving maternal and newborn health and reducing stillbirths in the Western Pacific Region–Current situation and the way forward. Lancet Reg. Health-West. Pac. 2022, 13, 100653. [Google Scholar] [CrossRef]
- van den Broek, N. Content and quality–integrated, holistic, one-stop antenatal care is needed for all. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 558. [Google Scholar] [CrossRef][Green Version]
- Available online: https://www.unicef.org/india/what-we-do/maternal-health (accessed on 6 February 2023).
- Maternal Health—National Health Mission. Available online: https://nhm.gov.in/index1.php?lang=1&level=2&sublinkid=822&lid=218 (accessed on 6 February 2023).
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: A systematic review. PLoS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef]
- Wagnew, F.; Dessie, G.; Alebel, A.; Mulugeta, H.; Belay, Y.A.; Abajobir, A.A. Does short message service improve focused antenatal care visit and skilled birth attendance? A systematic review and meta-analysis of randomised clinical trials. Reprod. Health 2018, 15, 191. [Google Scholar] [CrossRef]
- Modi, D.; Dholakia, N.; Gopalan, R.; Venkatraman, S.; Dave, K.; Shah, S.; Desai, G.; Qazi, S.A.; Sinha, A.; Pandey, R.M.; et al. mHealth intervention “ImTeCHO” to improve delivery of maternal, neonatal, and child care services—A cluster-randomised trial in tribal areas of Gujarat, India. PLoS Med. 2019, 16, e1002939. [Google Scholar] [CrossRef]
- Yadav, P.; Kant, R.; Kishore, S.; Barnwal, S.; Khapre, M. The Impact of Mobile Health Interventions on Antenatal and Postnatal Care Utilization in Low-and Middle-Income Countries: A Meta-Analysis. Cureus 2022, 14, e21256. [Google Scholar] [CrossRef]
- Rahman, M.O.; Yamaji, N.; Nagamatsu, Y.; Ota, E. Effects of mHealth Interventions on Improving Antenatal Care Visits and Skilled Delivery Care in Low-and Middle-Income Countries: Systematic Review and Meta-analysis. J. Med. Internet Res. 2022, 24, e34061. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.; Eriksen, J.; Black, V.; Thorson, A.; Hatcher, A. The mobile alliance for maternal action text message–Based mHealth intervention for maternal care in South Africa: Qualitative user study. JMIR Hum. Factors 2020, 7, e14078. [Google Scholar] [CrossRef] [PubMed]
- Murthy, N.; Chandrasekharan, S.; Prakash, M.P.; Ganju, A.; Peter, J.; Kaonga, N.; Mechael, P. Effects of an mHealth voice message service (mMitra) on maternal health knowledge and practices of low-income women in India: Findings from a pseudo-randomised controlled trial. BMC Public Health 2020, 20, 820. [Google Scholar] [CrossRef] [PubMed]
- Available online: http://www.prisma-statement.org/PRISMAStatement/FlowDiagram (accessed on 7 February 2023).
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook (accessed on 18 February 2023).
- Lund, S.; Nielsen, B.B.; Hemed, M.; Boas, I.M.; Said, A.; Said, K.; Makungu, M.H.; Rasch, V. Mobile phones improve antenatal care attendance in Zanzibar: A cluster randomised controlled trial. BMC Pregnancy Childbirth 2014, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Omole, O.; Ijadunola, M.Y.; Olotu, E.; Omotoso, O.; Bello, B.; Awoniran, O.; Phillips, A.; Fatusi, A. The effect of mobile phone short message service on maternal health in south—west Nigeria. Int. J. Health Plan. Manag. 2018, 33, 155–170. [Google Scholar] [CrossRef]
- Lund, S.; Rasch, V.; Hemed, M.; Boas, I.M.; Said, A.; Said, K.; Makundu, M.H.; Nielsen, B.B. Mobile phone intervention reduces perinatal mortality in zanzibar: Secondary outcomes of a cluster randomised controlled trial. JMIR mHealth uHealth 2014, 2, e2941. [Google Scholar] [CrossRef]
- Oliveira-Ciabati, L.; Vieira, C.S.; Franzon, A.C.; Alves, D.; Zaratini, F.S.; Braga, G.C.; Sanchez, J.A.; Bonifácio, L.P.; Andrade, M.S.; Fernandes, M.; et al. PRENACEL—A mHealth messaging system to complement antenatal care: A cluster randomized trial. Reprod. Health 2017, 14, 1–2. [Google Scholar] [CrossRef]
- Atnafu, A.; Otto, K.; Herbst, C.H. The role of mHealth intervention on maternal and child health service delivery: Findings from a randomized controlled field trial in rural Ethiopia. Mhealth 2017, 3, 39. [Google Scholar] [CrossRef]
- Bangal, V.B.; Borawake, S.K.; Gavhane, S.P.; Aher, K.H. Use of mobile phone for improvement in maternal health: A randomized control trial. Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 6, 5458–5464. [Google Scholar] [CrossRef]
- World Health Organization. Maternal and Reproductive Health. 2020. Available online: https://www.who.int/gho/maternal_health/mortality/maternal_mortality_text/en/#: (accessed on 15 February 2023).
- Kant, R.; Yadav, P.; Kishore, S.; Barnwal, S.; Kumar, R.; Khapre, M. Impact of mHealth interventions on antenatal and postnatal care utilisation in low and middle-income countries: A Systematic Review and Meta-Analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Fedha, T. Impact of mobile telephone on maternal health service care: A case of Njoro division. Open J. Prev. Med. 2014, 4, 365–376. [Google Scholar] [CrossRef]
- Balakrishnan, R.; Gopichandran, V.; Chaturvedi, S.; Chatterjee, R.; Mahapatra, T.; Chaudhuri, I. Continuum of Care Services for Maternal and Child Health using mobile technology—A health system strengthening strategy in low and middle income countries. BMC Med. Inform. Decis. Mak. 2016, 16, 84. [Google Scholar] [CrossRef] [PubMed]
- USAID. Mobile Technology Strengthens Behavior Change Communication and Referrals by Community Health Workers for Maternal, Newborn, and Child Health in Rural Afghanistan. World Vision. 2014. Available online: http://www.usaid.gov/sites/default/files/documents/1864/WorldVisionORBrief.pdf (accessed on 1 February 2015).
- Kaewkungwal, J.; Apidechkul, T.; Jandee, K.; Khamsiriwatchara, A.; Lawpoolsri, S.; Sawang, S.; Sangvichean, A.; Wansatid, P.; Krongrungroj, S. Application of mobile technology for improving expanded program on immunization among highland minority and stateless populations in northern Thailand border. JMIR mHealth uHealth 2015, 3, e3704. [Google Scholar] [CrossRef]
- Jareethum, R.; Titapant, V.; Tienthai, C.; Viboonchart, S.; Chuenwattana, P.; Chatchainoppakhun, J. Satisfaction of healthy pregnant women receiving short message service via mobile phone for prenatal support: A randomised controlled trial. Med. J. Med. Assoc. Thail. 2008, 91, 458. [Google Scholar]
- Ahmed, T.; Lucas, H.; Khan, A.S.; Islam, R.; Bhuiya, A.; Iqbal, M. eHealth and mHealth initiatives in Bangladesh: A scoping study. BMC Health Serv. Res. 2014, 14, 260. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies; Global Observatory for eHealth Series; World Health Organization: Geneva, Switzerland, 2011; Volume 3, pp. 1–101. [Google Scholar]
- Tamrat, T.; Ratanaprayul, N.; Barreix, M.; Tunçalp, Ö.; Lowrance, D.; Thompson, J.; Rosenblum, L.; Kidula, N.; Chahar, R.; Gaffield, M.E.; et al. Transitioning to Digital Systems: The Role of World Health Organization’s Digital Adaptation Kits in Operationalizing Recommendations and Interoperability Standards. Glob. Health Sci. Pract. 2022, 10, e2100320. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Pallikadavath, S.; Ram, F.; Ogollah, R. Inequalities in advice provided by public health workers to women during antenatal sessions in rural India. PLoS ONE 2012, 7, e44931. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E (accessed on 18 February 2023).
- World Health Organization. Maternal and Newborn Health. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/maternal-newborn-child-and-adolescent-health (accessed on 18 February 2023).




{kind=link}
{kind=link}
{kind=link}
| Study ID | General Information | Study Characteristics | Participant Characteristics | Intervention and Setting | Outcome Data/Results |
|---|---|---|---|---|---|
| Lund, 2014 [23] | Date of data extraction March 2009 to March 2010 Article title Mobile phones improve antenatal care attendance in Zanzibar: a cluster randomised controlled trial Country of origin Zanzibar, United Republic of Tanzania | Aim/objectives of the study To evaluate the association between a mobile phone intervention named “wired mothers” and antenatal care in Zanzibar Study design A pragmatic cluster-randomised controlled trial Study inclusion and exclusion criteria Women who attended antenatal care appointments at selected healthcare facilities. “Wired mothers” was used to describe women linked to the health system by use of a mobile phone intervention throughout their pregnancy and postpartum period Recruitment procedures used (e.g., details of randomization and blinding) Simple random allocation No masking | Characteristics of the participants at the beginning of the study 2550 pregnant women Interventions—131 Controls—1239 | Description of the intervention(s) and control(s) Automated short messaging service (SMS) system | ANC attendance Four or more antenatal care visits Intervention—574/1311 (44%) Control—385/1239 (31%) |
| Omole et al., 2017 [24] | Article title The effect of mobile phone short message service on maternal health in south-west Nigeria Country of origin Nigeria | Aim/objectives of the study
Recruitment procedures used (e.g., details of randomization and blinding) A pregnant woman attending any of the study facilities must reside in the Ife-Ijesa zone, must own a mobile phone, and must be able to read and write in English or the Yoruba (local dialect) language | Characteristics of the participants at the beginning of the study 508 clients participated in the study, consisting of 248 in the control group and 260 in the intervention group | Setting in which the intervention is delivered 6 government-owned secondary health facilities 89 primary healthcare facilities managed by local government authorities 103 non-government facilities, including mission-owned health facilities | Neonatal death Control—67/248, 40.4% Intervention—65/260, 36.5% ANC attendance Improved ANC attendance—(99.4%) |
| Lund et al., 2014 [25] | Article title Mobile Phone Intervention Reduces Perinatal Mortality in Zanzibar: Secondary Outcomes of a Cluster Randomized Controlled Trial Country of Origin Zanzibar | Aim/objectives of the study To evaluate the association between a mobile phone intervention and perinatal mortality in a resource-limited setting. Study design Cluster randomised controlled trial Study inclusion and exclusion criteria Recruitment procedures used (e.g., details of randomization and blinding) Cluster sampling Unit of allocation (e.g., participant, GP practice, etc.) Primary healthcare facilities in Zanzibar | Characteristics of the participants at the beginning of the study 2550 pregnant women Interventions—1311 Controls—1239 Total number— 2550 | Description of the intervention(s) and control(s) “Mobile Solutions Aiding Knowledge for Health Improvement” (M-SAKHI) | Major adverse maternal outcome Severe complications- Intervention—182/1311 (13.9%) Control—199/1239 (16.1%) ANC attendance Antenatal care (four or more visits) Intervention—574/1311 (43.8%) Control—385/1239 (31.1%) Stillbirth Intervention—22/54 Control—32/54 Perinatal mortality Intervention—25/69 Control—44/69 |
| Oliveira-Ciabati et al., 2017 [26] | Date of data extraction April 2015 and March 2016 Article title PRENACEL—a mHealth messaging system to complement antenatal care: a cluster randomised trial Country of Origin Brazil | Aim/objectives of the study To determine whether the use of a bi-directional short message service (PRENACEL) providing information on pregnancy, childbirth, antenatal and intrapartum care, and able to answer the specific queries of pregnant women increases the coverage of recommended antenatal practices. Study design Cluster randomised trial | Characteristics of the participants at the beginning of the study 1210 pregnant women Interventions—770 Controls—440 | Setting in which the intervention is delivered Primary health care units (PHCUs) Description of the intervention(s) and control(s) The PRENACEL SMS package was adapted from the Mobile Alliance for Maternal Action (MAMA) | ANC practices (≥6 antenatal visits) Intervention— Total—686/770 (89.1%) PRENACEL—112/116 (96.6%) Control—373/440 (84.8%) |
| Atnafu et al., 2017 [27] | Date of data extraction September 2012-October 2013 Article title The role of mHealth intervention on maternal and child health service delivery: findings from a randomised controlled field trial in rural Ethiopia Country of Origin Ethiopia | Aim/objectives of the study To assess the role of a mobile phone equipped with short message service (SMS)-based data-exchange software linking community health workers to health centers in rural Ethiopia and whether it affects selected MCH outcomes Study design Randomised control trial | Characteristics of the participants at the beginning of the study At baseline— Ezha (treatment 1)—1065 (98.6%) Abeshge (treatment 2)—1073 (99.35%) Sodo (control)—1080(100%) After intervention— Ezha (treatment 1)— 1066 (98.7%) Abeshge (treatment 2)—946 (87.6%) Sodo (control)— 1077 99.72%) | Setting in which the intervention is delivered Description of the intervention(s) and control(s) The FrontlineSMS-based application was offered only to the treatment groups, not the control groups. | Number of ANC visits (≥4)— At baseline— Ezha (treatment 1)—482/1065 (45.32%) Abeshge (treatment 2)—169/1073, (15.80%) Sodo (control)—264/1080, (24.48%) After intervention- Ezha (treatment 1)—637/1066, (59.84%) Abeshge (treatment 2)—297/946, (31.50%) Sodo (control)—250/1077 (23.27%) |
| Bangal VB et al., 2017 [28] | Date of data extraction September 2012-October 2013 Article title Use of mobile phone for improvement in maternal health: a randomised control trial Country of Origin India | Aim/objectives of the study To improve maternal health and pregnancy outcome through optimum utilisation of antenatal, natal, and postnatal care services, with the use of a mobile phone as a medium of communication between health care providers and communities in rural areas Study design Randomised control trial | Characteristics of the participants at the beginning of the study Total—400 Intervention—200 Control—200 | Setting in which the intervention is delivered Rural Medical College, Loni, Ahmednagar Description of the intervention(s) and control(s) Mobile phone calls and text messages (SMS)— important aspects of antenatal care at regular intervals. | Number of ANC visits 5–6 ANC visits Control—33/200 (16.50%) Intervention—67/200 (33.50%) >6 ANC visits Control—14/200 (07.00%) Intervention—48/200 (24.00%) |
| (a) | ||
| Bangal VB et al., 2017 [28] | ||
| Methods | Randomised control trial | |
| Participants | 400 | |
| Interventions | Mobile phone calls, Text messages (SMS) | |
| Outcomes | ANC Attendance | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors’ judgment | Support for judgment |
| Random sequence generation (selection bias) | Low risk | Randomly allocated to control and intervention group |
| Allocation concealment (selection bias) | Unclear risk | |
| Blinding of participants and personnel (performance bias) | Unclear risk | |
| Blinding of outcome assessment (detection bias) | Unclear risk | |
| Incomplete outcome data (attrition bias) | Low risk | |
| Selective reporting (reporting bias) | Unclear risk | |
| Other bias | Unclear risk | |
| (b) | ||
| Lund 2014 [23] | ||
| Methods | Pragmatic cluster-randomised controlled trial | |
| Participants | 2550 | |
| Interventions | Automated short messaging service (SMS) system | |
| Outcomes | ANC Attendance | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors’ judgment | Support for judgment |
| Random sequence generation (selection bias) | Low risk | Simple random allocation |
| Allocation concealment (selection bias) | Low risk | |
| Blinding of participants and personnel (performance bias) | High risk | Neither study participants nor clinic staff were masked |
| Blinding of outcome assessment (detection bias) | Low risk | |
| Incomplete outcome data (attrition bias) | Low risk | |
| Selective reporting (reporting bias) | Low risk | |
| Other bias | Low risk | |
| (c) | ||
| Lund et al., 2014 [25] | ||
| Methods | Cluster randomised controlled trial | |
| Participants | 2550 | |
| Interventions | Mobile Solutions Aiding Knowledge for Health Improvement (M-SAKHI) | |
| Outcomes | ANC Attendance, still birth, maternal complication, perinatal mortality | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors’ judgment | Support for judgment |
| Random sequence generation (selection bias) | Low risk | Simple random allocation |
| Allocation concealment (selection bias) | Low risk | |
| Blinding of participants and personnel (performance bias) | High risk | Cluster and study participant were not masked |
| Blinding of outcome assessment (detection bias) | Low risk | |
| Incomplete outcome data (attrition bias) | Low risk | |
| Selective reporting (reporting bias) | Low risk | |
| Other bias | Low risk | |
| (d) | ||
| Oliveria-Ciabati et al., 2017 [26] | ||
| Methods | Cluster randomised trial | |
| Participants | 1210 | |
| Interventions | PRENACEL SMS package | |
| Outcomes | ANC Attendance | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors’ judgment | Support for judgment |
| Random sequence generation (selection bias) | Low risk | Cluster randomisation |
| Allocation concealment (selection bias) | Low risk | |
| Blinding of participants and personnel (performance bias) | High risk | Participants and health professionals were not masked to the intervention |
| Blinding of outcome assessment (detection bias) | Low risk | |
| Incomplete outcome data (attrition bias) | Low risk | |
| Selective reporting (reporting bias) | Low risk | |
| Other bias | Low risk | |
| (e) | ||
| OMOLE et al., 2017 [24] | ||
| Methods | Experimental | |
| Participants | 508 | |
| Interventions | Short message service | |
| Outcomes | Neonatal death | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors’ judgment | Support for judgment |
| Random sequence generation (selection bias) | Low risk | |
| Allocation concealment (selection bias) | Low risk | |
| Blinding of participants and personnel (performance bias) | High risk | The research assistants and study subjects were not blinded |
| Blinding of outcome assessment (detection bias) | Low risk | |
| Incomplete outcome data (attrition bias) | Low risk | |
| Selective reporting (reporting bias) | Low risk | |
| Other bias | Low risk | |
| (f) | ||
| Atnafu et al., 2017 [27] | ||
| Methods | Randomized control trial | |
| Participants | 3218 | |
| Interventions | Frontline SMS-based application | |
| Outcomes | ANC Attendance | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors’ judgment | Support for judgment |
| Random sequence generation (selection bias) | Low risk | Randomly assigned by lottery method |
| Allocation concealment (selection bias) | Low risk | Random allocation |
| Blinding of participants and personnel (performance bias) | Unclear risk | |
| Blinding of outcome assessment (detection bias) | Unclear risk | |
| Incomplete outcome data (attrition bias) | Low risk | Data is recorded for all participants |
| Selective reporting (reporting bias) | Low risk | Prespecified outcome was reported |
| Other bias | Low risk | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mishra, M.; Parida, D.; Murmu, J.; Singh, D.; Rehman, T.; Kshatri, J.S.; Pati, S. Effectiveness of mHealth Interventions for Monitoring Antenatal Care among Pregnant Women in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 2635. https://doi.org/10.3390/healthcare11192635
Mishra M, Parida D, Murmu J, Singh D, Rehman T, Kshatri JS, Pati S. Effectiveness of mHealth Interventions for Monitoring Antenatal Care among Pregnant Women in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(19):2635. https://doi.org/10.3390/healthcare11192635
Chicago/Turabian StyleMishra, Manisha, Debasini Parida, Jogesh Murmu, Damini Singh, Tanveer Rehman, Jaya Singh Kshatri, and Sanghamitra Pati. 2023. "Effectiveness of mHealth Interventions for Monitoring Antenatal Care among Pregnant Women in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis" Healthcare 11, no. 19: 2635. https://doi.org/10.3390/healthcare11192635
APA StyleMishra, M., Parida, D., Murmu, J., Singh, D., Rehman, T., Kshatri, J. S., & Pati, S. (2023). Effectiveness of mHealth Interventions for Monitoring Antenatal Care among Pregnant Women in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Healthcare, 11(19), 2635. https://doi.org/10.3390/healthcare11192635