_MD__MPH_PhD.png)

Thirdhand Smoke Knowledge, Beliefs and Behaviors among Parents and Families: A Systematic Review


Abstract
:1. Introduction
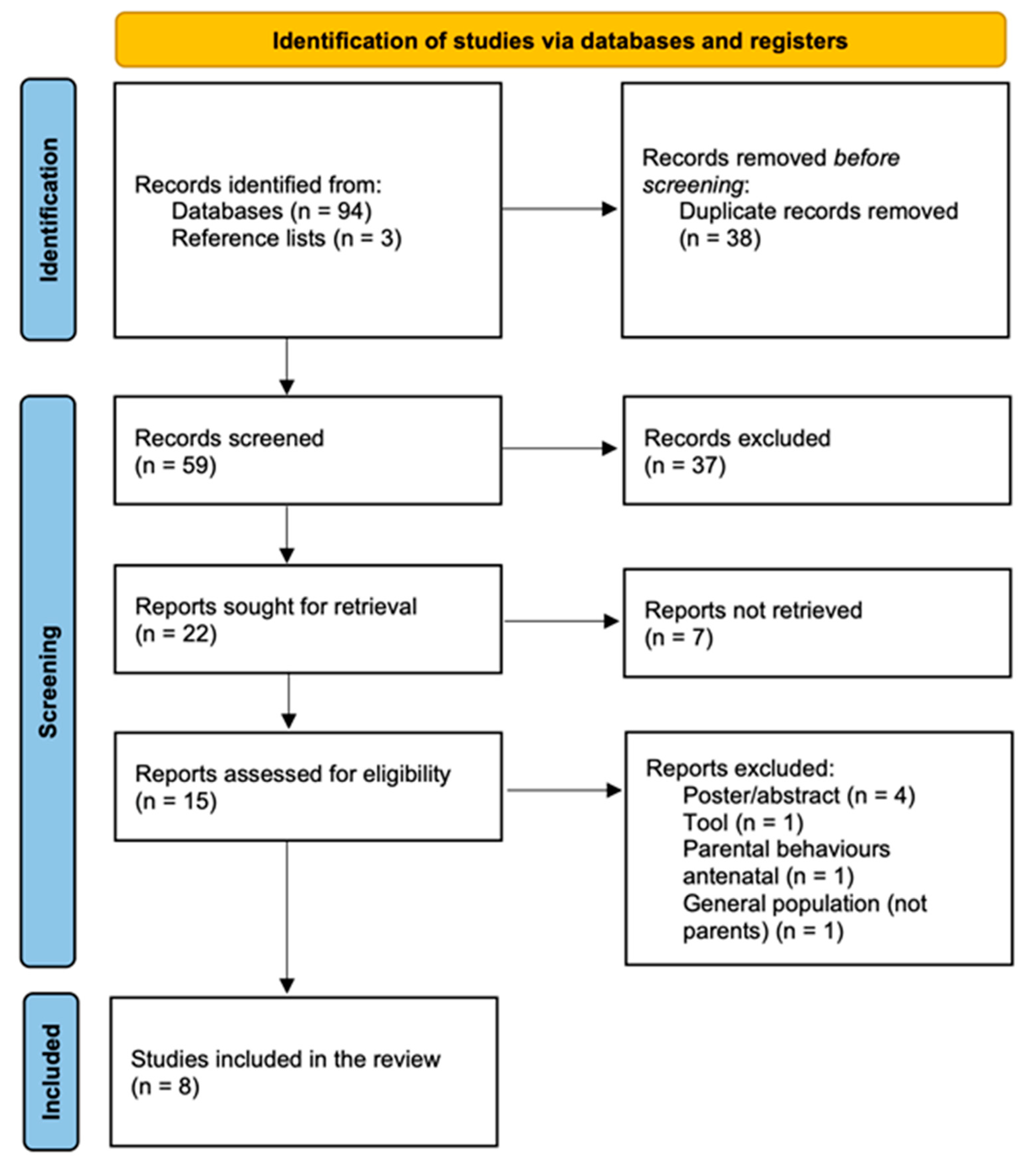
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Makadia, L.D.; Roper, P.J.; Andrews, J.O.; Tingen, M.S. Tobacco Use and Smoke Exposure in Children: New Trends, Harm, and Strategies to Improve Health Outcomes. Curr. Allergy Asthma Rep. 2017, 17, 55. [Google Scholar] [CrossRef] [PubMed]
- Al-Sayed, E.M.; Ibrahim, K.S. Second-Hand Tobacco Smoke and Children. Toxicol. Ind. Health 2014, 30, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Parks, J.; McLean, K.E.; McCandless, L.; de Souza, R.J.; Brook, J.R.; Scott, J.; Turvey, S.E.; Mandhane, P.J.; Becker, A.B.; Azad, M.B.; et al. Assessing Secondhand and Thirdhand Tobacco Smoke Exposure in Canadian Infants Using Questionnaires, Biomarkers, and Machine Learning. J. Expo. Sci. Environ. Epidemiol. 2022, 32, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Acuff, L.; Fristoe, K.; Hamblen, J.; Smith, M.; Chen, J. Third-Hand Smoke: Old Smoke, New Concerns. J. Community Health 2016, 41, 680–687. [Google Scholar] [CrossRef]
- Samet, J.M.; Chanson, D.; Wipfli, H. The Challenges of Limiting Exposure to THS in Vulnerable Populations. Curr. Environ. Health Rep. 2015, 2, 215–225. [Google Scholar] [CrossRef]
- Northrup, T.F.; Jacob, P.; Benowitz, N.L.; Hoh, E.; Quintana, P.J.E.; Hovell, M.F.; Matt, G.E.; Stotts, A.L. Thirdhand Smoke: State of the Science and a Call for Policy Expansion. Public Health Rep. 2016, 131, 233–238. [Google Scholar] [CrossRef]
- Matt, G.E.; Quintana, P.J.E.; Destaillats, H.; Gundel, L.A.; Sleiman, M.; Singer, B.C.; Jacob, P.; Benowitz, N.; Winickoff, J.P.; Rehan, V.; et al. Thirdhand Tobacco Smoke: Emerging Evidence and Arguments for a Multidisciplinary Research Agenda. Environ. Health Perspect. 2011, 119, 1218–1226. [Google Scholar] [CrossRef]
- Jacob, P.; Benowitz, N.L.; Destaillats, H.; Gundel, L.; Hang, B.; Martins-Green, M.; Matt, G.E.; Quintana, P.J.E.; Samet, J.M.; Schick, S.F.; et al. Thirdhand Smoke: New Evidence, Challenges, and Future Directions. Chem. Res. Toxicol. 2017, 30, 270–294. [Google Scholar] [CrossRef]
- Sleiman, M.; Logue, J.M.; Luo, W.; Pankow, J.F.; Gundel, L.A.; Destaillats, H. Inhalable Constituents of Thirdhand Tobacco Smoke: Chemical Characterization and Health Impact Considerations. Environ. Sci. Technol. 2014, 48, 13093–13101. [Google Scholar] [CrossRef]
- Martins-Green, M.; Adhami, N.; Frankos, M.; Valdez, M.; Goodwin, B.; Lyubovitsky, J.; Dhall, S.; Garcia, M.; Egiebor, I.; Martinez, B.; et al. Cigarette Smoke Toxins Deposited on Surfaces: Implications for Human Health. PLoS ONE 2014, 9, e86391. [Google Scholar] [CrossRef]
- Kuo, H.-W.; Rees, V.W. Third-Hand Smoke (THS): What Is It and What Should We Do about It? J. Formos. Med. Assoc. 2019, 118, 1478–1479. [Google Scholar] [CrossRef] [PubMed]
- Snijders, A.M.; Zhou, M.; Whitehead, T.P.; Fitch, B.; Pandey, P.; Hechmer, A.; Huang, A.; Schick, S.F.; de Smith, A.J.; Olshen, A.B.; et al. In Utero and Early-Life Exposure to Thirdhand Smoke Causes Profound Changes to the Immune System. Clin. Sci. 2021, 135, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Karim, Z.A.; Alshbool, F.Z.; Vemana, H.P.; Adhami, N.; Dhall, S.; Espinosa, E.V.P.; Martins-Green, M.; Khasawneh, F.T. Third-Hand Smoke: Impact on Hemostasis and Thrombogenesis. J. Cardiovasc. Pharmacol. 2015, 66, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.E.A.; Alarabi, A.B.; Karim, Z.A.; Rodriguez, V.; Hernandez, K.R.; Lozano, P.A.; El-Halawany, M.S.; Alshbool, F.Z.; Khasawneh, F.T. In Utero Thirdhand Smoke Exposure Modulates Platelet Function in a Sex-Dependent Manner. Haematologica 2021, 107, 312–315. [Google Scholar] [CrossRef]
- Ferrante, G.; Simoni, M.; Cibella, F.; Ferrara, F.; Liotta, G.; Malizia, V.; Corsello, G.; Viegi, G.; La Grutta, S. Third-Hand Smoke Exposure and Health Hazards in Children. Monaldi Arch. Chest Dis. 2015, 79, 38–43. [Google Scholar] [CrossRef]
- McGrath-Morrow, S.A.; Gorzkowski, J.; Groner, J.A.; Rule, A.M.; Wilson, K.; Tanski, S.E.; Collaco, J.M.; Klein, J.D. The Effects of Nicotine on Development. Pediatrics 2020, 145, e20191346. [Google Scholar] [CrossRef]
- Patel, S.; Hendry, P.; Kalynych, C.; Butterfield, R.; Lott, M.; Lukens-Bull, K. The Impact of Third-Hand Smoke Education in a Pediatric Emergency Department on Caregiver Smoking Policies and Quit Status: A Pilot Study. Int. J. Disabil. Hum. Dev. 2012, 11, 335–342. [Google Scholar] [CrossRef]
- Xie, Z.; Chen, M.; Fu, Z.; He, Y.; Tian, Y.; Zhang, X.; Feng, N. Thirdhand Smoke Beliefs and Behaviors among Families Ofprimary School Children in Shanghai. Tob. Induc. Dis. 2021, 19, 10. [Google Scholar] [CrossRef]
- Oktar, D.; Ozcan, L.; Onsuz, M.; Metintas, S. Parental Beliefs on the Harmfull Effects of Third Hand Smoke: Systematic Review and Meta-Analysis. Eur. J. Public Health 2021, 31, ckab165.247. [Google Scholar] [CrossRef]
- Mahabee-Gittens, E.M.; Merianos, A.L.; Hoh, E.; Quintana, P.J.; Matt, G.E. Nicotine on Children’s Hands: Limited Protection of Smoking Bans and Initial Clinical Findings. Tob. Use Insights 2019, 12, 1179173X1882349. [Google Scholar] [CrossRef]
- Mahabee-Gittens, E.M.; Matt, G.E.; Jandarov, R.J.; Merianos, A.L. Hand Nicotine and Cotinine In Children Exposed to Cigars: A Pilot Study. Tob. Regul. Sci. 2021, 7, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Munn, Z. (Eds.) JBI Manual for Evidence Synthesis; JBI: North Adelaide, Australia, 2020; ISBN 978-0-648-84880-6. [Google Scholar]
- Barker, T.H.; Stone, J.C.; Sears, K.; Klugar, M.; Leonardi-Bee, J.; Tufanaru, C.; Aromataris, E.; Munn, Z. Revising the JBI Quantitative Critical Appraisal Tools to Improve Their Applicability: An Overview of Methods and the Development Process. JBI Evid. Synth. 2023, 21, 478–493. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Drehmer, J.E.; Ossip, D.J.; Nabi-Burza, E.; Rigotti, N.A.; Hipple, B.; Woo, H.; Chang, Y.; Winickoff, J.P. Thirdhand Smoke Beliefs of Parents. Pediatrics 2014, 133, e850–e856. [Google Scholar] [CrossRef] [PubMed]
- Díez-Izquierdo, A.; Cassanello, P.; Cartanyà, A.; Matilla-Santander, N.; Balaguer Santamaria, A.; Martinez-Sanchez, J.M. Knowledge and Attitudes toward Thirdhand Smoke among Parents with Children under 3 Years in Spain. Pediatr. Res. 2018, 84, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Baheiraei, A.; Shirazi, M.G.; Raisi Dehkordi, Z.; Nejat, S. Prevalence of Home Smoking Bans and Its Determinants in Families with Infants. IJP Int. J. Pediatr. 2018, 6, 6987–6997. [Google Scholar] [CrossRef]
- Dai, S.; Au, C.T.; Chan, M.H.M.; Kam, R.K.T.; Li, A.M.; Chan, K.C.-C. Parental Knowledge, Attitude, and Practice on Tobacco Use, Smoking Cessation, and Children’s Environmental Tobacco Smoke Exposure. Front. Public Health 2021, 9, 733667. [Google Scholar] [CrossRef]
- Myers Gamliel, V.; Shiloh, S.; Zucker, D.M.; Rosen, L. Changing Exposure Perceptions: A Randomized Controlled Trial of an Intervention with Smoking Parents. Int. J. Environ. Res. Public Health 2020, 17, 3349. [Google Scholar] [CrossRef]
- Shehab, K.; Ziyab, A. Beliefs of Parents in Kuwait about Thirdhand Smoke and Its Relation to Home Smoking Rules: A Cross-Sectional Study. Tob. Induc. Dis. 2021, 19, 66. [Google Scholar] [CrossRef]
- Haardörfer, R.; Berg, C.J.; Escoffery, C.; Bundy, Ł.T.; Hovell, M.; Kegler, M.C. Development of a Scale Assessing Beliefs About ThirdHand Smoke (BATHS). Tob. Induc. Dis. 2017, 15, 4. [Google Scholar] [CrossRef]
- Jeonghoon, K.; Jin-Ha, Y.; Jihyun, K.; Wanhyung, L.; Yeong-Kwang, K.; Seunghyun, L.; KyooSang, K. Factors Associated with Beliefs among Adults in Korea about the Health Effects of Thirdhand Smoke on Children. J. Environ. Health Sci. 2018, 44, 90–97. [Google Scholar] [CrossRef]
- Winickoff, J.P.; Friebely, J.; Tanski, S.E.; Sherrod, C.; Matt, G.E.; Hovell, M.F.; McMillen, R.C. Beliefs About the Health Effects of “Thirdhand” Smoke and Home Smoking Bans. Pediatrics 2009, 123, e74–e79. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, C.; Souza, P.; Zorzan, A.; Bastos, B.; Bernhardt, T.; Wiese, B.; Bernhardt, P. Second and Third- Hand Smoke: Public Perceptions of the Risks for Children’s Health. Allergy 2019, 74, 882. [Google Scholar] [CrossRef]
- Roberts, C.; Wagler, G.; Carr, M.M. Environmental Tobacco Smoke: Public Perception of Risks of Exposing Children to Second- and Third-Hand Tobacco Smoke. J. Pediatr. Health Care 2016, 31, e7–e13. [Google Scholar] [CrossRef] [PubMed]
- Myers Gamliel, V.; Shiloh, S.; Rosen, L. Parental Perceptions of Exposure to Tobacco Smoke: A New Tool to Shed Light on Parental Smoking Behaviour. Tob. Induc. Dis. 2018, 16, 147. [Google Scholar] [CrossRef]
- Myers Gamliel, V.; Shiloh, S.; Rosen, L. Parental Perceptions of Children’s Exposure to Tobacco Smoke: Development and Validation of a New Measure. BMC Public Health 2018, 18, 1031. [Google Scholar] [CrossRef]
- Öberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide Burden of Disease from Exposure to Second-Hand Smoke: A Retrospective Analysis of Data from 192 Countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]

{kind=link}
| Authors | Country | Design | Population and Sample Size | Tool | Main Findings | JBI Critical Appraisal Score |
|---|---|---|---|---|---|---|
| Patel et al., 2012 [17] | USA | Pilot study | 40 caregivers (18 control–22 intervention group) | Self-report questionnaire | A total of 75% of parents recognized the negative impact of THS * on their child’s health. A brief THS * intervention influenced smokers to change smoking behaviors. | 6/13 |
| Drehmer et al., 2014 [25] | USA | Pre–post intervention study | 1980 parents | Pre–post survey + computer-aided telephone interview | The belief in the harmful effects of THS * was linked to a tightly enforced ban on smoking in the home and car, as well as efforts to quit smoking. Educating parents could contribute to positive results in controlling tobacco use | 6/13 |
| Díez-Izquierdo et al., 2018 [26] | Spain | Cross-sectional | 1406 parents with children between 3 and 36 months old | Online survey | A total of 80% of parents held the belief that exposing their children to THS * can be detrimental, and among participants with advanced levels of education, this percentage reached 90%. | 5/8 |
| Baheiraei et al., 2018 [27] | Iran | Cross-sectional | 1112 families of infants aged 1 year or younger | Questionnaires and face-to-face interviews | Almost half of parents completely agreed with the effects of THS * exposure on their infant’s health. | 5/8 |
| Myers Gamliel et al., 2020 [29] | Israel | RCT *** | 159 families of children <8 years old randomized into 3 groups | 23-item PPE **** online questionnaire | Parental perceptions of exposure were increased significantly post-intervention, indicating that they can be altered. | 7/13 |
| Shehab and Ziyab, 2021 [30] | Kuwait | Cross-sectional | 536 parents with at least one child aged <18 years | Web-based survey incl. BATHS ***** scale | Parents’ harm and persistence beliefs about THS * were associated with enforcing a strict home smoking ban. | 4/8 |
| Xie et al., 2021 [18] | China | Cross-sectional | 843 parents and grandparents of children aged 6–13 years | Paper-based survey incl. BATHS ***** scale (Chinese version) | Younger people with higher education levels obtained higher scores. | 4/8 |
| Dai et al., 2021 [28] | China | Cross-sectional | 145 parents of children with median age of 2.7 (1.2–6.3) years | Standardized questionnaire + KAP ** questionnaire | Discrepancy between knowledge and good practice related to THS *. | 6/8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanzi, V.; Marti, F.; Cattaruzza, M.S. Thirdhand Smoke Knowledge, Beliefs and Behaviors among Parents and Families: A Systematic Review. Healthcare 2023, 11, 2403. https://doi.org/10.3390/healthcare11172403
Vanzi V, Marti F, Cattaruzza MS. Thirdhand Smoke Knowledge, Beliefs and Behaviors among Parents and Families: A Systematic Review. Healthcare. 2023; 11(17):2403. https://doi.org/10.3390/healthcare11172403
Chicago/Turabian StyleVanzi, Valentina, Flavio Marti, and Maria Sofia Cattaruzza. 2023. "Thirdhand Smoke Knowledge, Beliefs and Behaviors among Parents and Families: A Systematic Review" Healthcare 11, no. 17: 2403. https://doi.org/10.3390/healthcare11172403
APA StyleVanzi, V., Marti, F., & Cattaruzza, M. S. (2023). Thirdhand Smoke Knowledge, Beliefs and Behaviors among Parents and Families: A Systematic Review. Healthcare, 11(17), 2403. https://doi.org/10.3390/healthcare11172403