
Assessing the Feasibility and Acceptability of a Primary Care Socio-Ecological Approach to Improve Physical Activity Adherence among People with Type 2 Diabetes: The SENWI Project

 ,
,  ,
,  ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Randomization and Blinding
2.4. Study Interventions
2.5. Measures, Data Collection, and Management
2.5.1. Quantitative Assessments
2.5.2. Quantitative Data Analysis
2.5.3. Qualitative Assessments
2.5.4. Qualitative Data Analysis
3. Results
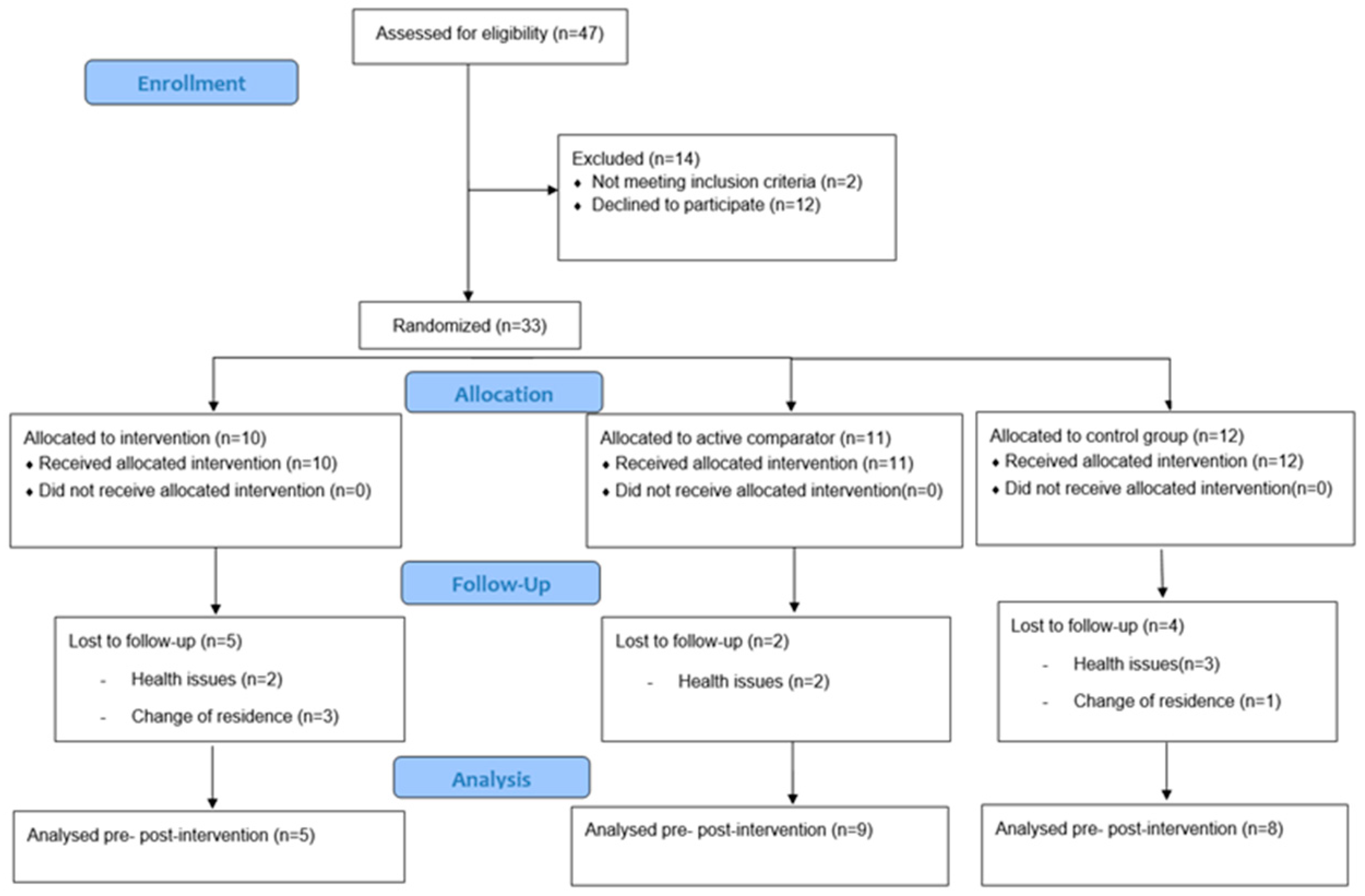
3.1. Participants Characteristics
3.2. Interventions Impact on PA, SB and Health Outcomes
3.3. Intervention Adherence and Withdraw
3.4. Intervention Feasibility and Acceptability
3.4.1. People with T2D Perceptions
- Theme 1: Useful but with expiry date
“At first, I had my doubts, but then, when I try the poles, they were helpful. And not only at the uphill, but also downhills!”(man; at the follow-up of the intervention)
“It was good to start doing something new, but once it is finish, what? What we have to do now to keep going on?”(man; at the follow-up of the intervention)
- Theme 2: Gender inequities
“Sometimes I had to choose to come here or to take care of my grandchildren. Sometimes I was not able always to skip my family duties.”(woman; at the follow-up of the intervention)
“It was great. I had a lot of free time, which was a good way to stay occupied throughout the day.”(man; at the follow-up of the intervention)
- Theme 3: Different PA capacity between individuals
“For me it was sometimes boring because other participants walk too slow.”(man; dropout of the intervention)
“It was not easy for me. It takes me a lot of time and get bored, that is the reason I drop out.”(woman; dropout of the intervention)
“I think it will be better to know what capacities have each one before we are assigned to a group.”(woman; at the follow-up of the intervention)
3.4.2. HCP Perceptions
- Theme 4: Feasibility in the healthcare system
“It was easy while the study was going on. But once it is finish; it is impossible to carry on without any help.”(HCP; nurse specialist)
“Without more resources and time, or even more, more healthcare professionals to do this job, I think that is not possible nowadays.”(HCP; physiotherapist)
- Theme 5: Intervention with bounded options
“At the beginning it was difficult to enroll some participants because they were not able to enroll in the morning groups. Maybe with more schedule groups will be easy.”(HCP; nurse specialist)
“It was clear from the beginning that some participants had difficulties to follow-up the sessions, while others express that we were going to slow. I think that some of them left the study because of that.”(HCP; physiotherapist)
4. Discussion
Strength and Limitations
5. Conclusions
Future Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Kaabi, J.A. Epidemiology of Type 2 Diabetes–Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef]
- Rosella, L.C.; Lebenbaum, M.; Fitzpatrick, T.; O’Reilly, D.; Wang, J.; Booth, G.L.; Stukel, T.A.; Wodchis, W.P. Impact of diabetes on healthcare costs in a population-based cohort: A cost analysis. Diabet. Med. 2016, 33, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Mata-Cases, M.; Casajuana, M.; Franch-Nadal, J.; Casellas, A.; Castell, C.; Vinagre, I.; Mauricio, D.; Bolibar, B. Direct medical costs attributable to type 2 diabetes mellitus: A population-based study in Catalonia, Spain. Eur. J. Health Econ. 2016, 17, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- Sedentary Behaviour Research Network. Letter to the editor: Standardized use of the terms “sedentary” and “sedentary behaviours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Marathe, P.H.; Gao, H.X.; Close, K.L. American Diabetes Association Standards of Medical Care in Diabetes 2017. J. Diabetes 2017, 9, 320–324. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.-L.; Pan, J.-H.; Chen, D.; Chen, J.; Chen, F.; Hu, T.-T. Efficacy of lifestyle interventions in patients with type 2 diabetes: A systematic review and meta-analysis. Eur. J. Intern. Med. 2016, 27, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Sheri, R.; Ronald, J.; Judith, G.; Bryan, J.; Richard, R.; Ann, L. Exercise and type 2 diabetes: The American College of Sports Medicine and The American Diabetes Association: Joint position statement executive summary. Diabetes Care 2016, 33, e147–e167. [Google Scholar]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M.; Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef] [PubMed]
- Kennerly, A.M.; Kirk, A. Physical activity and sedentary behaviour of adults with type 2 diabetes: A systematic review. Pract. Diabetes 2018, 35, 86–89g. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Owen, N.; Yates, T.E.; Kingwell, B.A.; Dunstan, D.W. Sitting Less and Moving More: Improved Glycaemic Control for Type 2 Diabetes Prevention and Management. Curr. Diab. Rep. 2016, 16, 114. [Google Scholar] [CrossRef] [PubMed]
- Jelleyman, C.; Yates, T.; O’Donovan, G.; Gray, L.J.; King, J.A.; Khunti, K.; Davies, M.J. The effects of high-intensity interval training on glucose regulation and insulin resistance: A meta-analysis. Obes. Rev. 2015, 16, 942–961. [Google Scholar] [CrossRef]
- Jung, M.E.; Bourne, J.E.; Beauchamp, M.R.; Robinson, E.; Little, J.P. High-intensity interval training as an efficacious alternative to moderate-intensity continuous training for adults with prediabetes. J. Diabetes Res. 2015, 2015, 191595. [Google Scholar] [CrossRef] [PubMed]
- Little, J.P.; Francois, M.E. High-intensity interval training for improving postprandial hyperglycemia. Res. Q. Exerc. Sport 2014, 85, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Tschentscher, M.; Niederseer, D.; Niebauer, J. Health benefits of nordic walking: A systematic review. Am. J. Prev. Med. 2013, 44, 76–84. [Google Scholar] [CrossRef]
- Takeshima, N.; Islam, M.M.; Rogers, M.E.; Rogers, N.L.; Sengoku, N.; Koizumi, D.; Kitabayashi, Y.; Imai, A.; Naruse, A. Effects of Nordic Walking Compared to Conventional Walking and Band-Based Resistance Exercise on Fitness in Older Adults. J. Sport. Sci. Med. 2013, 12, 422. [Google Scholar]
- Sanchez-Lastra, M.A.; Miller, K.J.; Martínez-Lemos, R.I.; Giráldez, A.; Ayán, C. Nordic walking for overweight and obese people: A systematic review and meta-analysis. J. Phys. Act. Health 2020, 17, 762–772. [Google Scholar] [CrossRef] [PubMed]
- González, K.; Fuentes, J.; Márquez, J.L. Physical inactivity, sedentary behavior and chronic diseases. Korean J. Fam. Med. 2017, 38, 111–115. [Google Scholar] [CrossRef]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; WHO: Geneva, Switzerland, 2003.
- Hill-Briggs, F.; Adler, N.E.; Berkowitz, S.A.; Chin, M.H.; Gary-Webb, T.L.; Navas-Acien, A.; Thornton, P.L.; Haire-Joshu, D. Social Determinants of Health and Diabetes: A Scientific Review. Diabetes Care 2021, 44, 258–279. [Google Scholar] [CrossRef]
- Cowley, E.S.; Watson, P.M.; Foweather, L.; Belton, S.; Thompson, A.; Thijssen, D.; Wagenmakers, A.J.M. “Girls Aren’t Meant to Exercise”: Perceived Influences on Physical Activity among Adolescent Girls–The HERizon Project. Children 2021, 8, 31. [Google Scholar] [CrossRef]
- Althoff, T.; Sosič, R.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nature 2017, 547, 336–339. [Google Scholar] [CrossRef]
- nternational Society for Physical Activity and Health (ISPAH). Las Ocho Inversiones de la ISPAH para Mejorar la Actividad Física. Int. Soc. Phys. Act. Health 2020, 17, 68–73. [Google Scholar]
- Jenkin, C.R.; Eime, R.M.; van Uffelen, J.G.Z.; Westerbeek, H. How to re-engage older adults in community sport? Reasons for drop-out and re-engagement. Leis. Stud. 2021, 40, 441–453. [Google Scholar] [CrossRef]
- Czwikla, G.; Boen, F.; Cook, D.G.; de Jong, J.; Harris, T.; Hilz, L.K.; Iliffe, S.; Lechner, L.; Morris, R.W.; Muellmann, S.; et al. Equity-specific effects of interventions to promote physical activity among middle-aged and older adults: Results from applying a novel equity-specific re-analysis strategy. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 65. [Google Scholar] [CrossRef]
- Haire-Joshu, D.; Hill-Briggs, F. The Next Generation of Diabetes Translation: A Path to Health Equity. Annu. Rev. Public Health 2019, 40, 391–410. [Google Scholar] [CrossRef]
- Albert, F.A.; Crowe, M.J.; Malau-Aduli, A.E.O.; Malau-Aduli, B.S. Physical activity promotion: A systematic review of the perceptions of healthcare professionals. Int. J. Environ. Res. Public Health 2020, 17, 4358. [Google Scholar] [CrossRef]
- Jabardo-Camprubí, G.; Bort-Roig, J.; Donat-Roca, R.; Martín-Horcajo, M.; Puig-Ribera, A.; McKenna, J. How patients with diabetes experience physical activity promotion during nursing consultations in the Spanish context. Enfermería Clín. Engl. Ed. 2022, 33, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Brannan, M.; Bernardotto, M.; Clarke, N.; Varney, J. Moving healthcare professionals–A whole system approach to embed physical activity in clinical practice. BMC Med. Educ. 2019, 19, 84. [Google Scholar] [CrossRef]
- Kime, N.; Pringle, A.; Zwolinsky, S.; Vishnubala, D. How prepared are healthcare professionals for delivering physical activity guidance to those with diabetes? A formative evaluation. BMC Health Serv. Res. 2020, 20, 8. [Google Scholar] [CrossRef]
- Bayón Cabeza, M.; Pérez Rivas, F.J.; Zamora Sarabia, A.L.; de las Heras Mosteiro, J.; Becerril Rojas, B.; Rodriguez Barrientos, R. Control del paciente diabético en Atención Primaria: Influencia de cartera de servicios y otros factores. Atención Primaria 2020, 52, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Ariza, C.; Gavara, V.; Mu, A. Atención Primaria Mejora en el control de los diabéticos tipo 2 tras una intervención conjunta: Educación diabetológica y ejercicio físico. Atención Primaria 2011, 43, 398–406. [Google Scholar] [CrossRef]
- Jabardo-Camprubí, G.; Bort-Roig, J.; Donat-Roca, R.; Milà-Villarroel, R.; Sitjà-Rabert, M.; McKenna, J.; Puig-Ribera, A. A socio-ecological approach to reduce the physical activity drop-out ratio in primary care-based patients with type 2 diabetes: The SENWI study protocol for a randomized control trial. Trials 2022, 23, 842. [Google Scholar] [CrossRef]
- Heisz, J.J.; Tejada, M.G.M.; Paolucci, E.M.; Muir, C. Enjoyment for high-intensity interval exercise increases during the first six weeks of training: Implications for promoting exercise adherence in sedentary adults. PLoS ONE 2016, 11, e0168534. [Google Scholar] [CrossRef]
- Piedra, L.M.; Andrade, F.C.D.; Hernandez, R.; Trejo, L.; Prohaska, T.R.; Sarkisian, C.A. Let’s walk! Age reattribution and physical activity among older Hispanic/Latino adults: Results from the ¡caminemos! Randomized trial. BMC Public Health 2018, 18, 964. [Google Scholar] [CrossRef] [PubMed]
- Burrows, B.; Andrade, F.C.D.; Piedra, L.; Xu, S.; Aguiñaga, S.; Steinberg, N.; Sarkisian, C.; Hernandez, R. The Influence of Evidence-Based Exercise and Age Reattribution on Physical Function in Hispanic Older Adults: Results From the ¡Caminemos! Randomized Controlled Trial. J. Appl. Gerontol. 2020, 40, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Levin-Zamir, D.; Badarne, S.; Najami, M.; Gan Noy, S.; Poraz, I.; Shapira, M.; Lieberman, N.; Goldfracht, M. The use of focus groups as a basis for planning and implementing culturally appropriate health promotion among people with diabetes in the Arab community. Glob. Health Promot. 2016, 23, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Berg, B.L.; Bruce, L.; Lune, H. Qualitative Research Methods for the Social Sciences, 9th ed.; Dodge, A., Ed.; Pearson: Essex, UK, 2017; 240p. [Google Scholar]
- Martland, R.; Teasdale, S.; Murray, R.M.; Gardner-Sood, P.; Smith, S.; Ismail, K.; Atakan, Z.; Greenwood, K.; Stubbs, B.; Gaughran, F. Dietary intake, physical activity and sedentary behaviour patterns in a sample with established psychosis and associations with mental health symptomatology. Psychol. Med. 2021, 53, 1565–1575. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.A. Health literacy and adherence to medical treatment in chronic and acute illness: A meta-analysis. Patient Educ. Couns. 2016, 99, 1079–1086. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.; Boyce, T.; Goldblatt, P.; Morrison, J. Health equity in England: The Marmot review 10 years on. BMJ 2020, 368, m693. [Google Scholar] [CrossRef]
- McGinnis, E.L.; Rogers, L.Q.; Fruhauf, C.A.; Jankowski, C.M.; Crisafio, M.E.; Leach, H.J. Feasibility of implementing physical activity behavior change counseling in an existing cancer-exercise program. Int. J. Environ. Res. Public Health 2021, 18, 12705. [Google Scholar] [CrossRef]
- Ramos, T.M. Ethnographic study on older women’s ageing from a gender and life course perspective. Prism. Soc. 2018, 21, 75–107. [Google Scholar]
- Sommer, R.; Linder, S.; Ziemainz, H.; Gelius, P. Key performance indicators of cooperative planning processes: Case study results from German sport science and physical activity promotion projects. Ger. J. Exerc. Sport. Res. 2022, 52, 24–38. [Google Scholar] [CrossRef]
- Ptack, K.; Strobl, H. Factors influencing the effectiveness of a Cooperative Planning approach in the school setting. Health Promot. Int. 2021, 36, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Galea, S. Macrosocial Determinants of Population Health; Springer: New York, NY, USA, 2007; 48p. [Google Scholar]
- Villa-García, L.; Davey, V.; Peréz, L.M.; Soto-Bagaria, L.; Risco, E.; Díaz, P.; Kuluski, K.; Giné-Garriga, M.; Castellano-Tejedor, C.; Inzitari, M. Co-designing implementation strategies to promote remote physical activity programs in frail older community-dwellers. Front. Public Health 2023, 11, 1062843. [Google Scholar] [CrossRef] [PubMed]
- Caperon, L.; Arjyal, A.; Puja, K.C.; Kuikel, J.; Newell, J.; Peters, R.; Prestwich, A.; King, R. Developing a socio-ecological model of dietary behaviour for people living with diabetes or high blood glucose levels in urban Nepal: A qualitative investigation. PLoS ONE 2019, 14, e0214142. [Google Scholar] [CrossRef] [PubMed]
- Owen, K.B.; Nau, T.; Reece, L.J.; Bellew, W.; Rose, C.; Bauman, A.; Halim, N.K.; Smith, B.J. Fair play? Participation equity in organised sport and physical activity among children and adolescents in high income countries: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 777–780. [Google Scholar] [CrossRef]
- Puig-Ribera, A.; Rofin, M.; Bort-Roig, J.; Aumatell, E.; Juncà, A.; Pedro, M.D.S.; Garcia-Cuyàs, F.; Chamorro, C.; Perona-Ribes, L.; Torrentó, J.R.; et al. Integrating Health into the Urban Master Plan of Vic, Barcelona: A Comprehensive Approach. Urban Plan. 2022, 7, 25–41. [Google Scholar] [CrossRef]
- Carrero Planes, V.; Trinidad Requena, A.; Soriano Miras, R.M. Teoriía Fundamentada Grounded Theory: El Desarrollo de Teoriía Desde la Generalizacioín Conceptual, 2nd ed.; Centro de Investigaciones Sociológicas: Madrid, Spain, 2012; 187p.


{kind=link}
| Participant Characteristics at Baseline | SENWI Group (n = 10) | NW Group (n = 11) | Control Group (n = 12) | Full Sample (n = 33) |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Sex | ||||
| Female | 4 (40) | 3 (27.3) | 5 (41.7) | 12 (36.4) |
| Male | 6 (60) | 8 (72.7) | 7 (58.3) | 21 (63.6) |
| Years from diagnosis | ||||
| >2 and <5 | 3 (30) | 3 (27.3) | 1 (8.3) | 7 (21.2) |
| >5 and <10 | 1 (10) | 5 (45.5) | 1 (8.3) | 7 (21.2) |
| <10 | 6 (60) | 3 (27.3) | 10 (83.3) | 19 (57.9) |
| Socioeconomic status | ||||
| Low | 7 (70) | 8 (72.7) | 7 (58.3) | 22 (66.7) |
| Medium | 0 (0) | 2 (18.2) | 2 (16.7) | 4 (12.1) |
| High | 3 (30) | 1 (9.1) | 3 (25) | 7 (21.2) |
| Physically Active (APAFB) | ||||
| No | 3 (30) | 6 (54.5) | 3 (25) | 12 (36.4) |
| Yes | 7 (70) | 5 (45.5) | 9 (75) | 21 (63.6) |
| Participant characteristics at baseline | SENWI Group (n = 10) | NW Group (n = 11) | Control Group (n = 12) | Full sample (n = 33) |
| Md (CI 95%) | Md (CI 95%) | Md (CI 95%) | Md (CI 95%) | |
| Age (years) | 69.5 (67–74) | 69 (67–73) | 72.5 (66–78) | 70 (69–74) |
| Waist circumference (cm) | 108 (95.9–113.8) | 109 (101.7–114.6) | 111 (96.5–118.8) | 109 (104.9–112.3) |
| BMI (kg/m2) | 30.3 (25.3–33.7) | 33.1 (27.8–35.1) | 30.1 (26.8–36.4) | 30.7 (29.1–33.1) |
| HbA1c (%) | 6.5 (6.2–7.5) | 7.1 (6.2–7.7) | 6.7 (5.9–7.4) | 6.8 (6.4–7.1) |
| SF-12 (PCS) | 48.6 (28.7–53.5) | 48.4 (41.9–54.5) | 34.2 (27.2–51.5) | 44.3 (39.4–48.9) |
| SF-12 (MCS) | 58.2 (44.8–61.9) | 54.5 (45.1–54.5) | 44.7 (34.8–56.5) | 54.4 (45.1–57.3) |
| Steps/day | 12,732.1 (7392.7–15,587.3) | 7239 (5033.2–9407.7) | 7536.6 (4948.1–10,918.8) | 7909.1 (6679.9–10,747) |
| Walking duration (min) | 150 (93.6–190.2) | 96 (72.6–126) | 97.5 (75–140.4) | 107.1 (90.6–129.6) |
| Stand-up duration (min) | 291 (201–313.2) | 226.8 (169.2–301.8) | 224.1 (183.6–252.6) | 231.9 (207.6–253.2) |
| Absolute time in SB (min) | 560.4 (413.4–615.6) | 595.8 (491.4–621) | 564.3 (517.2–706.8) | 564.3 (531–598.2) |
| Bouts < 30 min (min) | 247.5 (203.7–375.1) | 220.9 (189.8–292.3) | 298.7 (211.1–416.6) | 247.5 (220.1–301.8) |
| Bouts between 30 and 60 min (min) | 145.71 (81.9–166.6) | 126.5 (99.7–147.4) | 142.6 (61.8–161.1) | 138.7 (107.8–151.9) |
| Bouts > 60 min (min) | 107.7 (63.3–217.5) | 182.9 (128.6–231.1) | 125.7 (65.6–288.9) | 156.9 (115.8–205.9) |
| Sit-to-stand transitions (number) | 43 (37.1–55.8) | 45 (35.7–48.9) | 46.5 (43.3–73.3) | 45.5 (43–49.7) |
| Number of SB bouts < 30 min | 40 (32.2–49) | 37 (29.7–43.3) | 41.5 (39.3–70) | 41 (37.3–43.9) |
| Number of SB bouts between 30 and 60 min | 3 (2–4) | 3 (2–4) | 3 (1.3–4) | 3 (2.1–4) |
| Number of SB bouts > 60 min | 1 (1–2) | 2 (1.7–3) | 1.5 (1–2.7) | 2 (1–2) |
| LPA duration (min) | 109.6 (89.7–125.6) * | 89.1 (66.9–111.2) | 80.6 (63.6–98.3) * | 90.9 (81.9–107.2) |
| MVPA duration (min) | 20.9 (3.8–64.7) | 8.9 (6.8–17.3) | 8.3 (0.7–49.3) | 9.6 (6.7–17.3) |
| Participant Primary Metabolic and PA Outcomes | SENWI Group (n = 5) | NW Group (n = 9) | Control Group (n = 8) | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |
| Md (CI 95%) | Md (CI 95%) | Md (IC 95%) | Md (CI 95%) | Md (CI 95%) | Md (CI 95%) | |
| Waist circumference (cm) | 108 (89–114) | 105 (86–111) | 109 (69.9–113.7) | 109 (100.3–113.9) | 107 (95–122.2) | 104.5 (93.1–119.3) |
| BMI (kg/m2) | 31.1 (24.2–34.3) | 31.7 (24.1–32.1) | 33.1 (25.1–35.5) | 32.8 (24.7–35.2) | 29.4 (24.8–38.5) | 28.1 (24.8–37.9) |
| HbA1c (%) | 6.4 (5.8–7.6) | 6.8 (6.1–8) | 7.1 (6.1–8.7) | 6.9 (6.3–7.8) | 6.9 (5.8–7.5) | 6.9 (6.2–8.5) |
| SF-12 (PCS) | 44.3 (26.2–53.8) | 50.8 (27.7–53.4) | 48.4 (40.5–53.5) | 49.7 (42.4–52.4) * | 33.8 (26.2–54.9) | 30.9 (24.1–48.5) * |
| SF-12 (MCS) | 58.9 (33.2–62.2) | 59.9 (41.4–64.7) | 54.5 (50.3–60.7) | 57.9 (51.1–59.1) | 42.7 (31.6–59.8) | 42.1 (27.9–64.4) |
| Steps/day | 10,146.6 (6299–17,007) | 8769.5 (7321–10,404) | 7501 (5786.3–10,642.7) | 6921 (5913.3–10,509.1) | 7536.6 (3326.4–13,974.4) | 8142 (3225.7–18,870.9) |
| Walking duration (min) | 127.8 (90–194.4) | 119.4 (88.8–130.8) | 99.6 (78.6–143.6) | 99 (79.8–141.6) | 97.5 (53.8–171.6) | 112.2 (47.4–196.2) |
| Stand up duration (min) | 261.3 (228.6–301.8) | 270 (205.1–317.8) | 236.4 (180.9–321.6) | 254.4 (147.6–341.4) | 213.3 (121.2–268.7) | 242.4 (196.8–337.8) |
| Absolute time in SB (min) | 561 (333–616.8) | 598.8 (514.2–656.4) | 595.8 (445.4–616.4) | 545.4 (456–660) | 552.9 (482.4–739.2) | 543 (430.2–686.4) |
| Bouts < 30 min (min) | 246.3 (171.5–377.1) | 244.4 (220.7–407.1) | 220.9 (191.6–287.8) | 253.6 (199.4–338.7) | 277.6 (138.3–445.3) | 260.5 (181.1–369.2) |
| Bouts between 30 and 60 min (min) | 121.4 (75.7–166.7) | 152.6 (92.3–196.2) | 126.5 (96.1–147.1) | 125.3 (104.8–202.9) | 123.9 (41.9–157.5) | 151.9 (80.8–178.1) |
| Bouts > 60 min (min) | 126.3 (71.3–221.8) | 180.7 (84.2–211.5) | 164.4 (125.9–225.2) | 134.9 (94.1–217.7) | 165.8 (38.9–329.9) | 102.9 (53.3–282.9) |
| Sit-to-stand transitions (number) | 43.5 (35–67) | 49 (38–68) | 45 (36.2–47.9) | 49 (37.6–57.1) | 46.5 (30.6–85.3) | 39 (31.6–63.1) |
| Number of SB bouts < 30 min | 39 (30–64) | 44 (30–64) | 37 (30.1–42.9) | 45 (31.6–50.8) | 41.5 (26.9–82.6) | 34 (26.3–58.4) |
| Number of SB bouts between 30 and 60 min | 3 (2–4) | 3.5 (2–5) | 3 (2–3.9) | 3 (2–5) | 2.5 (0.7–4) | 4 (1.6–4) |
| Number of SB bouts > 60 min | 1.5 (1–2) | 2 (1–2) | 2 (1.8–2.9) | 2 (1–2) | 2 (0.7–3) | 1 (1–3) |
| LPA duration (min) | 104.3 (81.9–126.1) | 105.4 (81.2–107.5) | 92.8 (74.3–135.9) | 90.6 (64.1–131.77) | 104.3 (52.3–114.1) | 87.6 (37.8–111.9) |
| MVPA duration (min) | 25.2 (4.1–68.6) | 13.9 (6.6–24.1) | 11.2 (6.9–17.3) | 10.8 (3.4–18.9) | 25.2 (5.1–62.1) | 7.5 (1.5–113.1) |
| Participant Characteristics at Baseline | Follow-Up (n = 22) | Withdraw (n = 11) |
|---|---|---|
| n (%) | n (%) | |
| Sex | ||
| Female | 9 (40.9) | 3 (27.3) |
| Male | 13 (59.1) | 8 (72.7) |
| Years from diagnosis | ||
| >2 and <5 | 3 (13.6) | 4 (36.4) |
| >5 and <10 | 5 (22.7) | 2 (18.2) |
| <10 | 14 (63.6) | 5 (45.5) |
| Socioeconomic status | ||
| Low | 13 (59.1) | 9 (81.8) |
| Medium | 3 (13.6) | 1 (9.1) |
| High | 6 (27.3) | 1 (9.1) |
| Physically Active (APAFB) | ||
| No | 9 (40.9) | 3 (27.3) |
| Yes | 13 (59.1) | 8 (72.7) |
| Group | ||
| SENWI | 5 (50) | 5 (50) |
| NW | 9 (81.8) | 2 (18.2) |
| Control | 8 (66.7) | 4 (33.3) |
| Participant characteristics at baseline | Follow-up (n = 22) | Withdraw (n = 11) |
| Md (CI 95%) | Md (CI 95%) | |
| Age (years) | 69.5 (67–74) | 71 (69–74) |
| Waist circumference (cm) | 108.5 (100.6–111.2) | 111 (103.4–117.7) |
| BMI (kg/m2) | 30.8 (27.3–33.1) | 30.7 (27.6–35.1) |
| HbA1c (%) | 6.7 (6.2–7.2) | 6.9 (6.2–7.5) |
| SF-12 (PCS) | 43.5 (34.9–49.1) | 48.8 (32.6–53.7) |
| SF-12 (MCS) | 54.4 (44.4–59.1) | 55.7 (43.8–59.6) |
| Steps/day | 7531.1 (6438.7–9914.6) | 10,430 (5039.5–14,406.5) |
| Walking duration (min) | 99.6 (88.2–133.2) | 121.2 (72.6–180.6) |
| Stand-up duration (min) | 231.6 (208.8–268.8) | 250.2 (166.8–313.2) |
| Absolute time in SB (min) | 567.6 (519–608.4) | 561 (448.8–635.4) |
| Bouts < 30 min (min) | 236.9 (210.1–298.7) | 289.7 (203.7–348.1) |
| Bouts between 30 and 60 min (min) | 126.5 (88.1–150.3) | 145.7 (119.5–175.3) |
| Bouts > 60 min (min) | 164.4 (106.6–215.5) | 127.6 (66.1–236.5) |
| Sit-to-stand transitions (number) | 46 (38.9–49.1) | 44 (38.4–54.9) |
| Number of SB bouts < 30 min | 41 (34–43.5) | 40 (32.5–49) |
| Number of SB bouts between 30 and 60 min | 3 (2–4) | 3 (3–4) |
| Number of SB bouts > 60 min | 2 (1–2) | 1 (1–2.9) |
| LPA duration (min) | 89.1 (81.9–99.9) | 108.3 (60.9–115.7) |
| MVPA duration (min) | 10.3 (6.8–17.3) | 7.8 (2.1–59.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabardo-Camprubí, G.; Puig-Ribera, A.; Donat-Roca, R.; Farrés-Godayol, P.; Nazar-Gonzalez, S.; Sitjà-Rabert, M.; Espelt, A.; Bort-Roig, J. Assessing the Feasibility and Acceptability of a Primary Care Socio-Ecological Approach to Improve Physical Activity Adherence among People with Type 2 Diabetes: The SENWI Project. Healthcare 2023, 11, 1815. https://doi.org/10.3390/healthcare11131815
Jabardo-Camprubí G, Puig-Ribera A, Donat-Roca R, Farrés-Godayol P, Nazar-Gonzalez S, Sitjà-Rabert M, Espelt A, Bort-Roig J. Assessing the Feasibility and Acceptability of a Primary Care Socio-Ecological Approach to Improve Physical Activity Adherence among People with Type 2 Diabetes: The SENWI Project. Healthcare. 2023; 11(13):1815. https://doi.org/10.3390/healthcare11131815
Chicago/Turabian StyleJabardo-Camprubí, Guillem, Anna Puig-Ribera, Rafel Donat-Roca, Pau Farrés-Godayol, Sebastian Nazar-Gonzalez, Mercè Sitjà-Rabert, Albert Espelt, and Judit Bort-Roig. 2023. "Assessing the Feasibility and Acceptability of a Primary Care Socio-Ecological Approach to Improve Physical Activity Adherence among People with Type 2 Diabetes: The SENWI Project" Healthcare 11, no. 13: 1815. https://doi.org/10.3390/healthcare11131815
APA StyleJabardo-Camprubí, G., Puig-Ribera, A., Donat-Roca, R., Farrés-Godayol, P., Nazar-Gonzalez, S., Sitjà-Rabert, M., Espelt, A., & Bort-Roig, J. (2023). Assessing the Feasibility and Acceptability of a Primary Care Socio-Ecological Approach to Improve Physical Activity Adherence among People with Type 2 Diabetes: The SENWI Project. Healthcare, 11(13), 1815. https://doi.org/10.3390/healthcare11131815