

Effectiveness of a Therapeutic Educational Oral Health Program for Persons with Schizophrenia: A Cluster Randomized Controlled Trial and Qualitative Approach



 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Study Design
2.2. Intervention
2.3. Recruitment of Centres and Participants
2.4. Randomization
2.5. Outcomes
2.6. Analysis
2.7. Ethics
3. Results
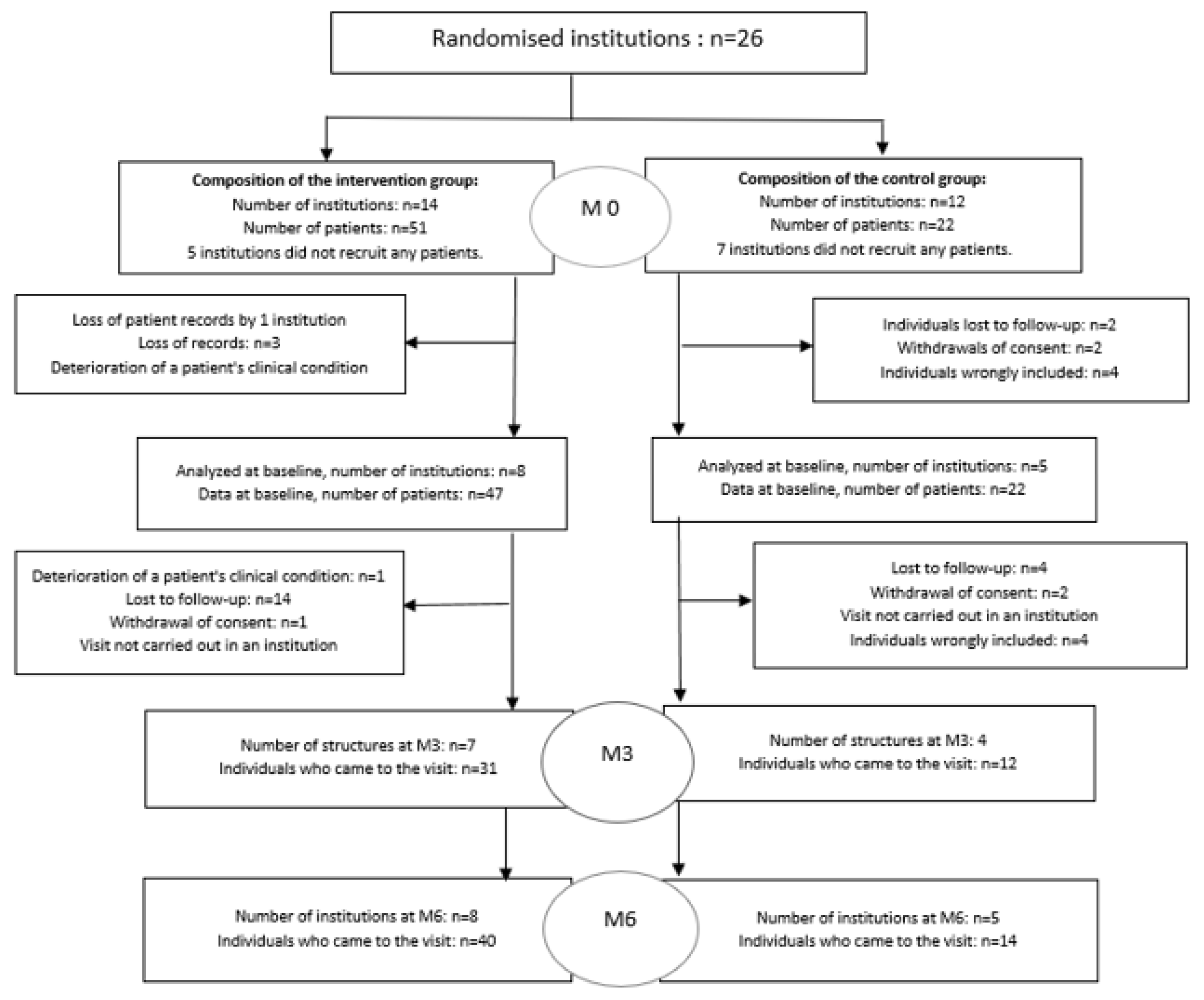
3.1. Results of the Cluster-Randomised Controlled Trial
3.2. Description of Study Population for the Cluster Randomized Controlled Trial
3.3. Description of the Assessment Criteria
3.4. Results of the Qualitative Study
3.4.1. The Organization and Coordination of the Programme
We included people but they were at the limit of the study. (…) I know that we had difficulty finding patients who met the criteria. (…) There were those who met the criteria for the number of teeth but some were too delirious to answer the questionnaires.(A nurse)
Our manager really carried the organisation of this study at arm’s length…it took a lot of work to contact the patients, to make the panoramic X-rays, to organise the appointments.(A nurse)
There were really no difficulties in setting up this Ebene Protocol. All the documents we had were very clear, and the patients agreed… There was really no difficulty at all.(A nurse)
Yes, it was good because with our patients it should not be too close or too far away because after a while, they forget…(A health care manager)
3.4.2. The Way in Which the Patients Mobilized for the Program
They were actually happy. Some of them were obliged to come in addition to what they usually did in the day hospital. We didn’t really need to remind them…it showed their motivation, because we ourselves, for certain types of care, when they are not motivated, they find excuses not to come… Whereas in your study, I think there were never any absentees… This is an indicator that shows that they were happy with this care.(A health care manager)
Everyone really took their appointments with great seriousness. With this pride in brushing their teeth well, in maintaining the level of hygiene.(A Nurse)
3.4.3. The Programme Effects
We give toothbrushes …so there are already things that exist… In most bathrooms they have posters on how to brush their teeth.(A Nurse)
I didn’t see any effect on the patients, and when I talked to the patients who are part of the study, there was no change in their tooth brushing habits… we tried to mobilise them… they say ‘yes we know’ but they didn’t do it.(A Nurse)
For some it was easier to go to the dentist after the TEPOH. So that’s already a big positive… It took away the fear of the dentist…(A health care manager)
It was interesting because they were proud afterwards to have maintained their level of good dental health.(A Nurse)
it made it possible, after EBENE, to propose to a patient at least once a week to brush his teeth.…(A Nurse)
The idea is that what we bring to them in psychoeducation in our workshops has an impact at home.(A Nurse)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Denis, F.; Goueslard, K.; Siu-Paredes, F.; Amador, G.; Rusch, E.; Bertaud, V.; Quantin, C. Oral health treatment habits of people with schizophrenia in France: A retrospective cohort study. PLoS ONE 2020, 15, e0229946. [Google Scholar] [CrossRef] [PubMed]
- Kisely, S.; Baghaie, H.; Lalloo, R.; Siskind, D.; Johnson, N.W. A systematic review and meta-analysis of the association between poor oral health and severe mental illness. Psychosom Med. 2015, 77, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Wey, M.C.; Loh, S.; Doss, J.G.; Abu Bakar, A.K.; Kisely, S. The oral health of people with chronic schizophrenia: A neglected public health burden. Aust. N. Z. J. Psychiatry 2015, 50, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Persson, K.; Olin, E.; Ostman, M. Oral health problems and support as experienced by people with severe mental illness living incommunity-based subsidised housing a qualitative study. Health Soc. Care Community 2010, 18, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, A.M.; Horvitz-Lennon, M.; Post, E.P.; McCarthy, J.F.; Cruz, M.; Welsh, D.; Blow, F.C. Oral health in Veterans Affairs patients diagnosed with serious mental illness. J. Public Health Dent. 2007, 67, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Grisso, T.; Appelbaum, P.S. Comparison of standards for assessing patients’ capacities to make treatment decisions. Am. J. Psychiatry 1995, 15, 1033–1037. [Google Scholar]
- Arnaiz, A.; Zumárraga, M.; Díez-Altuna, I.; Uriarte, J.J.; Moro, J.; Pérez-Ansorena, M.A. Oral health and the symptoms of schizophrenia. Psychiatry Res. 2011, 188, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Joukamaa, M.; Heliövaara, M.; Knekt, P.; Aromaa, A.; Raitasalo, R.; Lehtinen, V. Schizophrenia, neuroleptic medication and mortality. Br. J. Psychiatry J. Ment. Sci. 2006, 188, 122–127. [Google Scholar] [CrossRef]
- Suvisaari, J.; Partti, K.; Perälä, J.; Viertiö, S.; Saarni, S.E.; Lönnqvist, J.; Saarni, S.I.; Härkänen, T. Mortality and its determinants in people with psychotic disorder. Psychosom. Med. 2013, 75, 60–67. [Google Scholar] [CrossRef]
- Newcomer, J.W.; Hennekens, C.H. Severe mental illness and risk of cardiovascular disease. JAMA 2007, 298, 1794. [Google Scholar] [CrossRef]
- Jablensky, A. Epidemiology of schizophrenia: The global burden of disease and disability. Eur. Arch. Psychiatry Clin. Neurosci. 2000, 250, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Jachuck, S.; Brierley, H.; Willcox, P. The effect of hypotensive drugs on quality of life. J. R. Coll. Gen. Pract. 1982, 32, 103–105. [Google Scholar] [PubMed]
- Attkisson, C.; Cook, J.; Karno, M.; Lehman, A.; McGlashan, T.H.; Meltzer, H.Y.; O’Connor, M.; Richardson, D.; Rosenblatt, A.; Wells, K.; et al. Clinical services research. Schizophr. Bull. 1992, 18, 561–626. [Google Scholar] [CrossRef] [PubMed]
- Denis, F.; Siu-Paredes, F.; Maitre, Y.; Amador, G.; Rude, N. A qualitative study on experiences of persons with schizophrenia in oral-health-related quality of life. Braz. Oral Res. 2021, 22, e050. [Google Scholar] [CrossRef]
- Gremyr, A.; Andersson Gäre, B.; Thor, J.; Elwyn, G.; Batalden, P.; Andersson, A.C. The role of co-production in Learning Health Systems. Int. J. Qual. Health Care 2021, 33 (Suppl. 2), ii26–ii32. [Google Scholar] [CrossRef]
- Denis, F.; Millot, I.; Abello, N.; Carpentier, M.; Peteuil, A.; Soudry-Faure, A. Study protocol: A cluster randomized controlled trial to assess the effectiveness of a therapeutic educational program in oral health for persons with schizophrenia. Int. J. Ment. Health Syst. 2016, 10, 65. [Google Scholar] [CrossRef]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA; London, UK; New Delhi, India, 2000; pp. 125–155. [Google Scholar]
- Rat, C.; Peteuil, A.; Reynaud, M.; Millot, I.; Carpentier, M.; Soudry-Faure, A.; Denis, F. Un partenariat patients schizophrènes-soignants pour conduire un programme d’éducation en santé orale [A caregiver-person with schizophrenia partnership to improve oral health education]. Sante Publique 2019, 31, 405–415. [Google Scholar] [CrossRef]
- Peteuil, A.; Rat, C.; Moussa-Badran, S.; Carpentier, M.; Pelletier, J.F.; Denis, F. A Therapeutic Educational Program in Oral Health for Persons with Schizophrenia: A Qualitative Feasibility Study. Int. J. Dent. 2018, 2018, 6403063. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Desk Reference to the Diagnostic Criteria from DSM-5; American Psychiatric Association: Rosslyn, VA, USA, 2013. [Google Scholar]
- Ainamo, J.; Barmes, D.; Beagrie, G.; Cutress, T.; Martin, J.; Sardo-Infirri, J. Development of the World Health Organization (WHO) community periodontal index of treatment needs (CPITN). Int. Dent. J. 1982, 32, 281–291. [Google Scholar] [PubMed]
- Greene, J.G.; Vermilion, J.R. 1960. Available online: http://www.mah.se (accessed on 25 March 2016).
- Caries Process and Prevention Strategies: Epidemiology Continuing Education Course Dentalcare.com Course Pages DentalCare.com. Available online: http://www.dentalcare.com (accessed on 25 March 2016).
- Denis, F.; Hamad, M.; Trojak, B.; Tubert-Jeannin, S.; Rat, C.; Pelletier, J.F.; Rude, N. Psychometric characteristics of the “General Oral Health Assessment Index (GOHAI)” in a French representative sample of patients with schizophrenia. BMC Oral Health 2017, 17, 75. [Google Scholar] [CrossRef]
- Boyer, L.; Simeoni, M.-C.; Loundou, A.; D’Amato, T.; Reine, G.; Lancon, C.; Auquier, P. The development of the S-QoL 18: A shortened quality of life questionnaire for patients with schizophrenia. Schizophr. Res. 2010, 121, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T. Inventaire de Dépression de Beck, 2nd ed.; Manuel du BDI-II. les Éd. du Centre de Psychologie Appliquée (Ed.): Paris, France, 1996. [Google Scholar]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research:Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.C.; Bland, R.C.; Thompson, A.H. Long Term Course and Outcome in Schizophrenia: A 34 Year Follow-up Study in Alberta, Canada. Psychol. Med. 2012, 42, 2137–2143. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.C.; Dudgeon, P.; McGorry, P.D.; Jackson, H.J. The dimensionality of schizophrenia concepts in first-episode psychosis. Acta Psychiatr. Scand. 1998, 97, 334–342. [Google Scholar] [CrossRef]
- Verdoux, H. The current state of adult mental health care in France. Eur. Arch. Psychiatry Clin. Neurosci. 2007, 257, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030. Available online: https://www.who.int/publications-detail-redirect/9789240061484 (accessed on 18 June 2023).
- WHO; Health and Welfare Canada; Canadian Public Health Association. Ottawa Charter for Health Promotion: An International Conference on Health Promotion—The Move Towards a New Publichealth, 17–21 November 1986, Ottawa, ON, Canada; WHO: Geneva, Switzerland, 1986. [Google Scholar]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Pelto-Piri, V.; Engström, K.; Engström, I. Paternalism, autonomy and reciprocity: Ethical perspectives in encounters with patients in psychiatric in-patient care. BMC Med. Ethics 2013, 14, 49. [Google Scholar] [CrossRef]
- Guibet Lafaye, C. Pour une typologie des médecins psychiatres. L’information Psychiatrique 2016, 92, 453–465. [Google Scholar]
- Kane, H.; Baumgart, J.G.; Rusch, E.; Deloyer, J.; Fuenzalida, C.; Kelemen, G.; Krzystanek, M.; Marazziti, D.; Moraitou, M.; Reunanen, M.; et al. The impact of COVID-19 on psychiatric and mental health services in Europe: Suffering experienced by professionals. BMC Health Serv. Res. 2022, 22, 1360. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Taylor, G.W.; Borgnakke, W.S. Parodontal disease: Associations with diabetes, glycemic control and complications. Oral Dis. 2008, 3, 191–203. [Google Scholar] [CrossRef] [PubMed]
- Cutress, T.W.; Ainamo, J.; Sardo-Infirri, J. The community periodontal index of treatment needs (CPITN) procedure for population groups and individuals. Int. Dent. J. 1987, 37, 222–233. [Google Scholar] [PubMed]
- Greenstein, G.; Caton, J. Periodontal disease activity: A critical assessment. J Periodontol. 1990, 61, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Denis, F.; Rouached, I.; Siu-Paredes, F.; Delpierre, A.; Amador, G.; El-Hage, W.; Rude, N. Psychometric Properties of the Schizophrenia Oral Health Profile: Preliminary Results. Int. J. Environ. Res. Public Health 2021, 18, 9090. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Persons who have provided consent | Persons not covered by national health insurance |
| Persons of either sex over 18 years of age | Persons not stabilized from a psychiatric viewpoint or persons in an acute psychiatric episode |
| Persons with diagnosis of schizophrenia as defined in the Diagnostic and Statistical Manual of Mental Disorders-Fifth edition (DSM-5) | Pregnant or breast-feeding women Edentulous persons Persons hospitalized under stress |
| Receiving care in hospital (in- or outpatient) | Cannot understand or have a poor understanding of French Patients with risk of infective endocarditis a or major risk of superinfection People undergoing chemotherapy |
| Scale | Expected Findings Out |
|---|---|
| Global Oral Health Assessment Index (GOHAI) | To detect changes in oral health related quality of life |
| Schizophrenia Quality of Life Scale (S-QoL) | To detect changes that patient experience in quality of life of PWS |
| Beck Depression Inventory | To screen for and measure the severity of depressive symptoms. Depressive symptoms are strongly associated with poor oral health |
| Overall | Intervention Group | Control Group | |
|---|---|---|---|
| Characteristics | n = 69 | n = 47 | n = 22 |
| Age, years, mean ± sd | 44.4 ± 11.6 | 44.3 ± 11.3 | 44.7 ± 12.5 |
| Female, n (%) | 25 (36.2) | 17 (36.2) | 8 (36.4) |
| Body mass index, mean ± sd | 30.0 ± 6.3 | 29.3 ± 5.6 | 31.5 ± 7.6 |
| Lifestyle, n (%) | |||
| In couple or cohabitation | 19 (27.5) | 17 (36.2) | 2 (9.1) |
| Alone | 32 (46.4) | 23 (48.9) | 9 (40.9) |
| Institution | 18 (26.1) | 7 (14.9) | 11 (50.0) |
| Level of study a, n (%) | |||
| Primary level | 14 (20.6) | 8 (17.4) | 6 (27.3) |
| Secondary level and above | 54 (79.4) | 38(82.6) | 16 (72.7) |
| Time to care b, n (%) | |||
| Less than 5 years | 18 (26.9) | 13 (27.7) | 5 (25.0) |
| Between 5 and 15 years old | 18 (26.9) | 9 (19.1) | 9 (45.0) |
| More than 15 years | 31 (46.2) | 25 (53.2) | 6 (30.0) |
| CPI score, mean ± sd | 2.0 ± 1.2 | 2.3 ± 1.2 | 1.6 ± 1.1 |
| CPI score ≥ 3, n (%) | 22 (31.9) | 20 (42.5) | 2 (9.1) |
| CPITN, n (%) | |||
| TNO | 10 (14.5) | 5 (10.6) | 5 (22.7) |
| TN1 | 8 (11.6) | 5 (10.6) | 3 (13.6) |
| TN2 | 42 (60.9) | 29 (61.7) | 13 (59.1) |
| TN3 | 9 (13.0) | 8 (17.0) | 1 (4.6) |
| DMFT score, mean ± sd | 18.1 ± 8.2 | 17.6 ± 7.3 | 19.1 ± 9.9 |
| D | 2.9 ± 3.8 | 3.4 ± 4.1 | 1.9 ± 2.9 |
| M | 8.8 ± 7.1 | 7.7 ± 5.7 | 11.1 ± 9.3 |
| FT | 6.1 ± 5.1 | 6.2 ± 4.3 | 5.9 ± 6.5 |
| OHIS d Score, mean ± sd | 2.2 ± 1.2 | 2.2 ± 1.1 | 2.3 ± 1.3 |
| SQOL c Score, mean ± sd | 59.5 ± 11.1 | 60.5 ± 9.8 | 57.2 ± 13.6 |
| GOHAI e Score, mean ± sd | 47.3 ± 7.5 | 47.1 ± 7.3 | 47.8 ± 8.1 |
| Beck f Score, mean ± sd | 8.6 ± 7.2 | 8.6 ± 7.1 | 8.4 ± 7.7 |
| Frequency of visits to the dentist, n (%) | |||
| More than once a year | 13 (18.8) | 7 (14.9) | 6 (27.3) |
| occasional | 37 (53.6) | 24 (51.1) | 13 (59.1) |
| Never | 19 (27.5) | 16 (34.0) | 3 (13.6) |
| Frequency of brushing teeth, n(%) | |||
| Every day | 48 (69.6) | 31 (66.0) | 17 (77.3) |
| Less than once a day | 13 (18.8) | 11 (23.4) | 2 (9.1) |
| Never | 8 (11.6) | 5 (10.6) | 3 (13.6) |
| Consumption of soft drinks | |||
| Every day | 17 (24.6) | 10 (21.3) | 7 (31.8) |
| occasional | 37 (53.7) | 25 (53.2) | 12 (54.6) |
| Never | 15 (21.7) | 12 (25.5) | 3 (13.6) |
| Alcohol consumption g, n (%) | |||
| Every day | 2 (3.0) | 0 | 2 (9.1) |
| occasional | 17 (25.8) | 13 (29.5) | 4 (18.2) |
| Never | 47 (71.2) | 31 (70.5) | 16 (72.7) |
| Tobacco use, n (%) | 37 (53.6) | 27 (57.4) | 10 (45.4) |
| Recreational drug use, n (%) | 2 (2.9) | 2(4.3) | 0 |
| Snacking between meals, n (%) | |||
| Every day | 20 (29.0) | 12 (25.5) | 8 (36.4) |
| occasional | 34 (49.3) | 24 (51.1) | 10 (45.5) |
| Never | 15 (21.7) | 11 (23.4) | 4 (18.2) |
| Intervention Group | Control Group | |
|---|---|---|
| CPI index a, n(%) | ||
| Month 3, | n = 31 | n = 12 |
| <3 | 20 (64.5) | 9 (75.0) |
| ≥3 | 11 (35.5) | 3 (25.0) |
| Month 6, | n = 40 | n = 14 |
| <3 | 32 (80.0) | 12 (85.7) |
| ≥3 | 8 (20.0) | 2 (14.3) |
| DMFT score a, | ||
| Month 3, | n = 31 | n = 12 |
| Mean ± SD | 16.8 ± 7.2 | 17.7 ± 8.9 |
| Change from baseline | 0.1 ± 1.5 | 0.4 ± 0.9 |
| Month 6, | n = 40 | n = 14 |
| Mean ± SD | 17.2 ± 7.1 | 15.4 ± 8.9 |
| Change from baseline | 0.1 ± 2.4 | 0.1 ± 0.7 |
| OHIS score a, | ||
| Month 3, | n = 31 | n = 12 |
| Mean ± SD | 1.5 ± 1.2 | 1.9 ± 0.9 |
| Change from baseline | −0.5 ± 0.7 | −0.2 ± 0.9 |
| Month 6, | n = 40 | n = 14 |
| Mean ± SD | 1.1 ± 1.0 | 1.9 ± 1.2 |
| Change from baseline | −1.0 ± 1 | −0.0 ± 1.1 |
| SQOL score a, | ||
| Month 3, | n = 21 | n = 7 |
| Mean ± SD | 64.7 ± 9.9 | 52.0 ± 15.3 |
| Change from baseline | 2.8 ± 9.3 | −1.4 ± 6.8 |
| Month 6, | n = 31 | n = 10 |
| Mean ± SD | 64.0 ± 9.9 | 60.5 ± 15.5 |
| Change from baseline b | 4.1 ± 11.6 | 4.7 ± 19.7 |
| GOHAI score a, | ||
| Month 3, | n = 31 | n = 12 |
| Mean ± SD | 48.4 ± 6.7 | 48.3 ± 5.5 |
| Change from baseline c | 0.2 ± 4.9 | −1.5 ± 6.4 |
| Month 6, | n = 39 | n = 14 |
| Mean ± SD | 48.1 ± 6.2 | 49 ± 8.1 |
| Change from baseline c | 0.3 ± 5.7 | 0.7 ± 6.7 |
| Beck score a, | ||
| Month 3, | n = 30 | n = 8 |
| Mean ± SD | 5.9 ± 6.3 | 6.4 ± 6.5 |
| Change from baseline c | −0.7 ± 2.8 | −2.5 ± 4.6 |
| Month 6, | n = 37 | n = 11 |
| Mean ± SD | 7.4 ± 6.9 | 4.8 ± 5.0 |
| Change from baseline c | −1.2 ± 3.9 | −1.8 ± 2.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denis, F.; Rat, C.; Cros, L.; Bertaud, V.; El-Hage, W.; Jonval, L.; Soudry-Faure, A. Effectiveness of a Therapeutic Educational Oral Health Program for Persons with Schizophrenia: A Cluster Randomized Controlled Trial and Qualitative Approach. Healthcare 2023, 11, 1947. https://doi.org/10.3390/healthcare11131947
Denis F, Rat C, Cros L, Bertaud V, El-Hage W, Jonval L, Soudry-Faure A. Effectiveness of a Therapeutic Educational Oral Health Program for Persons with Schizophrenia: A Cluster Randomized Controlled Trial and Qualitative Approach. Healthcare. 2023; 11(13):1947. https://doi.org/10.3390/healthcare11131947
Chicago/Turabian StyleDenis, Frederic, Corinne Rat, Lucie Cros, Valerie Bertaud, Wissam El-Hage, Lysiane Jonval, and Agnès Soudry-Faure. 2023. "Effectiveness of a Therapeutic Educational Oral Health Program for Persons with Schizophrenia: A Cluster Randomized Controlled Trial and Qualitative Approach" Healthcare 11, no. 13: 1947. https://doi.org/10.3390/healthcare11131947
APA StyleDenis, F., Rat, C., Cros, L., Bertaud, V., El-Hage, W., Jonval, L., & Soudry-Faure, A. (2023). Effectiveness of a Therapeutic Educational Oral Health Program for Persons with Schizophrenia: A Cluster Randomized Controlled Trial and Qualitative Approach. Healthcare, 11(13), 1947. https://doi.org/10.3390/healthcare11131947