
Putting the Gaming Experience at the Center of the Therapy—The Video Game Therapy® Approach



Abstract
Simple Summary
Abstract
1. Introduction
- Engagement: Video games are designed to be engaging and immersive, which can make them effective at keeping individuals focused and motivated during therapy sessions.
- Interactivity: Video games are interactive, allowing individuals to actively participate in therapy. This can be especially beneficial for individuals with difficulty in verbalizing their thoughts and feelings.
- Visual and auditory feedback: Video games can provide visual and auditory feedback, which can be used to reinforce positive behaviors and provide instant feedback on progress.
- Customization: Video games can be customized to suit the specific needs and goals of the individual. This can include tailoring the difficulty level, the type of game, and the session length.
- Variety: Video games offer a wide range of options, from action games to puzzles and simulations, which can help individuals find a type of game that they enjoy and are motivated to play.
- Accessibility: Video games can be accessed remotely, making the therapy more convenient for individuals who may have difficulty traveling to a therapy office.
- Assessment: Video games can be used to assess an individual’s cognitive abilities, such as memory, attention, and decision-making skills.
- Virtual Reality: Video games can be used in virtual reality environments, allowing individuals to experience immersive and realistic simulations of real-world scenarios. This can be particularly beneficial for individuals with phobias or other anxiety disorders.
2. Video Game Therapy—Putting Video Games Together with Therapy
- Promoting emotional experimentation with the other (therapist), activating emphatic processes, through activating the emotional and affective sphere.
- Promoting emotional literacy;
- Encouraging awareness of the primary emotion of “discovery”, as compensation for an inferiority complex;
- Promoting a social feeling, the game becomes a tool for mutual cooperation and sharing of internal dynamics;
- Promoting awareness of one’s role or identity at a given moment in life, thanks to the correlation between the real-life lifestyle of the game and the protagonist’s avatar or a character in the virtual story;
- Activating cognitive processes of imagery, ideomotor training, and self-regulation;
- Reactivating the state of Flow, promoting concentration and mental processes related to attention, as well as problem solving, critical thinking, team building, proactivity, and decision making.
- Facilitating communication of parts of the Self.
3. Therapeutic Process in Video Game Therapy and Tools
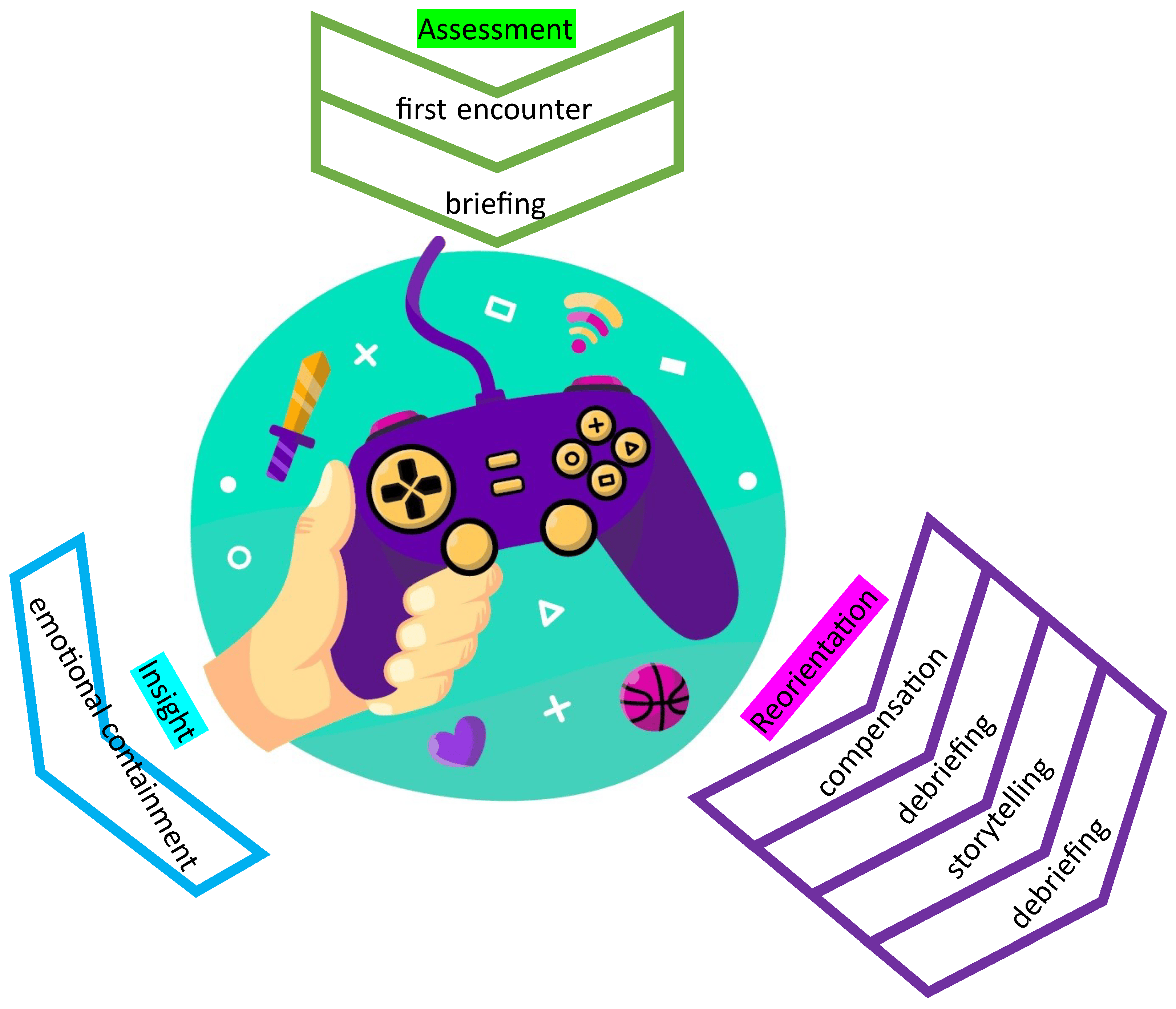
3.1. The Different Phases of the Process
3.2. Assessment and Play
3.3. Gaming and Flow State
- Clear goals: Subjects identify precise short-, medium-, and long-term goals and plan how to achieve them.
- Total concentration on the task: A high degree of engagement in a limited field of attention on the present. Attention is entirely focused on the action.
- Loss of self-awareness: The subject is so absorbed in the activity that they are unaware of it. They are aware of their actions, but it is as if they are not aware of this awareness.
- Distortion of the sense of time: Time perception is altered as one is completely absorbed in the experience and unaware of the passing of time.
- Direct and unambiguous feedback: The effect of the action is perceived by the subject immediately and clearly, providing unequivocal feedback.
- Balance between challenge and skill: The activity is proportionate to one’s abilities (therefore, there is no boredom or anxiety).
- Sense of control: A perception of complete control and ability to dominate the situation.
- Intrinsic pleasure: The action provides intrinsic satisfaction, which is an experience that is highly rewarding and satisfying, so much so that expressions such as “addicted to victory” or “addicted to success” are used.
- Integration between action and awareness: Concentration and effort encourage individuals to practice that activity, learn to understand their sensations better, and rediscover the maximum connection between mind and body.
3.4. Insight Phase
3.4.1. Knowledge of Feelings of Inferiority
3.4.2. Catharsis and Video Games
3.4.3. Desensitization
3.4.4. Exposition to Stimuli
3.5. Reorientation
Storytelling and Imaginative Techniques
4. The Foundation of the Individual Psychoanalytic Therapy Applied to Video Game Therapy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| VGT® | Video Game Therapy® |
| MBTI | Myers Briggs Type Indicator |
References
- Stenros, J. The Game Definition Game: A Review. Games Cult. 2017, 12, 499–520. [Google Scholar] [CrossRef]
- Huizinga, J. Homo Ludens—A Study of the Play Element in Culture; Beacon Press: Boston, MA, USA, 1950. [Google Scholar]
- Suits, B.; Hurka, T. The Grasshopper: Games, Life and Utopia; Broadview Press: Peterborough, ON, Canada, 2005. [Google Scholar]
- Salen, K.; Zimmerman, E. Rules of Play: Game Design Fundamentals; MIT Press: Cambridge, MA, USA, 2004; p. 672. [Google Scholar]
- Crawford, C. The Art of Computer Game Design; McGraw-Hill, Inc.: Chicago, IL, USA, 1984. [Google Scholar]
- Wilkinson, N.; Ang, R.P.; Goh, D.H. Online video game therapy for mental health concerns: A review. Int. J. Soc. Psychiatry 2008, 54, 370–382. [Google Scholar] [CrossRef]
- Bean, A. Working with Video Gamers and Games in Therapy: A Clinician’s Guide; Routledge: Milton Park, UK, 2018. [Google Scholar]
- Moreno, J.; Jonathan Fox, M. The Essential Moreno: Writings on Psychodrama, Group Method, and Spontaneity; Springer: Berlin/Heidelberg, Germany, 1987. [Google Scholar]
- Kowal, M.; Conroy, E.; Ramsbottom, N.; Smithies, T.; Toth, A.; Campbell, M. Gaming Your Mental Health: A Narrative Review on Mitigating Symptoms of Depression and Anxiety Using Commercial Video Games. JMIR Serious Games 2021, 9, e26575. [Google Scholar] [CrossRef] [PubMed]
- Moraes, T.M.; Zaninotto, A.L.; Neville, I.S.; Hayashi, C.Y.; Paiva, W.S. Immersive virtual reality in patients with moderate and severe traumatic brain injury: A feasibility study. Health Technol. 2021, 11, 1035–1044. [Google Scholar] [CrossRef]
- Tore, S.D.; Fulgione, M.; Sibilio, M. Dislessia e Videogames: Il Potenziale Didattico dei Videogiochi. Mediterr. J. Soc. Sci. 2014, 5, 1165. [Google Scholar]
- Evans, S.W.; Beauchaine, T.P.; Chronis-Tuscano, A.; Becker, S.P.; Chacko, A.; Gallagher, R.; Hartung, C.M.; Kofler, M.J.; Schultz, B.K.; Tamm, L.; et al. The Efficacy of Cognitive Videogame Training for ADHD and What FDA Clearance Means for Clinicians. Evid.-Based Pract. Child Adolesc. Ment. Health 2021, 6, 116–130. [Google Scholar] [CrossRef]
- Sokolov, A.A.; Collignon, A.; Bieler-Aeschlimann, M. Serious video games and virtual reality for prevention and neurorehabilitation of cognitive decline because of aging and neurodegeneration. Curr. Opin. Neurol. 2020, 33, 239–248. [Google Scholar] [CrossRef]
- Franceschini, S.; Bertoni, S. Improving action video games abilities increases the phonological decoding speed and phonological short-term memory in children with developmental dyslexia. Neuropsychologia 2019, 130, 100–106. [Google Scholar] [CrossRef]
- Ashinoff, B.K.; Abu-Akel, A. Hyperfocus: The forgotten frontier of attention. Psychol. Res. 2021, 85, 1–19. [Google Scholar] [CrossRef]
- Rohani, D.; Sørensen, H.; Puthusserypady, S. Brain-computer interface using P300 and virtual reality: A gaming approach for treating ADHD. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 3606–3609. [Google Scholar] [CrossRef]
- Anguera, J.A.; Brandes-Aitken, A.N.; Antovich, A.D.; Rolle, C.E.; Desai, S.S.; Marco, E.J. A pilot study to determine the feasibility of enhancing cognitive abilities in children with sensory processing dysfunction. PLoS ONE 2017, 12, e0172616. [Google Scholar] [CrossRef]
- Baniqued, P.; Kranz, M.; Voss, M.; Lee, H.; Cosman, J.; Severson, J.; Kramer, A. Cognitive training with casual video games: Points to consider. Front. Psychol. 2014, 4, 1010. [Google Scholar] [CrossRef]
- Jiménez-Muñoz, L.; Peñuelas-Calvo, I.; Calvo-Rivera, P.; Díaz-Oliván, I.; Moreno, M.; Baca-García, E.; Porras-Segovia, A. Video Games for the Treatment of Autism Spectrum Disorder: A Systematic Review. J. Autism Dev. Disord. 2022, 52, 169–188. [Google Scholar] [CrossRef]
- Pallavicini, F.; Pepe, A.; Mantovani, F. Commercial Off-The-Shelf Video Games for Reducing Stress and Anxiety: Systematic Review. JMIR Ment Health 2021, 8, e28150. [Google Scholar] [CrossRef]
- Ruiz, M.; Moreno, M.; Girela-Serrano, B.; Díaz-Oliván, I.; Muñoz, L.J.; González-Garrido, C.; Porras-Segovia, A. Winning The Game Against Depression: A Systematic Review of Video Games for the Treatment of Depressive Disorders. Curr. Psychiatry Rep. 2022, 24, 23–35. [Google Scholar] [CrossRef]
- Russoniello, C.V.; Fish, M.T.; O’Brien, K. The Efficacy of Playing Videogames Compared with Antidepressants in Reducing Treatment-Resistant Symptoms of Depression. Games Health J. 2019, 8, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Butler, O.; Herr, K.; Willmund, G.; Gallinat, J.; Kühn, S.; Zimmermann, P. Trauma, treatment and Tetris: Video gaming increases hippocampal volume in male patients with combat-related posttraumatic stress disorder. J. Psychiatry Neurosci. JPN 2020, 45, 279–287. [Google Scholar] [CrossRef]
- Iyadurai, L.; Blackwell, S.E.; Meiser-Stedman, R.; Watson, P.C.; Bonsall, M.B.; Geddes, J.R.; Nobre, A.C.; Holmes, E.A. Preventing intrusive memories after trauma via a brief intervention involving Tetris computer game play in the emergency department: A proof-of-concept randomized controlled trial. Mol. Psychiatry 2018, 23, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Al Husni Al Keilani, M.; Delvenne, V. Use of Video Games in a Child And Adolescent Psychiatric Unit. Psychiatr. Danub. 2020, 32, 167–171. [Google Scholar] [PubMed]
- Bean, A. Integrating Geek Culture into Therapeutic Practice: The Clinician’s Guide to Geek Therapy; Leyline Publishing: Fort Worth, TX, USA, 2020. [Google Scholar]
- Bocci, F.; Sala, E. Il videogioco come strumento creativo e terapeutico in Psicologia Individuale; l’approccio della Video Game Therapy. Riv. Di Psicol. Individ. Della Soc. Ital. Di Psicol. Individ. 2019, 86, 53–65. (In Italian) [Google Scholar]
- Bocci, F. (Ed.) Dentro il Videogioco. Viaggio Nella Psicologia dei Videogiochi e nei Suoi Ambiti Applicativi; Ananke Lab: Turin, Italy, 2019. [Google Scholar]
- Myers, I.B. The Myers-Briggs Type Indicator: Manual (1962); Consulting Psychologists Press: Palo Alto, CA, USA, 1962. [Google Scholar] [CrossRef]
- Bean, D.A. Video Gamers’ Personas: A Five Factor Study Exploring Personality Elements of the Video Gamer. Ph.D. Thesis, Pacifica Graduate Institute, Summerland, CA, USA, 2015. [Google Scholar]
- Bartle, R. Hearts, clubs, diamonds, spades: Players who suit MUDs. J. Mud Res. 1996, 1, 19. [Google Scholar]
- Csikszentmihalyi, M. Flow: The Psychology of Optimal Experience; Harper Collins: New York, NY, USA, 1990. [Google Scholar]
- Pallavicini, F.; Ferrari, A.; Pepe, A.; Garcea, G.; Zanacchi, A.; Mantovani, F. Effectiveness of Virtual Reality Survival Horror Games for the Emotional Elicitation: Preliminary Insights Using Resident Evil 7: Biohazard. In Proceedings of the Universal Access in Human-Computer Interaction. Virtual, Augmented, and Intelligent Environments: 12th International Conference, UAHCI 2018, Held as Part of HCI International 2018, Las Vegas, NV, USA, 15–20 July 2018; Proceedings, Part II. Springer: Berlin/Heidelberg, Germany, 2018; pp. 87–101. [Google Scholar] [CrossRef]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Moneta, G.B. The Flow Experience Across Cultures. J. Happiness Stud. 2004, 5, 115–121. [Google Scholar] [CrossRef]
- McGonigal, J. Reality Is Broken: Why Games Make Us Better and How They Can Change the World; Penguin Press: New York, NY, USA, 2011; p. 388. [Google Scholar]
- Ilies, R.; Wagner, D.; Wilson, K.; Ceja, L.; Johnson, M.; DeRue, S.; Ilgen, D. Flow at Work and Basic Psychological Needs: Effects on Well-Being. Appl. Psychol. 2016, 66, 3–24. [Google Scholar] [CrossRef]
- Popescu, M.; Romero, M.; Usart, M. Serious Games for Serious Learning Using SG for Business, Management and Defence Education. Int. J. Comput. Sci. Res. Appl. 2013, 3, 5–15. [Google Scholar]
- Juul, J. Half-Real: Video Games Between Real Rules and Fictional Worlds; MIT Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Salovey, P.; Mayer, J.D. Emotional intelligence. Imagin. Cogn. Personal. 1989, 9, 185–211. [Google Scholar] [CrossRef]
- Carissoli, C.; Villani, D. Can Videogames Be Used to Promote Emotional Intelligence in Teenagers? Results from EmotivaMente, a School Program. Games Health J. 2019, 8, 407–413. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.; Bhullar, N. The Assessing Emotions Scale; Springer: Berlin/Heidelberg, Germany, 2009; pp. 119–134. [Google Scholar] [CrossRef]
- Benedetti, W. Video Games Get Real and Grow up. 2010. Available online: https://www.nbcnews.com/id/wbna36968970 (accessed on 10 April 2023).
- Hemenover, S.; Bowman, N. Video games, emotion, and emotion regulation: Expanding the scope. Ann. Int. Commun. Assoc. 2018, 42, 125–143. [Google Scholar] [CrossRef]
- Colder Carras, M.; Kalbarczyk, A.; Wells, K.; Banks, J.; Kowert, R.; Gillespie, C.; Latkin, C. Connection, meaning, and distraction: A qualitative study of video game play and mental health recovery in veterans treated for mental and/or behavioral health problems. Soc. Sci. Med. (1982) 2018, 216, 124–132. [Google Scholar] [CrossRef]
- Rupp, M.A.; Sweetman, R.; Sosa, A.E.; Smither, J.A.; McConnell, D.S. Searching for Affective and Cognitive Restoration: Examining the Restorative Effects of Casual Video Game Play. Hum. Factors 2017, 59, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Desai, V.; Gupta, A.; Andersen, L.; Ronnestrand, B.; Wong, M. Stress-Reducing Effects of Playing a Casual Video Game among Undergraduate Students. Trends Psychol. 2021, 29, 563–579. [Google Scholar] [CrossRef]
- Rothblum, E.D. Fear of Failure-The Psychodynamic, Need Achievement, Fear of Success, and Procrastination Models. In Handbook of Social and Evaluation Anxiety; Leitenberg, H., Ed.; Springer: Boston, MA, USA, 1990; pp. 497–537. [Google Scholar] [CrossRef]
- McGregor, H.A.; Elliot, A.J. The Shame of Failure: Examining the Link Between Fear of Failure and Shame. Personal. Soc. Psychol. Bull. 2005, 31, 218–231. [Google Scholar] [CrossRef]
- Juul, J. The Art of Failure: An Essay on the Pain of Playing Video Games; Playful Thinking; MIT Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Beckett, S. Worstward Ho; Grove Press: New York, NY, USA, 1983. [Google Scholar]
- Aytemiz, B.; Smith, A.M. A Diagnostic Taxonomy of Failure in Videogames. In Proceedings of the FDG’20: International Conference on the Foundations of Digital Games, Bugibba, Malta, 15–18 September 2020; Yannakakis, G.N., Liapis, A., Kyburz, P., Volz, V., Khosmood, F., Lopes, P., Eds.; ACM: New York, NY, USA, 2020; pp. 18:1–18:11. [Google Scholar] [CrossRef]
- Costikyan, G. Uncertainty in Games; The MIT Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Bernhaupt, R. User Experience Evaluation in Entertainment and Games. In Proceedings of the Human-Computer Interaction—INTERACT 2011, Lisbon, Portugal, 5–9 September 2011; Campos, P., Graham, N., Jorge, J., Nunes, N., Palanque, P., Winckler, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 716–717. [Google Scholar]
- Kapur, M. Productive failure. Cogn. Instr. 2008, 26, 379–424. [Google Scholar] [CrossRef]
- Kapur, M.; Bielaczyc, K. Designing for productive failure. J. Learn. Sci. 2012, 21, 45–83. [Google Scholar] [CrossRef]
- Garris, R.; Ahlers, R.; Driskell, J.E. Games, Motivation, and Learning: A Research and Practice Model. Simul. Gaming 2002, 33, 441–467. [Google Scholar] [CrossRef]
- Foddy, B. Bennett Foddy on the Pitfalls of Perfectionism. 2018. Available online: https://thecreativeindependent.com/people/bennett-foddy-on-the-pitfalls-of-perfectionism/ (accessed on 20 April 2023).
- Harrer, S. From Losing to Loss: Exploring the Expressive Capacities of Videogames Beyond Death as Failure. Cult. Unbound: J. Curr. Cult. Res. 2013, 5, 607–620. [Google Scholar] [CrossRef]
- Rigby, C.S.; Przybylski, A.K. Virtual worlds and the learner hero: How today’s video games can inform tomorrow’s digital learning environments. Theory Res. Educ. 2009, 7, 214–223. [Google Scholar] [CrossRef]
- Przybylski, A.K.; Weinstein, N.; Murayama, K.; Lynch, M.F.; Ryan, R.M. The ideal self at play: The appeal of video games that let you be all you can be. Psychol. Sci. 2012, 23, 69–76. [Google Scholar] [CrossRef]
- Moran, C.; Voorhees, G.; Call, J.; Whitlock, K. The Generalization of Configurable Being: From RPGs to Facebook; Continuum: New York, NY, USA, 2012; pp. 343–362. [Google Scholar]
- Desario, N. Reconceptualizing Meritocracy: The Decline of Disparate Impact Discrimination Law. Harv. Law Rev. 2003, 38, 479. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Hojman, H. The positive use of video games and media in psychodynamic psychotherapy. Brown Univ. Child Adolesc. Behav. Lett. 2020, 36, 1–6. [Google Scholar] [CrossRef]
- Lee, E.J.; Kim, H.S.; Choi, S. Violent Video Games and Aggression: Stimulation or Catharsis or Both? Cyberpsychology, Behav. Soc. Netw. 2021, 24, 41–47. [Google Scholar] [CrossRef]
- Wolpe, J. Psychotherapy by Reciprocal Inhibition; Stanford University Press: Redwood City, CA, USA, 1958. [Google Scholar]
- Schindler, F.E. Treatment by systematic desensitization of a recurring nightmare of a real life trauma. J. Behav. Ther. Exp. Psychiatry 1980, 11, 53–54. [Google Scholar] [CrossRef]
- Frank, E.; Anderson, B.P.; Stewart, B.D.; Dancu, C.V.; Hughes, C.; West, D. Efficacy of cognitive behavior therapy and systematic desensitization in the treatment of rape trauma. Behav. Ther. 1988, 19, 403–420. [Google Scholar] [CrossRef]
- Harrer, S. Games and Bereavement: How Video Games Represent Attachment, Loss, and Grief; Transcript Verlag: Bielefeld, Germany, 2018. [Google Scholar] [CrossRef]
- Wolpe, J. Psychotherapy by reciprocal inhibition. Cond. Reflex A Pavlov. J. Res. Ther. 1968, 3, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Rachman, S. Studies in desensitization—II: Flooding. Behav. Res. Ther. 1966, 4, 10. [Google Scholar] [CrossRef]
- Gillihan, S.J.; Williams, M.T.; Malcoun, E.; Yadin, E.; Foa, E.B. Common Pitfalls in Exposure and Response Prevention (EX/RP) for OCD. J. Obs.-Compuls. Relat. Disord. 2012, 1, 251–257. [Google Scholar] [CrossRef]
- Moscovitch, D.A.; Antony, M.M.; Swinson, R.P. Exposure-Based Treatments for Anxiety Disorders: Theory and Process; Oxford Library of Psychology; Oxford University Press: New York, NY, USA, 2009; pp. 461–475. [Google Scholar]
- Foa, E.; Wilson, R. Venza Sus Obsesiones (Masters Salud (robin Book)); Ediciones S.L.: Guatemala City, Guatemala, 2016. (In Spanish) [Google Scholar]
- Foa, E.B.; Steketee, G.; Grayson, J.B. Imaginal and in vivo exposure: A comparison with obsessive-compulsive checkers. Behav. Ther. 1985, 16, 292–302. [Google Scholar] [CrossRef]
- Choy, Y.; Fyer, A.J.; Lipsitz, J.D. Treatment of specific phobia in adults. Clin. Psychol. Rev. 2007, 27, 266–286. [Google Scholar] [CrossRef] [PubMed]
- Murray, J. Hamlet on the Holodeck: The Future of Narrative in Cyberspace; Free Press: Los Angeles, CA, USA, 1997. [Google Scholar]
- Ermi, L.; Mäyrä, F. Player-Centred Game Design: Experiences in Using Scenario Study to Inform Mobile Game Design. Game Stud. 2005, 5, 1–10. [Google Scholar]
- Alexiou, A.; Schippers, M.; Oshri, I. Positive Psychology and Digital Games: The Role of Emotions and Psychological Flow in Serious Games Development. Psychology 2012, 3, 12. [Google Scholar] [CrossRef]
- Donchin, E. Video Games as research tools: The Space Fortress Game. Behav. Res. Methods Instrum. Comput. 1995, 27, 217–223. [Google Scholar] [CrossRef]
- Griffiths, M.; Kuss, D.; Ortiz de Gortari, A. Videogames as Therapy: An Updated Selective Review of the Medical and Psychological Literature. Int. J. Priv. Health Inf. Manag. 2017, 5, 71–96. [Google Scholar] [CrossRef]
- Washburn, D.A.; Gulledge, J.P. Game-like tasks for comparative research: Leveling the playing field. Behav. Res. Methods Instruments Comput. 1995, 27, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Horne-Moyer, H.L.; Moyer, B.H.; Messer, D.C.; Messer, E.S. The use of electronic games in therapy: A review with clinical implications. Curr. Psychiatry Rep. 2014, 16, 520. [Google Scholar] [CrossRef] [PubMed]
- Vincelli, F.; Riva, G. Virtual reality: A new tool for panic disorder therapy. Expert Rev. Neurother. 2002, 2, 377–383. [Google Scholar] [CrossRef]
- Wiederhold, B.K.; Wiederhold, M.D. Virtual Reality Therapy for Anxiety Disorders: Advances in Evaluation and Treatment; American Psychological Association: Worcester, MA, USA, 2005. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Adv. Behav. Res. Ther. 1978, 1, 139–161. [Google Scholar] [CrossRef]
- Wann, J.; Mon-Williams, M. What does virtual reality NEED?: Human factors issues in the design of three-dimensional computer environments. Int. J. Hum.-Comput. Stud. 1996, 44, 829–847. [Google Scholar] [CrossRef]
- North, M.M.; Schoeneman, C.M.; Mathis, J.R. Virtual Reality Therapy: Case study of fear of public speaking. Stud. Health Technol. Inform. 2002, 85, 318–320. [Google Scholar]
- Anderson, P.; Rothbaum, B. Virtual Reality as Treatment for Fear of Flying: A Review of Recent Research. Int. J. Behav. Consult. Ther. 2008, 4, 340–347. [Google Scholar] [CrossRef]
- Garcia-Palacios, A.; Hoffman, H.; Carlin, A.; Furness, T.A.R.; Botella, C. Virtual reality in the treatment of spider phobia: A controlled study. Behav. Res. Ther. 2002, 40, 983–993. [Google Scholar] [CrossRef]
- Walshe, D.G.; Lewis, E.J.; Kim, S.I.; O’Sullivan, K.; Wiederhold, B.K. Exploring the use of computer games and virtual reality in exposure therapy for fear of driving following a motor vehicle accident. Cyberpsychol. Behav. Impact Internet Multimed. Virtual Real. Behav. Soc. 2003, 6, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Coelho, C.M.; Waters, A.M.; Hine, T.J.; Wallis, G. The use of virtual reality in acrophobia research and treatment. J. Anxiety Disord. 2009, 23, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Aranda, F.; Jiménez-Murcia, S.; Santamaría, J.J.; Gunnard, K.; Soto, A.; Kalapanidas, E.; Bults, R.G.A.; Davarakis, C.; Ganchev, T.; Granero, R.; et al. Video games as a complementary therapy tool in mental disorders: PlayMancer, a European multicentre study. J. Ment. Health 2012, 21, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Colder Carras, M.; Van Rooij, A.J.; Spruijt-Metz, D.; Kvedar, J.; Griffiths, M.D.; Carabas, Y.; Labrique, A. Commercial Video Games as Therapy: A New Research Agenda to Unlock the Potential of a Global Pastime. Front. Psychiatry 2018, 8, 300. [Google Scholar] [CrossRef]
- Ceranoglu, T.A. Video Games in Psychotherapy. Rev. Gen. Psychol. 2010, 14, 141–146. [Google Scholar] [CrossRef]
- Derby, J.K. Virtual realities: The use of violent video games in U.S. military recruitment and treatment of mental disability caused by war. Disabil. Stud. Q. 2016, 36. [Google Scholar] [CrossRef]
- Schoneveld, E.A.; Malmberg, M.; Lichtwarck-Aschoff, A.; Verheijen, G.P.; Engels, R.C.; Granic, I. A neurofeedback video game (MindLight) to prevent anxiety in children: A randomized controlled trial. Comput. Hum. Behav. 2016, 63, 321–333. [Google Scholar] [CrossRef]
- Gackenbach, J.; Darlington, M.; Ferguson, M.L.; Boyes, A. Video game play as nightmare protection: A replication and extension. Dreaming 2013, 23, 97–111. [Google Scholar] [CrossRef]
- Holmes, E.A.; James, E.L.; Coode-Bate, T.; Deeprose, C. Can playing the computer game “Tetris” reduce the build-up of flashbacks for trauma? A proposal from cognitive science. PLoS ONE 2009, 4, e4153. [Google Scholar] [CrossRef]
- Ferrari, A.; Soraci, P. Ludonarrative Dissonance in The Last of Us Part II: Attempting to Create Empathy with a Villain. In Human Interaction & Emerging Technologies (IHIET 2022): Artificial Intelligence & Future Applications. AHFE (2022) International Conference. AHFE Open Access, Vol 68. AHFE International, USA; Ahram, T., Taiar, R., Eds.; IHIET: Nice, France, 2022; Volume 68. [Google Scholar] [CrossRef]
- Zhu, F. Computer games and the aesthetic practices of the self: Wandering, transformation, and transfiguration. Ph.D. Thesis, The University of Manchester, Manchester, UK, 2017. [Google Scholar]
- Cano, J.L.; Rebollar, R.; Sáenz, M.J. Simulation Games in the Project Management Environment. In Proceedings of the Games in Operations Management, IFIP TC5/WG5.7 Fourth International Workshop of the Special Interest Group on Integrated Production Management Systems and the European Group of University Teachers for Industrial Management EHTB, Ghent, Belgium, 26–29 November 1998; Riis, J.O., Smeds, R., Landeghem, R.V., Eds.; Kluwer: Alphen aan den Rijn, The Netherlands, 1998; Volume 170, pp. 113–124. [Google Scholar]
- Logas, H. Agency: A Character-Centric Approach to Single Player Digital Space Role Playing Games. Master’s Thesis, Georgia Institute of Technology, Atlanta, GA, USA, 2004. [Google Scholar]
- Jung, J.; Gillet, G. Psychotherapy mediated by videogames. Int. J. Psycho-Anal. 2021, 102, 281–296. [Google Scholar] [CrossRef] [PubMed]
- Kestenbaum, C.J. The creative process in child psychotherapy. Am. J. Psychother. 1985, 39, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Shubina, I. Creativity In Psychotherapy: The Possibilities Of Its Utilization. In Proceedings of the European Proceedings of Social and Behavioural Sciences, Brno, Czech Republic, 9–11 January 2017; pp. 99–111. [Google Scholar] [CrossRef]
- Klimczyk, P. The experience of playing video games as a possible building block for life story narratives. In Polskie Forum Psychologiczne. Uniwersytet Kazimierza Wielkiego w Bydgoszczy; Wydawnictwo Uniwersytetu Kazimierza Wielkiego w Bydgoszczy: Bydgoszcz, Poland, 2021; pp. 191–214. [Google Scholar] [CrossRef]
- Tokarska, U. Status podejścia narracyjnego we współczesnej psychologii [Status of narrative psychology in contemporary psychology]. Czas. Psychol. 2014, 20, 65–71. (In Polish) [Google Scholar]
- Adler, J.M.; Dunlop, W.L.; Fivush, R.; Lilgendahl, J.P.; Lodi-Smith, J.; McAdams, D.P.; McLean, K.C.; Pasupathi, M.; Syed, M. Research Methods for Studying Narrative Identity: A Primer. Soc. Psychol. Personal. Sci. 2017, 8, 519–527. [Google Scholar] [CrossRef]
- Baszczak, B. Tożsamość człowieka a pojęcie narracji (Human identity and narration). Analiza i Egzystencja. Czasopismo Filozoficzne 2011, 14, 123–140. (In Polish) [Google Scholar]
- Fivush, R.; Merrill, N. An ecological systems approach to family narratives. Mem. Stud. 2016, 9, 305–314. [Google Scholar] [CrossRef]
- Boydell, K.; Cheng, C.; Gladstone, B.; Nadin, S.; Stasiulis, E. Co-Producing Narratives on Access to Care in Rural Communities: Using Digital Storytelling to Foster Social Inclusion of Young People Experiencing Psychosis (Dispatch). Vis. Res. Soc. Justice 2017, 11, 298. [Google Scholar] [CrossRef]
- Meyer, T.; Ikani, N.; Morina, N. Spatio-temporal associations with memory cues are linked to analogue traumatic intrusions. Behav. Res. Ther. 2019, 123, 103481. [Google Scholar] [CrossRef] [PubMed]
- Klein, M. The Psycho-Analysis of Children; W W Norton & Co: New York, NY, USA, 1932; p. 393. [Google Scholar]
- Ferro, A. Psychoanalysis As Therapy and Storytelling. In New Library of Psychoanalysis; Routledge: London, UK, 2006. [Google Scholar]
- Carlson, J.; Englar-Carlson, M. Adlerian Psychotherapy; Theories of Psychotherapy Series; American Psychological Association: Washington, DC, USA, 2017. [Google Scholar] [CrossRef]
- Ferrigno, G. L’analisi e la Psicoterapia Psicodinamica Secondo il Modello Adleriano. Riv. Psicol. Individ. 2001, 49, 15–27. (In Italian) [Google Scholar]
- Winnicott, D. Playing and Reality; Routledge Classics Series; Routledge: Oxfordshire, UK, 1991. [Google Scholar]
- Propp, V. Morfologia Della Fiaba; Nuova biblioteca scientifica Einaudi, Einaudi: Turin, Italy, 1969. (In Italian) [Google Scholar]
- Gaggioli, A.; Riva, G.; Milani, L.; Mazzoni, E. Networked Flow. Towards an Understanding of Creative Networks; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Alvarez, A.; Reid, S. Autism and Personality: Findings from the Tavistock Autism Workshop; Taylor & Frances/Routledge: Florence, KY, USA, 1999. [Google Scholar]
- Shulman, Y.; Saroff, A. “Imagination for Two” Child Psychotherapy during Coronavirus Outbreak: Building a Space for Play When Space Collapses. J. Infant Child Adolesc. Psychother. 2020, 19, 339–345. [Google Scholar] [CrossRef]
- Greenberg, L.S. Emotion-Focused Therapy; Theories of psychotherapy; American Psychological Association: Washington, DC, USA, 2011. [Google Scholar]
- Frijda, N.H. The Emotions, Studies in Emotion and Social Interaction; Editions de la Maison des Sciences de l’Homme: Paris, France, 1986; p. 544. [Google Scholar]
- Greenberg, L.S.; Paivio, S.C. Working with Emotions in Psychotherapy; The Practicing Professional; Guilford Press: New York, NY, USA, 1997. [Google Scholar]
- Greenberg, L. Emotion–focused therapy. Clin. Psychol. Psychother. 2004, 11, 3–16. [Google Scholar] [CrossRef]
- LeDoux, J.E. The Emotional Brain: The Mysterious Underpinnings of Emotional Life; Simon & Schuster: New York, NY, USA, 1996; p. 384. [Google Scholar]
- Greenberg, L. Emotion-Focused Therapy: A Clinical Synthesis. FOCUS 2010, 8, 32–42. [Google Scholar] [CrossRef]
- Rice, L.; Greenberg, L. (Eds.) Patterns of Change: Intensive Analysis of Psychotherapy Process; Guilford Publications: New York, NY, USA, 1984. [Google Scholar]
- Rogers, C. A Theory of Therapy, Personality, and Interpersonal Relationships: As Developed in the Client-Centered Framework; McGraw-Hill: New York, NY, USA, 1959; Volume 3. [Google Scholar]
- Greenberg, L.S.; Johnson, S.M. Emotionally Focused Therapy for Couples; Greenberg, L.S., Johnson, S.M., Eds.; Guilford Press New York: New York, NY, USA, 1988. [Google Scholar]
- Greenberg, L.S. Emotion-Focused Therapy: Coaching Clients to Work through Their Feelings; American Psychological Association: Washington, DC, USA, 2002. [Google Scholar] [CrossRef]
- Zimbardo, P.; Ebbesen, E.; Ebbesen, E.; Maslach, C. Influencing Attitudes and Changing Behavior: An Introduction to Method, Theory, and Applications of Social Control and Personal Power; Science Series for the Young; Addison-Wesley Publishing Company: London, UK, 1977. [Google Scholar]
- Gaut, B. A Philosophy of Cinematic Art; Cambridge University Press: Cambridge, CA, USA, 2010. [Google Scholar] [CrossRef]
- Rice, R. Video Games in Psychotherapy, 1st ed.; Routledge: Oxfordshire, UK, 2022. [Google Scholar]
- Gillet, G. Réflexions sur les psychothérapies par le jeu vidéo [Reflections on psychotherapy through video games]. L’Évolution Psychiatr. 2021, 86, 363–374. (In French) [Google Scholar] [CrossRef]
- Arenas, D.L.; Viduani, A.; Araujo, R.B. Therapeutic Use of Role-Playing Game (RPG) in Mental Health: A Scoping Review. Simul. Gaming 2022, 53, 285–311. [Google Scholar] [CrossRef]
- Zayeni, D.; Raynaud, J.P.; Revet, A. Therapeutic and Preventive Use of Video Games in Child and Adolescent Psychiatry: A Systematic Review. Front. Psychiatry 2020, 11, 36. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.D.; Kuss, D.J.; de Gortari, A.B.O. Videogames as therapy: An updated selective review of the medical and psychological literature. In Alternative Pain Management: Solutions for Avoiding Prescription Drug Overuse; IGI Global: Hershey, PA, USA, 2020; pp. 324–363. [Google Scholar] [CrossRef]


{kind=link}
| Personality Typology | Game |
|---|---|
| Analysts | |
| Architect—INTJ | Tetris;Monument Valley2; Thomas Was Alone; Inscryption |
| Logician—INTP | Dorfromantik; Don’t Starve Together; Security Booth: Director’s Cut; Green Heel |
| Commander—ENTJ | Valiant Hearths: The Great War; 35MM; Saturnalia; This War Of Mine |
| Debater—ENTP | The Last Campfire; Syberia: The World Before; How Fish Is Made; Mothered |
| Diplomats | |
| Advocate—INFJ | Tiny Lands; House Flipper; Townscraper; Death Stranding |
| Mediator—INFP | Night In The Woods; Coffee Talk; Life Is Strange; Detroit: Become Human |
| Protagonist—ENFJ | Overcooked: All You Can Eat; Among Us; Cult Of The Lamb; The Walking Dead: The Talltale Series |
| Campaigner—ENFP | Feather; Penguins Can Fly; Minecraft; My Summer Car |
| Sentinels | |
| Logistician—ISTJ | We Were Here Together; Pentiment; For Goodness Sake; She Sees Red: Interactive Thriller |
| Defender—ISFJ | ICO; Stray; It Takes Two; Little Misfortune |
| Executive—ESTJ | Oxygen Not Included; Yes, Your Grace; Papers, Please; Not For Broadcast |
| Consul—ESFJ | Animal Crossing: New Horizons; Hokko Life; The Last Guardian; A Normal Lost Phone |
| Explorers | |
| Virtuoso—ISTP | Freud’s Bones; Road96; Fear To Fathom: Home Alone; Scorn |
| Adventurer—ISFP | Tunic; Little Orpheus; Epystory—Typing Chronicles; The Pathless |
| Entrepreneur—ESTP | Horizon Chase 2; Getting Over It With Bennett Foddy; Cuphead; The Binding Of Isaac |
| Entertainer—ESFP | Untitled Goose Game; Crypt Of The Necromancer; Find The Murderer 2; Dude Simulator 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bocci, F.; Ferrari, A.; Sarini, M. Putting the Gaming Experience at the Center of the Therapy—The Video Game Therapy® Approach. Healthcare 2023, 11, 1767. https://doi.org/10.3390/healthcare11121767
Bocci F, Ferrari A, Sarini M. Putting the Gaming Experience at the Center of the Therapy—The Video Game Therapy® Approach. Healthcare. 2023; 11(12):1767. https://doi.org/10.3390/healthcare11121767
Chicago/Turabian StyleBocci, Francesco, Ambra Ferrari, and Marcello Sarini. 2023. "Putting the Gaming Experience at the Center of the Therapy—The Video Game Therapy® Approach" Healthcare 11, no. 12: 1767. https://doi.org/10.3390/healthcare11121767
APA StyleBocci, F., Ferrari, A., & Sarini, M. (2023). Putting the Gaming Experience at the Center of the Therapy—The Video Game Therapy® Approach. Healthcare, 11(12), 1767. https://doi.org/10.3390/healthcare11121767