
Screening for Patients with Visual Acuity Loss in Primary Health Care: A Cross Sectional Study in a Deprived Hungarian Population

 ,
,
Abstract
1. Introduction
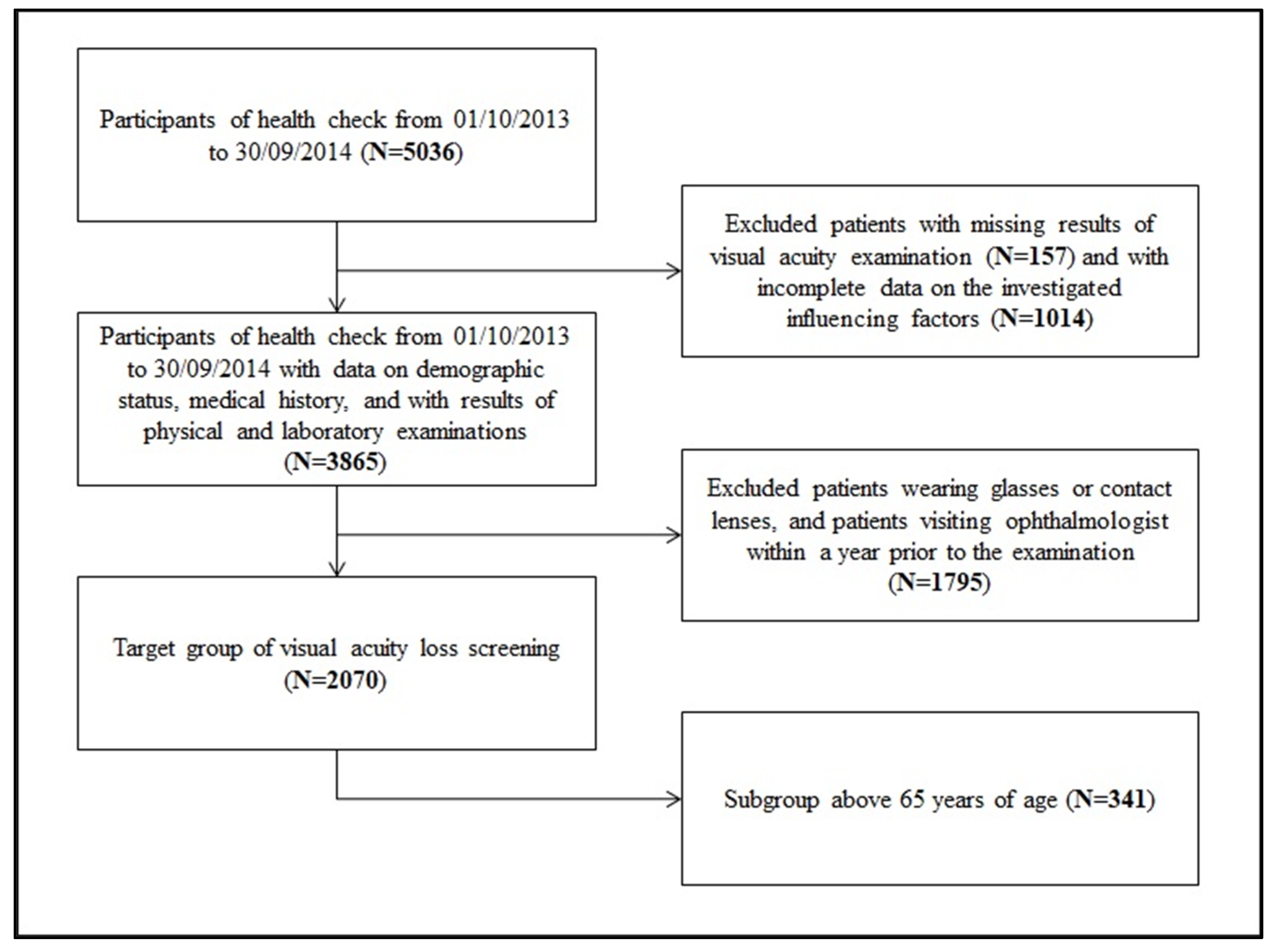
2. Materials and Methods
2.1. Setting
2.2. Data Collection
2.3. Visual Acuity Assessment
2.4. Data Analysis
2.5. Ethical Approval
3. Results
4. Discussion
4.1. Proportion of the Target Screening Group in the Whole Population
4.2. Yield of the Screening
4.3. Influencing Factors of Screening Positivity
4.4. Implications
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vision Impairment and Blindness. World Health Organization, 13 October 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment (accessed on 7 June 2023).
- World Report on Vision. World Health Organization, 8 October 2019. Available online: https://www.who.int/publications/i/item/9789241516570 (accessed on 7 June 2023).
- Bourne, R.; Steinmetz, J.D.; Flaxman, S.; Briant, P.S.; Taylor, H.R.; Resnikoff, S.; Casson, R.J.; Abdoli, A.; Abu-Gharbieh, E.; Afshin, A.; et al. Trends in Prevalence of Blindness and Distance and near Vision Impairment over 30 Years: An Analysis for the Global Burden of Disease Study. Lancet Glob. Health 2020, 9, E130–E143. [Google Scholar] [CrossRef] [PubMed]
- Majerníková, Ľ.; Hudáková, A.; Obročníková, A.; Grešš Halász, B.; Kaščáková, M. Quality of Life of Patients with Glaucoma in Slovakia. Int. J. Environ. Res. Public Health 2021, 18, 485. [Google Scholar] [CrossRef] [PubMed]
- Sburlan, E.A.; Voinea, L.-M.; Alexandrescu, C.; Istrate, S.; Iancu, R.; Pirvulescu, R.; Geamanu, A.; Ghita, M.; Ungureanu, E.; Radu, C. Rare Ophthalmology Diseases. Rom. J. Ophthalmol. 2019, 63, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Universal Eye Health: A Global Action Plan 2014–2019. World Health Organization, 26 October 2013. Available online: https://www.who.int/publications/i/item/universal-eye-health-a-global-action-plan-2014-2019 (accessed on 7 June 2023).
- Khan, M.A.; Soni, M.; Khan, M.D. Development of primary eye care as an integrated part of comprehensive health care. Community Eye Health 1998, 11, 24–26. [Google Scholar]
- Access to Primary and Secondary Eye Care. RNIB, 2023. Available online: https://www.rnib.org.uk/knowledge-and-research-hub/research-reports/prevention-sight-loss/access-eye-care (accessed on 7 June 2023).
- Holley, C.D.; Lee, P.P. Primary Care Provider Views of the Current Referral-to-Eye-Care Process: Focus Group Results. Investig. Opthalmology Vis. Sci. 2010, 51, 1866. [Google Scholar] [CrossRef]
- Nakano, T.; Kawashima, M.; Hiratsuka, Y.; Hiroshi, T.; Ono, K.; Murakami, A.; Tsubota, K.; Yamada, M. Assessment of Quality of Life in Patients with Visual Impairments Using a New Visual Function Questionnaire: The VFQ-J11. Clin. Ophthalmol. 2016, 10, 1939–1944. [Google Scholar] [CrossRef]
- Nickels, S.; Schuster, A.K.; Elflein, H.; Wolfram, C.; Schulz, A.; Münzel, T.; Beutel, M.E.; Schmidtmann, I.; Finger, R.P.; Pfeiffer, N. Vision-Related Quality of Life Considering Both Eyes: Results from the German Population-Based Gutenberg Health Study (GHS). Health Qual. Life Outcomes 2019, 17, 98. [Google Scholar] [CrossRef]
- Senra, H.; Hernandez-Moreno, L.; Moreno, N.; Macedo, A.F. Anxiety Levels Moderate the Association between Visual Acuity and Health-Related Quality of Life in Chronic Eye Disease Patients. Sci. Rep. 2022, 12, 2313. [Google Scholar] [CrossRef]
- Man, R.E.; Gan, A.T.; Fenwick, E.K.; Gupta, P.; Thakur, S.; Fang, X.L.; Cheng, C.-Y.; Wong, T.Y.; Lamoureux, E.L. The Differential Impact of Age on Vision-Related Quality of Life across the Visual Impairment Spectrum. Ophthalmology 2021, 128, 354–363. [Google Scholar] [CrossRef]
- Crews, J.E.; Chou, C.-F.; Zack, M.M.; Zhang, X.; Bullard, K.M.; Morse, A.R.; Saaddine, J.B. The Association of Health-Related Quality of Life with Severity of Visual Impairment among People Aged 40–64 Years: Findings from the 2006–2010 Behavioral Risk Factor Surveillance System. Ophthalmic Epidemiol. 2016, 23, 145–153. [Google Scholar] [CrossRef]
- Pondorfer, S.G.; Terheyden, J.H.; Heinemann, M.; Wintergerst, M.W.; Holz, F.G.; Finger, R.P. Association of Vision-Related Quality of Life with Visual Function in Age-Related Macular Degeneration. Sci. Rep. 2019, 9, 15326. [Google Scholar] [CrossRef]
- Varma, R.; Vajaranant, T.S.; Burkemper, B.; Wu, S.; Torres, M.; Hsu, C.; Choudhury, F.; McKean-Cowdin, R. Visual Impairment and Blindness in Adults in the United States. JAMA Ophthalmol. 2016, 134, 802–809. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.S.; Stevens, V.M.; Byanju, R.; Kandel, R.P.; Bhandari, G.; Bhandari, S.; Melo, J.S.; Porco, T.C.; Lietman, T.M.; Keenan, J.D. Cluster-Randomised Trial of Community-Based Screening for Eye Disease in Adults in Nepal: The Village-Integrated Eye Worker Trial II (View II) Trial Protocol. BMJ Open 2020, 10, e040219. [Google Scholar] [CrossRef] [PubMed]
- Ivers, R.Q. Visual Impairment and Hip Fracture. Am. J. Epidemiol. 2000, 152, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Testa, G.; De Salvo, S.; Boscaglia, S.; Montemagno, M.; Longo, A.; Russo, A.; Sessa, G.; Pavone, V. Hip Fractures and Visual Impairment: Is There a Cause–Consequence Mechanism? J. Clin. Med. 2022, 11, 3926. [Google Scholar] [CrossRef]
- Zhang, X.; Bullard, K.M.; Cotch, M.F.; Wilson, M.R.; Rovner, B.W.; McGwin, G.; Owsley, C.; Barker, L.; Crews, J.E.; Saaddine, J.B. Association between Depression and Functional Vision Loss in Persons 20 Years of Age or Older in the United States, NHANES 2005–2008. JAMA Ophthalmol. 2013, 131, 573–581. [Google Scholar] [CrossRef]
- Jones, G.C.; Rovner, B.W.; Crews, J.E.; Danielson, M.L. Effects of Depressive Symptoms on Health Behavior Practices among Older Adults with Vision Loss. Rehabil. Psychol. 2009, 54, 164–172. [Google Scholar] [CrossRef]
- Demmin, D.L.; Silverstein, S.M. visual Impairment and Mental Health: UNMET Needs and Treatment Options. Clin. Ophthalmol. 2020, 14, 4229–4251. [Google Scholar] [CrossRef]
- Wang, L.; Zhu, Z.; Scheetz, J.; He, M. Visual Impairment and Ten-Year Mortality: The Liwan Eye Study. Eye 2020, 35, 2173–2179. [Google Scholar] [CrossRef]
- Lee, D.J. Visual Acuity Impairment and Mortality in US Adults. Arch. Ophthalmol. 2002, 120, 1544–1550. [Google Scholar] [CrossRef]
- Mangione, C.M.; Barry, M.J.; Nicholson, W.K.; Cabana, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Epling, J.W.; Jaén, C.R.; et al. Screening for Impaired Visual Acuity in Older Adults. JAMA 2022, 327, 2123–2128. [Google Scholar]
- Visual Difficulties and Impairment. AAFP, 2018. Available online: https://www.aafp.org/family-physician/patient-care/clinical-recommendations/all-clinical-recommendations/visual.html (accessed on 7 June 2023).
- Wilson, B.J.; Courage, S.; Bacchus, M.; Dickinson, J.A.; Klarenbach, S.; Jaramillo Garcia, A.; Sims-Jones, N.; Thombs, B.D.; Canadian Task Force on Preventive Health Care. Screening for impaired vision in community-dwelling adults aged 65 years and older in primary care settings. CMAJ 2018, 190, E588–E594. [Google Scholar] [CrossRef]
- Frequency of Ocular Examinations—2015. American Academy of Ophthalmology, 2017. Available online: https://www.aao.org/clinical-statement/frequency-of-ocular-examinations (accessed on 7 June 2023).
- RACGP—Guidelines for Preventive Activities in General Practice. 2021. Available online: https://www.racgp.org.au/getattachment/1ad1a26f-9c8b-4e3c-b45b-3237272b3a04/Guidelines-for-preventive-activities-in-general-practice.aspx (accessed on 6 June 2023).
- Impaired Visual Acuity in Older Adults: Screening. Recommendation: Impaired Visual Acuity in Older Adults: Screening. United States Preventive Services Taskforce, 2022. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/impaired-visual-acuity-screening-older-adults (accessed on 7 June 2023).
- Szabó, D.; Sándor, G.L.; Tóth, G.; Pék, A.; Lukács, R.; Szalai, I.; Tóth, G.Z.; Papp, A.; Nagy, Z.Z.; Limburg, H.; et al. Visual Impairment and Blindness in Hungary. Acta Ophthalmol. 2017, 96, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Losonczy, G.; Piko, P.; Klevering, B.J.; Kosa, Z.; Sandor, J.; Adany, R. Low Prevalence of Spectacle Use in the Hungarian Roma Population Indicates Unmet Health Needs. Sci. Rep. 2022, 12, 3873. [Google Scholar] [CrossRef] [PubMed]
- Adany, R.; Kosa, K.; Sandor, J.; Papp, M.; Furjes, G. General Practitioners’ Cluster: A Model to Reorient Primary Health Care to Public Health Services. Eur. J. Public Health 2013, 23, 529–530. [Google Scholar] [CrossRef] [PubMed]
- Sandor, J.; Kosa, K.; Furjes, G.; Papp, M.; Csordas, A.; Rurik, I.; Adany, R. Public Health Services Provided in the Framework of General Practitioners’ Clusters. Eur. J. Public Health 2013, 23, 530–532. [Google Scholar] [CrossRef]
- Sándor, J.; Kósa, K.; Papp, M.; Fürjes, G.; Kőrösi, L.; Jakovljevic, M.; Ádány, R. Capitation-Based Financing Hampers the Provision of Preventive Services in Primary Health Care. Front. Public Health 2016, 4, 200. [Google Scholar] [CrossRef]
- Operations Manual for GPs’ Cluster on Public Health Services in Primary Health Care. Version 05. 2013. Available online: https://nepegeszseg.hu/Swiss/SH.8.1_operations_manual_version5.pdf (accessed on 7 June 2023).
- Mastropasqua, L.; D’Aloisio, R.; Mastrocola, A.; Perna, F.; Cerino, L.; Cerbara, L.; Cruciani, F.; Toto, L. Epidemiological surveillance of eye disease and people awareness in the Abruzzo region, Italy. Medicina 2021, 57, 978. [Google Scholar] [CrossRef]
- Smeeth, L. Screening Older People for Impaired Vision in Primary Care: Cluster Randomised Trial. BMJ 2003, 327, 1027. [Google Scholar] [CrossRef]
- Otte, B.; Woodward, M.A.; Ehrlich, J.R.; Stagg, B.C. Self-Reported Eyeglass Use by US Medicare Beneficiaries Aged 65 Years or Older. JAMA Ophthalmol. 2018, 136, 1047–1050. [Google Scholar] [CrossRef]
- Taipale, J.; Mikhailova, A.; Ojamo, M.; Nättinen, J.; Väätäinen, S.; Gissler, M.; Koskinen, S.; Rissanen, H.; Sainio, P.; Uusitalo, H. Low Vision Status and Declining Vision Decrease Health-Related Quality of Life: Results from a Nationwide 11-Year Follow-up Study. Qual. Life Res. 2019, 28, 3225–3236. [Google Scholar] [CrossRef] [PubMed]
- Havstam Johansson, L.; Škiljić, D.; Falk Erhag, H.; Ahlner, F.; Pernheim, C.; Rydberg Sterner, T.; Wetterberg, H.; Skoog, I.; Zetterberg, M. Vision-related Quality of Life and Visual Function in a 70-year-old Swedish Population. Acta Ophthalmol. 2020, 98, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.; Kuper, H.; Macleod, D.; Musendo, D.; Irunga, P.; Yip, J.L. Population Need for Primary Eye Care in Rwanda: A National Survey. PLoS ONE 2018, 13, e0193817. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, S.; Vashist, P.; Gupta, N.; Kalaivani, M.; Rath, R.; Gupta, S. Prevalence and Causes of Visual Impairment among Adults Aged 15–49 Years in a Rural Area of North India—A Population-Based Study. Indian J. Ophthalmol. 2018, 66, 951–956. [Google Scholar] [CrossRef]
- Burkemper, B.; Torres, M.; Jiang, X.; McKean-Cowdin, R.; Varma, R. Factors Associated with Visual Impairment in Chinese American Adults: The Chinese American Eye Study. Ophthalmic Epidemiol. 2019, 26, 329–335. [Google Scholar] [CrossRef]
- Zebardast, N.; Friedman, D.S.; Vitale, S. The Prevalence and Demographic Associations of Presenting Near-Vision Impairment among Adults Living in the United States. Am. J. Ophthalmol. 2017, 174, 134–144. [Google Scholar] [CrossRef]
- Iwano, M.; Nomura, H.; Ando, F.; Niino, N.; Miyake, Y.; Shimokata, H. Visual Acuity in a Community-Dwelling Japanese Population and Factors Associated with Visual Impairment. Jpn. J. Ophthalmol. 2004, 48, 37–43. [Google Scholar] [CrossRef]
- Arrieta-Camacho, J.; Graue-Hernández, E.; Ramirez-Miranda, A.; Jimenez-Corona, A. Visual Acuity and Associated Risk Factors in indigenous and non-indigenous Mexican population. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5729. [Google Scholar]
- Vajaranant, T.S.; Nayak, S.; Wilensky, J.T.; Joslin, C.E. Gender and Glaucoma: What We Know and What We Need to Know. Curr. Opin. Ophthalmol. 2010, 21, 91–99. [Google Scholar] [CrossRef]
- Chakravarthy, U.; Wong, T.Y.; Fletcher, A.; Piault, E.; Evans, C.; Zlateva, G.; Buggage, R.; Pleil, A.; Mitchell, P. Clinical Risk Factors for Age-Related Macular Degeneration: A Systematic Review and Meta-Analysis. BMC Ophthalmol. 2010, 10, 31. [Google Scholar] [CrossRef]
- Bhartiya, S.; Kumar, N.; Dhingra, D.; Wadhwani, M. Habitual Visual Acuity in a Large Urban Cohort of Western India and Factors Influencing Poor Habitual Vision. Indian J. Ophthalmol. 2021, 69, 842–846. [Google Scholar] [CrossRef] [PubMed]
- Jan, C.; Li, S.-M.; Kang, M.-T.; Liu, L.; Li, H.; Jin, L.; Qin, X.; Congdon, N.; Wang, N. Association of Visual Acuity with Educational Outcomes: A Prospective Cohort Study. Br. J. Ophthalmol. 2019, 103, 1666–1671. [Google Scholar] [CrossRef] [PubMed]
- Brunes, A.; Heir, T. Visual Impairment and Employment in Norway. BMC Public Health 2022, 22, 648. [Google Scholar] [CrossRef]
- Jeon, B.; Koo, H.; Lee, H.-J.; Han, E. Effect of the Age of Visual Impairment Onset on Employment Outcomes in South Korea: Analysis of the National Survey on Persons with Disabilities Data. BMC Public Health 2022, 22, 1613. [Google Scholar] [CrossRef] [PubMed]
- Soltész, B.; Pikó, P.; Sándor, J.; Kósa, Z.; Ádány, R.; Fiatal, S. The Genetic Risk for Hypertension Is Lower among the Hungarian Roma Population Compared to the General Population. PLoS ONE 2020, 15, e0234547. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.G.; Berezovsky, A.; Watanabe, S.E.; Mitsuhiro, M.R.; Cypel, M.C.; Ferraz, N.N.; Furtado, J.M.; Sacai, P.Y.; Muñoz, S.; Cunha, C.C.; et al. Prevalence of Ocular Findings Regardless of Visual Acuity Status in Older Adults from the Brazilian Amazon Region. Sci. Rep. 2021, 11, 23710. [Google Scholar] [CrossRef]
- Leley, S.P.; Ciulla, T.A.; Bhatwadekar, A. Diabetic Retinopathy in the Aging Population: A Perspective of Pathogenesis and Treatment. Clin. Interv. Aging 2021, 16, 1367–1378. [Google Scholar] [CrossRef]
- Davari, M.; Bayazidi, Y.; Kebriaeezadeh, A.; Esteghamati, A.; Bandarian, F.; Kashi, Z.; Bahar, A.; Yousefi, S. Quality of Care in Type 2 Diabetes in Iran; a Cross-Sectional Study Using Patient-Level Data. BMC Endocr. Disord. 2022, 22, 133. [Google Scholar] [CrossRef]
- RACGP—The Royal Australian College of General Practitioners. 2016. Available online: https://www.racgp.org.au/download/Documents/Guidelines/Redbook9/17048-Red-Book-9th-Edition.pdf (accessed on 19 February 2023).
- UK National Screening Committee. Vision Defects. 2019. Available online: https://view-health-screening-recommendations.service.gov.uk/vision-defects/ (accessed on 19 February 2023).



{kind=link}
{kind=link}
| Adults (18+ Years of Age) | Above 65 Years of Age | ||
|---|---|---|---|
| Sex | Male | 768 (37.1%) | 140 (41.1%) |
| Female | 1302 (62.9%) | 201 (58.9%) | |
| Age | mean (±SD) | 47.8 (±15.9) | 71.9 (±5.52) |
| Education | non-completed primary school | 233 (11.3%) | 45 (13.2%) |
| completed primary school | 640 (30.9%) | 148 (43.4%) | |
| secondary school without graduation | 511 (24.7%) | 57 (16.7%) | |
| secondary school with graduation | 533 (25.7%) | 70 (20.5%) | |
| higher education | 153 (7.4%) | 21 (6.2%) | |
| Employment | Unemployed | 1079 (52.1%) | 336 (98.5%) |
| Employed | 991 (47.9%) | 5 (1.5%) | |
| Ethnicity | non-Roma | 1825 (88.2%) | 334 (97.9%) |
| Roma | 245 (11.8%) | 7 (2.1%) | |
| Hypertension | Normotensive | 882 (42.6%) | 31 (9.1%) |
| untreated hypertension | 279 (13.5%) | 47 (13.8%) | |
| insufficiently treated hypertension | 487 (23.5%) | 144 (42.2%) | |
| properly treated hypertension | 422 (20.4%) | 119 (34.9%) | |
| Diabetes | Normoglycemic | 1786 (86.3%) | 246 (72.1%) |
| untreated diabetes | 75 (3.6%) | 24 (7.0%) | |
| insufficiently treated diabetes | 128 (6.2%) | 41 (12.0%) | |
| properly treated diabetes | 81 (3.9%) | 30 (8.8%) | |
| Visual acuity | visual acuity ≥ 0.5 | 1994 (96.3%) | 310 (90.9%) |
| visual acuity < 0.5 | 76 (3.7%) | 31 (9.1%) | |
| Total number of participants | 2070 (100%) | 341 (100%) | |
| Influencing Factors | Adults (18+ Years of Age) | Above 65 Years of Age | |
|---|---|---|---|
| Sex | Male | 0 (reference) | 0 (reference) |
| Female | 1.27 [0.35; 2.18] | 3.85 [0.5; 7.2] | |
| Age | Year | 0.15 [0.12; 0.19] | 0.39 [0.1; 0.67] |
| Education | non-completed primary school | 0 (reference) | 0 (reference) |
| completed primary school | 0.45 [−1.03; 1.94] | 1.15 [−3.83; 6.12] | |
| secondary school without graduation | −2.06 [−3.64; −0.47] | −2.58 [−8.76; 3.59] | |
| secondary school with graduation | −2.08 [−3.65; −0.51] | −1.22 [−6.94; 4.51] | |
| higher education | −1.82 [−3.89; 0.25] | −0.24 [−7.91; 7.42] | |
| Employment | Unemployed | 0 (reference) | --- |
| Employed | −1.33 [−2.25; −0.4] | nc | |
| Ethnicity | non-Roma | 1 (reference) | 1 (reference) |
| Roma | 2.6 [1.22; 3.97] | 24.79 [13.83; 35.76] | |
| Hypertension | Normotensive | 0 (reference) | 0 (reference) |
| untreated hypertension | 0.31 [−1.08; 1.7] | 0.76 [−5.79; 7.31] | |
| insufficiently treated hypertension | 0.36 [−0.92; 1.64] | 1.17 [−4.46; 6.8] | |
| properly treated hypertension | −0.6 [−1.87; 0.68] | 0.02 [−5.7; 5.74] | |
| Diabetes mellitus | Normoglycemic | 0 (reference) | 0 (reference) |
| untreated diabetes | 0.68 [−1.61; 2.98] | 7.3 [1.29; 13.31] | |
| insufficiently treated diabetes | 0.37 [−1.45; 2.19] | 1.73 [−3.06; 6.51] | |
| properly treated diabetes | −2.84 [−5.08; −0.6] | −0.8 [−6.38; 4.78] | |
| Influencing Factors | Adults (18+ Years of Age) * | Above 65 Years of Age * | |
|---|---|---|---|
| Sex | Male | 1 (reference) | 1 (reference) |
| Female | 1.75 [0.98; 3.14] | 2.56 [0.91; 7.16] | |
| Age | Year | 1.06 [1.04; 1.08] | 1.1 [1.03; 1.18] |
| Education | non-completed primary school | 1 (reference) | 1 (reference) |
| completed primary school | 1.14 [0.59; 2.19] | 1.16 [0.38; 3.56] | |
| secondary school without graduation | 0.61 [0.25; 1.49] | 0.3 [0.03; 3.10] | |
| secondary school with graduation | 0.35 [0.13; 0.93] | 0.51 [0.10; 2.44] | |
| higher education | 1.18 [0.41; 3.37] | 1.7 [0.33; 8.83] | |
| Employment | Unemployed | 1 (reference) | --- |
| Employed | 0.57 [0.30; 1.12] | nc | |
| Ethnicity | non-Roma | 1 (reference) | 1 (reference) |
| Roma | 2.80 [1.41; 5.55] | 7.81 [1.36; 44.68] | |
| Hypertension | Normotensive | 1 (reference) | 1 (reference) |
| untreated hypertension | 0.50 [0.20; 1.26] | 0.96 [0.08; 12.3] | |
| insufficiently treated hypertension | 0.80 [0.40; 1.6] | 2.56 [0.31; 21.34] | |
| properly treated hypertension | 0.71 [0.35; 1.45] | 2.48 [0.29; 21.00] | |
| Diabetes mellitus | Normoglycemic | 1 (reference) | 1 (reference) |
| untreated diabetes | 1.16 [0.43; 3.12] | 2.03 [0.56; 7.42] | |
| insufficiently treated diabetes | 1.17 [0.52; 2.64] | 1.34 [0.39; 4.63] | |
| properly treated diabetes | 0.18 [0.02; 1.32] | 0.34 [0.04; 2.87] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wasnik, R.N.; Győri-Dani, V.; Vincze, F.; Papp, M.; Pálinkás, A.; Sándor, J. Screening for Patients with Visual Acuity Loss in Primary Health Care: A Cross Sectional Study in a Deprived Hungarian Population. Healthcare 2023, 11, 1941. https://doi.org/10.3390/healthcare11131941
Wasnik RN, Győri-Dani V, Vincze F, Papp M, Pálinkás A, Sándor J. Screening for Patients with Visual Acuity Loss in Primary Health Care: A Cross Sectional Study in a Deprived Hungarian Population. Healthcare. 2023; 11(13):1941. https://doi.org/10.3390/healthcare11131941
Chicago/Turabian StyleWasnik, Rahul Naresh, Veronika Győri-Dani, Ferenc Vincze, Magor Papp, Anita Pálinkás, and János Sándor. 2023. "Screening for Patients with Visual Acuity Loss in Primary Health Care: A Cross Sectional Study in a Deprived Hungarian Population" Healthcare 11, no. 13: 1941. https://doi.org/10.3390/healthcare11131941
APA StyleWasnik, R. N., Győri-Dani, V., Vincze, F., Papp, M., Pálinkás, A., & Sándor, J. (2023). Screening for Patients with Visual Acuity Loss in Primary Health Care: A Cross Sectional Study in a Deprived Hungarian Population. Healthcare, 11(13), 1941. https://doi.org/10.3390/healthcare11131941