


The Effectiveness of a Smartphone Application for Tinnitus Relief

Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Procedures
2.3. Hearing and Tinnitus Assessment
2.4. Stress Assessment
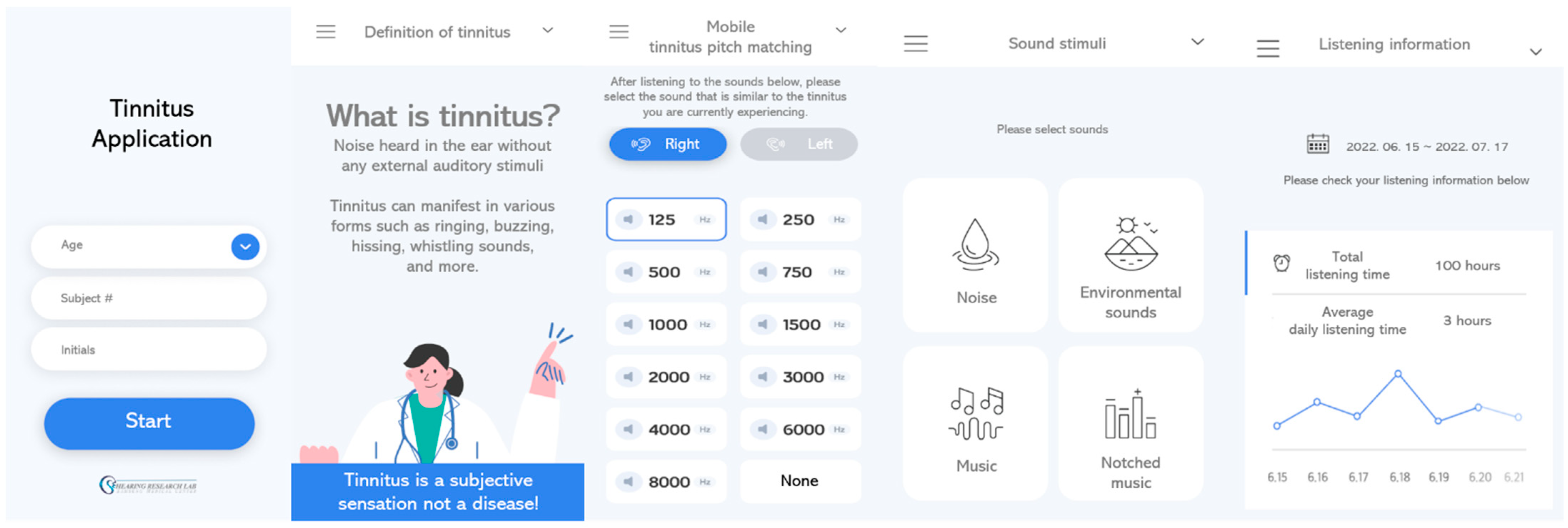
2.5. Tinnitus Relief through a Smartphone Application
2.6. Questionnaire
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Tinnitus Characteristics
3.3. Stress
3.4. Questionnaires
3.5. Sound Preference
3.6. Tinnitus Application Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jastreboff, P.J. Phantom auditory perception (tinnitus): Mechanisms of generation and perception. Neurosci. Res. 1990, 8, 221–254. [Google Scholar] [CrossRef] [PubMed]
- Mavrogeni, P.; Maihoub, S.; Tamás, L.; Molnár, A. Tinnitus characteristics and associated variables on Tinnitus Handicap Inventory among a Hungarian population. J. Otol. 2022, 17, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Szibor, A.; Makitie, A.; Aarnisalo, A.A. Tinnitus and suicide: An unresolved relation. Audiol. Res. 2019, 9, 222. [Google Scholar] [CrossRef] [PubMed]
- Lugo, A.; Trpchevska, N.; Liu, X.; Biswas, R.; Magnusson, C.; Gallus, S.; Cederroth, C.R. Sex-Specific Association of Tinnitus with Suicide Attempts. JAMA Otolaryngol.—Head Neck Surg. 2019, 145, 685–687. [Google Scholar] [CrossRef] [PubMed]
- Molnár, A.; Mavrogeni, P.; Tamás, L.; Maihoub, S. Correlation between Tinnitus Handicap and Depression and Anxiety Scores. Ear Nose Throat J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.M.; Han, K.D.; Kong, S.K.; Nam, E.C.; Park, S.N.; Shim, H.J.; Byun, J.Y.; Park, H.J.; Im, G.J.; Lee, I.W. Epidemiology of Clinically Significant Tinnitus: A 10-Year Trend from Nationwide Health Claims Data in South Korea. Otol. Neurotol. 2018, 39, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, J.M.; Lin, H.W.; Bhattacharyya, N. Prevalence, severity, exposures, and treatment patterns of tinnitus in the United States. JAMA Otolaryngol.–Head Neck Surg. 2016, 142, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.; Cooke, B.; Eitutis, S.; Simpson, M.T.W.; Beyea, J.A. Approach to tinnitus management. Can. Fam. Physician 2018, 64, 491–495. [Google Scholar]
- Surr, R.K.; Montgomery, A.A.; Mueller, H.G. Effect of amplification on tinnitus among new hearing aid users. Ear Hear. 1985, 6, 71–75. [Google Scholar] [CrossRef]
- Elgoyhen, A.B.; Langguth, B. Pharmacological approaches to the treatment of tinnitus. Drug Discov. Today 2010, 15, 300–305. [Google Scholar] [CrossRef]
- Folmer, R.L.; Carroll, J.R. Long-term effectiveness of ear-level devices for tinnitus. Otolaryngol. Head Neck Surg. 2006, 134, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Nagaraj, M.K.; Prabhu, P. Internet/smartphone-based applications for the treatment of tinnitus: A systematic review. Eur. Arch. Otorhinolaryngol. 2020, 277, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Kleinjung, T.; Langguth, B. Avenue for future tinnitus treatments. Otolaryngol. Clin. North Am. 2020, 53, 667–683. [Google Scholar] [CrossRef]
- Mehdi, M.; Stach, M.; Riha, C.; Neff, P.; Dode, A.; Pryss, R.; Schlee, W.; Reichert, M.; Hauck, F.J. Smartphone and Mobile Health Apps for Tinnitus: Systematic Identification, Analysis, and Assessment. JMIR Mhealth Uhealth 2020, 8, e21767. [Google Scholar] [CrossRef] [PubMed]
- Kutyba, J.; Gos, E.; Jedrzejczak, W.W.; Raj-Koziak, D.; Karpiesz, L.; Niedzialek, I.; Skarzynski, H.; Skarzynski, P.H. Effectiveness of tinnitus therapy using a mobile application. Eur. Arch. Otorhinolaryngol. 2022, 279, 1257–1267. [Google Scholar] [CrossRef] [PubMed]
- Engelke, M.; Simoes, J.; Vogel, C.; Schoisswohl, S.; Schecklmann, M.; Wolflick, S.; Pryss, R.; Probst, T.; Langguth, B.; Schlee, W. Pilot study of a smartphone-based tinnitus therapy using structured counseling and sound therapy: A multiple-baseline design with ecological momentary assessment. PLOS Digit. Health 2023, 2, e0000183. [Google Scholar] [CrossRef] [PubMed]
- Mehdi, M.; Riha, C.; Neff, P.; Dode, A.; Pryss, R.; Schlee, W.; Reichert, M.; Hauck, F.J. Smartphone Apps in the Context of Tinnitus: Systematic Review. Sensors 2020, 20, 1725. [Google Scholar] [CrossRef]
- Searchfield, G.D.; Durai, M.; Linford, T. A State-of-the-Art Review: Personalization of Tinnitus Sound Therapy. Front. Psychol. 2017, 8, 1599. [Google Scholar] [CrossRef]
- Weise, C.; Kleinstauber, M.; Andersson, G. Internet-Delivered Cognitive-Behavior Therapy for Tinnitus: A Randomized Controlled Trial. Psychosom. Med. 2016, 78, 501–510. [Google Scholar] [CrossRef]
- Wilson, M.B.; Kallogjeri, D.; Joplin, C.N.; Gorman, M.D.; Krings, J.G.; Lenze, E.J.; Nicklaus, J.E.; Spitznagel, E.E., Jr.; Piccirillo, J.F. Ecological momentary assessment of tinnitus using smartphone technology: A pilot study. Otolaryngol. Head Neck Surg. 2015, 152, 897–903. [Google Scholar] [CrossRef]
- Casale, M.; Costantino, A.; Rinaldi, V.; Forte, A.; Grimaldi, M.; Sabatino, L.; Oliveto, G.; Aloise, F.; Pontari, D.; Salvinelli, F. Mobile applications in otolaryngology for patients: An update. Laryngoscope Investig. Otolaryngol. 2018, 3, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, S.Y.; Kim, C.H.; Lim, S.L.; Shin, J.N.; Chung, W.H.; Yu, B.H.; Hong, S.H. Reliability and validity of a Korean adaptation of the Tinnitus Handicap Inventory. Korean J. Otorhinolaryngol.-Head Neck Surg. 2002, 45, 328–334. [Google Scholar]
- Lee, Y. A study of the reliability and the validity of the BDI, SDS, and MMPI-D scales. Korean J. Clin. Psychol. 1991, 10, 98–113. [Google Scholar]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Seol, H.Y.; Kim, G.Y.; Jo, M.; Kang, S.; Cho, Y.S.; Hong, S.H.; Moon, I.J. Content validity of the tinnitus outcome questionnaire for sound management. PLoS ONE 2021, 16, e0251244. [Google Scholar] [CrossRef] [PubMed]
- Sereda, M.; Stockdale, D.; Newton, K.; Smith, S. Mobile applications for management of tinnitus. J. Hear. Sci. 2017, 7, 124–125. [Google Scholar]
- Kutyba, J.J.; Jedrzejczak, W.W.; Gos, E.; Raj-Koziak, D.; Skarzynski, P.H. Chronic Tinnitus and the Positive Effects of Sound Treatment via a Smartphone App: Mixed-Design Study. JMIR Mhealth Uhealth 2022, 10, e33543. [Google Scholar] [CrossRef]
- Wallhäußer-Franke, E.; Brade, J.; Balkenhol, T.; D’Amelio, R.; Seegmüller, A.; Delb, W. Tinnitus: Distinguishing between subjectively perceived loudness and tinnitus-related distress. PLoS ONE 2012, 7, e34583. [Google Scholar] [CrossRef]
- Baigi, A.; Oden, A.; Almlid-Larsen, V.; Barrenäs, M.-L.; Holgers, K.-M. Tinnitus in the general population with a focus on noise and stress: A public health study. Ear Hear. 2011, 32, 787–789. [Google Scholar] [CrossRef]
- Mckenna, L.; Irwin, R. Sound therapy for tinnitus–sacred cow or idol worship?: An investigation of the evidence. Audiol. Med. 2008, 6, 16–24. [Google Scholar] [CrossRef]
- Hobson, J.; Chisholm, E.; El Refaie, A. Sound therapy (masking) in the management of tinnitus in adults. Cochrane Database Syst. Rev. 2012, 11, CD006371. [Google Scholar] [CrossRef]
- Shekhawat, G.S.; Searchfield, G.D.; Stinear, C.M. Randomized Trial of Transcranial Direct Current Stimulation and Hearing Aids for Tinnitus Management. Neurorehabilit. Neural Repair 2014, 28, 410–419. [Google Scholar] [CrossRef]
- De Ridder, D.; Kilgard, M.; Engineer, N.; Vanneste, S. Placebo-controlled vagus nerve stimulation paired with tones in a patient with refractory tinnitus: A case report. Otol. Neurotol. 2015, 36, 575–580. [Google Scholar] [CrossRef]
- Bommakanti, K.K.; Smith, L.L.; Liu, L.; Do, D.; Cuevas-Mota, J.; Collins, K.; Munoz, F.; Rodwell, T.C.; Garfein, R.S. Requiring smartphone ownership for mHealth interventions: Who could be left out? BMC Public Health 2020, 20, 81. [Google Scholar] [CrossRef]

{kind=link}
| Laterality | 8 (Unilateral), 14 (Bilateral) |
|---|---|
| Duration (months) | 75.1 (SD = 71.1) |
| Onset | 17 (sudden), 5 (gradual) |
| Frequency | 7 (low), 6 (mid), 9 (high) |
| Loudness | 35.7 dB (SD = 21.6) |
| Sound | 2 (buzzing), 13 (pure tone), 5 (noise), 2 (other) |
| Consistency | 11 (consistent), 11 (fluctuating) |
| Subjective loudness | 4.9 (SD = 1.9) |
| Subjective annoyance | 5.4 (SD = 2.6) |
| Questionnaire | Mean Scores (SD) | p | ||
|---|---|---|---|---|
| Visit 1 | Visit 2 | Visit 3 | ||
| BDI | 8.0 (4.8) | 6.4 (4.1) | 5.7 (5.4) | 0.123 |
| THI | 33.2 (20.8) | 29.4 (18.0) | 24.8 (19.3) | 0.024 * |
| Variable | Mean Scores (SD) | p | ||
|---|---|---|---|---|
| Visit 1 | Visit 2 | Visit 3 | ||
| Loudness | 4.9 (1.9) | 4.4 (2.1) | 4.0 (2.1) | 0.041 * |
| Annoyance | 5.4 (2.6) | 4.6 (2.8) | 3.6 (2.4) | <0.001 ** |
| Visit | Preference Ranking | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| 2 | Music | Environmental sound | Notched music | Noise |
| 3 | Environmental sound | Music | Notched music | Noise |
| Domain | Question | Average Score |
|---|---|---|
| Accessibility | Was the application easy to use? | 4.5 |
| Was it easy to understand the information in the application? | 4.2 | |
| Efficiency | Was it easy to switch between menus? | 4.1 |
| Was the application running stably? | 4.2 | |
| Design | Was the design of the application appropriate? | 3.9 |
| Were the text size and color appropriate? | 4.0 | |
| Was the icon size appropriate? | 4.0 | |
| Satisfaction | Overall, were you satisfied with the application? | 4.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seol, H.Y.; Jo, M.; Moon, I.J. The Effectiveness of a Smartphone Application for Tinnitus Relief. Healthcare 2023, 11, 2368. https://doi.org/10.3390/healthcare11172368
Seol HY, Jo M, Moon IJ. The Effectiveness of a Smartphone Application for Tinnitus Relief. Healthcare. 2023; 11(17):2368. https://doi.org/10.3390/healthcare11172368
Chicago/Turabian StyleSeol, Hye Yoon, Mini Jo, and Il Joon Moon. 2023. "The Effectiveness of a Smartphone Application for Tinnitus Relief" Healthcare 11, no. 17: 2368. https://doi.org/10.3390/healthcare11172368
APA StyleSeol, H. Y., Jo, M., & Moon, I. J. (2023). The Effectiveness of a Smartphone Application for Tinnitus Relief. Healthcare, 11(17), 2368. https://doi.org/10.3390/healthcare11172368