
Efficacy and Safety of Respiratory Telerehabilitation in Patients with Long COVID-19: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Meta-Analysis
3. Results
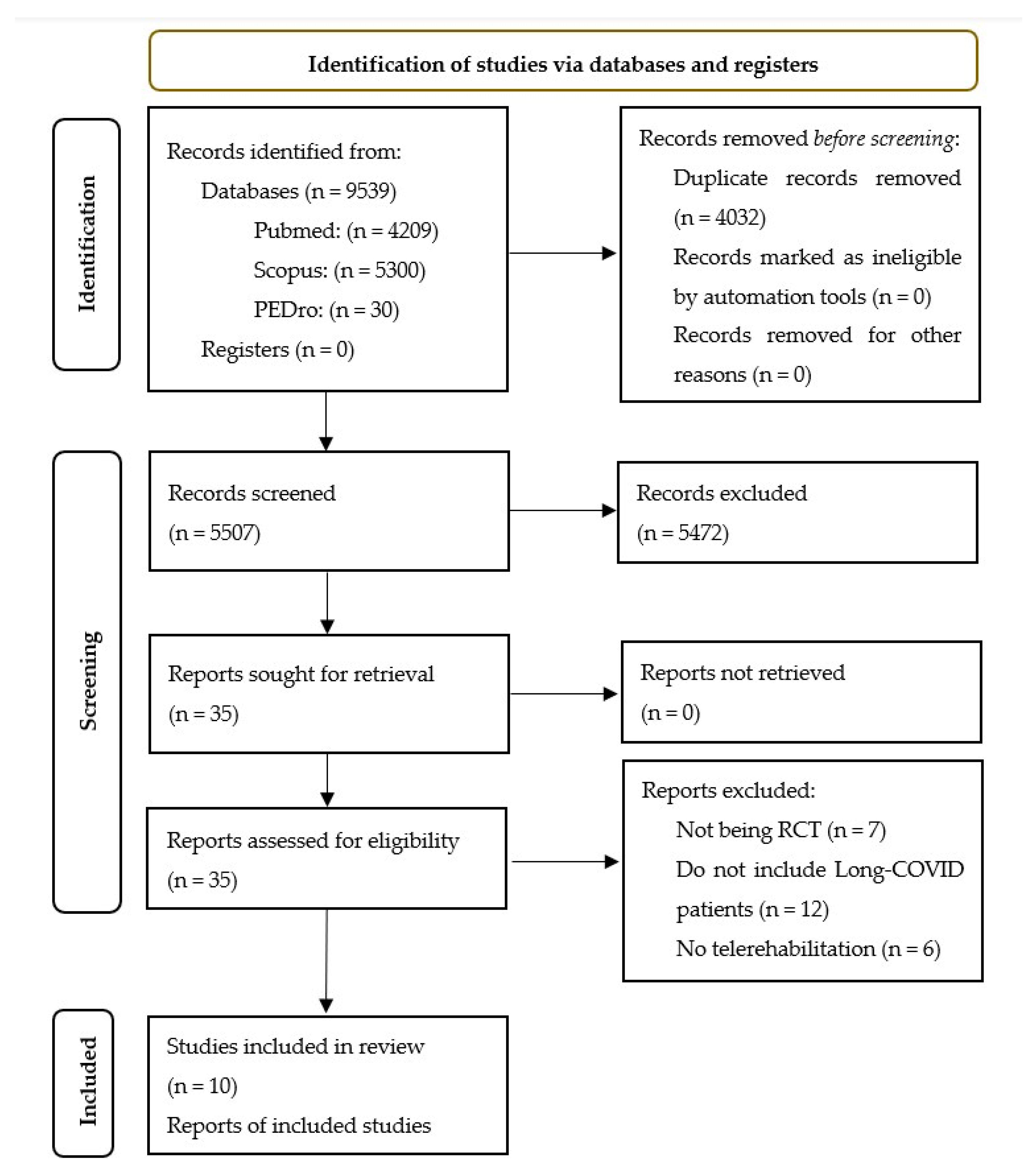
3.1. Study Selection
3.2. Study Characteristics
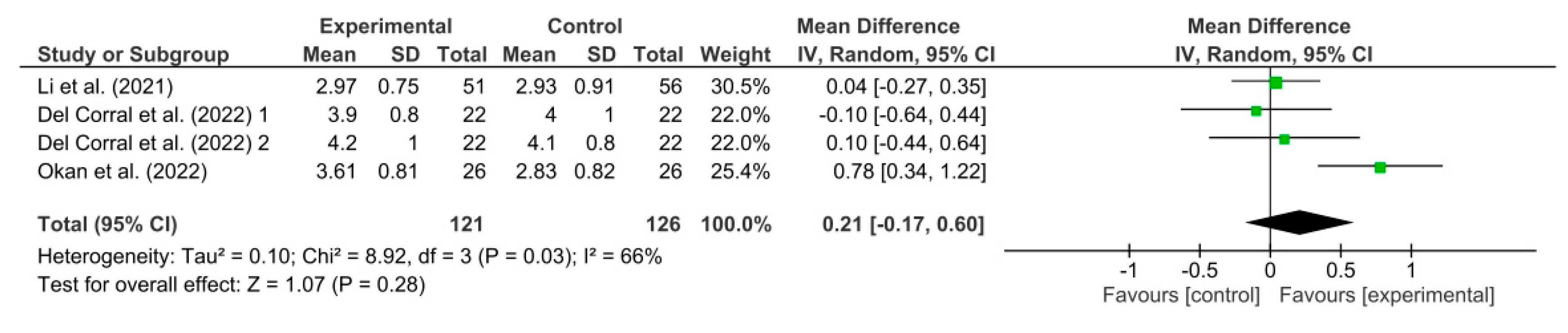
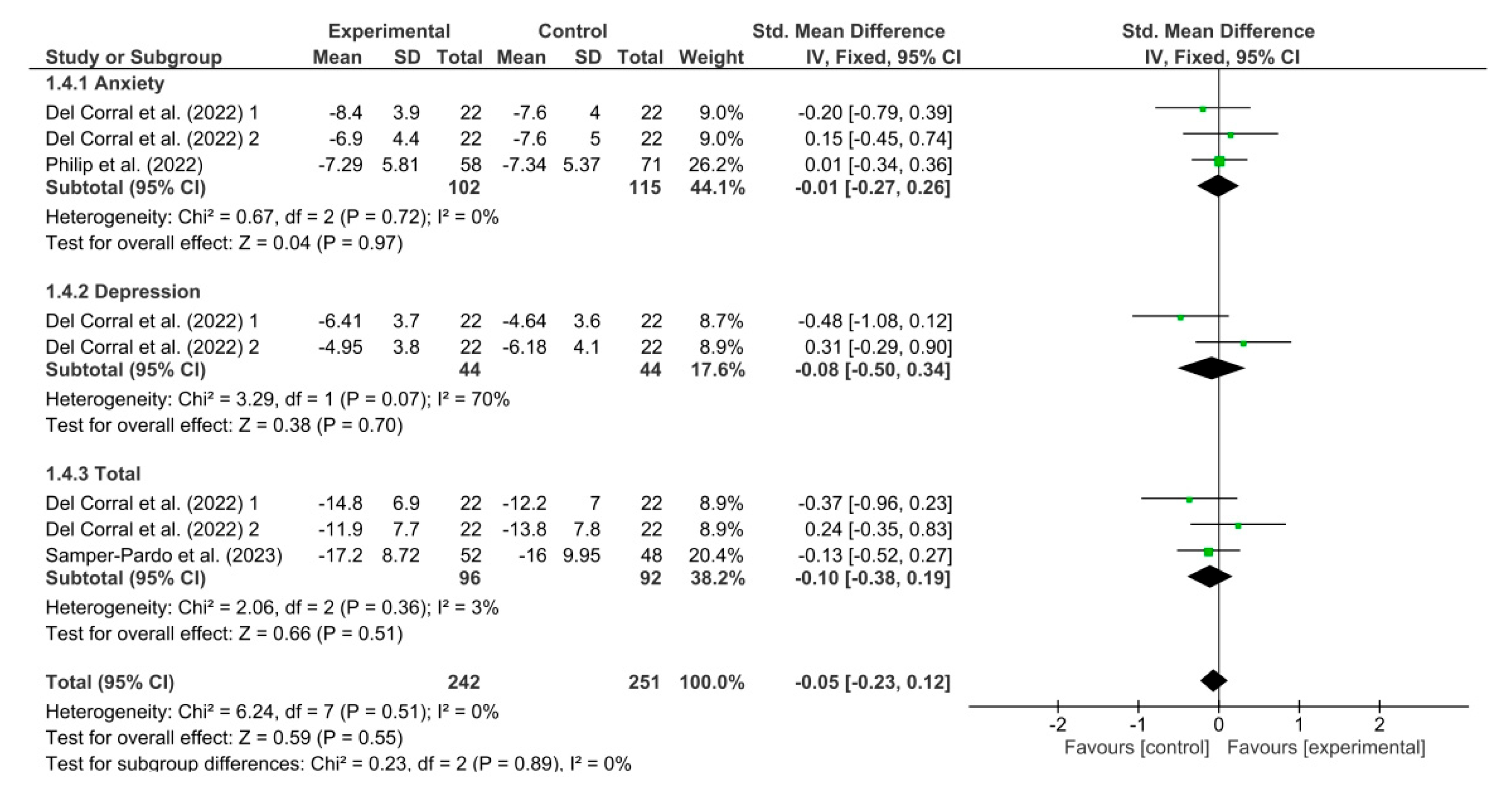
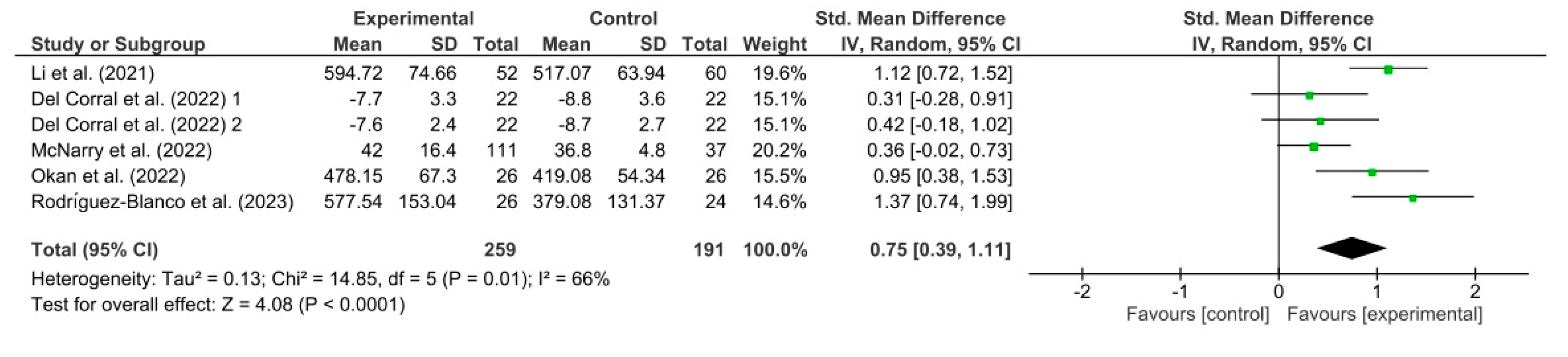
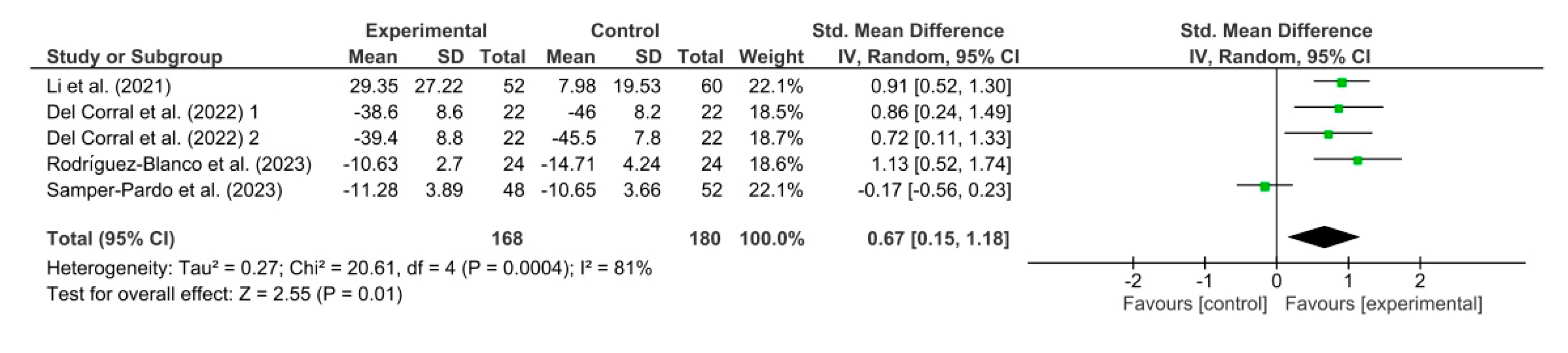
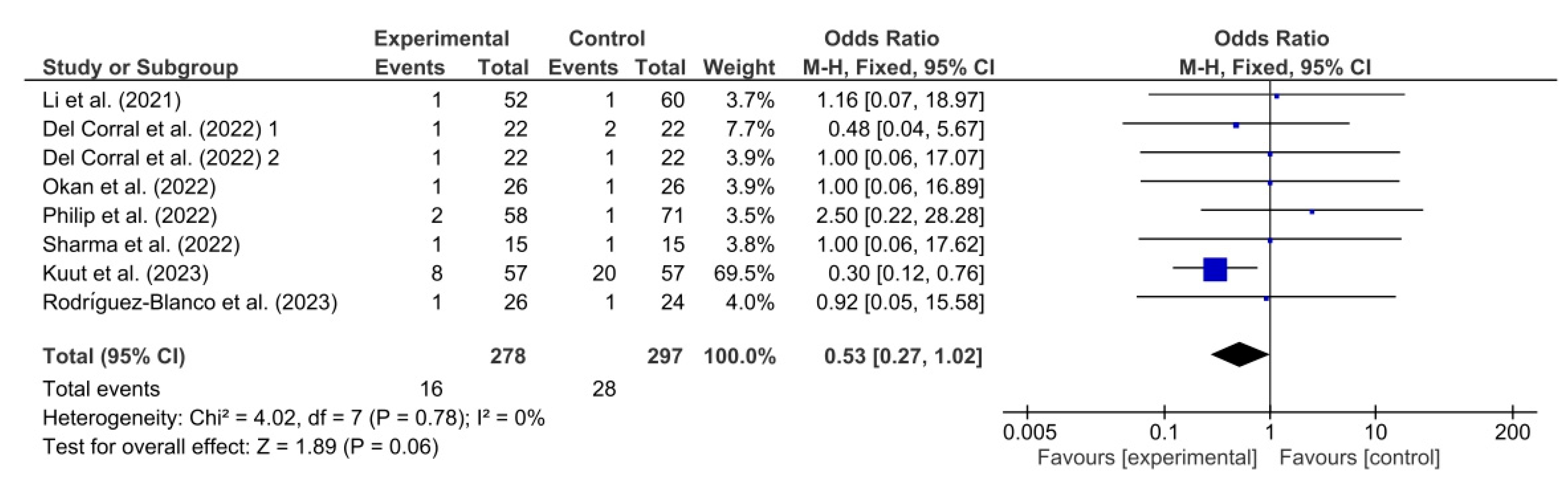
3.3. Results Obtained in Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
References
- World Health Organization. Guideline Clinical Management of COVID-19: Living Guideline. 2023. Available online: http://apps.who.int/bookorders (accessed on 7 September 2023).
- World Health Organization. Clinical Case Definition Working Group on Post COVID-19 Condition. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. 6 October 2021. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-post-covid-19-condition?gclid=Cj0KCQjw9fqnBhDSARIsAHlcQYQ2QjkKZgDSasiJIat7gXkyHeZZY5LyfMzEOkW6x_2_M3jztBEnXBgaAjA2EALw_wcB (accessed on 7 September 2023).
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef] [PubMed]
- O’Mahoney, L.L.; Routen, A.; Gillies, C.; Ekezie, W.; Welford, A.; Zhang, A.; Karamchandani, U.; Simms-Williams, N.; Cassambai, S.; Ardavani, A.; et al. The prevalence and long-term health effects of Long COVID among hospitalised and non-hospitalised populations: A systematic review and meta-analysis. EClinicalMedicine 2022, 55, 101762. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Billig Rose, E.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. IVY Network Investigators; CDC COVID-19 Response Team; IVY Network Investigators. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United States, March–June 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 993–998. [Google Scholar]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Menges, D.; Ballouz, T.; Anagnostopoulos, A.; Aschmann, H.E.; Domenghino, A.; Fehr, J.S.; Puhan, M.A. Burden of post-COVID-19 syndrome and implications for healthcare service planning: A population-based cohort study. PLoS ONE 2021, 16, e0254523. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, P. NICE guideline on long COVID. Lancet Respir. Med. 2021, 9, 129. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- FAIR Health. A Detailed Study of Patients with Long-Haul COVID; FAIR Health: New York, NY, USA, 2021. [Google Scholar]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 Long-term effects of COVID-19: A systematic review and meta-analysis. medRxiv 2021. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Knowledge for Better Health: Strengthening Health Systems; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Christensen, C. The Innovator’s Dilemma: When New Technologies Cause Great Firms to Fail; Harvard Business Review Press: Boston, MA, USA, 2013. [Google Scholar]
- Laver, K.E.; Adey-Wakeling, Z.; Crotty, M.; Lannin, N.A.; George, S.; Sherrington, C. Telerehabilitation services for stroke. Cochrane Database Syst. Rev. 2020, 1, CD010255. [Google Scholar] [CrossRef]
- Seron, P.; Oliveros, M.J.; Gutierrez-Arias, R.; Fuentes-Aspe, R.; Torres-Castro, R.C.; Merino-Osorio, C.; Nahuelhual, P.; Inostroza, J.; Jalil, Y.; Solano, R.; et al. Effectiveness of Telerehabilitation in Physical Therapy: A Rapid Overview. Phys. Ther. 2021, 101, pzab053. [Google Scholar] [CrossRef]
- Groenveld, T.; Achttien, R.; Smits, M.; de Vries, M.; van Heerde, R.; Staal, B.; van Goor, H. COVID Rehab Group. Feasibility of Virtual Reality Exercises at Home for Post-COVID-19 Condition: Cohort Study. JMIR Rehabil. Assist. Technol. 2022, 9, e36836. [Google Scholar] [CrossRef] [PubMed]
- Kolbe, L.; Jaywant, A.; Gupta, A.; Vanderlind, W.M.; Jabbour, G. Use of virtual reality in the inpatient rehabilitation of COVID-19 patients. Gen. Hosp. Psychiatry 2021, 71, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Cotelli, M.; Manenti, R.; Brambilla, M.; Gobbi, E.; Ferrari, C.; Binetti, G.; Cappa, S.F. Cognitive telerehabilitation in mild cog-nitive impairment, Alzheimer’s disease and frontotemporal dementia: A systematic review. J. Telemed. Telecare 2019, 25, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Amatya, B.; Galea, M.P.; Kesselring, J.; Khan, F. Effectiveness of telerehabilitation interventions in persons with multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2015, 4, 358–369. [Google Scholar] [CrossRef]
- Cramer, S.C.; Dodakian, L.; Le, V.; See, J.; Augsburger, R.; McKenzie, A.; Zhou, R.J.; Chiu, N.L.; Heckhausen, J.; Cassidy, J.M. National Institutes of Health StrokeNet Telerehab Investigators. Efficacy of Home-Based Telerehabilitation vs. In-Clinic Therapy for Adults After Stroke: A Randomized Clinical Trial. JAMA Neurol. 2019, 76, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Cheville, A.L.; Moynihan, T.; Herrin, J.; Loprinzi, C.; Kroenke, K. Effect of Collaborative Telerehabilitation on Functional Impairment and Pain Among Patients with Advanced-Stage Cancer: A Randomized Clinical Trial. JAMA Oncol. 2019, 5, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Yamabayashi, C.; Syed, N.; Kirkham, A.; Camp, P.G. Exercise Telemonitoring and Telerehabilitation Compared with Traditional Cardiac and Pulmonary Rehabilitation: A Systematic Review and Meta-Analysis. Physiother. Can. 2016, 68, 242–251. [Google Scholar] [CrossRef] [PubMed]
- British Society of Rehabilitation Medicine. Rehabilitation in the Wake of COVID-19—A Phoenix from the Ashes. 2020. Available online: www.bsrm.org.uk/downloads/covid-19bsrmissue1-published-27-4-2020.pdf (accessed on 5 September 2023).
- Chartered Society of Physiotherapy. Rehabilitation and COVID-19—CSP Policy Statement. 2020. Available online: www.csp.org.uk/professional-clinical/improvement-innovation/community-rehabilitation/rehab-covid-19-policy-statement (accessed on 5 September 2023).
- British Thoracic Society. Delivering Rehabilitation to Patients Surviving COVID-19 Using an Adapted Pulmonary Rehabilitation Approach—BTS Guidance. 2020. Available online: www.brit-thoracic.org.uk/covid-19/covid-19-information-for-the-respiratory-community/ (accessed on 5 September 2023).
- Wade, D.T. What is rehabilitation? An empirical investigation leading to an evidence-based description. Clin. Rehabil. 2020, 34, 571–583. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 (Updated March 2011); The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Demiris, G.; Shigaki, C.L.; Schopp, L.H. An evaluation framework for a rural home-based telerehabilitation network. J. Med. Syst. 2005, 29, 595–603. [Google Scholar] [CrossRef]
- Ricker, J.H.; Rosenthal, M.; Garay, E.; DeLuca, J.; Germain, A.; Abraham-Fuchs, K.; Schmidt, K.U. Telerehabilitation needs: A survey of persons with acquired brain injury. J. Head. Trauma. Rehabil. 2002, 17, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; European Carotid Surgery Trial Collaborative Group. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, iii–x, 1–173. [Google Scholar] [CrossRef] [PubMed]
- Saunders, L.D.; Soomro, G.M.; Buckingham, J.; Jamtvedt, G.; Raina, P. Assessing the methodological quality of non-randomized intervention studies. West. J. Nurs. Res. 2003, 25, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2019. [Google Scholar]
- Kuss, O. Statistical methods for meta-analyses including information from studies without any events—Add nothing to nothing and succeed nevertheless. Stat. Med. 2015, 34, 1097–1116. [Google Scholar] [CrossRef]
- Li, J.; Xia, W.; Zhan, C.; Liu, S.; Yin, Z.; Wang, J.; Chong, Y.; Zheng, C.; Fang, X.; Cheng, W.; et al. A telerehabilitation programme in post-discharge COVID-19 patients (TERECO): A randomised controlled trial. Thorax 2022, 77, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Del Corral, T.; Fabero-Garrido, R.; Plaza-Manzano, G.; Fernández-de-Las-Peñas, C.; Navarro-Santana, M.; López-de-Uralde-Villanueva, I. Home-based respiratory muscle training on quality of life and exercise tolerance in long-term post-COVID-19: Randomized controlled trial. Ann. Phys. Rehabil. Med. 2023, 66, 101709. [Google Scholar] [CrossRef]
- McNarry, M.A.; Berg, R.M.G.; Shelley, J.; Hudson, J.; Saynor, Z.L.; Duckers, J.; Lewis, K.; Davies, G.A.; Mackintosh, K.A. Inspiratory muscle training enhances recovery post-COVID-19: A randomised controlled trial. Eur. Respir. J. 2022, 60, 2103101. [Google Scholar] [CrossRef]
- Okan, F.; Okan, S.; Duran Yücesoy, F. Evaluating the Efficiency of Breathing Exercises via Telemedicine in Post-COVID-19 Patients: Randomized Controlled Study. Clin. Nurs. Res. 2022, 31, 771–781. [Google Scholar] [CrossRef]
- Philip, K.E.J.; Owles, H.; McVey, S.; Pagnuco, T.; Bruce, K.; Brunjes, H.; Banya, W.; Mollica, J.; Lound, A.; Zumpe, S.; et al. An online breathing and wellbeing pro-gramme (ENO Breathe) for people with persistent symptoms following COVID-19: A parallel-group, single-blind, randomised controlled trial. Lancet Respir. Med. 2022, 10, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Goswami, S.K. Pulmonary Tele-Rehabilitation in Patients (Post COVID-19) With Respiratory Complications: A Randomized Controlled Trial. Indian. J. Physiother. Occup. 2022, 16, 182–189. [Google Scholar]
- Vallier, J.M.; Simon, C.; Bronstein, A.; Dumont, M.; Jobic, A.; Paleiron, N.; Laurent, M.E.L.Y. Randomized controlled trial of home-based vs. hospital-based pulmonary rehabilitation in post COVID-19 patients. Eur. J. Phys. Rehabil. Med. 2023, 59, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Kuut, T.A.; Müller, F.; Csorba, I.; Braamse, A.; Aldenkamp, A.; Appelman, B.; Assmann-Schuilwerve, E.; Geerlings, S.E.; Gibney, K.B.; Kanaan, R.A.; et al. Efficacy of cognitive behavioral therapy targeting severe fatigue following COVID-19: Results of a randomized controlled trial. Clin. Infect. Dis. 2023, ciad257. [Google Scholar] [CrossRef]
- Rodriguez-Blanco, C.; Bernal-Utrera, C.; Anarte-Lazo, E.; Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M. A 14-Day Therapeutic Exercise Telerehabilitation Protocol of Physiotherapy Is Effective in Non-Hospitalized Post-COVID-19 Conditions: A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 776. [Google Scholar] [CrossRef] [PubMed]
- Samper-Pardo, M.; León-Herrera, S.; Oliván-Blázquez, B.; Méndez-López, F.; Domínguez-García, M.; Sánchez-Recio, R. Effectiveness of a telerehabilitation intervention using ReCOVery APP of long COVID patients: A randomized, 3-month follow-up clinical trial. Sci. Rep. 2023, 13, 7943. [Google Scholar] [CrossRef]
- Notarte, K.I.; de Oliveira, M.H.S.; Peligro, P.J.; Velasco, J.V.; Macaranas, I.; Ver, A.T.; Pangilinan, F.C.; Pastrana, A.; Goldrich, N.; Kavteladze, D.; et al. Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7314. [Google Scholar] [CrossRef]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Martín-Guerrero, J.D.; Pellicer-Valero, Ó.J.; Navarro-Pardo, E.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Cigarán-Méndez, M.; Hernández-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef]
- Ashra, F.; Jen, H.J.; Liu, D.; Lee, T.Y.; Pien, L.C.; Chen, R.; Lin, H.C.; Chou, K.R. Effectiveness of respiratory rehabilitation in patients with COVID-19: A meta-analysis. J. Clin. Nurs. 2023, 32, 4972–4987. [Google Scholar] [CrossRef]
- Triberti, S.; Savioni, L.; Sebri, V.; Pravettoni, G. eHealth for improving quality of life in breast cancer patients: A systematic review. Cancer Treat. Rev. 2019, 74, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Fridriksdottir, N.; Gunnarsdottir, S.; Zoëga, S.; Ingadottir, B.; Hafsteinsdottir, E.J.G. Effects of web-based interventions on cancer patients’ symptoms: Review of randomized trials. Support. Care Cancer 2018, 26, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Reychler, G.; Piraux, E.; Beaumont, M.; Caty, G.; Liistro, G. Telerehabilitation as a Form of Pulmonary Rehabilitation in Chronic Lung Disease: A Systematic Review. Healthcare 2022, 10, 1795. [Google Scholar] [CrossRef] [PubMed]
- Ora, J.; Prendi, E.; Attinà, M.L.; Cazzola, M.; Calzetta, L.; Rogliani, P. Efficacy of respiratory tele-rehabilitation in COPD patients: Systematic review and meta-analysis. Monaldi Arch. Chest Dis. 2022, 92. [Google Scholar] [CrossRef] [PubMed]
- Hoaas, H.; Andreassen, H.K.; Lien, L.A.; Hjalmarsen, A.; Zanaboni, P. Adherence and factors affecting satisfaction in long-term telerehabilitation for patients with chronic obstructive pulmonary disease: A mixed methods study. BMC Med. Inform. Decis. Mak. 2016, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.K.; Stellefson, M.; Bernhardt, J.M. Healthy Aging 2.0: The potential of new media and technology. Prev. Chronic Dis. 2012, 9, E67. [Google Scholar] [CrossRef][Green Version]
- Donner, C.F.; Raskin, J.; ZuWallack, R.; Nici, L.; Ambrosino, N.; Balbi, B.; Blackstock, F.; Casaburi, R.; Dreher, M.; Effing, T.; et al. Incorporating telemedicine into the integrated care of the COPD patient a summary of an interdisciplinary workshop held in Stresa, Italy, 7–8 September 2017. Respir. Med. 2018, 143, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Stellefson, M.; Chaney, B.; Barry, A.E.; Chavarria, E.; Tennant, B.; Walsh-Childers, K.; Sriram, P.S.; Zagora, J. Web 2.0 chronic disease self-management for older adults: A systematic review. J. Med. Internet Res. 2013, 15, e35. [Google Scholar] [CrossRef]
- Proffitt, R.; Lange, B. Feasibility of a Customized, In-Home, Game-Based Stroke Exercise Program Using the Microsoft Kinect® Sensor. Int. J. Telerehabil. 2015, 7, 23–34. [Google Scholar] [CrossRef]
- Gil-Pagés, M.; Solana, J.; Sánchez-Carrión, R.; Tormos, J.M.; Enseñat-Cantallops, A.; García-Molina, A. A customized home-based computerized cognitive rehabilitation platform for patients with chronic-stage stroke: Study protocol for a randomized controlled trial. Trials 2018, 19, 191. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens de Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; Van den Heede, K. Pathophysiology and mechanism of long COVID: A comprehensive review. Ann. Med. 2022, 54, 1473–1487. [Google Scholar] [CrossRef] [PubMed]
- Yuehong, Y.I.N.; Zeng, Y.; Chen, X.; Fan, Y. The internet of things in healthcare: An overview. J. Ind. Inf. Integr. 2016, 1, 3–13. [Google Scholar]
- Snoswell, C.L.; Taylor, M.L.; Comans, T.A.; Smith, A.C.; Gray, L.C.; Caffery, L.J. Determining if Telehealth Can Reduce Health System Costs: Scoping Review. J. Med. Internet Res. 2020, 22, e17298. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Sample Size (n (% Female)) and Age (Mean) | Time since Acute Infection (Days) | Hospital Admission (%) | Length of Hospital Stay (Days) | Severity of Acute Infection | Quality Assessment Downs and Black (Risk of Bias) |
|---|---|---|---|---|---|---|
| Li et al. (2021) [37] | 119 (66), 51 | 103.7 | 100 | 26.2 | Severe and critical | 25 (low risk) |
| Del Corral et al. (2022) [38] | 88 (71), 46 | 350.8 | 31.8 | NR | Mild, moderate, severe, and critical | 27 (low risk) |
| McNarry et al. (2022) [39] | 148 (90), 47 | 270 | NR | NR | Mild, moderate, severe, and critical | 23 (low risk) |
| Okan et al. (2022) [40] | 52 (48), 51 | 86.9 | 100 | 9.5 | Severe and critical | 25 (low risk) |
| Philip et al. (2022) [41] | 150 (80), 50 | 320 | 17.3 | NR | Mild, moderate, and severe | 24 (low risk) |
| Sharma et al. (2022) [42] | 30 (NR), NR | NR | NR | NR | Mild | 14 (high risk) |
| Vallier et al. (2022) [43] | 17 (29), 55 | 140.9 | 76.5 | 11.3 | Mild, moderate, severe, and critical | 19 (high risk) |
| Kuut et al. (2023) [44] | 114 (72.8), 46 | 187.5 | 11.4 | NR | Mild, moderate, severe, and critical | 22 (some concerns) |
| Rodríguez-Blanco et al. (2023) [45] | 48 (54), 41 | NR | 0 | Not applicable | Mild | 21 (low risk) |
| Samper-Pardo et al. (2023) [46] | 100 (80), 48 | 483.6 | NR | NR | Mild, moderate, severe, and critical | 22 (low risk) |
| Study (Year) | Intervention and Comparator Group | Telerehabilitation Components | Duration, Frequency, Volume, and Intensity | Intervention Technology and Intervention Monitoring | Outcome Measures |
|---|---|---|---|---|---|
| Li et al. (2021) [37] | IG: Breathing exercises + Aerobic exercise + Strength exercises CG: Educational instructions |
|
|
| Quality of life (SF-12): IG ** > CG (p < 0.05) Dyspnea (mMRC): IG ** > CG (p < 0.001) Lung function (FVC): IG * vs. CG * (NSD) Functional capacity (6MWT): IG ** > CG (p < 0.001) Adverse events: IG (0) vs. CG (0) |
| Del Corral et al. (2022) [38] | IG1: Respiratory training (inspiratory musculature) IG2: Respiratory training (inspiratory/expiratory musculature) CG1: Sham respiratory training CG2: Sham respiratory training |
|
|
| Quality of life (EQ-5D): IG1 * vs. CG1 * (NSD) IG2 * > CG2 (p < 0.001) Lung function (FVC): IG1 vs. CG1 (NSD) IG2 vs. CG2 (NSD) Anxiety and depression (HADS): IG1 * vs. CG1 * (NSD) IG2 * vs. CG2 (NSD) MIP: IG1 * > CG1 * (p < 0.05) IG2 * > CG2 * (p < 0.05) Functional capacity (RT): IG1 vs. CG1 (NSD) IG2 * vs. CG2 (NSD) Lower limb strength (1STS): IG1 * > CG1 (p < 0.05) IG2 * > CG2 (p < 0.05) Adverse events: IG1 (0) vs. CG1 (1) IG2 (0) vs. CG2 (0) |
| McNarry et al. (2022) [39] | IG: Respiratory training CG: Usual care |
|
|
| Quality of life (K-BILD): IG ** vs. CG (NSD) Dyspnea (TDI): IG > CG (p < 0.05) Adverse events: NR |
| Okan et al. (2022) [40] | IG: Breathing exercises CG: Education brochure |
|
|
| Quality of life (SGRQ): IG ** > CG ** (p < 0.001) Dyspnea (mMRC): IG ** > CG * (p < 0.001) Lung function (FVC): IG ** vs. CG (p < 0.001) Functional capacity (6MWT): IG ** > CG (p < 0.001) Adverse events: IG (0) vs. CG (0) |
| Philip et al. (2022) [41] | IG: Breathing control and anxiety self-management exercises CG: Usual care |
|
|
| Quality of life (SF-36): IG > CG (p < 0.05) Dyspnea (MD-12): IG vs. CG (NSD) Anxiety and depression (GAD-7): IG vs. CG (NSD) Adverse events: IG (1) vs. CG (0) |
| Sharma et al. (2022) [42] | IG: Breathing exercises + Aerobic exercise + Strength exercises CG: Usual care |
|
|
| Dyspnea (mMRC): IG * > CG (p < 0.05) Fatigue (VAS): IG * > CG (p < 0.05) Adverse events: IG (0) vs. CG (0) |
| Vallier et al. (2022) [43] | IG: Aerobic exercise + Strength exercises + Relaxation exercises CG: Face-to-face physiotherapy |
|
|
| Quality of life (VQ11): IG * vs. CG * (NSD) Dyspnea (mMRC): IG * vs. CG * (NSD) Lung Function (FVC): IG * vs. CG * (NSD) Fatigue (MFI): IG ** > CG ** (p < 0.05) Functional capacity (6MWT): IG ** vs. CG ** (NSD) Lower limb strength (1STS): IG ** vs. CG ** (NSD) Adverse events: NR |
| Kuut et al. (2023) [44] | IG: Multidisciplinary telerehabilitation based on cognitive behavioral therapy CG: Usual care |
|
|
| Quality of life (SF-36): IG > CG (p < 0.001) Fatigue (CIS-F): IG > CG (p < 0.001) Adverse events: IG (8) vs. CG (20) |
| Rodríguez-Blanco et al. (2023) [45] | IG: Breathing exercises + Strength exercises CG: No intervention |
|
|
| Dyspnea (MD-12): IG ** > CG (p < 0.001) Fatigue (VAS): IG ** > CG (p < 0.001) Functional capacity (6MWT): IG ** > CG (p < 0.001) Lower limb strength (30STS): IG ** > CG (p < 0.001) Adverse events: IG (0) vs. CG (0) |
| Samper-Pardo et al. (2023) [46] | IG: Breathing exercises + Aerobic exercise CG: Usual care |
|
|
| Quality of life (SF-36): IG vs. CG (NSD) Anxiety and depression (HADS): IG vs. CG (NSD) Lower limb strength (30STS): IG vs. CG (NSD) Adverse events: NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvache-Mateo, A.; Heredia-Ciuró, A.; Martín-Núñez, J.; Hernández-Hernández, S.; Reychler, G.; López-López, L.; Valenza, M.C. Efficacy and Safety of Respiratory Telerehabilitation in Patients with Long COVID-19: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 2519. https://doi.org/10.3390/healthcare11182519
Calvache-Mateo A, Heredia-Ciuró A, Martín-Núñez J, Hernández-Hernández S, Reychler G, López-López L, Valenza MC. Efficacy and Safety of Respiratory Telerehabilitation in Patients with Long COVID-19: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(18):2519. https://doi.org/10.3390/healthcare11182519
Chicago/Turabian StyleCalvache-Mateo, Andrés, Alejandro Heredia-Ciuró, Javier Martín-Núñez, Sofía Hernández-Hernández, Gregory Reychler, Laura López-López, and Marie Carmen Valenza. 2023. "Efficacy and Safety of Respiratory Telerehabilitation in Patients with Long COVID-19: A Systematic Review and Meta-Analysis" Healthcare 11, no. 18: 2519. https://doi.org/10.3390/healthcare11182519
APA StyleCalvache-Mateo, A., Heredia-Ciuró, A., Martín-Núñez, J., Hernández-Hernández, S., Reychler, G., López-López, L., & Valenza, M. C. (2023). Efficacy and Safety of Respiratory Telerehabilitation in Patients with Long COVID-19: A Systematic Review and Meta-Analysis. Healthcare, 11(18), 2519. https://doi.org/10.3390/healthcare11182519