
Associations between Degenerative Lumbar Scoliosis Structures and Pain Distribution in Adults with Chronic Low Back Pain


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethics and Consent Forms
2.3. Eligibility
2.4. Participants
2.5. Assessment of Scoliosis
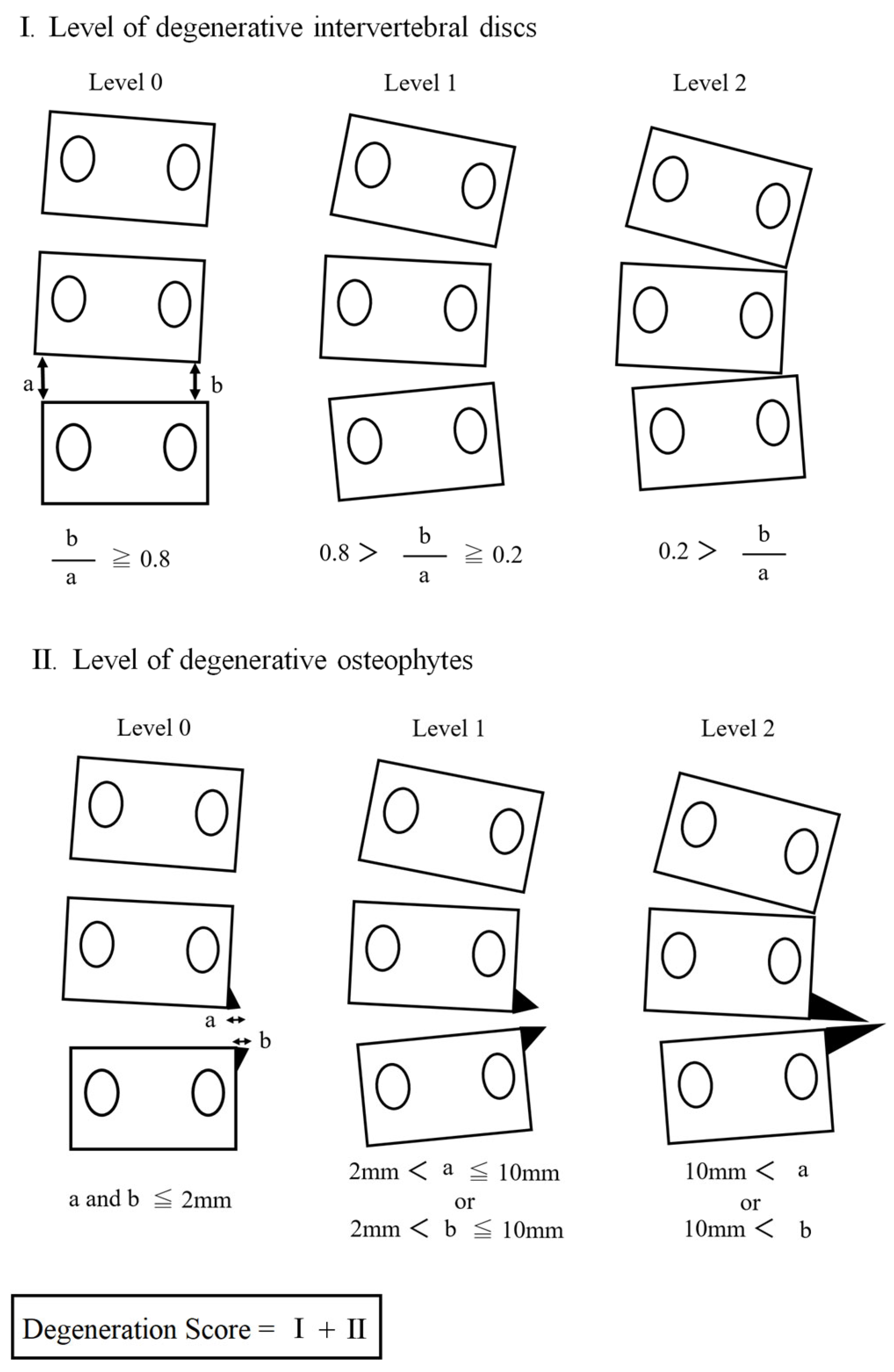
2.6. Assessment of Degeneration
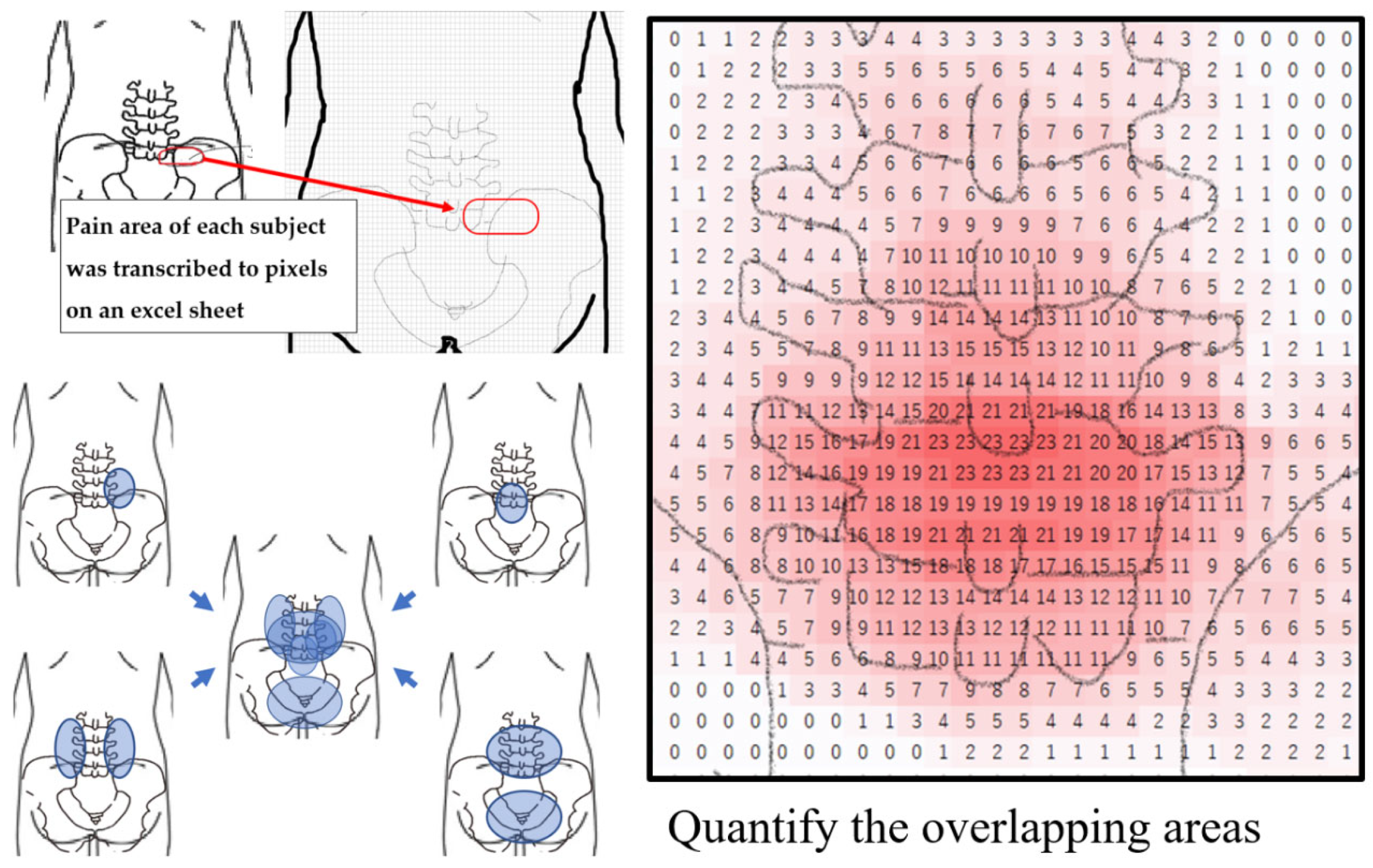
2.7. Assessment of Pain
2.8. Sample Size
2.9. Statistics
3. Results
3.1. Characteristics of the Participants
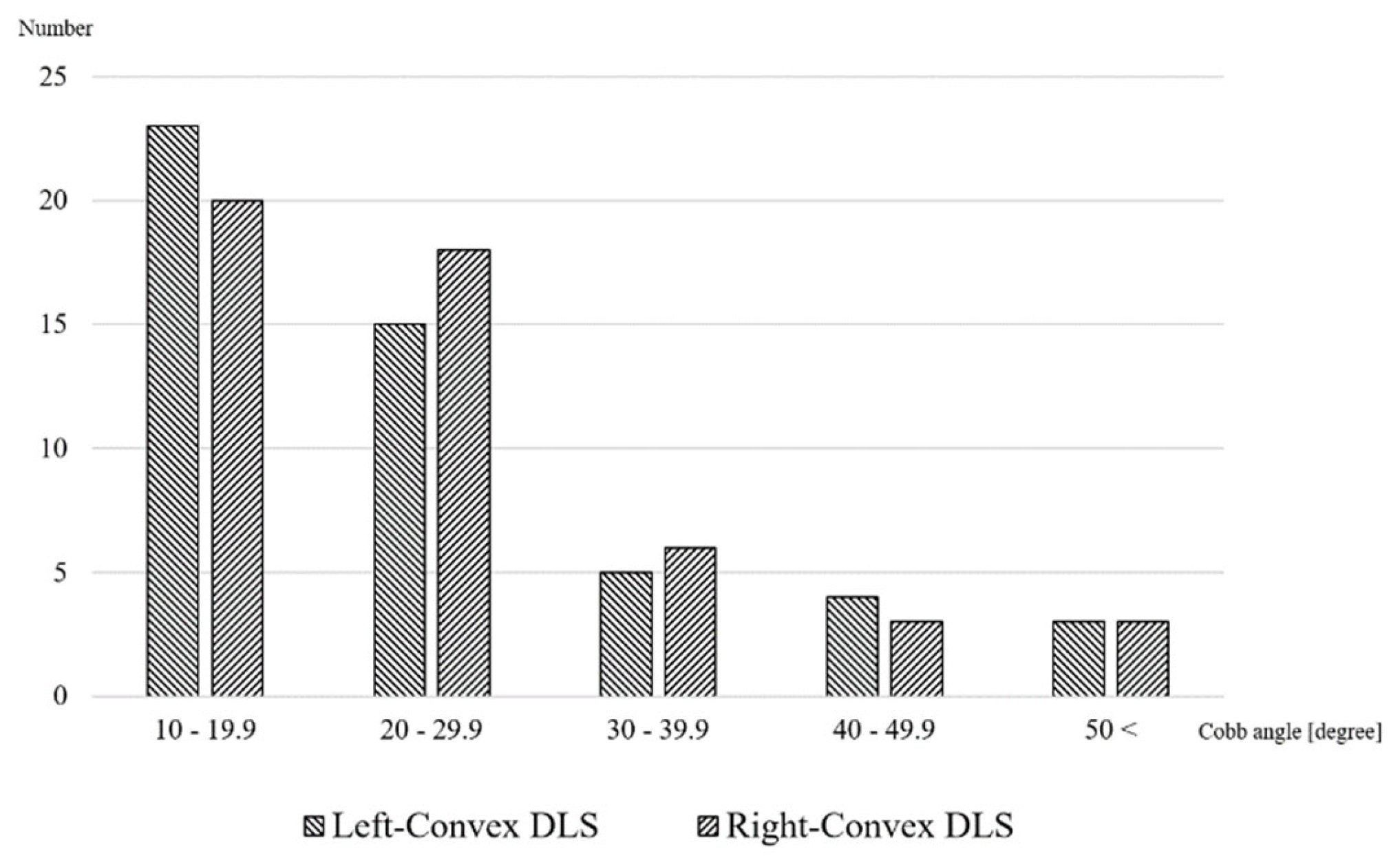
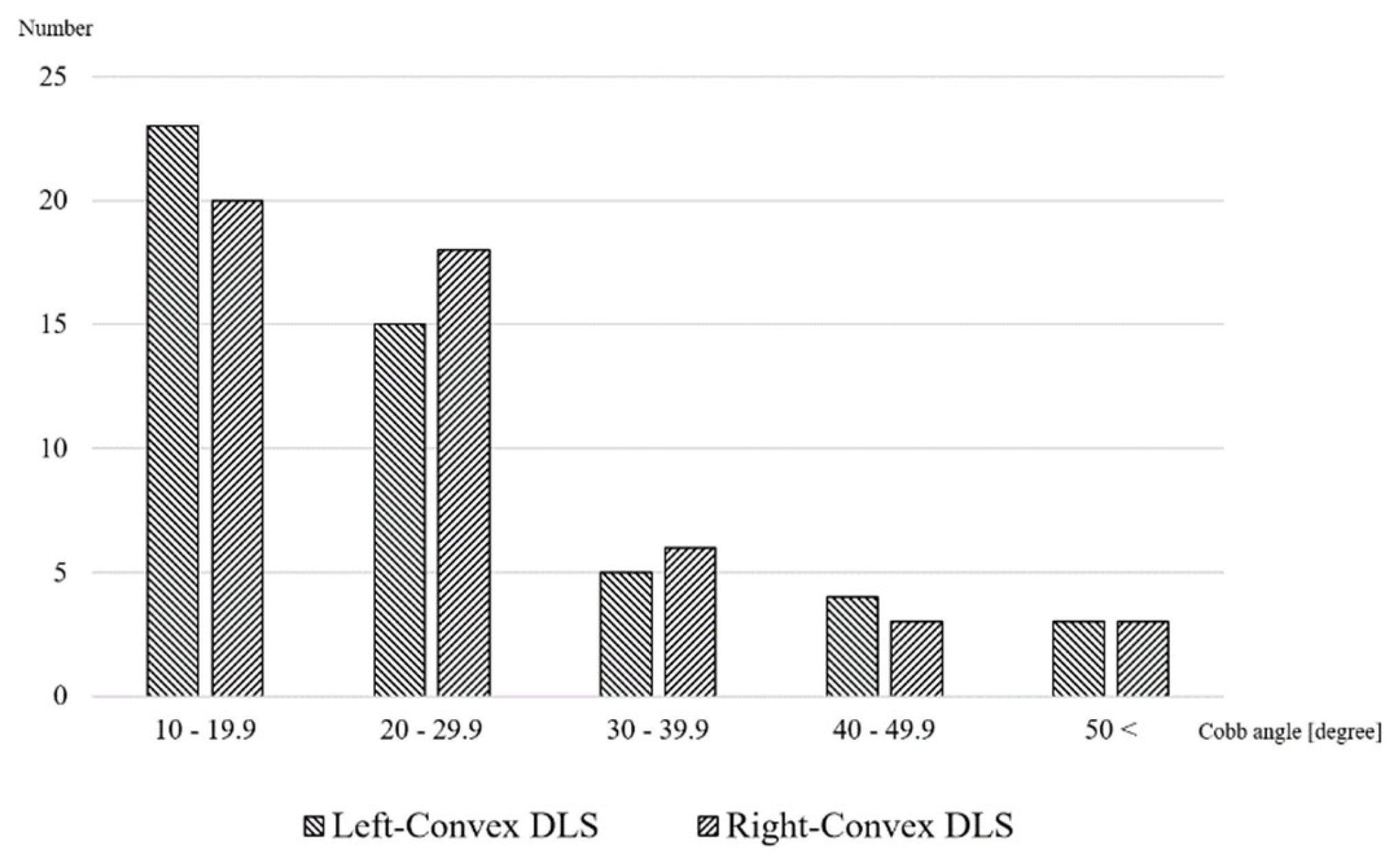
3.2. Radiographic Parameter, Pain Locations and Distributions in the Participants
3.3. Predictors for Pain Intensity or Area
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kotwal, S.; Pumberger, M.; Hughes, A.; Girardi, F. Degenerative scoliosis: A review. HSS J. 2011, 7, 257–264. [Google Scholar] [CrossRef] [PubMed]
- York, P.J.; Kim, H.J. Degenerative Scoliosis. Curr. Rev. Musculoskelet. Med. 2017, 10, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Pizones, J.; Pérez Martin-Buitrago, M.; Perez-Grueso, F.J.S.; Vila-Casademunt, A.; Alanay, A.; Obeid, I.; Kleinstück, F.; Acaroglu, E.R.; Pellisé, F. Function and Clinical Symptoms are the Main Factors that Motivate Thoracolumbar Adult Scoliosis Patients to Pursue Surgery. Spine 2017, 42, E31–E36. [Google Scholar] [CrossRef] [PubMed]
- Aebi, M. The adult scoliosis. Eur. Spine J. 2005, 14, 925–948. [Google Scholar] [CrossRef]
- Kelly, A.; Younus, A.; Lekgwara, P. Adult degenerative scoliosis—A literature review. Interdiscip. Neurosurg. 2020, 20, 100661. [Google Scholar] [CrossRef]
- Glassman, S.D.; Berven, S.; Bridwell, K.; Horton, W.; Dimar, J.R. Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine 2005, 30, 682–688. [Google Scholar] [CrossRef]
- Glassman, S.D.; Schwab, F.J.; Bridwell, K.H.; Ondra, S.L.; Berven, S.; Lenke, L.G. The selection of operative versus nonoperative treatment in patients with adult scoliosis. Spine 2007, 32, 93–97. [Google Scholar] [CrossRef]
- Smith, J.S.; Shaffrey, C.I.; Berven, S.; Glassman, S.; Hamill, C.; Horton, W.; Ondra, S.; Schwab, F.; Shainline, M.; Fu, K.-M.; et al. Improvement of back pain with operative and nonoperative treatment in adults with scoliosis. Neurosurgery 2009, 65, 86–93; discussion 93–94. [Google Scholar] [CrossRef]
- Robin, G.C.; Span, Y.; Steinberg, R.; Makin, M.; Menczel, J. Scoliosis in the elderly: A follow-up study. Spine 1982, 7, 355–359. [Google Scholar] [CrossRef]
- Schwab, F.; Dubey, A.; Gamez, L.; El Fegoun, A.B.; Hwang, K.; Pagala, M.; Farcy, J.P. Adult scoliosis: Prevalence, SF-36, and nutritional parameters in an elderly volunteer population. Spine 2005, 30, 1082–1085. [Google Scholar] [CrossRef]
- Winter, R.B.; Lonstein, J.E.; Denis, F. Pain patterns in adult scoliosis. Orthop. Clin. N. Am. 1988, 19, 339–345. [Google Scholar] [CrossRef]
- Ploumis, A.; Transfledt, E.E.; Denis, F. Degenerative lumbar scoliosis associated with spinal stenosis. Spine J. 2007, 7, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.; Saifuddin, A. Imaging of painful scoliosis. Skelet. Radiol. 2009, 38, 207–223. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, B.; Chen, S.; Lu, X.; Li, Z.-Y.; Guo, Q. A Validated Finite Element Analysis of Facet Joint Stress in Degenerative Lumbar Scoliosis. World Neurosurg. 2016, 95, 126–133. [Google Scholar] [CrossRef]
- de Vries, A.A.B.; Mullender, M.G.; Pluymakers, W.J.; Castelein, R.M.; van Royen, B.J. Spinal decompensation in degenerative lumbar scoliosis. Eur. Spine J. 2010, 19, 1540–1544. [Google Scholar] [CrossRef]
- Poulsen, E.; Overgaard, S.; Vestergaard, J.T.; Christensen, H.W.; Hartvigsen, J. Pain distribution in primary care patients with hip osteoarthritis. Fam. Pract. 2016, 33, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Lluch Girbés, E.; Dueñas, L.; Barbero, M.; Falla, D.; Baert, I.A.C.; Meeus, M.; Sánchez-Frutos, J.; Aguilella, L.; Nijs, J. Expanded Distribution of Pain as a Sign of Central Sensitization in Individuals With Symptomatic Knee Osteoarthritis. Phys. Ther. 2016, 96, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Ohnmeiss, D.D. Repeatability of pain drawings in a low back pain population. Spine 2000, 25, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Barbero, M.; Moresi, F.; Leoni, D.; Gatti, R.; Egloff, M.; Falla, D. Test-retest reliability of pain extent and pain location using a novel method for pain drawing analysis. Eur. J. Pain 2015, 19, 1129–1138. [Google Scholar] [CrossRef]
- Margolis, R.B.; Tait, R.C.; Krause, S.J. A rating system for use with patient pain drawings. Pain 1986, 24, 57–65. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Bull. World Health Organ. 2007, 85, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Vellinga, A.; Cormican, M.; Hanahoe, B.; Bennett, K.; Murphy, A.W. Opt-out as an acceptable method of obtaining consent in medical research: A short report. BMC Med. Res. Methodol. 2011, 11, 40. [Google Scholar] [CrossRef]
- Lowe, T.; Berven, S.H.; Schwab, F.J.; Bridwell, K.H. The SRS classification for adult spinal deformity: Building on the King/Moe and Lenke classification systems. Spine 2006, 31 (Suppl. 19), S119–S125. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Bao, H.; Yan, P.; Liu, S.; Bao, M.; Zhu, Z.; Qiu, Y. Do the disc degeneration and osteophyte contribute to the curve rigidity of degenerative scoliosis? BMC Musculoskelet. Disord. 2017, 18, 128. [Google Scholar] [CrossRef]
- Riley, J.L., 3rd; Robinson, M.E.; Wise, E.A.; Myers, C.D.; Fillingim, R.B. Sex differences in the perception of noxious experimental stimuli: A meta-analysis. Pain 1998, 74, 181–187. [Google Scholar] [CrossRef] [PubMed]
- de Williams, A.C.C.; Fisher, E.; Hearn, L.; Eccleston, C. Evidence-based psychological interventions for adults with chronic pain: Precision, control, quality, and equipoise. Pain 2021, 162, 2149–2153. [Google Scholar] [CrossRef]
- Nelder, J.A.; Wedderburn, R.W.M. Generalized Linear Models. J. R. Stat. Soc. Ser. A. 1972, 135, 370–384. [Google Scholar] [CrossRef]
- Birknes, J.K.; White, A.P.; Albert, T.J.; Shaffrey, C.I.; Harrop, J.S. Adult degenerative scoliosis: A review. Neurosurgery 2008, 63 (Suppl. 3), 94–103. [Google Scholar] [CrossRef]
- Balagué, F.; Pellisé, F. Adolescent idiopathic scoliosis and back pain. Scoliosis Spinal Disord. 2016, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Koes, B.W.; van Tulder, M.W.; Thomas, S. Diagnosis and treatment of low back pain. BMJ 2006, 332, 1430–1434. [Google Scholar] [CrossRef]
- Chiarotto, A.; Koes, B.W. Nonspecific Low Back Pain. N. Engl. J. Med. 2022, 386, 1732–1740. [Google Scholar] [CrossRef]
- Bogduk, N.; Aprill, C.; Derby, R. Lumbar discogenic pain: State-of-the-art review. Pain Med. 2013, 14, 813–836. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Kim, H.I.; Shin, D.A.; Shin, D.G.; Lee, J.O.; Kim, H.J.; Chung, J.-H. Usefulness of pain distribution pattern assessment in decision-making for the patients with lumbar zygapophyseal and sacroiliac joint arthropathy. J. Korean Med. Sci. 2007, 22, 1048–1054. [Google Scholar] [CrossRef]
- Cohen, S.P.; Raja, S.N. Pathogenesis, diagnosis, and treatment of lumbar zygapophysial (facet) joint pain. Anesthesiology 2007, 106, 591–614. [Google Scholar] [CrossRef] [PubMed]
- Noonan, A.M.; Brown, S.H.M. Paraspinal muscle pathophysiology associated with low back pain and spine degenerative disorders. JOR Spine 2021, 4, e1171. [Google Scholar] [CrossRef]
- Han, C.S.; Hancock, M.J.; Sharma, S.; Sharma, S.; Harris, I.A.; Cohen, S.P.; Magnussen, J.; Maher, C.G.; Traeger, A.C. Low back pain of disc, sacroiliac joint, or facet joint origin: A diagnostic accuracy systematic review. eClinicalMedicine 2023, 59, 101960. [Google Scholar] [CrossRef] [PubMed]
- Takata, K.; Hirotani, H. Pain drawing in the evaluation of low back pain. Int. Orthop. 1995, 19, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Ransford, A.O.; Cairns, D.; Mooney, V. The pain drawing as an aid to the psychologic evaluation of patients with low-back pain. Spine 1976, 1, 127–134. [Google Scholar] [CrossRef]
- Hayashi, K.; Arai, Y.-C.P.; Morimoto, A.; Aono, S.; Yoshimoto, T.; Nishihara, M.; Osuga, T.; Inoue, S.; Ushida, T. Associations between pain drawing and psychological characteristics of different body region pains. Pain Pract. 2015, 15, 300–307. [Google Scholar] [CrossRef]
- Reis, F.; Guimarães, F.; Nogueira, L.C.; Meziat-Filho, N.; Sanchez, T.A.; Wideman, T. Association between pain drawing and psychological factors in musculoskeletal chronic pain: A systematic review. Physiother. Theory Pract. 2019, 35, 533–542. [Google Scholar] [CrossRef]
- McIntyre, S.; Nagi, S.S.; McGlone, F.; Olausson, H. The Effects of Ageing on Tactile Function in Humans. Neuroscience 2021, 464, 53–58. [Google Scholar] [CrossRef]
- Lautenbacher, S.; Peters, J.H.; Heesen, M.; Scheel, J.; Kunz, M. Age changes in pain perception: A systematic-review and meta-analysis of age effects on pain and tolerance thresholds. Neurosci. Biobehav. Rev. 2017, 75, 104–113. [Google Scholar] [CrossRef]
- El Tumi, H.; Johnson, M.I.; Dantas, P.B.F.; Maynard, M.J.; Tashani, O.A. Age-related changes in pain sensitivity in healthy humans: A systematic review with meta-analysis. Eur. J. Pain 2017, 21, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Macefield, V.G.; Gandevia, S.C.; Henderson, L.A. Discrete changes in cortical activation during experimentally induced referred muscle pain: A single-trial fMRI study. Cereb. Cortex 2007, 17, 2050–2059. [Google Scholar] [CrossRef] [PubMed]
- Peters, R. Ageing and the brain. Postgrad. Med. J. 2006, 82, 84–88. [Google Scholar] [CrossRef]
- Schwab, F.; Ungar, B.; Blondel, B.; Buchowski, J.; Coe, J.; Deinlein, D.; Lafage, V. Scoliosis Research Society-Schwab adult spinal deformity classification: A validation study. Spine 2012, 37, 1077–1082. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Lt-DLS | Rt-DLS | p Value |
|---|---|---|---|
| Age (yrs) | 76.7 (10.3) | 75.4 (6.9) | 0.48 |
| Female (%) | 80.0 | 66.0 | 0.11 |
| Pain intensity | 5 [4] | 4 [5] | 0.90 |
| Pain area (AU) | 95.3 [132.3] | 147.1 [279.3] | 0.23 |
| Variables | Lt DLS (n = 50) | Rt DLS (n = 50) | p Value |
|---|---|---|---|
| Apical vertebrae | |||
| L1 (n) | 13 | 8 | 0.26 |
| L2 (n) | 15 | 20 | |
| L3 (n) | 20 | 22 | |
| L4 (n) | 2 | 0 | |
| Degeneration score | 2 [1.8] | 2 [1] | 0.91 |
| Cobb angle (degree) | 21.0 [12.8] | 22.6 [14.9] | 0.80 |
| Major pain site | |||
| Convex side dominant (n) | 15 | 18 | 0.67 |
| Center dominant (n) | 17 | 18 | |
| Concave side dominant (n) | 18 | 14 |
| Variables | Pain Intensity | Pain Area | ||
|---|---|---|---|---|
| β | p-Value | β | p-Value | |
| Age | <0.01 | 0.92 | −0.03 | <0.01 |
| Sex | 0.02 (female) | 0.87 | −0.07 (female) | 0.41 |
| Curve side | 0.01 (Lt), 0.00 (Rt) # | 0.92 | −0.45 (Lt), 0.00 (Rt) # | 0.03 |
| Cobb angle | <0.01 | 0.36 | −0.01 | 0.21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kojima, S.; Ikemoto, T.; Arai, Y.-C.; Hirasawa, A.; Deie, M.; Takahashi, N. Associations between Degenerative Lumbar Scoliosis Structures and Pain Distribution in Adults with Chronic Low Back Pain. Healthcare 2023, 11, 2357. https://doi.org/10.3390/healthcare11162357
Kojima S, Ikemoto T, Arai Y-C, Hirasawa A, Deie M, Takahashi N. Associations between Degenerative Lumbar Scoliosis Structures and Pain Distribution in Adults with Chronic Low Back Pain. Healthcare. 2023; 11(16):2357. https://doi.org/10.3390/healthcare11162357
Chicago/Turabian StyleKojima, Shoji, Tatsunori Ikemoto, Young-Chang Arai, Atsuhiko Hirasawa, Masataka Deie, and Nobunori Takahashi. 2023. "Associations between Degenerative Lumbar Scoliosis Structures and Pain Distribution in Adults with Chronic Low Back Pain" Healthcare 11, no. 16: 2357. https://doi.org/10.3390/healthcare11162357
APA StyleKojima, S., Ikemoto, T., Arai, Y.-C., Hirasawa, A., Deie, M., & Takahashi, N. (2023). Associations between Degenerative Lumbar Scoliosis Structures and Pain Distribution in Adults with Chronic Low Back Pain. Healthcare, 11(16), 2357. https://doi.org/10.3390/healthcare11162357