
Machine Learning Applications in Sarcopenia Detection and Management: A Comprehensive Survey


Abstract
:1. Introduction
2. Physical Performance Test for Sarcopenia
2.1. Grip Strength
2.2. Short Physical Performance Battery (SPPB)
2.3. Gait Speed
2.4. Timed Up and Go (TUG) Test
2.5. Five Times Sit-to-Stand Test
2.6. Physical Performance Test: Challenges and Future Work
3. Cut-Offs for Diagnosing Sarcopenia
3.1. Cut-Offs of Asian Working Group of Sarcopenia
- Screening older adults for sarcopenia using a combination of muscle mass, muscle strength, and physical performance measures.
- Implementing lifestyle interventions and providing related health education for primary healthcare and preventive service users with potential sarcopenia.
- Referring patients to a hospital for a confirmatory diagnosis if sarcopenia is suspected.
- Investigating potential underlying causes of sarcopenia, particularly reversible ones, in hospital and research settings.
- Developing appropriate personalized intervention programs for older adults with sarcopenia, including resistance training, nutritional support, and pharmacological interventions if necessary.
3.2. Cut-Offs of European Working Group of Sarcopenia
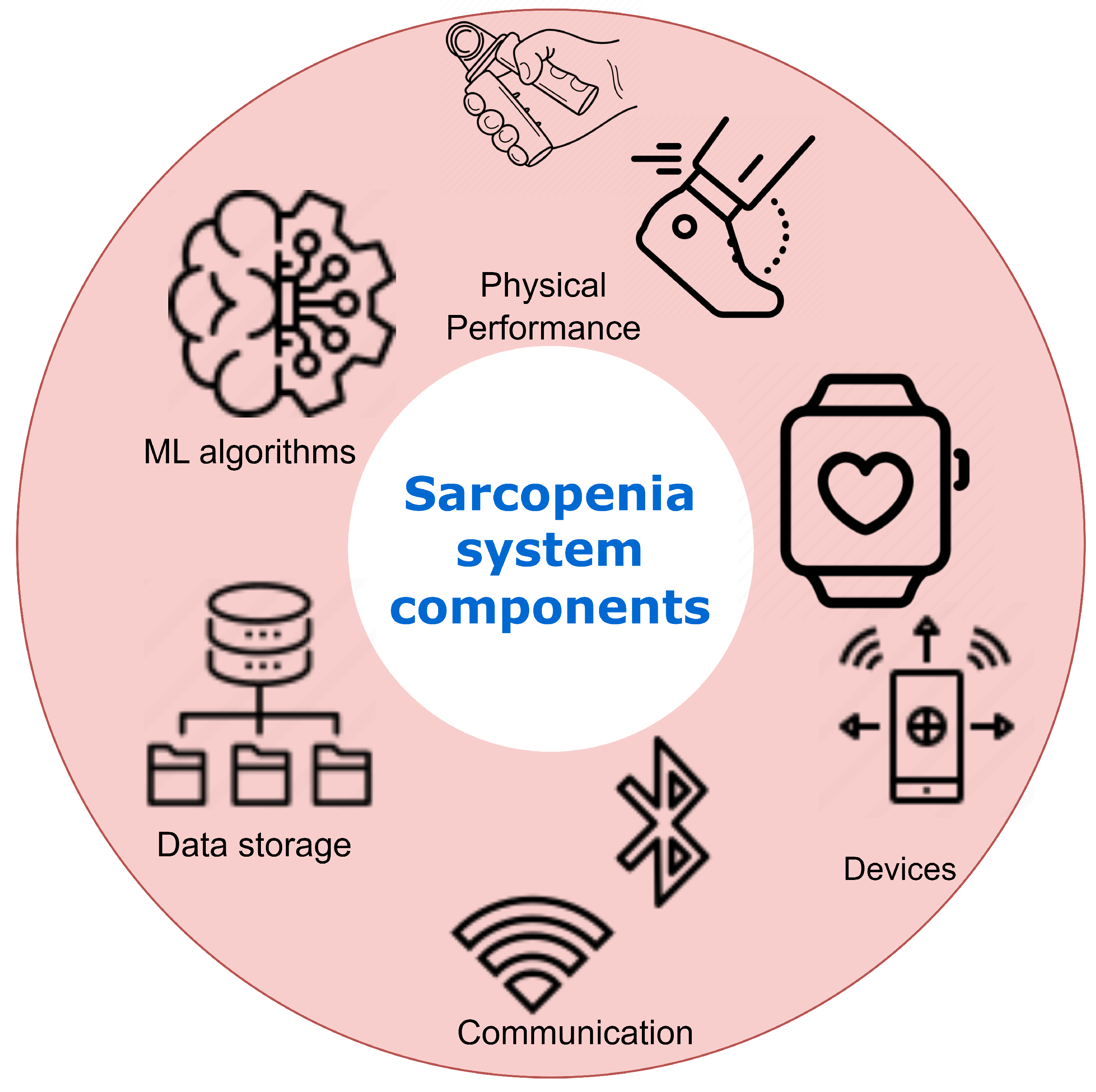
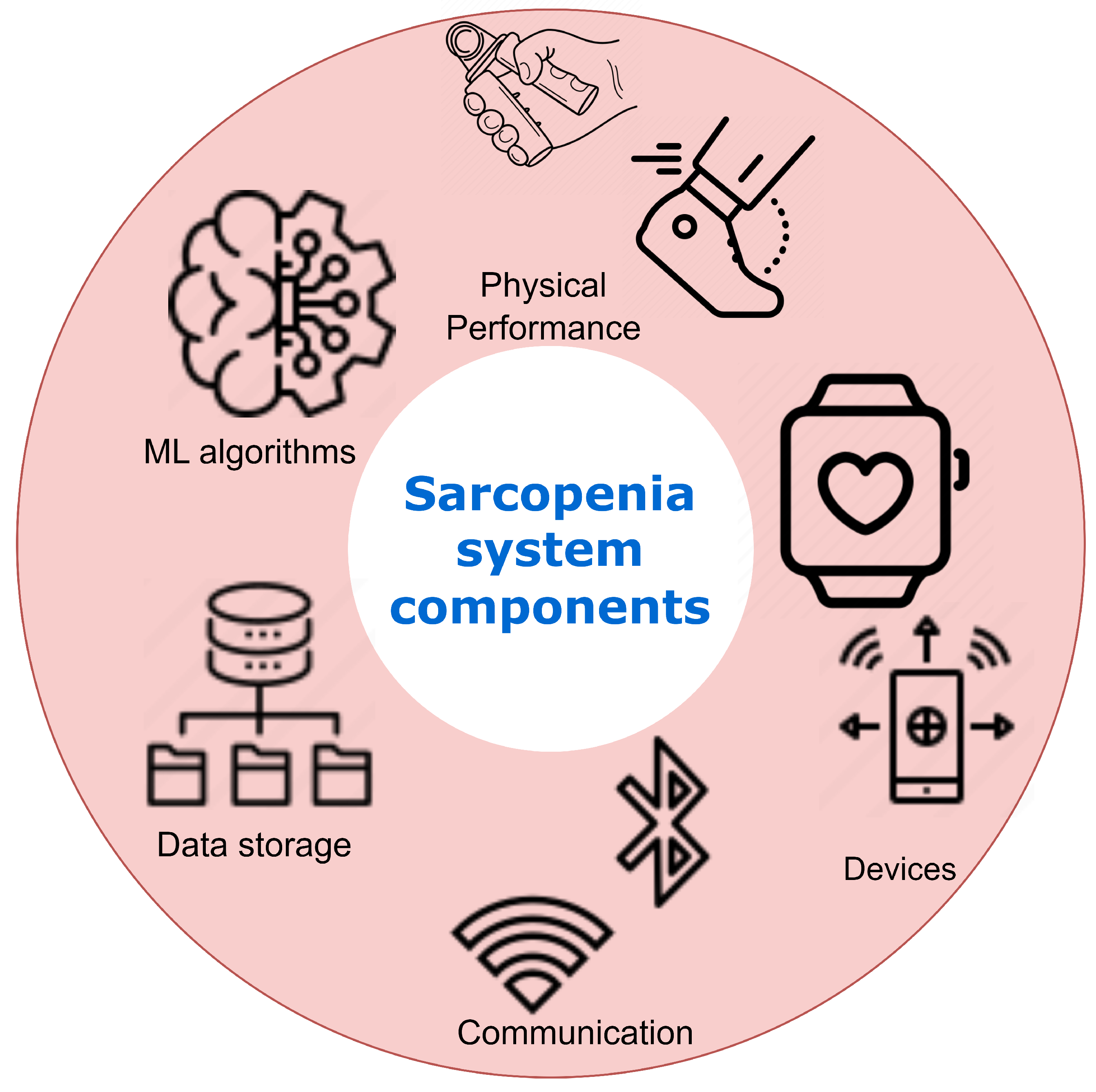
4. Digital Health Technologies and IoT Devices for Sarcopenia Management
4.1. Physical Activity Monitoring
4.2. IoT Integration
4.3. Edge Computing Infrastructure
4.4. AI and Machine Learning
4.5. User Interface and Clinical Feedback
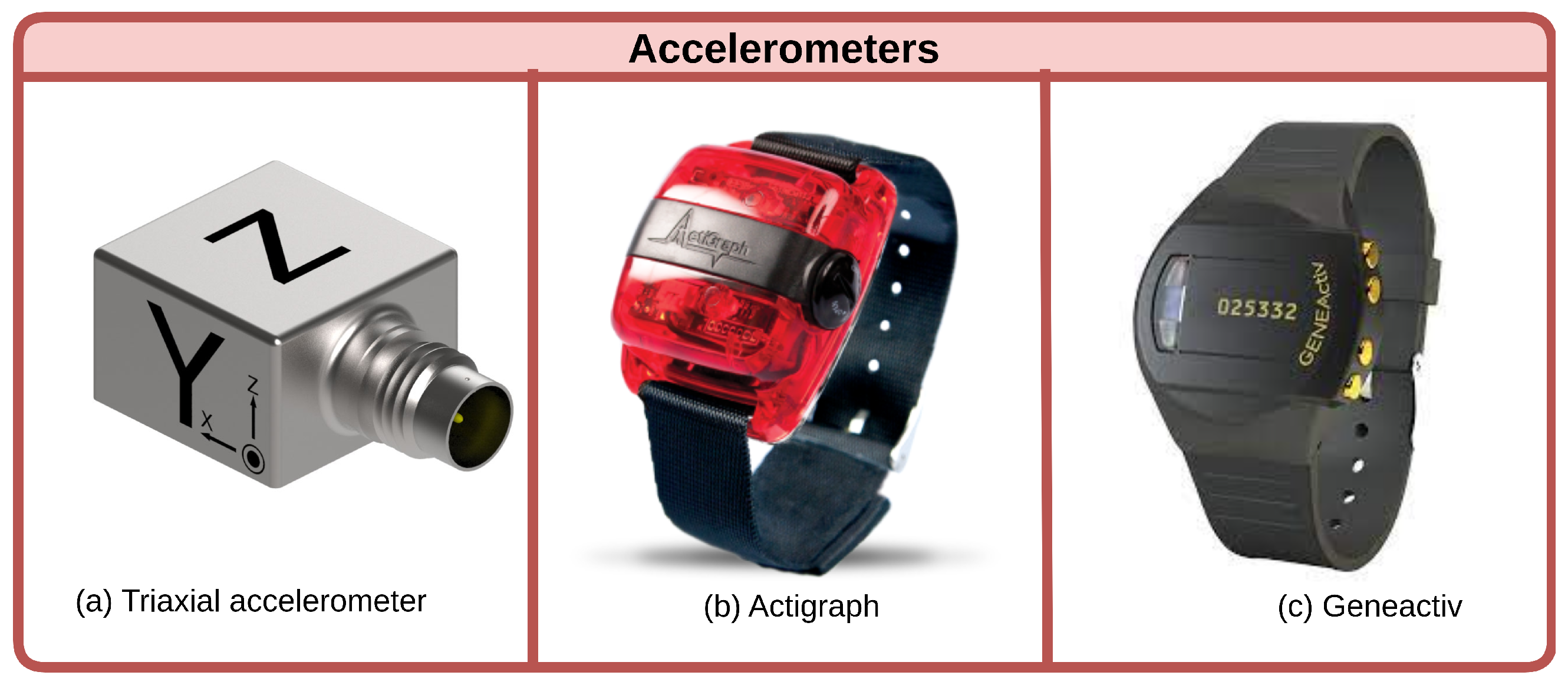
4.6. Accelerometers
4.7. Pedometers
4.8. Inertial Measurement Units (IMUs)
4.9. Pressure-Sensitive Insoles
4.10. Smartphone Applications
4.11. Challenges and Future Work
5. Healthcare Platform
5.1. Sarcopenia Datasets
5.2. Cloud Computing in Healthcare
5.3. Blockchain in Healthcare
5.4. Edge in Healthcare
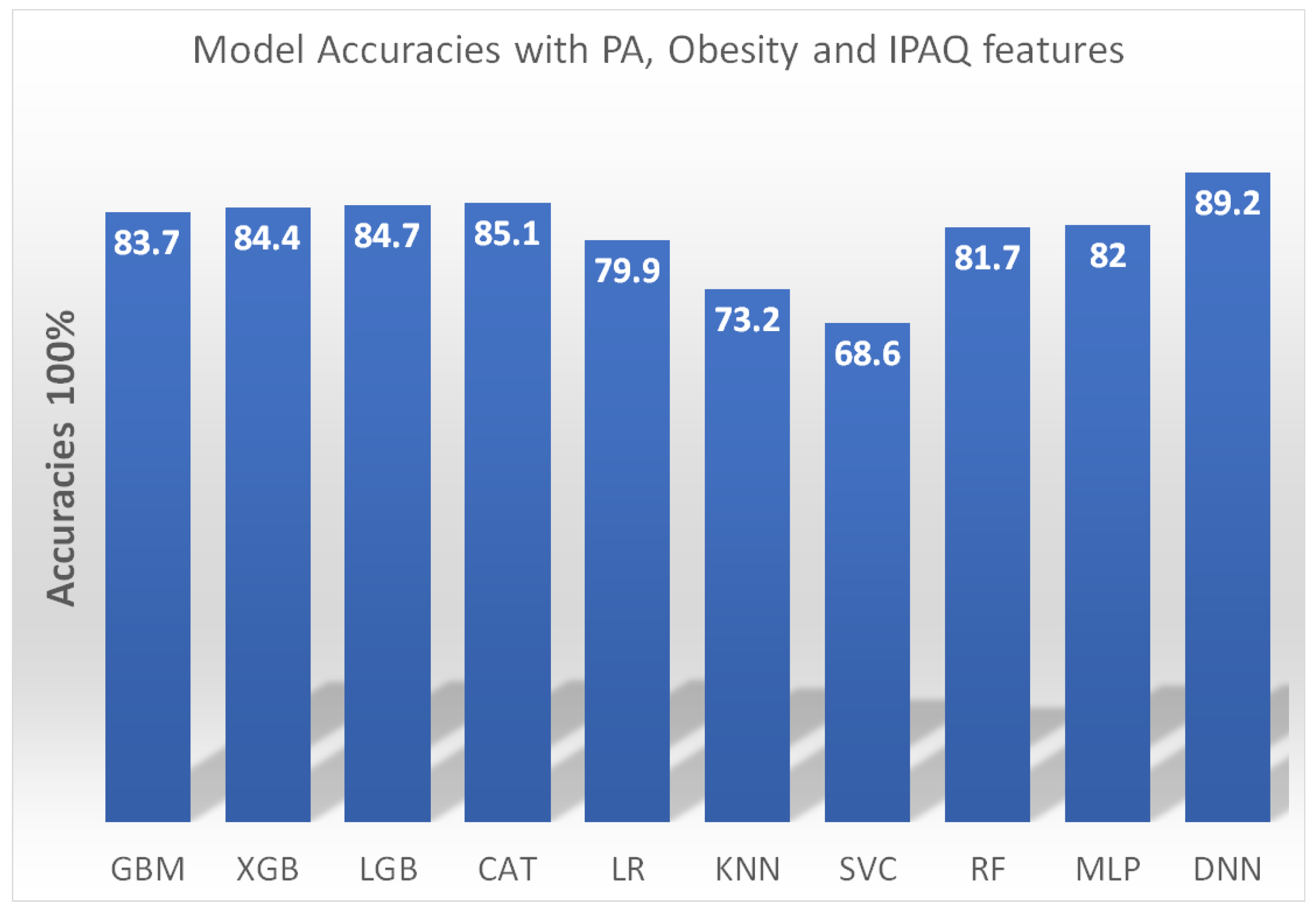
6. Machine Learning Algorithms
6.1. Logistic Regression
6.2. Support Vector Machine
- As underlined by Seok and Kim [99], one primary constraint lies in the data limitation. SVM is inherently dependent on ample datasets for effective model training. However, accumulating extensive data for sarcopenia prediction is daunting, as it necessitates specialized apparatus and expertise.
- Kang et al. [89] elaborate on the sensitivity of SVM towards feature selection. The careful selection of appropriate features becomes a pivotal aspect of achieving optimum accuracy in sarcopenia prediction.
- E Kim [105] raises a valid concern about the generalizability of SVM models. Due to the specific datasets used for model training, SVM models may lack the ability to generalize across new datasets or varied populations. This could potentially limit the model’s capacity to encapsulate the complete variation of sarcopenia across disparate populations.
- A significant interpretability issue is raised by Castillo et al. [106]. They highlight that SVM models are frequently seen as “black box” models, which pose a challenge in interpreting the path leading to the model’s predictions. This could hinder our understanding of the underpinning mechanisms of sarcopenia and the development of targeted interventions.
6.3. Random Forest
6.4. Gradient Boosting Machines
6.5. K-Nearest Neighbors
6.6. Explainable AI
7. Research Challenges
7.1. Machine Learning Challenges in Sarcopenia Detection
7.2. Challenges in Physical Performance Measurement
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Abbreviation | Explanation |
| EWGSOP | European Working Group on Sarcopenia in Older People |
| AWGSOP | Asian Working Group for Sarcopenia |
| DEXA | Dual-energy X-ray absorptiometry |
| CT | Computed tomography |
| MRI | Magnetic resonance imaging |
| ADMA | Asymmetric dimethylarginine |
| SPPB | Short Physical Performance Battery |
| TUG | Timed up and go test |
| 5TSTS | Five times sit-to-stand test |
| MVPA | Moderate-to-vigorous physical activity |
| ALM | Appendicular lean mass |
| SMOTE | Synthetic Minority Oversampling Technique |
| SVM | Support vector machine |
| RF | Random forest |
| GBM | Gradient boosting machines |
| KNN | K-nearest neighbors |
| IMU | Inertial measurement unit |
| IoT | Internet of Things |
| ICT | Information and communication technology |
| AI | Artificial intelligence |
| ML | Machine learning |
References
- Supriya, R.; Singh, K.P.; Gao, Y.; Li, F.; Dutheil, F.; Baker, J.S. A multifactorial approach for sarcopenia assessment: A literature review. Biology 2021, 10, 1354. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.; Yang, Y.; Zeng, Y.; Qiu, Y.; Chen, Y.; Zhu, L.; Fu, P.; Yan, F.; Chen, Y.; Yuan, H. Use machine learning to help identify possible sarcopenia cases in maintenance hemodialysis patients. BMC Nephrol. 2023, 24, 34. [Google Scholar]
- Hegde, P.; Maddikunta, P.K.R. Amalgamation of Blockchain with resource-constrained IoT devices for Healthcare applications–State of Art, Challenges and Future Directions. Int. J. Cogn. Comput. Eng. 2023, 4, 220–239. [Google Scholar] [CrossRef]
- Cooper, R.; Shkolnikov, V.M.; Kudryavtsev, A.V.; Malyutina, S.; Ryabikov, A.; Arnesdatter Hopstock, L.; Johansson, J.; Cook, S.; Leon, D.A.; Strand, B.H. Between-study differences in grip strength: A comparison of Norwegian and Russian adults aged 40–69 years. J. Cachexia Sarcopenia Muscle 2021, 12, 2091–2100. [Google Scholar] [CrossRef]
- Ha, Y.C.; Hwang, S.C.; Song, S.Y.; Lee, C.; Park, K.S.; Yoo, J.I. Hand grip strength measurement in different epidemiologic studies using various methods for diagnosis of sarcopenia: A systematic review. Eur. Geriatr. Med. 2018, 9, 277–288. [Google Scholar] [CrossRef]
- Jeong, H.Y.; Kim, N.H.; Choi, J.H.; Lee, C.S. Hand Grip Strength Estimation for Sarcopenia Diagnosis by Finger Tracking. In Proceedings of the 2021 IEEE International Conference on Consumer Electronics-Asia (ICCE-Asia), Gangwon, Republic of Korea, 1–3 November 2021; pp. 1–3. [Google Scholar]
- Barrios, L.; Oldrati, P.; Lindlbauer, D.; Hilty, M.; Hayward-Koennecke, H.; Holz, C.; Lutterotti, A. A rapid tapping task on commodity smartphones to assess motor fatigability. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020; pp. 1–10. [Google Scholar]
- Soysal, P.; Isik, A.T. Different hand-grip strength cut-offs to define sarcopenia in Turkish population. Aging Clin. Exp. Res. 2021, 33, 209–210. [Google Scholar] [CrossRef]
- Fernandes, S.; Rodrigues da Silva, E.; New York, B.; Macedo, P.; Gonçalves, R.; Camara, S.; Larco, R.; Maciel, A. Cutoff Points for Grip Strength in Screening for Sarcopenia in Community-Dwelling Older-Adults: A Systematic Review. J. Nutr. Health Aging 2022, 26, 452–460. [Google Scholar] [CrossRef]
- Lim, J.P.; Yew, S.; Tay, L.; Chew, J.; Yeo, A.; Ismail, N.H.; Ding, Y.; Lim, W. Grip strength criterion matters: Impact of average versus maximum handgrip strength on sarcopenia prevalence and predictive validity for low physical performance. J. Nutr. Health Aging 2020, 24, 1031–1035. [Google Scholar] [CrossRef]
- De, A.; Kumari, S.; Kaur, A.; Singh, A.; Kalra, N.; Singh, V. Hand-grip strength as a screening tool for sarcopenia in males with decompensated cirrhosis. Indian J. Gastroenterol. 2022, 41, 284–291. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Schaap, L.; Fox, B.; Henwood, T.; Bruyère, O.; Reginster, J.Y.; Beaudart, C.; Buckinx, F.; Roberts, H.; Cooper, C.; Cherubini, A.; et al. Grip strength measurement: Towards a standardized approach in sarcopenia research and practice. Eur. Geriatr. Med. 2016, 7, 247–255. [Google Scholar] [CrossRef]
- Yokoro, M.; Otaki, N.; Yano, M.; Imamura, T.; Tanino, N.; Fukuo, K. Association between asymmetric dimethylarginine and sarcopenia in community-dwelling older women. Sci. Rep. 2023, 13, 5510. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Cao, L.; Wang, J.; Wang, Y.; Hao, H.; Huang, L. Characterization of serum protein expression profiles in the early sarcopenia older adults with low grip strength: A cross-sectional study. BMC Musculoskelet. Disord. 2022, 23, 894. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Choo, P.L.; Pang, B.W.J.; Lau, L.K.; Jabbar, K.A.; Seah, W.T.; Chen, K.K.; Ng, T.P.; Wee, S.L. SPPB reference values and performance in assessing sarcopenia in community-dwelling Singaporeans–Yishun study. BMC Geriatr. 2021, 21, 213. [Google Scholar] [CrossRef] [PubMed]
- Phu, S.; Kirk, B.; Bani Hassan, E.; Vogrin, S.; Zanker, J.; Bernardo, S.; Duque, G. The diagnostic value of the Short Physical Performance Battery for sarcopenia. BMC Geriatr. 2020, 20, 242. [Google Scholar] [CrossRef]
- Soh, Y.; Won, C.W. Sex differences in impact of sarcopenia on falls in community-dwelling Korean older adults. BMC Geriatr. 2021, 21, 716. [Google Scholar] [CrossRef]
- Yasuda, T.; Nakajima, T.; Sawaguchi, T.; Nozawa, N.; Arakawa, T.; Takahashi, R.; Mizushima, Y.; Katayanagi, S.; Matsumoto, K.; Toyoda, S.; et al. Short Physical Performance Battery for cardiovascular disease inpatients: Implications for critical factors and sarcopenia. Sci. Rep. 2017, 7, 17425. [Google Scholar] [CrossRef]
- Sheng, Y.; Ma, D.; Zhou, Q.; Wang, L.; Sun, M.; Wang, S.; Qi, H.; Liu, J.; Ding, G.; Duan, Y. Association of thyroid function with sarcopenia in elderly Chinese euthyroid subjects. Aging Clin. Exp. Res. 2019, 31, 1113–1120. [Google Scholar] [CrossRef]
- Choi, S.; Chon, J.; Lee, S.A.; Yoo, M.C.; Yun, Y.; Chung, S.J.; Kim, M.; Lee, E.T.; Kyu Choi, M.; Won, C.W.; et al. Central obesity is associated with lower prevalence of sarcopenia in older women, but not in men: A cross-sectional study. BMC Geriatr. 2022, 22, 406. [Google Scholar] [CrossRef]
- Maurus, J.; Terzer, T.; Benner, A.; Goisser, S.; Eidam, A.; Roth, A.; Janssen, M.; Jaramillo, S.; Lorenz, H.M.; Micol, W.; et al. Validation of a proxy-reported SARC-F questionnaire for current and retrospective screening of sarcopenia-related functional impairments. J. Cachexia Sarcopenia Muscle 2022, 13, 264–275. [Google Scholar] [CrossRef]
- Perez-Sousa, M.A.; Venegas-Sanabria, L.C.; Chavarro-Carvajal, D.A.; Cano-Gutierrez, C.A.; Izquierdo, M.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Gait speed as a mediator of the effect of sarcopenia on dependency in activities of daily living. J. Cachexia Sarcopenia Muscle 2019, 10, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Chen, H.C.; Liou, T.H.; Lin, C.L.; Huang, S.W. Impact of sarcopenia and obesity on gait speed after total knee replacement. J. Am. Med. Dir. Assoc. 2022, 23, 631–637. [Google Scholar] [CrossRef]
- Fan, Y.; Zhang, B.; Huang, G.; Zhang, G.; Ding, Z.; Li, Z.; Sinclair, J.; Fan, Y. Sarcopenia: Body composition and gait analysis. Front. Aging Neurosci. 2022, 14, 909551. [Google Scholar] [CrossRef] [PubMed]
- Merchant, R.A.; Chan, Y.H.; Hui, R.J.Y.; Lim, J.Y.; Kwek, S.C.; Seetharaman, S.K.; Au, L.S.Y.; Morley, J.E. Possible sarcopenia and impact of dual-task exercise on gait speed, handgrip strength, falls, and perceived health. Front. Med. 2021, 8, 660463. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Murata, S.; Goda, A.; Kikuchi, Y.; Shiraiwa, K.; Horie, J.; Nakano, H. Gait Characteristics of Dynapenia, Sarcopenia, and Presarcopenia in Community-Dwelling Japanese Older Women: A Cross-Sectional Study. Healthcare 2022, 10, 1905. [Google Scholar] [CrossRef]
- Kang, M.g.; Kang, S.J.; Roh, H.K.; Jung, H.Y.; Kim, S.w.; Choi, J.Y.; Kim, K.i. Accuracy and Diversity of Wearable Device–Based Gait Speed Measurement Among Older Men: Observational Study. J. Med. Internet Res. 2021, 23, e29884. [Google Scholar] [CrossRef]
- Zhou, Z.; Huang, Y.; Wang, J.; Su, H.; Tang, H.; Wang, Y. A novel digital biomarker of sarcopenia in frail elderly: New combination of gait parameters under dual-task walking. Front. Aging Neurosci. 2023, 15, 1087318. [Google Scholar] [CrossRef]
- Kim, M.; Won, C.W. Sarcopenia is associated with cognitive impairment mainly due to slow gait speed: Results from the Korean Frailty and Aging Cohort Study (KFACS). Int. J. Environ. Res. Public Health 2019, 16, 1491. [Google Scholar] [CrossRef]
- Sakai, Y.; Wakao, N.; Matsui, H.; Tomita, K.; Watanabe, T.; Iida, H. Surgical results in older patients with lumbar spinal stenosis according to gait speed in relation to the diagnosis for sarcopenia. J. Orthop. Surg. 2020, 28, 2309499020918422. [Google Scholar] [CrossRef]
- Kostka, J.; Sosowska, N.; Guligowska, A.; Kostka, T. A Proposed Method of Converting Gait Speed and TUG Test in Older Subjects. Int. J. Environ. Res. Public Health 2022, 19, 12145. [Google Scholar] [CrossRef]
- Kovelis, D.; Gomes, A.R.S.; Mazzarin, C.; de Miranda, A.; Valderramas, S. Association between the results of the timed up-and-go test adjusted for disease severity and sarcopenia in patients with chronic obstructive pulmonary disease: A pilot study. Clinics 2019, 74, e930. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Park, K.S.; Yoo, J.I. Associations between the quality of life in sarcopenia measured with the SarQoL® and nutritional status. Health Qual. Life Outcomes 2021, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Bahat, G.; Kilic, C.; Eris, S.; Karan, M. Power versus sarcopenia: Associations with functionality and physical performance measures. J. Nutr. Health Aging 2021, 25, 13–17. [Google Scholar] [CrossRef]
- Santos, C.A.; Cinza, A.M.; Laranjeira, Â.; Amaro, M.; Carvalho, M.; Bravo, J.; Martins, S.; Raimundo, A. A dataset on skeletal muscle mass index, body composition and strength to determinate sarcopenia in bariatric patients. Data Brief 2023, 46, 108881. [Google Scholar] [CrossRef] [PubMed]
- Yee, X.S.; Ng, Y.S.; Allen, J.C.; Latib, A.; Tay, E.L.; Abu Bakar, H.M.; Ho, C.Y.J.; Koh, W.C.C.; Kwek, H.H.T.; Tay, L. Performance on sit-to-stand tests in relation to measures of functional fitness and sarcopenia diagnosis in community-dwelling older adults. Eur. Rev. Aging Phys. Act. 2021, 18, 1. [Google Scholar] [CrossRef]
- Alcazar, J.; Losa-Reyna, J.; Rodriguez-Lopez, C.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Alegre, L.M. The sit-to-stand muscle power test: An easy, inexpensive and portable procedure to assess muscle power in older people. Exp. Gerontol. 2018, 112, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Oytun, M.G.; Doğu, B.; Cankurtaran, M.; Halil, M. Association of sarcopenia and fall risk according to five-times sit to stand test in older adults. Age 2021, 76, 70-64. [Google Scholar]
- Montemurro, A.; Ruiz-Cárdenas, J.D.; del Mar Martínez-García, M.; Rodríguez-Juan, J.J. Consequences of applying the different criteria of the EWGSOP2 guideline for sarcopenia case-finding in Spanish community-dwelling older adults. Arch. Gerontol. Geriatr. 2023, 109, 104964. [Google Scholar] [CrossRef]
- Yoshiko, A.; Ogawa, M.; Shimizu, K.; Radaelli, R.; Neske, R.; Maeda, H.; Maeda, K.; Teodoro, J.; Tanaka, N.; Pinto, R.S.; et al. Chair sit-to-stand performance is associated with diagnostic features of sarcopenia in older men and women. Arch. Gerontol. Geriatr. 2021, 96, 104463. [Google Scholar] [CrossRef]
- Porto, J.M.; Peres-Ueno, M.J.; Braghin, R.d.M.B.; Scudilio, G.M.; de Abreu, D.C.C. Diagnostic accuracy of the five times stand-to-sit test for the screening of global muscle weakness in community-dwelling older women. Exp. Gerontol. 2023, 171, 112027. [Google Scholar] [CrossRef]
- Bohannon, R.W. Grip strength: An indispensable biomarker for older adults. Clin. Interv. Aging 2019, 14, 1681–1691. [Google Scholar] [CrossRef] [PubMed]
- Pratt, J.; De Vito, G.; Narici, M.; Segurado, R.; Dolan, J.; Conroy, J.; Boreham, C. Grip strength performance from 9431 participants of the GenoFit study: Normative data and associated factors. Geroscience 2021, 43, 2533–2546. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Pardo, P.J.; González-Gálvez, N.; Carbonell-Baeza, A.; Jiménez-Pavón, D.; Vaquero-Cristóbal, R. GDLAM and SPPB batteries for screening sarcopenia in community-dwelling Spanish older adults: Healthy-age network study. Exp. Gerontol. 2023, 172, 112044. [Google Scholar] [CrossRef]
- Beaudart, C.; McCloskey, E.; Bruyère, O.; Cesari, M.; Rolland, Y.; Rizzoli, R.; Araujo de Carvalho, I.; Amuthavalli Thiyagarajan, J.; Bautmans, I.; Bertière, M.C.; et al. Sarcopenia in daily practice: Assessment and management. BMC Geriatr. 2016, 16, 170. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.I.; Kim, M.C. Physical Therapy Assessment Tool Threshold Values to Identify Sarcopenia and Locomotive Syndrome in the Elderly. Int. J. Environ. Res. Public Health 2023, 20, 6098. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Spexoto, M.C.B.; Ramírez, P.C.; de Oliveira Máximo, R.; Steptoe, A.; De Oliveira, C.; Alexandre, T.d.S. European Working Group on Sarcopenia in Older People 2010 (EWGSOP1) and 2019 (EWGSOP2) criteria or slowness: Which is the best predictor of mortality risk in older adults? Age Ageing 2022, 51, afac164. [Google Scholar] [CrossRef]
- Scott, D.; Johansson, J.; Gandham, A.; Ebeling, P.R.; Nordstrom, P.; Nordstrom, A. Associations of accelerometer-determined physical activity and sedentary behavior with sarcopenia and incident falls over 12 months in community-dwelling Swedish older adults. J. Sport Health Sci. 2021, 10, 577–584. [Google Scholar] [CrossRef]
- Johansson, J.; Morseth, B.; Scott, D.; Strand, B.H.; Hopstock, L.A.; Grimsgaard, S. Moderate-to-vigorous physical activity modifies the relationship between sedentary time and sarcopenia: The Tromsø Study 2015–2016. J. Cachexia Sarcopenia Muscle 2021, 12, 955–963. [Google Scholar] [CrossRef]
- Iwasaka, C.; Yamada, Y.; Nishida, Y.; Hara, M.; Yasukata, J.; Miyoshi, N.; Shimanoe, C.; Nanri, H.; Furukawa, T.; Koga, K.; et al. Dose-response relationship between daily step count and prevalence of sarcopenia: A cross-sectional study. Exp. Gerontol. 2023, 175, 112135. [Google Scholar] [CrossRef]
- Kitamura, M.; Izawa, K.P.; Ishihara, K.; Matsuda, H.; Okamura, S.; Fujioka, K. Physical activity and sarcopenia in community-dwelling older adults with long-term care insurance. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1610–1618. [Google Scholar] [CrossRef] [PubMed]
- Ohtsubo, T.; Nozoe, M.; Kanai, M.; Yasumoto, I.; Ueno, K. Association of sarcopenia and physical activity with functional outcome in older Asian patients hospitalized for rehabilitation. Aging Clin. Exp. Res. 2022, 34, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Connolly, K.; Cunningham, C.; Murphy, N.; Romero-Ortuno, R.; Horgan, F. Using accelerometers in the assessment of sarcopenia in older adults attending a day hospital service in Ireland. J. Frailty Sarcopenia Falls 2021, 6, 98. [Google Scholar] [CrossRef] [PubMed]
- Westbury, L.D.; Dodds, R.M.; Syddall, H.E.; Baczynska, A.M.; Shaw, S.C.; Dennison, E.M.; Roberts, H.C.; Sayer, A.A.; Cooper, C.; Patel, H.P. Associations between objectively measured physical activity, body composition and sarcopenia: Findings from the Hertfordshire Sarcopenia Study (HSS). Calcif. Tissue Int. 2018, 103, 237–245. [Google Scholar] [CrossRef]
- Ramsey, K.A.; Rojer, A.G.; D’Andrea, L.; Otten, R.H.; Heymans, M.W.; Trappenburg, M.C.; Verlaan, S.; Whittaker, A.C.; Meskers, C.G.; Maier, A.B. The association of objectively measured physical activity and sedentary behavior with skeletal muscle strength and muscle power in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 67, 101266. [Google Scholar] [CrossRef]
- Yuenyongchaiwat, K.; Akekawatchai, C.; Khattiya, J. Effects of a Pedometer-Based Walking Home Program Plus Resistance Training on Inflammatory Cytokines and Depression in Thai Older People with Sarcopenia: A Three-Arm Randomized Controlled Trial. Clin. Gerontol. 2022, 1–12. [Google Scholar] [CrossRef]
- Meier, N.F.; Lee, D.c. Physical activity and sarcopenia in older adults. Aging Clin. Exp. Res. 2020, 32, 1675–1687. [Google Scholar] [CrossRef]
- Park, H.; Park, S.; Shephard, R.J.; Aoyagi, Y. Yearlong physical activity and sarcopenia in older adults: The Nakanojo Study. Eur. J. Appl. Physiol. 2010, 109, 953–961. [Google Scholar] [CrossRef]
- Yuenyongchaiwat, K.; Akekawatchai, C. Beneficial effects of walking-based home program for improving cardio-respiratory performance and physical activity in sarcopenic older people: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2022. [Google Scholar] [CrossRef]
- Ortega-Bastidas, P.; Aqueveque, P.; Gómez, B.; Saavedra, F.; Cano-de-la Cuerda, R. Use of a single wireless IMU for the segmentation and automatic analysis of activities performed in the 3-m timed up & go test. Sensors 2019, 19, 1647. [Google Scholar]
- Kim, J.K.; Bae, M.N.; Lee, K.; Kim, J.C.; Hong, S.G. Explainable Artificial Intelligence and Wearable Sensor-Based Gait Analysis to Identify Patients with Osteopenia and Sarcopenia in Daily Life. Biosensors 2022, 12, 167. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Youm, C.; Park, H.; Lee, M.; Choi, H. Association of Muscle Mass, Muscle Strength, and Muscle Function with Gait Ability Assessed Using Inertial Measurement Unit Sensors in Older Women. Int. J. Environ. Res. Public Health 2022, 19, 9901. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Bae, M.N.; Lee, K.B.; Hong, S.G. Identification of patients with sarcopenia using gait parameters based on inertial sensors. Sensors 2021, 21, 1786. [Google Scholar] [CrossRef] [PubMed]
- Byun, S.; Lee, H.J.; Han, J.W.; Kim, J.S.; Choi, E.; Kim, K.W. Walking-speed estimation using a single inertial measurement unit for the older adults. PLoS ONE 2019, 14, e0227075. [Google Scholar] [CrossRef]
- Kraus, M.; Saller, M.M.; Baumbach, S.F.; Neuerburg, C.; Stumpf, U.C.; Böcker, W.; Keppler, A.M. Prediction of physical frailty in orthogeriatric patients using sensor insole–based gait analysis and machine learning algorithms: Cross-sectional study. JMIR Med. Inform. 2022, 10, e32724. [Google Scholar] [CrossRef]
- Anzai, E.; Ren, D.; Cazenille, L.; Aubert-Kato, N.; Tripette, J.; Ohta, Y. Random forest algorithms to classify frailty and falling history in seniors using plantar pressure measurement insoles: A large-scale feasibility study. BMC Geriatr. 2022, 22, 746. [Google Scholar]
- Drăgulinescu, A.; Drăgulinescu, A.M.; Zincă, G.; Bucur, D.; Feieș, V.; Neagu, D.M. Smart socks and in-shoe systems: State-of-the-art for two popular technologies for foot motion analysis, sports, and medical applications. Sensors 2020, 20, 4316. [Google Scholar] [CrossRef]
- Atreya, S.; Sharma, U.; Anand, S. The effect of accessing workplace heights on plantar pressure distribution in elderly. Gait Posture 2020, 81, 15–16. [Google Scholar] [CrossRef]
- Martini, E.; Fiumalbi, T.; Dell’Agnello, F.; Ivanić, Z.; Munih, M.; Vitiello, N.; Crea, S. Pressure-sensitive insoles for real-time gait-related applications. Sensors 2020, 20, 1448. [Google Scholar] [CrossRef]
- Silva, P.M.; Holanda, L.J.; Granados, E.E.; Morya, E. Building Pressure-Sensitive Foot Insoles for Public Health Evaluation in Smart Cities. In Proceedings of the 2017 IEEE First Summer School on Smart Cities (S3C), Natal, Brazil, 6–11 August 2017; pp. 153–156. [Google Scholar]
- Subramaniam, S.; Faisal, A.I.; Deen, M.J. Wearable sensor systems for fall risk assessment: A review. Front. Digit. Health 2022, 4, 921506. [Google Scholar] [CrossRef]
- Kato, Y.; Sakamoto, R.; Hori, A.; Momosaki, R. Innovation in Digital Health Interventions for Frailty and Sarcopenia. J. Clin. Med. 2023, 12, 2341. [Google Scholar] [CrossRef]
- Scott, R.A.; Callisaya, M.L.; Duque, G.; Ebeling, P.R.; Scott, D. Assistive technologies to overcome sarcopenia in ageing. Maturitas 2018, 112, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, A.; Ruiz-Cárdenas, J.D.; Martínez-García, M.d.M.; Rodríguez-Juan, J.J. Validity of an iPhone App to Detect Prefrailty and Sarcopenia Syndromes in Community-Dwelling Older Adults: The Protocol for a Diagnostic Accuracy Study. Sensors 2022, 22, 6010. [Google Scholar] [CrossRef] [PubMed]
- Mohieldin, S.; Minor, C.M.; Petersen, C.L.; Batsis, J.A.; Halter, R.J. BandPass: A Bluetooth-Enabled Remote Monitoring Device for Sarcopenia. In Proceedings of the 2021 IEEE International Conference on Communications Workshops (ICC Workshops), Montreal, QC, Canada, 14–23 June 2021; pp. 1–6. [Google Scholar]
- Lera, L.; Angel, B.; Márquez, C.; Saguez, R.; Albala, C. Software for the diagnosis of sarcopenia in community-dwelling older adults: Design and Validation Study. JMIR Med. Inform. 2020, 8, e13657. [Google Scholar] [CrossRef]
- Tannir, H.; Itani, L.; Kreidieh, D.; El Masri, D.; El Ghoch, M. Can Intentional Weight Loss Ameliorate Sarcopenia in Individuals with Obesity? A Longitudinal Interventional Study. Clin. Pract. 2022, 12, 106–112. [Google Scholar] [CrossRef]
- Warmerdam, E.; Hansen, C.; Romijnders, R.; Hobert, M.A.; Welzel, J.; Maetzler, W. Full-body mobility data to validate inertial measurement unit algorithms in healthy and neurological cohorts. Data 2022, 7, 136. [Google Scholar] [CrossRef]
- Sconfienza, L.M. Sarcopenia: Ultrasound today, smartphones tomorrow? Eur. Radiol. 2019, 29, 1–2. [Google Scholar] [CrossRef]
- Zhang, H.; Yin, M.; Liu, Q.; Ding, F.; Hou, L.; Deng, Y.; Cui, T.; Han, Y.; Pang, W.; Ye, W.; et al. Machine and deep learning-based clinical characteristics and laboratory markers for the prediction of sarcopenia. Chin. Med. J. 2023, 136, 967–973. [Google Scholar] [CrossRef]
- Castillo-Olea, C.; Garcia-Zapirain Soto, B.; Zuñiga, C. Evaluation of prevalence of the sarcopenia level using machine learning techniques: Case study in Tijuana Baja California, Mexico. Int. J. Environ. Res. Public Health 2020, 17, 1917. [Google Scholar] [CrossRef]
- Zupo, R.; Moroni, A.; Castellana, F.; Gasparri, C.; Catino, F.; Lampignano, L.; Perna, S.; Clodoveo, M.L.; Sardone, R.; Rondanelli, M. A Machine-Learning Approach to Target Clinical and Biological Features Associated with Sarcopenia: Findings from Northern and Southern Italian Aging Populations. Metabolites 2023, 13, 565. [Google Scholar] [CrossRef]
- Wu, L.W.; OuYoung, T.; Chiu, Y.C.; Hsieh, H.F.; Hsiu, H. Discrimination between possible sarcopenia and metabolic syndrome using the arterial pulse spectrum and machine-learning analysis. Sci. Rep. 2022, 12, 21452. [Google Scholar] [CrossRef] [PubMed]
- Cernea, A.; Fernández-Martínez, J.L.; de Andrés-Galiana, E.J.; Fernández-Muñiz, Z.; Bermejo-Millo, J.C.; González-Blanco, L.; Solano, J.J.; Abizanda, P.; Coto-Montes, A.; Caballero, B. Prognostic networks for unraveling the biological mechanisms of Sarcopenia. Mech. Ageing Dev. 2019, 182, 111129. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Won, C.W. Sarcopenia in Korean community-dwelling adults aged 70 years and older: Application of screening and diagnostic tools from the Asian working group for sarcopenia 2019 update. J. Am. Med. Dir. Assoc. 2020, 21, 752–758. [Google Scholar] [CrossRef]
- Lee, H.; Yim, H.W.; Won, H.S.; Ko, Y.H. The impact of sarcopenia on health-related quality of life in elderly people: Korean National Health and Nutrition Examination Survey. Korean J. Intern. Med. 2019, 34, 877. [Google Scholar]
- Kang, Y.J.; Yoo, J.I.; Ha, Y.c. Sarcopenia feature selection and risk prediction using machine learning: A cross-sectional study. Medicine 2019, 98. [Google Scholar] [CrossRef]
- Zhang, Y.; Sun, Y.; Jin, R.; Lin, K.; Liu, W. High-performance isolation computing technology for smart IoT healthcare in cloud environments. IEEE Internet Things J. 2021, 8, 16872–16879. [Google Scholar] [CrossRef]
- Dang, L.M.; Piran, M.J.; Han, D.; Min, K.; Moon, H. A survey on internet of things and cloud computing for healthcare. Electronics 2019, 8, 768. [Google Scholar] [CrossRef]
- Masud, M.; Gaba, G.S.; Choudhary, K.; Alroobaea, R.; Hossain, M.S. A robust and lightweight secure access scheme for cloud based E-healthcare services. Peer-Peer Netw. Appl. 2021, 14, 3043–3057. [Google Scholar] [CrossRef]
- Sahu, M.L.; Atulkar, M.; Ahirwal, M.K.; Ahamad, A. Cloud-based remote patient monitoring system with abnormality detection and alert notification. Mob. Netw. Appl. 2022, 27, 1894–1909. [Google Scholar] [CrossRef]
- Sha M, M.; Rahamathulla, M.P. Cloud-based Healthcare data management Framework. KSII Trans. Internet Inf. Syst. (TIIS) 2020, 14, 1014–1025. [Google Scholar]
- Zakzouk, A.; El-Sayed, A.; Hemdan, E.E.D. A blockchain-based electronic medical records management framework in smart healthcare infrastructure. Multimed. Tools Appl. 2023, 1–19. [Google Scholar] [CrossRef]
- Zhou, T.; Li, X.; Zhao, H. Med-PPPHIS: Blockchain-based personal healthcare information system for national physique monitoring and scientific exercise guiding. J. Med. Syst. 2019, 43, 305. [Google Scholar] [CrossRef] [PubMed]
- Chelladurai, U.; Pandian, S. A novel blockchain based electronic health record automation system for healthcare. J. Ambient. Intell. Humaniz. Comput. 2022, 13, 693–703. [Google Scholar] [CrossRef]
- Pawar, P.; Parolia, N.; Shinde, S.; Edoh, T.O.; Singh, M. eHealthChain—A blockchain-based personal health information management system. Ann. Telecommun. 2022, 77, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Seok, M.; Kim, W. Sarcopenia Prediction for Elderly People Using Machine Learning: A Case Study on Physical Activity. Healthcare 2023, 11, 1334. [Google Scholar] [CrossRef]
- Kaur, S.; Abdullah, A.; Hairi, N.N.; Sivanesan, S.K. Logistic regression modeling to predict sarcopenia frailty among aging adults. Int. J. Adv. Comput. Sci. Appl. 2021, 12, 497–504. [Google Scholar] [CrossRef]
- Agnes, T.; Vishal, K.; Girish, N. Regression model for the prediction of risk of sarcopenia among older adults. Muscles Ligaments Tendons J. (MLTJ) 2019, 9, 425–432. [Google Scholar] [CrossRef]
- Yin, G.; Qin, J.; Wang, Z.; Lv, F.; Ye, X. A nomogram to predict the risk of sarcopenia in older people. Medicine 2023, 102, e33581. [Google Scholar] [CrossRef]
- Austin, P.C.; Steyerberg, E.W. The Integrated Calibration Index (ICI) and related metrics for quantifying the calibration of logistic regression models. Stat. Med. 2019, 38, 4051–4065. [Google Scholar] [CrossRef]
- Ko, J.B.; Kim, K.B.; Shin, Y.S.; Han, H.; Han, S.K.; Jung, D.Y.; Hong, J.S. Predicting Sarcopenia of Female Elderly from Physical Activity Performance Measurement Using Machine Learning Classifiers. Clin. Interv. Aging 2021, 16, 1723–1733. [Google Scholar] [CrossRef]
- Kim, E. Machine Learning Classifier Models for Predicting Sarcopenia in the Elderly Based on Physical Factors. medRxiv 2023. [Google Scholar] [CrossRef]
- Castillo-Olea, C.; García-Zapirain Soto, B.; Carballo Lozano, C.; Zuñiga, C. Automatic classification of sarcopenia level in older adults: A case study at Tijuana General Hospital. Int. J. Environ. Res. Public Health 2019, 16, 3275. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.G.; Oh, D.; Noh, J.M.; Cho, W.K.; Sun, J.M.; Kim, H.K.; Zo, J.I.; Shim, Y.M.; Kim, K. Machine learning model for predicting excessive muscle loss during neoadjuvant chemoradiotherapy in oesophageal cancer. J. Cachexia Sarcopenia Muscle 2021, 12, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J. Machine learning models for sarcopenia identification based on radiomic features of muscles in computed tomography. Int. J. Environ. Res. Public Health 2021, 18, 8710. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Rescio, G.; Manni, A.; Siciliano, P.; Caroppo, A. Comparative analysis of supervised classifiers for the evaluation of sarcopenia using a sEMG-based platform. Sensors 2022, 22, 2721. [Google Scholar] [CrossRef]
- Uddin, S.; Haque, I.; Lu, H.; Moni, M.A.; Gide, E. Comparative performance analysis of K-nearest neighbour (KNN) algorithm and its different variants for disease prediction. Sci. Rep. 2022, 12, 6256. [Google Scholar] [CrossRef] [PubMed]
- Sangaiah, A.K.; Rezaei, S.; Javadpour, A.; Zhang, W. Explainable AI in big data intelligence of community detection for digitalization e-healthcare services. Appl. Soft Comput. 2023, 136, 110119. [Google Scholar] [CrossRef]
- Tagliafico, A.S.; Bignotti, B.; Torri, L.; Rossi, F. Sarcopenia: How to measure, when and why. Radiol. Med. 2022, 127, 228–237. [Google Scholar] [CrossRef]
- Dent, E.; Woo, J.; Scott, D.; Hoogendijk, E.O. Sarcopenia measurement in research and clinical practice. Eur. J. Intern. Med. 2021, 90, 1–9. [Google Scholar] [CrossRef]
- Chen, Z.; Ho, M.; Chau, P.H. Prevalence, incidence, and associated factors of possible sarcopenia in community-dwelling Chinese older adults: A population-based longitudinal study. Front. Med. 2022, 8, 2285. [Google Scholar] [CrossRef]
- Turimov Mustapoevich, D.; Muhamediyeva Tulkunovna, D.; Safarova Ulmasovna, L.; Primova, H.; Kim, W. Improved Cattle Disease Diagnosis Based on Fuzzy Logic Algorithms. Sensors 2023, 23, 2107. [Google Scholar] [CrossRef] [PubMed]
- Nodirov, J.; Abdusalomov, A.B.; Whangbo, T.K. Attention 3D U-Net with Multiple Skip Connections for Segmentation of Brain Tumor Images. Sensors 2022, 22, 6501. [Google Scholar] [CrossRef] [PubMed]
- Abdusalomov, A.B.; Nasimov, R.; Nasimova, N.; Muminov, B.; Whangbo, T.K. Evaluating Synthetic Medical Images Using Artificial Intelligence with the GAN Algorithm. Sensors 2023, 23, 3440. [Google Scholar] [CrossRef] [PubMed]
- Jakhongir, N.; Abdusalomov, A.; Whangbo, T.K. 3D Volume Reconstruction from MRI Slices based on VTK. In Proceedings of the 2021 International Conference on Information and Communication Technology Convergence (ICTC), Jeju Island, Republic of Korea, 20–22 October 2021; pp. 689–692. [Google Scholar]
- Avazov, K.; Abdusalomov, A.; Mukhiddinov, M.; Baratov, N.; Makhmudov, F.; Cho, Y.I. An improvement for the automatic classification method for ultrasound images used on CNN. Int. J. Wavelets Multiresolut. Inf. Process. 2022, 20, 2150054. [Google Scholar] [CrossRef]
- Umirzakova, S.; Abdusalomov, A.; Whangbo, T.K. Fully Automatic Stroke Symptom Detection Method Based on Facial Features and Moving Hand Differences. In Proceedings of the 2019 International Symposium on Multimedia and Communication Technology (ISMAC), Quezon City, Philippines, 19–21 August 2019; pp. 1–5. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Review Methodology | Details |
|---|---|
| Literature Search |
|
| Inclusion Criteria |
|
| Information Extraction |
|
| Synthesis Approach |
|
| Criteria | Measurements |
|---|---|
| Low Muscle Mass | DXA: <7.0 kg/m in men and <5.4 kg/m in women |
| BIA: <7.0 kg/m in men and <5.7 kg/m in women | |
| DXA (NIH criteria): <0.789 kg/BMI for men and <0.512 kg/BMI for women | |
| Low Muscle Strength | Grip Strength: <28 kg in men and <18 kg in women |
| Low Physical Performance | Gait Speed: ≤0.8 m/s |
| Criteria | Measurements |
|---|---|
| LMM (Low Muscle Mass) | ASM (Appendicular Skeletal Muscle mass) divided by height squared: <7.0 kg/m for men and <5.7 kg/m for women |
| LMS (Low Muscle Strength) | Grip Strength: <27 kg for men and <16 kg for women |
| Low Physical Performance | Gait Speed: <0.8 m/s |
| Study | Dataset Description | Population | Measurements | Key Findings |
|---|---|---|---|---|
| Zhang et al. [82] | West China Health and Aging Trend (WCHAT) | 4057 people aged ≥ 50 | Age, arm circumference, liver enzymes | 12 routine clinical variables could effectively predict sarcopenia status |
| Castillo-Gonzalez et al. [83] | Baja California, Mexico | 166 patients, mean age 77.24 | Medical history, tests, comorbidities, functional capacity, nutrition status, biochemical data, and sociodemographics | The Decision Tree classifier on 5 key variables achieved high accuracy in assessing sarcopenia status and severity |
| Zupo et al. [84] | Clinical records and fluid markers, northern (Pavia) and southern (Apulia) Italy | 1971 adults aged > 65 | Low muscle mass, low muscle strength, and/or low physical performance according to EWGSOP2 guidelines. | Key variables identified include muscle mass, strength, sex, inflammation, and nutritional biomarkers |
| Wu et al. [85] | Tri-Service General Hospital (TSGHIRB 2-108-05-161) | 133 subjects aged 71 years on average | Dynapenia, presarcopenia, and sarcopenia groups based on muscle strength, gait speed, and muscle mass measurements | Effectively discriminate possible sarcopenia subjects based on the noninvasive pulse measurements |
| Carnea et al. [86] | FRADEA (Frailty and Dependence in Albacete) | 200 people aged ≥ 70 | Fat-free mass, gait speed, body mass index, oxidative stress biomarkers, presence of depression, and use of proton pump inhibitors | The multifactorial nature of sarcopenia, with muscle mass, function, and quality as well as systemic factors like inflammation and oxidative stress contributing |
| Kim et al. [87] | Nationwide Korean Frailty and Aging Cohort Study (KFACS) | 2123 community-dwelling older adults aged 70–84 | Handgrip strength, usual gait speed, appendicular skeletal muscle mass | Higher prevalence of sarcopenia under AWGS 2019 definitions compared to AWGS 2014 |
| Santos et al. [36] | Dataset on skeletal muscle mass index, body composition and strength in bariatric patients | 46 bariatric surgery patients aged 18–60 | Skeletal muscle mass index, body composition, strength | Provided a granular view of the impact of bariatric surgery and exercise on sarcopenia risk |
| Sun et al. [88] | 2008 to 2011 Korean National Health and Nutrition Examination Survey | 4937 adults aged 60 and older | Dual-energy X-ray absorptiometry scan | Prevalence of sarcopenia at 6.6%, with men more likely than women |
| Kang et al. [89] | Medical records of Korean postmenopausal women | 4020 postmenopausal women | BMI, BUN, RBC count, dietary factors (water, fibre, protein intake) | Identified significant risk factors for sarcopenia using machine learning algorithms |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turimov Mustapoevich, D.; Kim, W. Machine Learning Applications in Sarcopenia Detection and Management: A Comprehensive Survey. Healthcare 2023, 11, 2483. https://doi.org/10.3390/healthcare11182483
Turimov Mustapoevich D, Kim W. Machine Learning Applications in Sarcopenia Detection and Management: A Comprehensive Survey. Healthcare. 2023; 11(18):2483. https://doi.org/10.3390/healthcare11182483
Chicago/Turabian StyleTurimov Mustapoevich, Dilmurod, and Wooseong Kim. 2023. "Machine Learning Applications in Sarcopenia Detection and Management: A Comprehensive Survey" Healthcare 11, no. 18: 2483. https://doi.org/10.3390/healthcare11182483
APA StyleTurimov Mustapoevich, D., & Kim, W. (2023). Machine Learning Applications in Sarcopenia Detection and Management: A Comprehensive Survey. Healthcare, 11(18), 2483. https://doi.org/10.3390/healthcare11182483