
Factors Associated with Depression, Anxiety, and Somatic Symptoms among International Salespeople in the Medical Device Industry: A Cross-Sectional Study in China

 , ,
, ,  ,
,
Abstract
1. Introduction
1.1. Job Obligations and Responsibilities of IVD International Salespeople
1.2. Effort–Reward Imbalance
1.3. Health-Promoting Leadership and Health Climate
1.4. Positive Mental Health
1.5. Socio-Demographic Characteristics
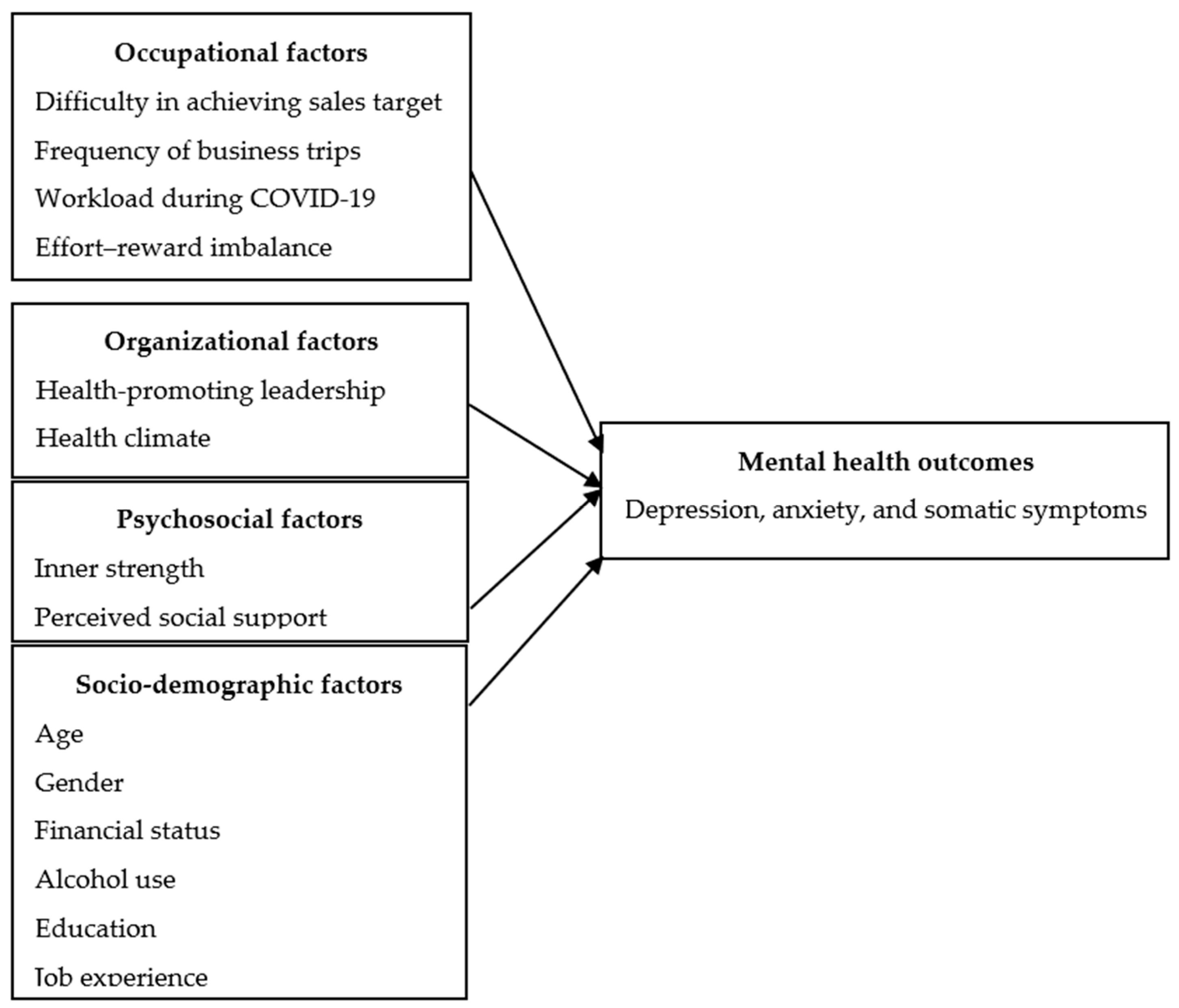
1.6. Current Study
2. Materials and Methods
2.1. Study Design
2.2. Participants
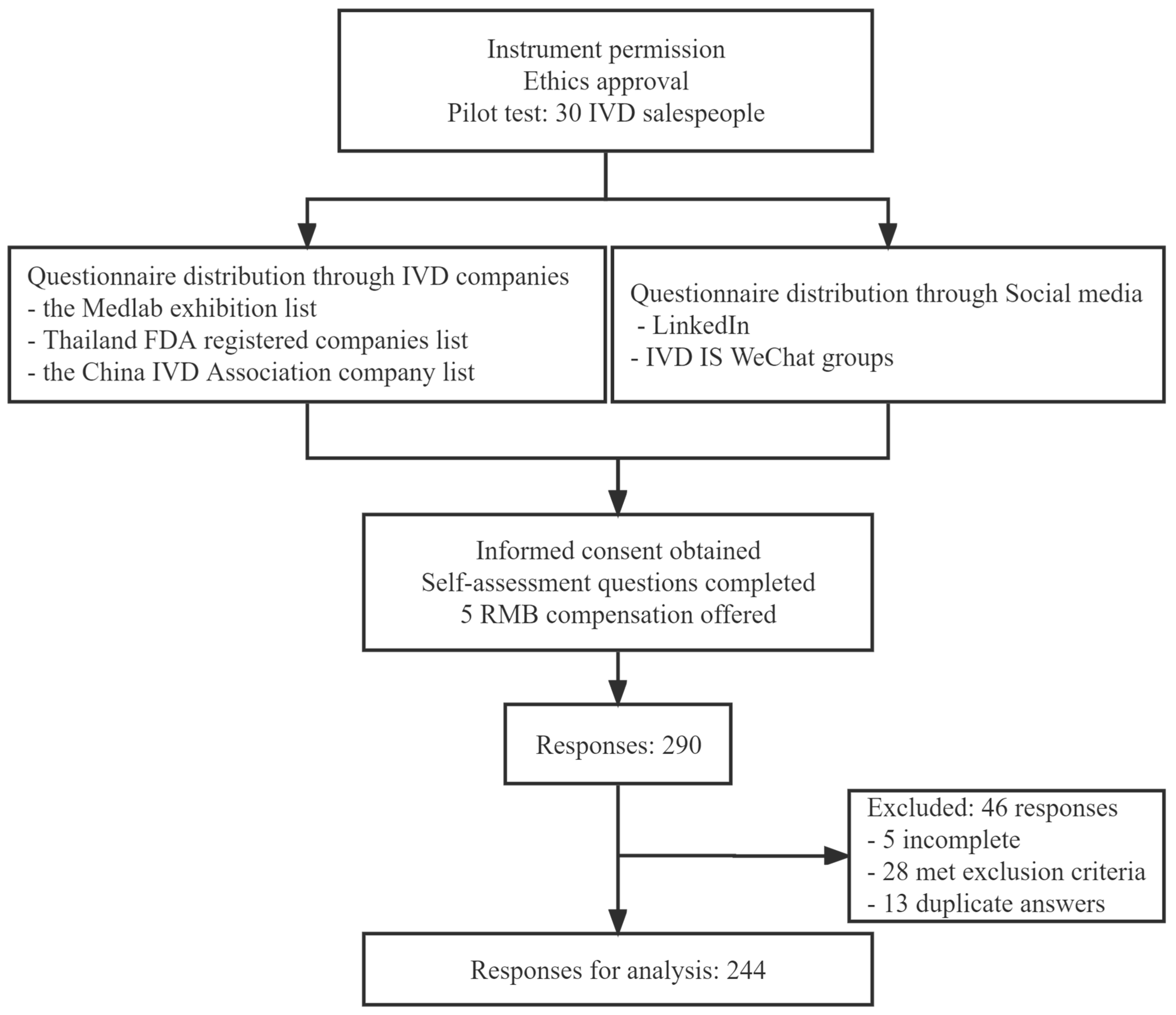
2.3. Procedure
2.4. Measurements
2.4.1. Core Symptoms Index
2.4.2. Effort–Reward Imbalance
2.4.3. Health-Promoting Leadership
2.4.4. Health Climate
2.4.5. Inner Strength-Based Inventory
2.4.6. Multidimensional Scale of Perceived Social Support
2.4.7. Characteristics of Participants
2.5. Statistical Analysis
3. Results
3.1. Socio-Demographic and Psychological Characteristics of Participants
3.2. Psychological Variables and Characteristics of Participants
3.3. Pearson’s Correlation among Psychological Variables
3.4. Factors Predicting Mental Health Outcomes in IVD International Salespeople
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lelliott, P.; Tulloch, S.; Boardman, J.; Harvey, S.; Henderson, H. Mental Health and Work; Royal College of Psychiatrists: London, UK, 2008. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/212266/hwwb-mental-health-and-work.pdf (accessed on 6 July 2023).
- OECD. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2016; ISBN 978-92-64-30335-5. [Google Scholar]
- Australian Bureau of Statistics. National Survey of Mental Health and Wellbeing: Summary of Results. Available online: https://www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/latest-release#content (accessed on 21 January 2022).
- Center for Disease Control and Prevention Mental Health in the Workplace. Mental Health in the Workplace. Available online: https://www.cdc.gov/workplacehealthpromotion/tools-resources/workplace-health/mental-health/index.html (accessed on 6 July 2023).
- Zhang, S.X.; Batra, K.; Liu, T.; Dong, R.K.; Xu, W.; Yin, A.; Delios, A.; Chen, B.Z.; Chen, R.Z.; Miller, S.; et al. Meta-analytical evidence on mental disorder symptoms during the COVID-19 pandemic in Latin America. medRxiv 2021. [Google Scholar] [CrossRef]
- Zhu, X. The Relationship between Organizational Commitment and Metal Health in Import and Export Company Employee. Master’s Thesis, Ningbo University, Ningbo, China, 2008. Available online: https://kns.cnki.net/KCMS/detail/detail.aspx?dbname=CMFD2011&filename=2010025913.nh (accessed on 11 January 2020).
- Huang, Y.; Wang, Y.; Wang, H.; Liu, Z.; Yu, X.; Yan, J.; Yu, Y.; Kou, C.; Xu, X.; Lu, J.; et al. Prevalence of mental disorders in China: A cross-sectional epidemiological study. Lancet Psychiatry 2019, 6, 211–224. [Google Scholar] [CrossRef]
- Li, Q.; Cheng, L.G. Employee Assistance Program (EAP): An Effective Way to Improve Employee Mental Health. J. Minjiang Univ. 2004, 25, 125–128. [Google Scholar] [CrossRef]
- The Lancet Global Health, Mental Health Matters. The Lancet Global Health. Available online: https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(20)30432-0/fulltext (accessed on 8 November 2020).
- Dragioti, E.; Li, H.; Tsitsas, G.; Lee, K.H.; Choi, J.; Kim, J.; Choi, Y.J.; Tsamakis, K.; Estradé, A.; Agorastos, A.; et al. A large-scale meta-analytic atlas of mental health problems prevalence during the COVID-19 early pandemic. J. Med. Virol. 2021, 94, 1935–1949. [Google Scholar] [CrossRef]
- Duan, H.; Yan, L.; Ding, X.; Gan, Y.; Kohn, N.; Wu, J. Impact of the COVID-19 pandemic on mental health in the general Chinese population: Changes, predictors and psychosocial correlates. Psychiatry Res. 2020, 293, 113396. [Google Scholar] [CrossRef]
- Pierre-Olivier, G.; International Monetary Fund. Global Economic Growth Slows Amid Gloomy and More Uncertain Outlook. Available online: https://www.imf.org/en/Blogs/Articles/2022/07/26/blog-weo-update-july-2022 (accessed on 26 July 2022).
- World Health Organization. Mental Health at Work; World Health Organization: Geneva, Switzerland, 2022; Volume 2023. [Google Scholar]
- Vashist, S.K. In Vitro Diagnostic Assays for COVID-19: Recent Advances and Emerging Trends. Diagnostics 2020, 10, 202. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Sumant, O. In Vitro Diagnostics IVD Market Research Report. Available online: https://www.marketresearchengine.com/reportdetails/global-in-vitro-diagnostics-ivd-market# (accessed on 15 October 2020).
- Kalorama Information. 2021 IVD Market Update and COVID-19 Impact; Kalorama Information: Bruce Carlson, VA, USA, 2021; Volume 21-016. [Google Scholar]
- Erbach, G. In Vitro Diagnostic Medical Devices. Available online: https://www.europarl.europa.eu/RegData/etudes/BRIE/2014/542151/EPRS_BRI(2014)542151_REV1_EN.pdf (accessed on 16 October 2020).
- O’Connor, B.; Pollner, F.; Fugh-Berman, A. Salespeople in the Surgical Suite: Relationships between Surgeons and Medical Device Representatives. PLoS ONE 2016, 11, e0158510. [Google Scholar] [CrossRef]
- Wondfo Biotech. Guangzhou Wondfo Biotech Co., Ltd. 2021 Annual Report; Wondfo Biotech: Guangzhou, China, 2022. [Google Scholar]
- McKinsey Health Institute. Addressing Employee Burnout: Are You Solving the Right Problem? Available online: https://www.mckinsey.com/mhi/our-insights/addressing-employee-burnout-are-you-solving-the-right-problem (accessed on 11 July 2023).
- Atif, M.; Bashir, A.; Saleem, Q.; Hussain, R.; Scahill, S.; Babar, Z.U. Health-related quality of life and depression among medical sales representatives in Pakistan. Springerplus 2016, 5, 1048. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.B.; Meena, J.S.; Sb, P.; Js, M. Work Induced Stress among Medical Representatives in Aurangabad City, Maharashtra. Natl. J. Community Med. 2013, 4, 277–281. [Google Scholar]
- Zhang, Z.; Ding, M.; Pu, X.; Xie, C. Mental health status of 239 foreign employees in Guangzhou. South China J. Prev. Med. 2011, 37, 21–24, 28. [Google Scholar]
- Pensri, P.; Janwantanakul, P.; Chaikumarn, M. Prevalence of self-reported musculoskeletal symptoms in salespersons. Occup. Med. 2009, 59, 499–501. [Google Scholar] [CrossRef] [PubMed]
- Burkholder, J.D.; Joines, R.; Cunningham-Hill, M.; Xu, B. Health and well-being factors associated with international business travel. J. Travel Med. 2010, 17, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. Sleep and Sleep Disorders. Available online: https://www.cdc.gov/sleep/index.html (accessed on 11 March 2022).
- Siegrist, J.; Wahrendorf, M. Work Stress and Health in a Globalized Economy: The Model of Effort-Reward Imbalance; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Ren, C.; Li, X.; Yao, X.; Pi, Z.; Qi, S. Psychometric Properties of the Effort-Reward Imbalance Questionnaire for Teachers (Teacher ERIQ). Front. Psychol. 2019, 10, 2047. [Google Scholar] [CrossRef]
- Ji, Y.Q.; Li, S.; Wang, J.; Liu, X.M.; Ren, J.; Wang, C. Association of occupational stress with job burnout and depression tendency in workers in Internet companies. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2018, 36, 241–246. [Google Scholar]
- Maslach, C.; Leiter, M.P. Early predictors of job burnout and engagement. J. Appl. Psychol. 2008, 93, 498–512. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.; Li, P.; Wildy, H. Health-Promoting Leadership: Concept, Measurement, and Research Framework. Front. Psychol. 2021, 12, 602333. [Google Scholar] [CrossRef]
- Bregenzer, A.; Felfe, J.; Bergner, S.; Jiménez, P. How followers’ emotional stability and cultural value orientations moderate the impact of health-promoting leadership and abusive supervision on health-related resources. Ger. J. Hum. Resour. Manag. 2019, 33, 307–336. [Google Scholar] [CrossRef]
- Franke, F.; Felfe, J.; Pundt, A. The Impact of Health-Oriented Leadership on Follower Health: Development and Test of a New Instrument Measuring Health-Promoting Leadership. Ger. J. Hum. Resour. Manag. 2014, 28, 139–161. [Google Scholar] [CrossRef]
- Vonderlin, R.; Schmidt, B.; Müller, G.; Biermann, M.; Kleindienst, N.; Bohus, M.; Lyssenko, L. Health-Oriented Leadership and Mental Health From Supervisor and Employee Perspectives: A Multilevel and Multisource Approach. Front. Psychol. 2021, 11, 614803. [Google Scholar] [CrossRef]
- Liu, S.; Song, Z.; Xiao, J.; Chen, P. How and When Health-Promoting Leadership Facilitates Employee Health Status: The Critical Role of Healthy Climate and Work Unit Structure. Front. Psychol. 2021, 12, 727887. [Google Scholar] [CrossRef]
- Shuang, L. Influencing Mechanism of Health-Promoting Leadership on Health Human Capital; Southwestern University of Finance and Economics: Chengdu, China, 2018. [Google Scholar]
- Goetzel, R.Z.; Ozminkowski, R.J. The health and cost benefits of work site health-promotion programs. Annu. Rev. Public Health 2008, 29, 303–323. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.E.; Earp, J.A.; Kozma, C.M.; Hertz-Picciotto, I. Effect of organization-level variables on differential employee participation in 10 federal worksite health promotion programs. Health Educ. Q. 1996, 23, 204–223. [Google Scholar] [CrossRef]
- Ribisl, K.M.; Reischl, T.M. Measuring the climate for health at organizations. Development of the worksite health climate scales. J. Occup. Med. 1993, 35, 812–824. [Google Scholar] [CrossRef] [PubMed]
- Buddhaghosa, B. The Path of Purification (Visuddhimagga). Available online: https://www.accesstoinsight.org/lib/authors/nanamoli/PathofPurification2011.pdf (accessed on 16 March 2021).
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Wongpakaran, T. Strength-Based Therapy (SBT): Incorporation of the ‘Great Human Strength’ Concept within the Psychotherapy Model. In Proceedings of the 44th Annual Conference Society of Psychotherapy Research (SPR), Brisbane, Australia, 10–13 July 2013. [Google Scholar]
- Boman, E.; Gustafson, Y.; Häggblom, A.; Santamäki Fischer, R.; Nygren, B. Inner strength—Associated with reduced prevalence of depression among older women. Aging Ment. Health 2015, 19, 1078–1083. [Google Scholar] [CrossRef]
- Viglund, K.; Jonsén, E.; Strandberg, G.; Lundman, B.; Nygren, B. Inner strength as a mediator of the relationship between disease and self-rated health among old people. J. Adv. Nurs. 2014, 70, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Wongpakaran, N.; Wongpakaran, T.; Kuntawong, P. Development and validation of the (inner) Strength-Based Inventory. Ment. Health Relig. Cult. 2020, 23, 263–273. [Google Scholar] [CrossRef]
- Petkari, E.; Ortiz-Tallo, M. Towards Youth Happiness and Mental Health in the United Arab Emirates: The Path of Character Strengths in a Multicultural Population. J. Happiness Stud. 2018, 19, 333–350. [Google Scholar] [CrossRef]
- Brummett, B.H.; Mark, D.B.; Siegler, I.C.; Williams, R.B.; Babyak, M.A.; Clapp-Channing, N.E.; Barefoot, J.C. Perceived social support as a predictor of mortality in coronary patients: Effects of smoking, sedentary behavior, and depressive symptoms. Psychosom. Med. 2005, 67, 40–45. [Google Scholar] [CrossRef]
- Sand, G.; Miyazaki, A. The impact of social support on salesperson burnout and burnout components. Psychol. Mark. 2000, 17, 13–26. [Google Scholar] [CrossRef]
- Chung, Y.J.; Jung, W.C.; Kim, H.; Cho, S.S. Association of Emotional Labor and Occupational Stressors with Depressive Symptoms among Women Sales Workers at a Clothing Shopping Mall in the Republic of Korea: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 1440. [Google Scholar] [CrossRef]
- Cho, J.J.; Kim, J.Y.; Chang, S.J.; Fiedler, N.; Koh, S.B.; Crabtree, B.F.; Kang, D.M.; Kim, Y.K.; Choi, Y.H. Occupational stress and depression in Korean employees. Int. Arch. Occup. Environ. Health 2008, 82, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.B.; Gjerstad, J.; Frone, M. Alcohol use among Norwegian workers: Associations with health and well-being. Occup. Med. 2018, 68, 96–98. [Google Scholar] [CrossRef] [PubMed]
- Boyd, A.; Van de Velde, S.; Vilagut, G.; de Graaf, R.; O’Neill, S.; Florescu, S.; Alonso, J.; Kovess-Masfety, V. Gender differences in mental disorders and suicidality in Europe: Results from a large cross-sectional population-based study. J. Affect Disord. 2015, 173, 245–254. [Google Scholar] [CrossRef] [PubMed]
- McLean, C.P.; Asnaani, A.; Litz, B.T.; Hofmann, S.G. Gender differences in anxiety disorders: Prevalence, course of illness, comorbidity and burden of illness. J. Psychiatr. Res. 2011, 45, 1027–1035. [Google Scholar] [CrossRef]
- National Medical Products Administration. Situation of Chinese Medical Device Manufacturers in 2020; National Medical Products Administration: Beijing, China, 2020. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T.; Lertkachatarn, S.; Sirirak, T.; Kuntawong, P. Core Symptom Index (CSI): Testing for bifactor model and differential item functioning. Int. Psychogeriatr. 2019, 31, 1769–1779. [Google Scholar] [CrossRef]
- Siergist, J. Adverse health effects of high effort-low reward conditions at work. J. Occup. Health Psychol. 1996, 1, 27–43. [Google Scholar]
- Yang, W.; Li, J. Measurement of psychosocial factors in the workplace—Application of two occupational stress detection models. Chin. J. Occup. Health Occup. Dis. 2004, 6, 22–26. [Google Scholar]
- Dai, J.; Yu, H.; Wu, J.; Fu, H. Development of a concise occupational stress questionnaire and construction of an assessment model. Fudan J. (Med. Ed.) 2007, 05, 656–661. [Google Scholar]
- Yu, H. An Empirical Study on Job Burnout from the Aspect of Effort-Reward Imbalance; East China University of Science and Technology: Shanghai, China, 2013. [Google Scholar]
- Köppe, C.; Kammerhoff, J.; Schütz, A. Leader-follower crossover: Exhaustion predicts somatic complaints via StaffCare behavior. J. Manag. Psychol. 2018, 33, 297–310. [Google Scholar] [CrossRef]
- Liu, B. Health-Promotion Leadership: Its Definition, Measurement and Effect on Employees’ Health. China Hum. Resour. Dev. 2016, 15, 48–56. [Google Scholar]
- Basen-Engquist, K.; Hudmon, K.S.; Tripp, M.; Chamberlain, R. Worksite health and safety climate: Scale development and effects of a health promotion intervention. Prev. Med. 1998, 27, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Wang, X.; Wang, X.; Ma, H. An updated version of the Manual of Mental Health Rating Scale. Beijing Chin. J. Ment. Health 1999, 13, 131–133. Available online: http://course.sdu.edu.cn/Download2/112bcc58-8a24-4dbf-a616-13baf72c5fc2.pdf (accessed on 16 May 2022).
- Lei, H.; Li, J.; Zhang, X. The influence of social support on depression in adolescents: An analysis of moderated mediating effects. Psychol. Mon. 2022, 17, 39–42. [Google Scholar]
- Sun, L.; Meng, H.; Zhong, W. Employees’ Core Self-evaluation and Life Satisfaction: The Mediating Role of Perceived Social Support. J. Psychol. Sci. 2014, 37, 1232–1237. [Google Scholar]
- Cotrin, P.; Moura, W.; Gambardela-Tkacz, C.M.; Pelloso, F.C.; Santos, L.D.; Carvalho, M.D.B.; Pelloso, S.M.; Freitas, K.M.S. Healthcare Workers in Brazil during the COVID-19 Pandemic: A Cross-Sectional Online Survey. Inquiry 2020, 57, 46958020963711. [Google Scholar] [CrossRef]
- Hall, B.J.; Li, G.; Chen, W.; Shelley, D.; Tang, W. Prevalence of depression, anxiety, and suicidal ideation during the Shanghai 2022 Lockdown: A cross-sectional study. J. Affect Disord. 2023, 330, 283–290. [Google Scholar] [CrossRef]
- Gan, Y.; Ma, J.; Wu, J.; Chen, Y.; Zhu, H.; Hall, B.J. Immediate and delayed psychological effects of province-wide lockdown and personal quarantine during the COVID-19 outbreak in China. Psychol. Med. 2022, 52, 1321–1332. [Google Scholar] [CrossRef]
- Aknin, L.B.; Andretti, B.; Goldszmidt, R.; Helliwell, J.F.; Petherick, A.; De Neve, J.E.; Dunn, E.W.; Fancourt, D.; Goldberg, E.; Jones, S.P.; et al. Policy stringency and mental health during the COVID-19 pandemic: A longitudinal analysis of data from 15 countries. Lancet Public Health 2022, 7, e417–e426. [Google Scholar] [CrossRef]
- Qian, Z. China to Remove Quarantine for Inbound Travelers Starting January 8, 2023. China Briefing, 27 December 2022. [Google Scholar]
- Xu, W.; Tan, W.; Li, X.; Huang, Z.; Zheng, H.; Hou, C.; Jia, F.; Wang, S. Prevalence and correlates of depressive and anxiety symptoms among adults in Guangdong Province of China: A population-based study. J. Affect Disord. 2022, 308, 535–544. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhou, Y.; Wei, Y.; Zeng, L.; Yang, J.; Li, Y.; Song, X.; Li, H.; He, H.; Li, T.; et al. Differences in the Association of Anxiety, Insomnia and Somatic Symptoms between Medical Staff and the General Population During the Outbreak of COVID-19. Neuropsychiatr. Dis. Treat. 2021, 17, 1907–1915. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Tsai, W.; Kodish, T.; Trung, L.T.; Lau, A.S.; Weiss, B. Cultural variation in temporal associations among somatic complaints, anxiety, and depressive symptoms in adolescence. J. Psychosom. Res. 2019, 124, 109763. [Google Scholar] [CrossRef]
- Kalibatseva, Z.; Leong, F.T.L. Cultural Factors, Depressive and Somatic Symptoms among Chinese American and European American College Students. J. Cross-Cult. Psychol. 2018, 49, 1556–1572. [Google Scholar] [CrossRef]
- Zhang, D. Depression and Culture—A Chinese Perspective. Can. J. Couns. Psychother. 1995, 29, 227–233. [Google Scholar]
- Bekhuis, E.; Boschloo, L.; Rosmalen, J.G.; Schoevers, R.A. Differential associations of specific depressive and anxiety disorders with somatic symptoms. J. Psychosom. Res. 2015, 78, 116–122. [Google Scholar] [CrossRef]
- Lallukka, T.; Mekuria, G.B.; Nummi, T.; Virtanen, P.; Virtanen, M.; Hammarström, A. Co-occurrence of depressive, anxiety, and somatic symptoms: Trajectories from adolescence to midlife using group-based joint trajectory analysis. BMC Psychiatry 2019, 19, 236. [Google Scholar] [CrossRef]
- World Mental Health. Depression. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 12 March 2022).
- Farhane-Medina, N.Z.; Luque, B.; Tabernero, C.; Castillo-Mayén, R. Factors associated with gender and sex differences in anxiety prevalence and comorbidity: A systematic review. Sci. Prog. 2022, 105, 00368504221135469. [Google Scholar] [CrossRef]
- Van Droogenbroeck, F.; Spruyt, B.; Keppens, G. Gender differences in mental health problems among adolescents and the role of social support: Results from the Belgian health interview surveys 2008 and 2013. BMC Psychiatry 2018, 18, 6. [Google Scholar] [CrossRef] [PubMed]
- Delisle, V.C.; Beck, A.T.; Dobson, K.S.; Dozois, D.J.; Thombs, B.D. Revisiting gender differences in somatic symptoms of depression: Much ado about nothing? PLoS ONE 2012, 7, e32490. [Google Scholar] [CrossRef] [PubMed]
- Ernst, C.; Angst, J. The Zurich Study. XII. Sex differences in depression. Evidence from longitudinal epidemiological data. Eur. Arch. Psychiatry Clin. Neurosci. 1992, 241, 222–230. [Google Scholar] [CrossRef]
- Silverstein, B. Gender differences in the prevalence of somatic versus pure depression: A replication. Am. J. Psychiatry 2002, 159, 1051–1052. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Xiong, Y.; Michaëlsson, M.; Michaëlsson, K.; Larsson, S.C. Genetically predicted education attainment in relation to somatic and mental health. Sci. Rep. 2021, 11, 4296. [Google Scholar] [CrossRef]
- Chang-Quan, H.; Zheng-Rong, W.; Yong-Hong, L.; Yi-Zhou, X.; Qing-Xiu, L. Education and risk for late life depression: A meta-analysis of published literature. Int. J. Psychiatry Med. 2010, 40, 109–124. [Google Scholar] [CrossRef]
- Anderson, E.L.; Howe, L.D.; Wade, K.H.; Ben-Shlomo, Y.; Hill, W.D.; Deary, I.J.; Sanderson, E.C.; Zheng, J.; Korologou-Linden, R.; Stergiakouli, E.; et al. Education, intelligence and Alzheimer’s disease: Evidence from a multivariable two-sample Mendelian randomization study. Int. J. Epidemiol. 2020, 49, 1163–1172. [Google Scholar] [CrossRef]
- Davies, N.M.; Hill, W.D.; Anderson, E.L.; Sanderson, E.; Deary, I.J.; Davey Smith, G. Multivariable two-sample Mendelian randomization estimates of the effects of intelligence and education on health. eLife 2019, 8, e43990. [Google Scholar] [CrossRef]
- Roche. Sales Representative—Diagnostic. Available online: https://careers.roche.com/global/en/job/ROCHGLOBAL202305111374EXTERNALENGLOBAL/Sales-Representative-Diagnostic (accessed on 1 June 2022).
- Dixon, J.M.; Banwell, C.; Strazdins, L.; Corr, L.; Burgess, J. Flexible employment policies, temporal control and health promoting practices: A qualitative study in two Australian worksites. PLoS ONE 2019, 14, e0224542. [Google Scholar] [CrossRef]
- Halpern, D. How time-flexible work policies can reduce stress, improve health, and save money. Stress Health 2005, 21, 157–168. [Google Scholar] [CrossRef]
- Yong, X.; Gao, X.; Zhang, Z.; Ge, H.; Sun, X.; Ma, X.; Liu, J. Associations of occupational stress with job burn-out, depression and hypertension in coal miners of Xinjiang, China: A cross-sectional study. BMJ Open 2020, 10, e036087. [Google Scholar] [CrossRef]
- Blackmore, E.; Stansfeld, S.; Weller, I.; Munce, S.; Zagorski, B.; Stewart, D. Major Depressive Episodes and Work Stress: Results From a National Population Survey. Am. J. Public Health 2007, 97, 2088–2093. [Google Scholar] [CrossRef]
- Keser, A.; Li, J.; Siegrist, J. Examining Effort–Reward Imbalance and Depressive Symptoms Among Turkish University Workers. Workplace Health Saf. 2018, 67, 131–136. [Google Scholar] [CrossRef]
- Zweber, Z.M.; Henning, R.A.; Magley, V.J. A practical scale for Multi-Faceted Organizational Health Climate Assessment. J. Occup. Health Psychol. 2016, 21, 250–259. [Google Scholar] [CrossRef]
- Schulz, H.; Zacher, H.; Lippke, S. The Importance of Team Health Climate for Health-Related Outcomes of White-Collar Workers. Front. Psychol. 2017, 8, 74. [Google Scholar] [CrossRef]
- Sonnentag, S.; Pundt, A. Organisational health behavior climate: Organisations can encourage healthy eating and physical exercise. Appl. Psychol. 2016, 65, 259–286. [Google Scholar] [CrossRef]
- Wongpakaran, T.; Yang, T.; Varnado, P.; Siriai, Y.; Mirnics, Z.; Kövi, Z.; Wongpakaran, N. The development and validation of a new resilience inventory based on inner strength. Sci. Rep. 2023, 13, 2506. [Google Scholar] [CrossRef] [PubMed]
- Moe, A.; Hellzen, O.; Ekker, K.; Enmarker, I. Inner strength in relation to perceived physical and mental health among the oldest old people with chronic illness. Aging Ment. Health 2013, 17, 189–196. [Google Scholar] [CrossRef]
- Lundman, B.; Aléx, L.; Jonsén, E.; Norberg, A.; Nygren, B.; Santamäki Fischer, R.; Strandberg, G. Inner strength—A theoretical analysis of salutogenic concepts. Int. J. Nurs. Stud. 2010, 47, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Zamanian, H.; Amini-Tehrani, M.; Jalali, Z.; Daryaafzoon, M.; Ala, S.; Tabrizian, S.; Foroozanfar, S. Perceived social support, coping strategies, anxiety and depression among women with breast cancer: Evaluation of a mediation model. Eur. J. Oncol. Nurs. 2021, 50, 101892. [Google Scholar] [CrossRef] [PubMed]
- Eom, C.S.; Shin, D.W.; Kim, S.Y.; Yang, H.K.; Jo, H.S.; Kweon, S.S.; Kang, Y.S.; Kim, J.H.; Cho, B.L.; Park, J.H. Impact of perceived social support on the mental health and health-related quality of life in cancer patients: Results from a nationwide, multicenter survey in South Korea. Psychooncology 2013, 22, 1283–1290. [Google Scholar] [CrossRef]
- Saikkonen, S.; Karukivi, M.; Vahlberg, T.; Saarijärvi, S. Associations of social support and alexithymia with psychological distress in Finnish young adults. Scand. J. Psychol. 2018, 59, 602–609. [Google Scholar] [CrossRef]
- Barrech, A.; Riedel, N.; Li, J.; Herr, R.M.; Mörtl, K.; Angerer, P.; Gündel, H. The long-term impact of a change in Effort–Reward imbalance on mental health—Results from the prospective MAN-GO study. Eur. J. Public Health 2017, 27, 1021–1026. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Mean (SD) or n (%) |
|---|---|
| Age, n (%) | |
| 18–24 | 34 (13.9) |
| 25–34 | 130 (53.3) |
| 35–44 | 67 (27.5) |
| 44–54 | 11 (4.5) |
| 54 and order | 2 (0.8) |
| Gender, n (%) | |
| Male | 126 (51.6) |
| Female | 118 (48.4) |
| Financial status, n (%) | |
| Not enough income or incurring debt | 19 (7.8) |
| Barely sufficient income, adequate income without debt | 102 (41.8) |
| Enough income without savings | 56 (23.0) |
| Enough income with some savings | 67 (27.4) |
| Alcohol use, n (%) | |
| Yes | 100 (41.2) |
| No | 143 (58.8) |
| Educational, n (%) | |
| Bachelor’s degree or below | 195 (79.9) |
| Master’s degree or above | 49 (20.1) |
| Job experience, n (%) | |
| Less than a year | 52 (21.4) |
| 1–3 years | 85 (35.0) |
| 4–6 years | 57 (23.4) |
| More than 6 years | 49 (20.2) |
| Marital status, n (%) | |
| Single | 108 (44.3) |
| Married/living together/cohabiting | 134 (54.9) |
| Divorced/separated | 2 (0.8) |
| Occupational factors | |
| Sales target, n (%) | |
| Easily achievable | 74 (30.4) |
| Difficult to achieve | 152 (62.6) |
| Not achievable | 17 (7.0) |
| Frequency of business trip, n (%) | |
| 0 trips/year | 98 (40.2) |
| 1–3 trips/year | 101 (41.4) |
| >3 trips/year | 45 (18.4) |
| Workload during COVID-19, n (%) | |
| Significantly decreased | 55 (22.5) |
| Decreased | 40 (16.4) |
| Not changed | 37 (15.2) |
| Increased | 74 (30.3) |
| Significantly increased | 38 (15.6) |
| Effort–reward imbalance (>1 imbalance), n (%) | 78 (32.0) |
| Organizational factors | |
| Health-promoting leadership (range 0–15) | 9.79 (2.63) |
| Health climate (range 0–25) | 17.21 (3.96) |
| Psychological factors | |
| Inner strength (range 10–50) | 31.18 (8.08) |
| Perceived social support–total score (range 12–84) | 54.36 (13.44) |
| Perceived social support from significant others (mean scores range 1–7) | 4.43 (1.20) |
| Perceived social support from family members (mean scores range 1–7) | 4.48 (1.16) |
| Perceived social support from friends (mean scores range 1–7) | 4.57 (1.27) |
| Mental health outcomes, n (%) and mean (SD) | |
| CSI total score (range 0–60) | 12.89 (10.68) |
| CSI-depression score (range 0–18) | 4.69 (4.11) |
| CSI-anxiety score (range 0–13) | 3.81 (3.00) |
| CSI-somatization (somatic symptoms) (range 0–17) | 4.38 (4.32) |
| Major depression (CSI depression score ≥ 9), n (%) | 45 (18.4) |
| Anxiety disorder (CSI anxiety score ≥ 9), n (%) | 25 (10.2) |
| Variables | n (%) | CSI Total Score | Anxiety Score | Somatic Score | Major Depression | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age | Mean ± SD | p-Value | Mean ± SD | p-Value | Mean ± SD | p-Value | Non-MD N (%) | MD N (%) | p-Value | |
| 35 or older | 80 (32.8) 164 (67.2) | 10.36 ± 9.88 14.13 ± 10.87 | 0.009 | 2.98 ± 2.82 4.23 ± 3.20 | 0.003 | 3.91 ± 4.23 4.61 ± 4.36 | 0.238 | 71 (35.7) 128 (64.3) | 9 (20.0) 36 (80.0) | 0.053 |
| 18–34 years | ||||||||||
| Gender | ||||||||||
| Male | 126 (51.6) 118 (48.4) | 10.05 ± 8.54 15.93 ± 11.88 | <0.001 | 3.17 ± 2.49 4.51 ± 3.57 | <0.001 | 3.34 ± 3.61 5.49 ± 4.74 | <0.001 | 116 (58.3) 83 (41.7) | 10 (22.2) 35 (77.8) | <0.001 |
| Female | ||||||||||
| Financial status | ||||||||||
| Sufficient income | 123 (50.4) 121 (49.6) | 11.01 ± 10.11 14.80 ± 10.95 | 0.005 | 3.37 ± 2.98 4.26 ± 3.23 | 0.026 | 3.77 ± 4.01 5.00 ± 4.55 | 0.026 | 109 (54.8) 90 (45.2) | 14 (31.1) 31 (68.9) | 0.005 |
| Insufficient income | ||||||||||
| Alcohol use | ||||||||||
| No Yes | 143 (58.8) 100 (41.2) | 12.20 ± 10.19 13.88 ± 11.39 | 0.230 | 3.66 ± 2.95 4.06 ± 3.39 | 0.326 | 4.10 ± 4.21 4.76 ± 4.49 | 0.247 | 120 (60.6) 78 (39.4) | 23 (51.1) 22 (48.9) | 0.246 |
| Education | ||||||||||
| Bachelor’s degree or below | 195 (79.9) 49 (20.1) | 13.27 ± 10.84 11.41 ± 10.02 | 0.277 | 3.85 ± 3.11 3.67 ± 3.23 | 0.723 | 4.66 ± 4.41 3.27 ± 3.78 | 0.043 | 158 (79.4) 41 (20.6) | 37 (82.2) 8 (17.8) | 0.837 |
| Master’s degree or above | ||||||||||
| Job experience | ||||||||||
| More than 1 year | 191 (78.6) 52 (21.4) | 12.25 ± 10.26 15.13 ±12.02 | 0.085 | 3.67 ± 3.05 4.33 ± 3.41 | 0.181 | 4.19 ± 4.19 5.08 ± 4.79 | 0.190 | 165 (82.9) 34 (17.1) | 26 (59.1) 18 (40.9) | <0.001 |
| Less than a year | ||||||||||
| Marital status | ||||||||||
| In relationship | 134 (54.9) 110 (45.1) | 11.31 ± 10.14 14.82 ± 11.05 | 0.010 | 3.36 ± 2.98 4.37 ± 3.23 | 0.012 | 4.07 ± 4.34 4.76 ± 4.29 | 0.211 | 113 (56.8) 86 (43.2) | 21 (46.7) 24 (53.3) | 0.247 |
| Single | ||||||||||
| Frequency of business trips | ||||||||||
| 0 trips/year | 199 (81.6) 45 (18.4) | 13.48 ± 10.81 10.29 ± 9.82 | 0.070 | 3.98 ± 3.14 3.09 ± 3.03 | 0.085 | 4.48 ± 4.35 3.96 ± 4.23 | 0.466 | 158 (79.4) 41 (20.6) | 41 (91.1) 4 (8.9) | 0.087 |
| >1 trips/year | ||||||||||
| Workload during COVID-19 | ||||||||||
| Decreased or not changed | 132 (54.1) 112 (45.9) | 13.27 ± 10.24 12.45 ± 11.21 | 0.055 | 3.80 ± 3.09 3.83 ± 3.19 | 0.946 | 4.89 ± 4.10 3.78 ± 4.50 | 0.044 | 105 (52.8) 94 (47.2) | 27 (60.0) 18 (40.0) | 0.411 |
| Increased | ||||||||||
| Sales target | ||||||||||
| Easy to achieve | 74 (30.5) 169 (69.5) | 12.28 ± 10.49 13.12 ± 10.81 | 0.574 | 3.36± 3.06 4.00 ± 3.16 | 0.143 | 4.89 ± 4.31 4.15 ± 4.33 | 0.222 | 63 (31.7) 136 (68.3) | 11 (25.0) 33 (75.0) | 0.470 |
| Difficult or not achievable | ||||||||||
| Variable | CSI | Depression | Anxiety | Somatic | ERI | HPL | HC | SBI | MSPSS Total | MSPSS— Family | MSPSS— Friends | MSPSS—SO |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CSI | 1 | |||||||||||
| Depression | 0.928 ** | 1 | ||||||||||
| Anxiety | 0.915 ** | 0.798 ** | 1 | |||||||||
| Somatic symptom | 0.926 ** | 0.763 ** | 0.778 ** | 1 | ||||||||
| ERI | 0.310 ** | 0.361 ** | 0.320 ** | 0.192 ** | 1 | |||||||
| HPL | −0.092 | −0.113 | −0.085 | −0.059 | −0.126 * | 1 | ||||||
| HC | −0.115 | −0.132 * | −0.053 | −0.120 | −0.096 | 0.743 ** | 1 | |||||
| SBI | −0.300 ** | −0.306 ** | −0.278 ** | −0.248 ** | −0.240 ** | 0.537 ** | 0.534 ** | 1 | ||||
| MSPSS—Total | −0.195 ** | −0.186 ** | −0.194 ** | −0.166 ** | −0.012 | 0.550 ** | 0.546 ** | 0.481 ** | 1 | |||
| MSPSS—family members | −0.228 ** | −0.237 ** | −0.223 ** | −0.176 ** | −0.044 | 0.529 ** | 0.534 ** | 0.411 ** | 0.896 ** | 1 | ||
| MSPSS—friends | −0.147 * | −0.128 * | −0.165 ** | −0.121 | 0.014 | 0.490 ** | 0.449 ** | 0.421 ** | 0.932 ** | 0.816 ** | 1 | |
| MSPSS—significant others | −0.163 * | −0.153 * | −0.164 * | −0.139 * | −0.035 | 0.535 ** | 0.549 ** | 0.469 ** | 0.921 ** | 0.726 ** | 0.781 ** | 1 |
| Variable | Predictor | B | SE | β | p | 95% LL-CI | 95% UL-CI |
|---|---|---|---|---|---|---|---|
| CSI total score *** | Age | 1.502 | 1.497 | 0.066 | 0.317 | −1.447 | 4.451 |
| Gender | 3.898 | 1.285 | 0.183 | 0.003 | 1.366 | 6.430 | |
| Marital status | 0.021 | 1.416 | 0.001 | 0.988 | −2.768 | 2.809 | |
| Financial status | −0.233 | 1.328 | −0.011 | 0.861 | −2.849 | 2.384 | |
| ERI–score | 7.132 | 1.352 | 0.312 | 0.000 | 4.468 | 9.795 | |
| SBI–score | −0.217 | 0.091 | −0.164 | 0.018 | −0.395 | −0.038 | |
| MSPSS–total score | −0.091 | 0.053 | −0.114 | 0.086 | −0.195 | 0.013 | |
| Major depression ** | Age | −0.629 | 0.501 | 1.875 | 0.209 | 0.703 | 5.003 |
| Gender | −1.399 | 0.443 | 4.052 | 0.002 | 1.702 | 9.647 | |
| Job experience | −0.725 | 0.441 | 2.065 | 0.100 | 0.870 | 4.900 | |
| Financial status | −0.083 | 0.432 | 1.086 | 0.848 | 0.465 | 2.535 | |
| ERI–score | −1.988 | 0.434 | 7.303 | 0.000 | 3.119 | 17.103 | |
| SBI–score | −0.083 | 0.032 | 0.920 | 0.009 | 0.865 | 0.979 | |
| MSPSS–total score | −0.028 | 0.016 | 0.973 | 0.087 | 0.942 | 1.004 | |
| Anxiety score *** | Age | 0.704 | 0.450 | 0.106 | 0.119 | −0.181 | 1.590 |
| Gender | 0.813 | 0.386 | 0.130 | 0.036 | 0.053 | 1.574 | |
| Marital status | −0.011 | 0.425 | −0.002 | 0.980 | −0.848 | 0.827 | |
| Financial status | −0.236 | 0.399 | −0.038 | 0.554 | −1.022 | 0.550 | |
| ERI–score | 1.958 | 0.406 | 0.292 | 0.000 | 1.158 | 2.758 | |
| SBI–score | −0.059 | 0.027 | −0.152 | 0.031 | −0.113 | −0.005 | |
| MSPSS–total score | −0.029 | 0.016 | −0.124 | 0.069 | −0.060 | 0.002 | |
| Somatic score *** | Gender | 1.508 | 0.536 | 0.175 | 0.005 | 0.451 | 2.565 |
| Education | −1.301 | 0.647 | −0.121 | 0.046 | −2.576 | −0.025 | |
| Financial status | −0.243 | 0.551 | −0.028 | 0.659 | −1.328 | 0.842 | |
| Workload during COVID-19 | −1.056 | 0.542 | −0.122 | 0.052 | −2.123 | 0.011 | |
| ERI–score | 2.454 | 0.570 | 0.265 | 0.000 | 1.332 | 3.577 | |
| SBI–score | −0.078 | 0.038 | −0.146 | 0.039 | −0.153 | −0.004 | |
| MSPSS–total score | −0.023 | 0.022 | −0.073 | 0.289 | −0.067 | 0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mao, B.; Kanjanarat, P.; Wongpakaran, T.; Permsuwan, U.; O’Donnell, R. Factors Associated with Depression, Anxiety, and Somatic Symptoms among International Salespeople in the Medical Device Industry: A Cross-Sectional Study in China. Healthcare 2023, 11, 2174. https://doi.org/10.3390/healthcare11152174
Mao B, Kanjanarat P, Wongpakaran T, Permsuwan U, O’Donnell R. Factors Associated with Depression, Anxiety, and Somatic Symptoms among International Salespeople in the Medical Device Industry: A Cross-Sectional Study in China. Healthcare. 2023; 11(15):2174. https://doi.org/10.3390/healthcare11152174
Chicago/Turabian StyleMao, Beibei, Penkarn Kanjanarat, Tinakon Wongpakaran, Unchalee Permsuwan, and Ronald O’Donnell. 2023. "Factors Associated with Depression, Anxiety, and Somatic Symptoms among International Salespeople in the Medical Device Industry: A Cross-Sectional Study in China" Healthcare 11, no. 15: 2174. https://doi.org/10.3390/healthcare11152174
APA StyleMao, B., Kanjanarat, P., Wongpakaran, T., Permsuwan, U., & O’Donnell, R. (2023). Factors Associated with Depression, Anxiety, and Somatic Symptoms among International Salespeople in the Medical Device Industry: A Cross-Sectional Study in China. Healthcare, 11(15), 2174. https://doi.org/10.3390/healthcare11152174