Looking Back, Looking Forward: A Study Protocol for a Mixed-Methods Multiple-Case Study to Examine Improvement Sustainability of Large-Scale Initiatives in Tertiary Hospitals


Abstract
1. Introduction
Study Aims and Research Questions
- (1)
- What are the enablers and barriers to sustaining the improvement?
- (2)
- How do relevant organizational records demonstrate the initiative outcome?
- (3)
- What factors in hospital-wide change implementation lead to sustained improvement?
- (4)
- What hospital-wide change processes enable sustained improvement?
2. Design and Methods
2.1. Study Design
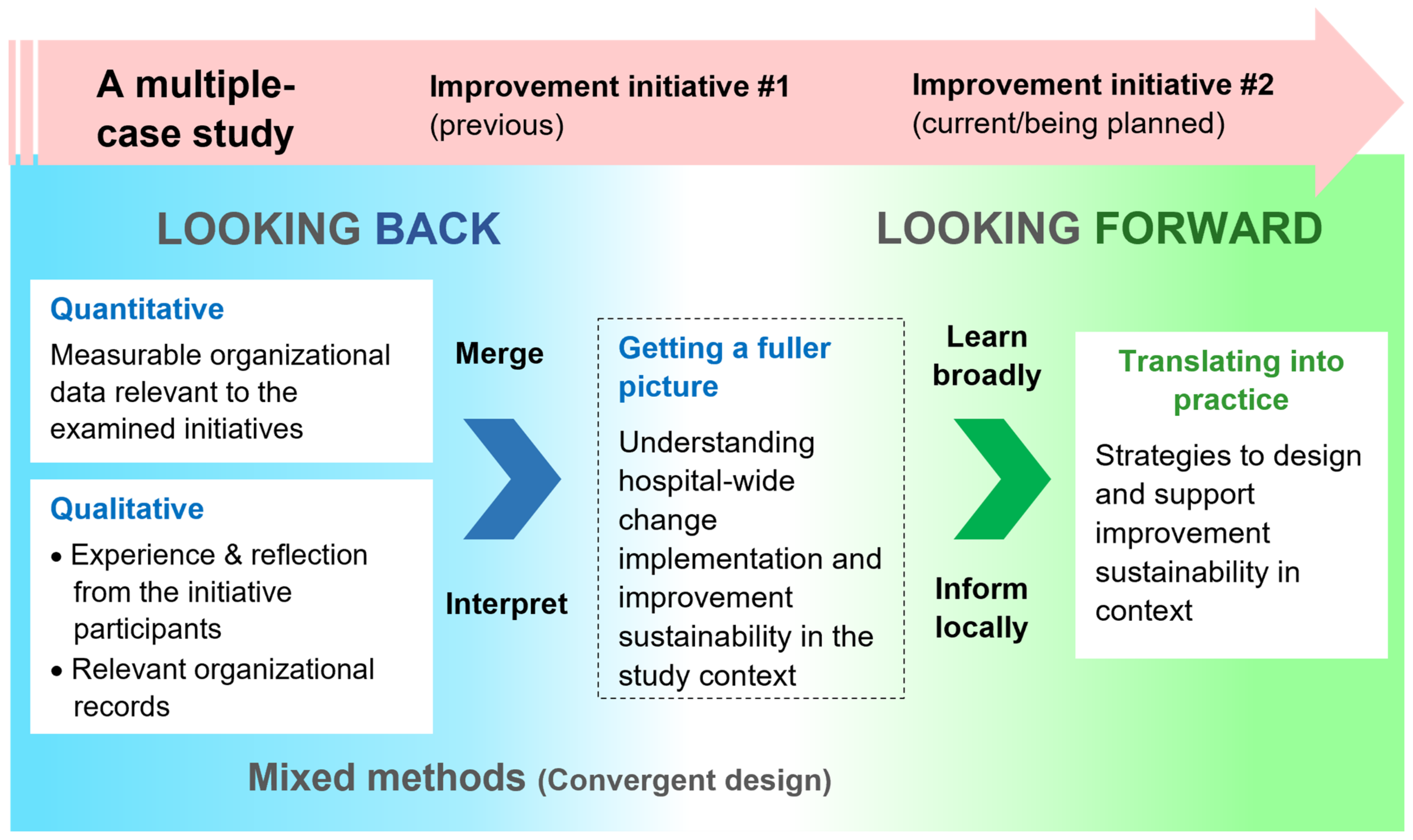
2.1.1. Multiple-Case Study
2.1.2. Mixed Methods
2.2. Study Setting
2.3. Initiatives Selected for This Study
2.3.1. Right Time Every Time (Initiative #1)
2.3.2. Speaking Up for SafetyTM (Initiative #2)
3. Study Procedures
3.1. Quantitative Data Collection—Routinely Collected Organizational Data
3.2. Qualitative Data Collection
3.2.1. Semi-Structured Individual Staff Interviews
Participant Stratification
Interview Questions
3.2.2. Organizational Records
3.3. Data Analysis
3.3.1. Multiple-Case Analysis
3.3.2. Quantitative Data Analysis
3.3.3. Qualitative Data Analysis
3.3.4. Integrating Mixed-Methods Data
4. Discussion
5. Conclusions
6. Dissemination
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Slawomirski, L.; Auraaen, A.; Klazinga, N. The Economics of Patient Safety: Strengthening a Value-Based Approach to Reducing Patient Harm at National Level; Organisation for Economic Co-operation and Development: Paris, France, 2017. [Google Scholar]
- Donnelly, L.F. Avoiding failure: Tools for successful and sustainable quality-improvement projects. Pediatr. Radiol. 2017, 47, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Lawson, T.; Weekes, L.; Hill, M. Ensuring success and sustainability of a quality improvement project. BJA Educ. 2018, 18, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Scoville, R.; Little, K.; Rakover, J.; Luther, K.; Mate, K. Sustaining Improvement—IHI White Paper; Institute for Healthcare Improvement: Cambridge, MA, USA, 2016. [Google Scholar]
- Moore, J.E.; Mascarenhas, A.; Bain, J.; Straus, S.E. Developing a comprehensive definition of sustainability. Implement. Sci. 2017, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, J.; Ludlow, K.; Testa, L.; Herkes, J.; Augustsson, H.; Lamprell, G.; McPherson, E.; Zurynski, Y. Built to last? The sustainability of healthcare system improvements, programmes and interventions: A systematic integrative review. BMJ Open 2020, 10, e036453. [Google Scholar] [CrossRef]
- Braithwaite, J.; Churruca, K.; Long, J.C.; Ellis, L.A.; Herkes, J. When complexity science meets implementation science: A theoretical and empirical analysis of systems change. BMC Med. 2018, 16, 63. [Google Scholar] [CrossRef]
- Thompson, D.S.; Fazio, X.; Kustra, E.; Patrick, L.; Stanley, D. Scoping review of complexity theory in health services research. BMC Health Serv. Res. 2016, 16, 87. [Google Scholar] [CrossRef]
- Cowie, J.; Nicoll, A.; Dimova, E.D.; Campbell, P.; Duncan, E.A. The barriers and facilitators influencing the sustainability of hospital-based interventions: A systematic review. BMC Health Serv. Res. 2020, 20, 588. [Google Scholar] [CrossRef]
- De Silva, D. What’s Getting in the Way? Barriers to Improvement in the NHS; The Health Foundation: London, UK, 2015. [Google Scholar]
- Baker, D.; Quinn, B.; Ewan, V.; Giuliano, K.K. Sustaining quality improvement: Long-term reduction of nonventilator hospital-acquired pneumonia. J. Nurs. Care Qual. 2019, 34, 223–229. [Google Scholar] [CrossRef]
- Baloh, J.; Zhu, X.; Ward, M.M. What influences sustainment and nonsustainment of facilitation activities in implementation? Analysis of organizational factors in hospitals implementing TeamSTEPPS. Med. Care Res. Rev. 2021, 78, 146–156. [Google Scholar] [CrossRef]
- Silver, S.A.; McQuillan, R.; Harel, Z.; Weizman, A.V.; Thomas, A.; Nesrallah, G.; Bell, C.M.; Chan, C.T.; Chertow, G.M. How to sustain change and support continuous quality improvement. Clin. J. Am. Soc. Nephrol. 2016, 11, 916–924. [Google Scholar] [CrossRef]
- Glasgow, J.M.; Davies, M.L.; Kaboli, P.J. Findings from a national improvement collaborative: Are improvements sustained? BMJ Qual. Saf. 2012, 21, 663. [Google Scholar] [CrossRef]
- Robert, G.; Sarre, S.; Maben, J.; Griffiths, P.; Chable, R. Exploring the sustainability of quality improvement interventions in healthcare organisations: A multiple methods study of the 10-year impact of the ‘Productive Ward: Releasing Time to Care’ programme in English acute hospitals. BMJ Qual. Saf. 2020, 29, 31–40. [Google Scholar] [CrossRef]
- Pieterse, J.H.; Caniëls, M.C.J.; Homan, T. Professional discourses and resistance to change. J. Organ. Chang. Manag. 2012, 25, 798–818. [Google Scholar] [CrossRef]
- NHS Institute of Innovation and Improvement. Improvement Leaders’ Guide: Sustainability and its Relationship with Spread and Adoption. Available online: https://www.england.nhs.uk/improvement-hub/publication/improvement-leaders-guide-sustainability-and-its-relationship-with-spread-and-adoption-general-improvement-skills/ (accessed on 13 April 2023).
- Shelton, R.C.; Cooper, B.R.; Stirman, S.W. The sustainability of evidence-based interventions and practices in public health and health care. Annu. Rev. Public Health 2018, 39, 55–76. [Google Scholar] [CrossRef]
- Lennox, L.; Maher, L.; Reed, J. Navigating the sustainability landscape: A systematic review of sustainability approaches in healthcare. Implement. Sci. 2018, 13, 27. [Google Scholar] [CrossRef]
- Cadilhac, D.A.; Andrew, N.E.; Stroil Salama, E.; Hill, K.; Middleton, S.; Horton, E.; Meade, I.; Kuhle, S.; Nelson, M.R.; Grimley, R. Improving discharge care: The potential of a new organisational intervention to improve discharge after hospitalisation for acute stroke, a controlled before–after pilot study. BMJ Open 2017, 7, e016010. [Google Scholar] [CrossRef]
- Li, S.A.; Jeffs, L.; Barwick, M.; Stevens, B. Organizational contextual features that influence the implementation of evidence-based practices across healthcare settings: A systematic integrative review. Syst. Rev. 2018, 7, 72. [Google Scholar] [CrossRef]
- Cummings, A.; Lund, S.; Campling, N.; May, C.R.; Richardson, A.; Myall, M. Implementing communication and decision-making interventions directed at goals of care: A theory-led scoping review. BMJ Open 2017, 7, e017056. [Google Scholar] [CrossRef]
- Kaplan, H.C.; Brady, P.W.; Dritz, M.C.; Hooper, D.K.; Linam, W.M.; Froehle, C.M.; Margolis, P. The influence of context on quality improvement success in health care: A systematic review of the literature. Milbank Q. 2010, 88, 500–559. [Google Scholar] [CrossRef]
- Ross, J.; Stevenson, F.; Lau, R.; Murray, E. Factors that influence the implementation of e-health: A systematic review of systematic reviews (an update). Implement. Sci. 2016, 11, 146. [Google Scholar] [CrossRef]
- Hulscher, M.E.; Schouten, L.M.; Grol, R.P.; Buchan, H. Determinants of success of quality improvement collaboratives: What does the literature show? BMJ Qual. Saf. 2013, 22, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Ament, S.M.C.; Gillissen, F.; Moser, A.; Maessen, J.M.C.; Dirksen, C.D.; von Meyenfeldt, M.F.; van der Weijden, T. Factors associated with sustainability of 2 quality improvement programs after achieving early implementation success. A qualitative case study. J. Eval. Clin. Pract. 2017, 23, 1135–1143. [Google Scholar] [CrossRef] [PubMed]
- Ilott, I.; Gerrish, K.; Booth, A.; Field, B. Testing the Consolidated Framework for Implementation Research on health care innovations from South Yorkshire. J. Eval. Clin. Pract. 2013, 19, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Skingley, A.; Marshall, J. Challenges of implementing and embedding a programme to improve care for older people with dementia on hospital wards. Nurs. Older People 2018, 30, 29–33. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lewin, K. Frontiers in group dynamics: Concept, method and reality in social science; social equilibria and social change. Hum. Relat. 1947, 1, 5–41. [Google Scholar] [CrossRef]
- Burnes, B. The origins of Lewin’s Three-Step Model of Change. J. Appl. Behav. Sci. 2020, 56, 32–59. [Google Scholar] [CrossRef]
- Burnes, B. Kurt Lewin and complexity theories: Back to the future? J. Chang. Manag. 2004, 4, 309–325. [Google Scholar] [CrossRef]
- Stouten, J.; Rousseau, D.M.; De Cremer, D. Successful organizational change: Integrating the management practice and scholarly literatures. Acad. Manag. Ann. 2018, 12, 752–788. [Google Scholar] [CrossRef]
- Harrison, R.; Fischer, S.; Walpola, R.; Chauhan, A.; Babalola, T.; Mears, S.; Le-Dao, H. Where do models for change management, improvement and implementation meet? A systematic review of the applications of change management models in healthcare. J. Healthc. Leadersh. 2021, 13, 85–108. [Google Scholar] [CrossRef]
- French, W.L.; Bell, C.M. A definition and history of Organisation Development: Some comments. Acad. Manag. Proc. 1971, 1971, 146–153. [Google Scholar] [CrossRef]
- Argote, L.; Miron-Spektor, E. Organizational learning: From experience to knowledge. Organ. Sci. 2011, 22, 1123–1137. [Google Scholar] [CrossRef]
- Tosey, P.; Visser, M.; Saunders, M.N. The origins and conceptualizations of ‘triple-loop’ learning: A critical review. Manag. Learn. 2012, 43, 291–307. [Google Scholar] [CrossRef]
- Dixon-Woods, M.; McNicol, S.; Martin, G. Ten challenges in improving quality in healthcare: Lessons from the Health Foundation’s programme evaluations and relevant literature. BMJ Qual. Saf. 2012, 21, 876. [Google Scholar] [CrossRef]
- Mitchell, S.E.; Weigel, G.M.; Laurens, V.; Martin, J.; Jack, B.W. Implementation and adaptation of the Re-Engineered Discharge (RED) in five California hospitals: A qualitative research study. BMC Health Serv. Res. 2017, 17, 291. [Google Scholar] [CrossRef]
- Moon, S.E.; Hogden, A.; Eljiz, K. Sustaining improvement of hospital-wide initiative for patient safety and quality: A systematic scoping review. BMJ Open Qual. 2022, 11, e002057. [Google Scholar] [CrossRef]
- Coles, E.; Anderson, J.; Maxwell, M.; Harris, F.M.; Gray, N.M.; Milner, G.; MacGillivray, S. The influence of contextual factors on healthcare quality improvement initiatives: A realist review. Syst. Rev. 2020, 9, 94. [Google Scholar] [CrossRef]
- Fulop, N.J.; Ramsay, A.I.G. How organisations contribute to improving the quality of healthcare. BMJ 2019, 365, l1773. [Google Scholar] [CrossRef]
- Ammerman, A.; Smith, T.W.; Calancie, L. Practice-Based Evidence in Public Health: Improving Reach, Relevance, and Results. Annu. Rev. Public Health 2014, 35, 47–63. [Google Scholar] [CrossRef]
- Higgs, M.J.; Kuipers, B.S.; Steijn, B. Change leadership and change embeddedness in public organizations: Connecting macrolevel reform to microlevel implementation. Public Adm. 2022, 100, 1–15. [Google Scholar] [CrossRef]
- Lee, S.-Y.D.; Iott, B.; Banaszak-Holl, J.; Shih, S.-F.; Raj, M.; Johnson, K.E.; Kiessling, K.; Moore-Petinak, N.d. Application of mixed methods in health services management research: A systematic review. Med. Care Res. Rev. 2022, 79, 331–344. [Google Scholar] [CrossRef]
- Stake, R.E. Multiple Case Study Analysis; Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Yin, R.K. Case Study Research and Applications: Design and Methods, 6th ed.; Sage: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Crowe, S.; Cresswell, K.; Robertson, A.; Huby, G.; Avery, A.; Sheikh, A. The case study approach. BMC Med. Res. Methodol. 2011, 11, 100. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative and Mixed Methods Approaches, 5th ed.; Sage Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Hill, J.N.; Guihan, M.; Hogan, T.P.; Smith, B.M.; LaVela, S.L.; Weaver, F.M.; Anaya, H.D.; Evans, C.T. Use of the PARIHS Framework for retrospective and prospective Implementation evaluations. Worldviews Evid. Based Nurs. 2017, 14, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Snapshot of Australia. Available online: https://www.abs.gov.au/statistics/people/people-and-communities/snapshot-australia/2021 (accessed on 21 May 2023).
- Australian Institute of Health and Welfare. Glossary. Available online: https://www.aihw.gov.au/reports-data/myhospitals/content/glossary (accessed on 16 July 2023).
- Australian Commission on Safety and Quality in Health Care. National Standard Medication Chart (NSMC) Audit. Available online: https://www.safetyandquality.gov.au/our-work/medication-safety/national-standard-medication-chart-nsmc-audit (accessed on 21 May 2023).
- Cognitive Institute. Speaking Up for Safety™ Programme. Available online: https://www.cognitiveinstitute.org/healthcare-courses/speaking-up-for-safety-programme/ (accessed on 18 March 2023).
- De Jonckheere, M.; Vaughn, L.M. Semistructured interviewing in primary care research: A balance of relationship and rigour. Fam. Med. Community Health 2019, 7, e000057. [Google Scholar] [CrossRef] [PubMed]
- Nyström, M.E.; Höög, E.; Garvare, R.; Andersson Bäck, M.; Terris, D.D.; Hansson, J. Exploring the potential of a multi-level approach to improve capability for continuous organizational improvement and learning in a Swedish healthcare region. BMC Health Serv. Res. 2018, 18, 376. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Taher, S.; Muramatsu, N.; Odoms-Young, A.; Peacock, N.; Michael, C.F.; Courtney, K.S. An embedded multiple case study: Using CFIR to map clinical food security screening constructs for the development of primary care practice guidelines. BMC Public Health 2022, 22, 97. [Google Scholar] [CrossRef]
- Patridge, E.F.; Bardyn, T.P. Research Electronic Data Capture (REDCap). J. Med. Libr. Assoc. 2018, 106, 142–144. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic analysis: Striving to meet the trustworthiness criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Dalglish, S.L.; Khalid, H.; McMahon, S.A. Document analysis in health policy research: The READ approach. Health Policy Plan. 2020, 35, 1424–1431. [Google Scholar] [CrossRef]
- Pomare, C.; Churruca, K.; Long, J.C.; Ellis, L.A.; Gardiner, B.; Braithwaite, J. Exploring the ripple effects of an Australian hospital redevelopment: A protocol for a longitudinal, mixed-methods study. BMJ Open 2019, 9, e027186. [Google Scholar] [CrossRef]
- QSR International Pyt Ltd. NVivo (Released in March 2020). 2020. Available online: https://support.qsrinternational.com/s/ (accessed on 27 July 2023).
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs-principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef]
- Curry, L.A.; Krumholz, H.M.; O’Cathain, A.; Clark, V.L.P.; Cherlin, E.; Bradley, E.H. Mixed methods in biomedical and health services research. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 119–123. [Google Scholar] [CrossRef]
- Brown, K.M.; Elliott, S.J.; Leatherdale, S.T.; Robertson-Wilson, J. Searching for rigour in the reporting of mixed methods population health research: A methodological review. Health Educ. Res. 2015, 30, 811–839. [Google Scholar] [CrossRef]
- Nilsen, P.; Bernhardsson, S. Context matters in implementation science: A scoping review of determinant frameworks that describe contextual determinants for implementation outcomes. BMC Health Serv. Res. 2019, 19, 189. [Google Scholar] [CrossRef]
- Chambers, D.A.; Glasgow, R.E.; Stange, K.C. The dynamic sustainability framework: Addressing the paradox of sustainment amid ongoing change. Implement. Sci. 2013, 8, 117. [Google Scholar] [CrossRef]
- Marshall, M.; Silva, D.d.; Cruickshank, L.; Shand, J.; Wei, L.; Anderson, J. What we know about designing an effective improvement intervention (but too often fail to put into practice). BMJ Qual. Saf. 2017, 26, 578–582. [Google Scholar] [CrossRef]
- Oreg, S.; Vakola, M.; Armenakis, A. Change recipients’ reactions to organisational change: A 60-year review of quantitative studies. J. Appl. Behav. Sci. 2011, 47, 461–524. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Reardon, C.M.; Widerquist, M.A.O.; Lowery, J. The updated Consolidated Framework for Implementation Research based on user feedback. Implement. Sci. 2022, 17, 75. [Google Scholar] [CrossRef]
- Harvey, G.; Kitson, A. PARIHS revisited: From heuristic to integrated framework for the successful implementation of knowledge into practice. Implement. Sci. 2016, 11, 33. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mixed-Methods Data | Initiative #1 (2014–2015) | Initiative #2 (2020–Present) |
|---|---|---|
| Quantitative data: Routinely collected organizational data |
|
|
|
| |
| Qualitative data: Interviews and organizational records |
|
|
|
|
| Participant Group | Initiative #1 | Initiative #2 | Total |
|---|---|---|---|
| Group 1: Senior managers | 3–4 | 5 | 8–9 |
| Group 2: Implementation team members | 3–4 | 5 | 8–9 |
| Group 3: Frontline managers | 3–4 | 5 | 8–9 |
| Group 4: Frontline staff | 3–4 | 5 | 8–9 |
| Total Interview participant no. | 12–16 | 20 | 32–36 |
| Initiative Code | Participant Group Code | Profession Code |
|---|---|---|
| Initiative #1: 1 | Group 1: G1 | Nurse: NR |
| Initiative #2: 2 | Group 2: G2 | Doctor: DR |
| Group 3: G3 | Allied Health: AH | |
| Group 4: G4 | Non-clinical professionals: NC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, S.E.J.; Hogden, A.; Eljiz, K.; Siddiqui, N. Looking Back, Looking Forward: A Study Protocol for a Mixed-Methods Multiple-Case Study to Examine Improvement Sustainability of Large-Scale Initiatives in Tertiary Hospitals. Healthcare 2023, 11, 2175. https://doi.org/10.3390/healthcare11152175
Moon SEJ, Hogden A, Eljiz K, Siddiqui N. Looking Back, Looking Forward: A Study Protocol for a Mixed-Methods Multiple-Case Study to Examine Improvement Sustainability of Large-Scale Initiatives in Tertiary Hospitals. Healthcare. 2023; 11(15):2175. https://doi.org/10.3390/healthcare11152175
Chicago/Turabian StyleMoon, Sarah E. J., Anne Hogden, Kathy Eljiz, and Nazlee Siddiqui. 2023. "Looking Back, Looking Forward: A Study Protocol for a Mixed-Methods Multiple-Case Study to Examine Improvement Sustainability of Large-Scale Initiatives in Tertiary Hospitals" Healthcare 11, no. 15: 2175. https://doi.org/10.3390/healthcare11152175
APA StyleMoon, S. E. J., Hogden, A., Eljiz, K., & Siddiqui, N. (2023). Looking Back, Looking Forward: A Study Protocol for a Mixed-Methods Multiple-Case Study to Examine Improvement Sustainability of Large-Scale Initiatives in Tertiary Hospitals. Healthcare, 11(15), 2175. https://doi.org/10.3390/healthcare11152175