
Role of Natural Products in the Management of COVID-19: A Saudi Arabian Perspective


 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Participants and Settings
2.2. Determination of Sample Size
2.3. Study Questionnaire, Validation and Pretest
2.4. Study Questionnaire
2.4.1. Sociodemographic Characteristics
2.4.2. COVID-19 Infection Status
2.4.3. Use of NPs in the Treatment of Diseases
2.4.4. Use of NPs for the Treatment of COVID-19
2.5. Data Analysis
3. Results
3.1. Sociodemographic Characteristics of the Participants
3.2. Sociodemographic Characteristics with the Use of NPs for Disease Management
3.3. Sociodemographic Characteristics and the Use of NPs for COVID-19
3.4. The Use of NPs for COVID-19 and Their Practices
3.5. The Use of NPs during COVID-19 and Its Outcomes
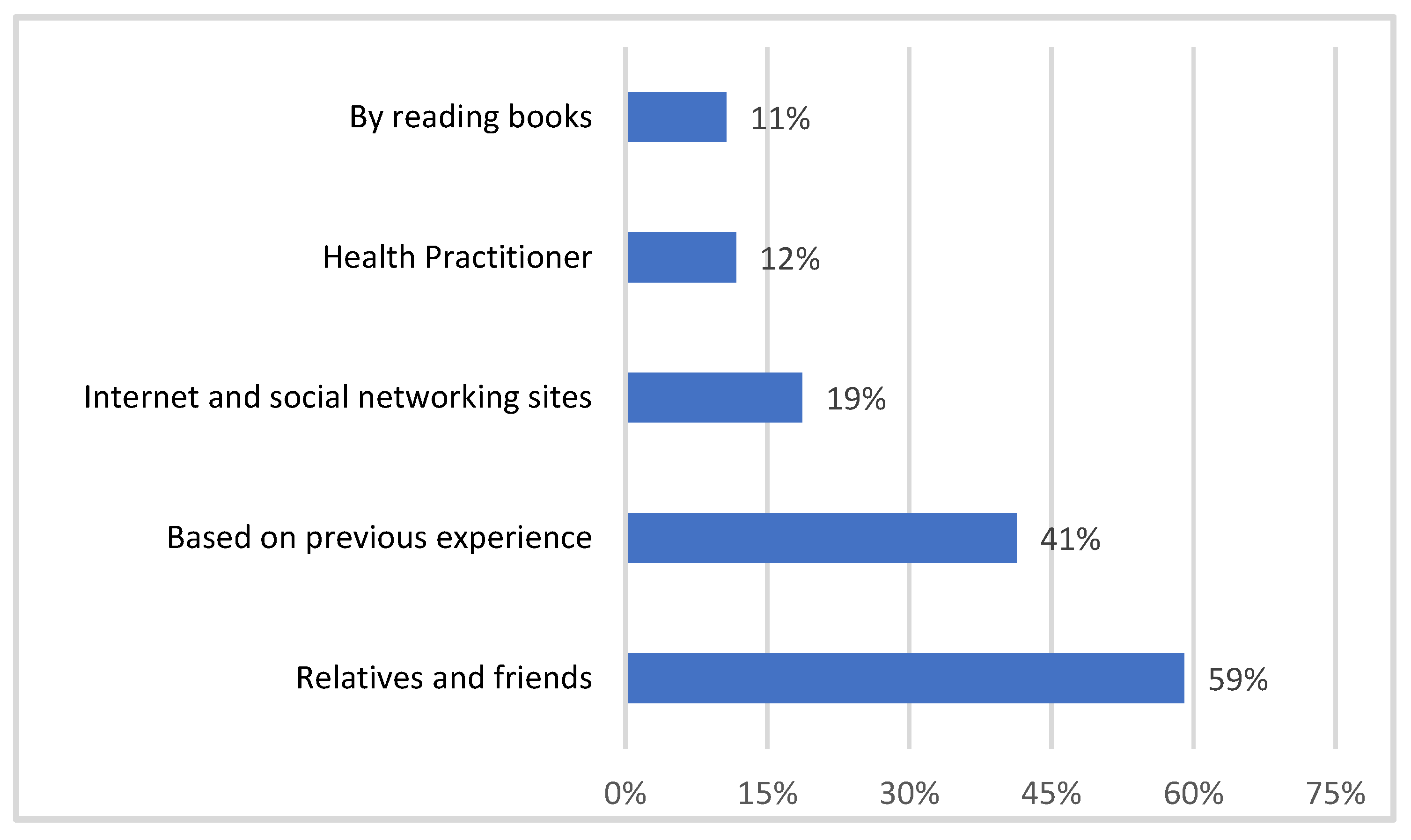
3.6. Sources of Information for the Use of NPs
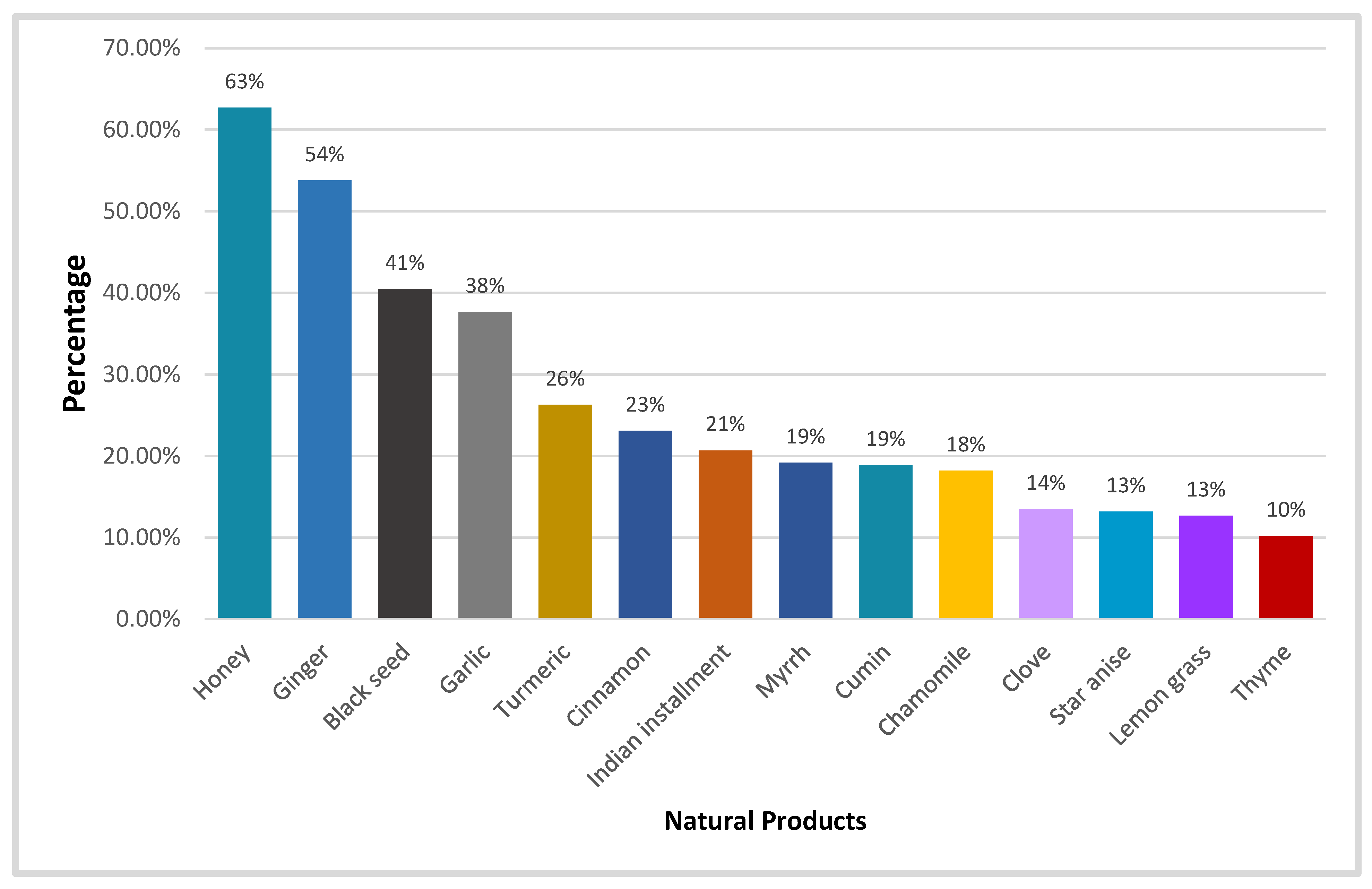
3.7. Distribution of Most Utilized NPs for COVID-19
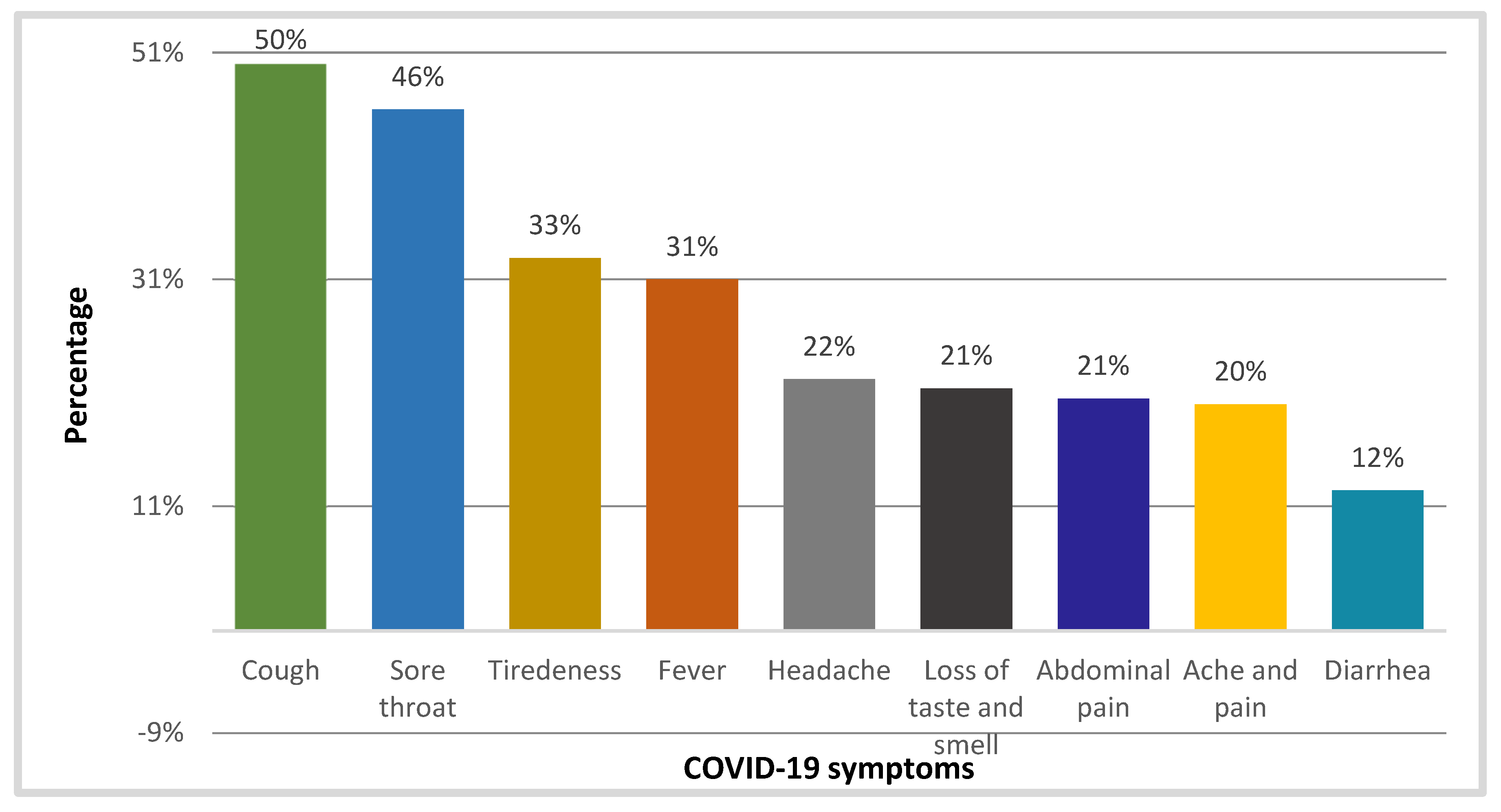
3.8. Distribution of COVID-19 Symptoms for Which NPs Are Used
3.9. Stepwise Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Rai, P.; Kumar, B.K.; Deekshit, V.K.; Karunasagar, I.; Karunasagar, I. Detection technologies and recent developments in the diagnosis of COVID-19 infection. Appl. Microbiol. Biotechnol. 2021, 105, 441–455. [Google Scholar] [CrossRef]
- Available online: https://www.worldometers.info/coronavirus/ (accessed on 9 May 2023).
- Böger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am. J. Infect. Control. 2020, 49, 21–29. [Google Scholar] [CrossRef]
- Pribanić Matešić, M.; Kučan Brlić, P.; Lenac Roviš, T.; Mačak Šafranko, Ž.; Chaouat, A.E.; Miklić, K.; Malić, S.; Ivanković, N.; Schubert, M.; Bertoglio, F.; et al. Collection of Monoclonal Antibodies Targeting SARS-CoV-2 Proteins. Viruses 2022, 14, 443. [Google Scholar] [CrossRef]
- Yang, L.; Wang, Z. Natural Products, Alone or in Combination with FDA-Approved Drugs, to Treat COVID-19 and Lung Cancer. Biomedicines 2021, 9, 689. [Google Scholar] [CrossRef]
- Warrer, M.M.; Granholm, A.; Nainan, S.M.; Kumar, B.T.V.; Cronhjort, M.; Rubenson, R.W.; Jakob, S.M.; Cioccari, L.; Kjær, M.; Vesterlund, G.; et al. Higher vs lower doses of dexamethasone in patients with COVID-19 and severe hypoxia (COVID STEROID 2) trial: Protocol and statistical analysis plan. Acta Anaesthesiol. Scand. 2021, 65, 834–845. [Google Scholar]
- Young, B.; Tan, T.T.; Leo, Y.S. The place for remdesivir in COVID-19 treatment. Lancet Infect. Dis. 2020, 21, 20–21. [Google Scholar] [CrossRef]
- Gandhi, S.; Klein, J.; Robertson, A.J.; Peña-Hernández, M.A.; Lin, M.J.; Roychoudhury, P.; Lu, P.; Fournier, J.; Ferguson, D.; Bakhash, S.A.K.M.; et al. De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: A case report. Nat. Commun. 2022, 13, 1547. [Google Scholar] [CrossRef]
- Aschenbrenner, D.S. Monoclonal Antibodies Receive EUA to Treat Mild to Moderate COVID-19. AJN Am. J. Nurs. 2021, 121, 26. [Google Scholar] [CrossRef]
- Dhand, A.; Lobo, S.A.; Wolfe, K.; Feola, N.; Lee, L.; Nog, R.; Chen, D.; Glicklich, D.; Diflo, T.; Nabors, C. Casirivimab-imdevimab for Treatment of COVID-19 in Solid Organ Transplant Recipients: An Early Experience. Transplantation 2021, 105, e68–e69. [Google Scholar] [CrossRef]
- Bignardi, P.R.; Vengrus, C.S.; Aquino, B.M.; Neto, A.C. Use of hydroxychloroquine and chloroquine in patients with COVID-19: A meta-analysis of randomized clinical trials. Ann. Trop. Med. Parasitol. 2021, 115, 139–150. [Google Scholar] [CrossRef]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Aljindan, R.Y.; Al-Subaie, A.M.; Al-Ohali, A.I.; Thirumal Kumar, D.; George Priya Doss, C.; Kamaraj, B. Investigation of nonsynonymous mutations in the spike protein of SARS-CoV-2 and its interaction with the ACE2 receptor by molecular docking and MM/GBSA approach. Comput. Biol. Med. 2021, 135, 104654. [Google Scholar] [CrossRef] [PubMed]
- Borgio, J.F.; Alsuwat, H.S.; Al Otaibi, W.M.; Ibrahim, A.M.; Almandil, N.; Al Asoom, L.I.; Salahuddin, M.; Kamaraj, B.; AbdulAzeez, S. State-of-the-art tools unveil potent drug targets amongst clinically approved drugs to inhibit helicase in SARS-CoV-2. Arch. Med. Sci. 2020, 16, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Huang, J.; Zhang, L.; Chen, S.; Gao, J.; Jiao, H. The global transmission of new coronavirus variants. Environ. Res. 2021, 206, 112240. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Chaudhary, V. Biotherapeutics and its applications in Microbiology. Environ. Conserv. J. 2021, 22, 63–78. [Google Scholar] [CrossRef]
- Bent, S. Herbal Medicine in the United States: Review of Efficacy, Safety, and Regulation. J. Gen. Intern. Med. 2008, 23, 854–859. [Google Scholar] [CrossRef]
- Atanasov, A.G.; Waltenberger, B.; Pferschy-Wenzig, E.-M.; Linder, T.; Wawrosch, C.; Uhrin, P.; Temml, V.; Wang, L.; Schwaiger, S.; Heiss, E.H.; et al. Discovery and resupply of pharmacologically active plant-derived natural products: A review. Biotechnol. Adv. 2015, 33, 1582–1614. [Google Scholar] [CrossRef]
- Harvey, A.L.; Edrada-Ebel, R.; Quinn, R.J. The re-emergence of natural products for drug discovery in the genomics era. Nat. Rev. Drug Discov. 2015, 14, 111–129. [Google Scholar] [CrossRef]
- Waltenberger, B.; Mocan, A.; Šmejkal, K.; Heiss, E.H.; Atanasov, A.G. Natural Products to Counteract the Epidemic of Cardiovascular and Metabolic Disorders. Molecules 2016, 21, 807. [Google Scholar] [CrossRef]
- Tintore, M.; Vidal-Jordana, A.; Sastre-Garriga, J. Treatment of multiple sclerosis—Success from bench to bedside. Nat. Rev. Neurol. 2019, 15, 53–58. [Google Scholar] [CrossRef]
- Lachance, H.; Wetzel, S.; Kumar, K.; Waldmann, H. Charting, Navigating, and Populating Natural Product Chemical Space for Drug Discovery. J. Med. Chem. 2012, 55, 5989–6001. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Kivimäki, M.; Gale, C.R.; Batty, G.D. Lifestyle risk factors, inflammatory mechanisms, and COVID-19 hospitalization: A community-based cohort study of 387,109 adults in UK. Brain Behav. Immun. 2020, 87, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Brüggen, M.-C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Morais, A.H.D.A.; Aquino, J.D.S.; da Silva-Maia, J.K.; Vale, S.H.D.L.; Maciel, B.L.L.; Passos, T.S. Nutritional status, diet and viral respiratory infections: Perspectives for severe acute respiratory syndrome coronavirus 2. Br. J. Nutr. 2020, 125, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Briguglio, M.; Pregliasco, F.E.; Lombardi, G.; Perazzo, P.; Banfi, G. The malnutritional status of the host as a virulence factor for new Coronavirus SARS-CoV-2. Front. Med. 2020, 7, 146. [Google Scholar] [CrossRef] [PubMed]
- Panyod, S.; Ho, C.-T.; Sheen, L.-Y. Dietary therapy and herbal medicine for COVID-19 prevention: A review and perspective. J. Tradit. Complement. Med. 2020, 10, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Conlon, M.; Ren, W.; Chen, B.B.; Bączek, T. Natural products as targeted nodulators of the immune system. J. Immunol. Res. 2018, 2018, 7862782. [Google Scholar] [CrossRef]
- Diederich, M. Natural products target the hallmarks of chronic diseases. Biochem. Pharmacol. 2020, 173, 113828. [Google Scholar] [CrossRef]
- Lin, L.T.; Hsu, W.C.; Lin, C.C. Antiviral natural products and herbal medicines. J. Tradit. Complement. Med. 2014, 4, 24–35. [Google Scholar] [CrossRef]
- Ang, L.; Lee, H.W.; Choi, J.Y.; Zhang, J.; Lee, M.S. Herbal medicine and pattern identification for treating COVID-19: A rapid review of guidelines. Integr. Med. Res. 2020, 9, 100407. [Google Scholar] [CrossRef] [PubMed]
- El Alami, A.; Fattah, A.; Abderrahman, C. Medicinal Plants used for the Prevention Purposes during the COVID-19 Pandemic in Morocco. J. Anal. Sci. Appl. Biotechnol. 2020, 2, 4–11. [Google Scholar]
- Ang, L.; Song, E.; Lee, H.W.; Lee, M.S. Herbal Medicine for the Treatment of Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 1583. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, N.; Yang, L.; Song, X.-Q. Bioactive natural products in COVID-19 therapy. Front. Pharmacol. 2022, 13, 6507. [Google Scholar] [CrossRef]
- Demeke, C.A.; Woldeyohanins, A.E.; Kifle, Z.D. Herbal medicine use for the management of COVID-19: A review article. Metab. Open 2021, 12, 100141. [Google Scholar] [CrossRef] [PubMed]
- Aldwihi, L.A.; Khan, S.I.; Alamri, F.F.; AlRuthia, Y.; Alqahtani, F.; Fantoukh, O.I.; Assiri, A.; Almohammed, O.A. Patients’ Behavior Regarding Dietary or Herbal Supplements before and during COVID-19 in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 5086. [Google Scholar] [CrossRef]
- Alyami, H.S.; Orabi, M.A.; Aldhabbah, F.M.; Alturki, H.N.; Aburas, W.I.; Alfayez, A.I.; Alharbi, A.S.; Almasuood, R.A.; Alsuhaibani, N.A. Knowledge about COVID-19 and beliefs about and use of herbal products during the COVID-19 pandemic: A cross-sectional study in Saudi Arabia. Saudi Pharm. J. 2020, 28, 1326–1332. [Google Scholar] [CrossRef]
- Alkharashi, N. The consumption of nutritional supplements and herbal products for the prevention and treatment of COVID-19 infection among the Saudi population in Riyadh. Clin. Nutr. Open Sci. 2021, 39, 11–20. [Google Scholar] [CrossRef]
- AlNajrany, S.M.; Asiri, Y.; Sales, I.; AlRuthia, Y. The Commonly Utilized Natural Products during the COVID-19 Pandemic in Saudi Arabia: A Cross-Sectional Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 4688. [Google Scholar] [CrossRef]
- Villena-Tejada, M.; Vera-Ferchau, I.; Cardona-Rivero, A.; Zamalloa-Cornejo, R.; Quispe-Florez, M.; Frisancho-Triveño, Z.; Abarca-Meléndez, R.C.; Alvarez-Sucari, S.G.; Mejia, C.R.; Yañez, J.A. Use of medicinal plants for COVID-19 prevention and respiratory symptom treatment during the pandemic in Cusco, Peru: A cross-sectional survey. PLoS ONE 2021, 16, e0257165. [Google Scholar] [CrossRef]
- Jahan, I.; Onay, A. Potentials of plant-based substance to inhabit and probable cure for the COVID-19. Turk. J. Biol. 2020, 44, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Jamiu, A.T.; Aruwa, C.E.; Abdulakeem, I.A.; Ajao, A.A.-N.; Sabiu, S. Phytotherapeutic Evidence Against Coronaviruses and Prospects for COVID-19. Pharmacogn. J. 2020, 12, 1252–1267. [Google Scholar] [CrossRef]
- Al-Hatamleh, M.A.I.; Hatmal, M.M.; Sattar, K.; Ahmad, S.; Mustafa, M.Z.; Bittencourt, M.D.C.; Mohamud, R. Antiviral and Immunomodulatory Effects of Phytochemicals from Honey against COVID-19: Potential Mechanisms of Action and Future Directions. Molecules 2020, 25, 5017. [Google Scholar] [CrossRef] [PubMed]
- Shariatpanahi, Z.V.; Taleban, F.A.; Mokhtari, M.; Shahbazi, S. Ginger extract reduces delayed gastric emptying and nosocomial pneumonia in adult respiratory distress syndrome patients hospitalized in an intensive care unit. J. Crit. Care 2010, 25, 647–650. [Google Scholar] [CrossRef]
- Kulkarni, R.A.; Deshpande, A.R. Anti-inflammatory and antioxidant effect of ginger in tuberculosis. J. Complement. Integr. Med. 2016, 13, 201–206. [Google Scholar] [CrossRef]
- Forouzanfar, F.; Bazzaz, B.S.F.; Hosseinzadeh, H. Black cumin (Nigella sativa) and its constituent (thymoquinone): A review on antimicrobial effects. Iran. J. Basic Med. Sci. 2014, 17, 929–938. [Google Scholar] [CrossRef]
- Koca, I.; Tasci, B. Garlic as a functional food. In VII International Symposium on Edible Alliaceae; Acta Horticulturae: Nigde, Turkey, 2016; pp. 139–146. [Google Scholar]
- Khubber, S.; Hashemifesharaki, R.; Mohammadi, M.; Gharibzahedi, S.M.T. Garlic (Allium sativum L.): A potential unique therapeutic food rich in organosulfur and flavonoid compounds to fight with COVID-19. Nutr. J. 2020, 19, 124. [Google Scholar] [CrossRef]
- Donma, M.M.; Donma, O. The effects of allium sativum on immunity within the scope of COVID-19 infection. Med. Hypotheses 2020, 144, 109934. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, M.; He, L.; Li, Y. Chinese herbs combined with Western medicine for severe acute respiratory syndrome (SARS). Cochrane Database Syst. Rev. 2012, 10, CD004882. [Google Scholar] [CrossRef]
- Asdaq, S.M.B.; Inamdar, M.N. Pharmacodynamic interaction of garlic with hydrochlorothiazide in rats. Indian J. Physiol. Pharmacol. 2010, 53, 127–136. [Google Scholar]
- Izzo, A.A. Interactions between Herbs and Conventional Drugs: Overview of the Clinical Data. Med. Princ. Pract. 2012, 21, 404–428. [Google Scholar] [CrossRef] [PubMed]
- Capell, T.; Twyman, R.M.; Armario-Najera, V.; Ma, J.K.-C.; Schillberg, S.; Christou, P. Potential Applications of Plant Biotechnology against SARS-CoV-2. Trends Plant Sci. 2020, 25, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Fischer, R.; Buyel, J.F. Molecular farming—The slope of enlightenment. Biotechnol. Adv. 2020, 40, 107519. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Options | Use of NPs for Disease Management, [n (%)] | Total (677) | p Value * | ||
|---|---|---|---|---|---|---|
| Always | Sometime | Never | ||||
| Age | 18–25 | 52 (29) | 99 (55) | 28 (16) | 179 | 0.048 |
| 26–40 | 128 (38) | 166 (49) | 42 (13) | 336 | ||
| More than 40 years | 55 (34) | 95 (59) | 12 (7) | 162 | ||
| Gender | Female | 182 (37) | 254 (52) | 50 (10) | 486 | 0.013 |
| Male | 53 (28) | 106 (55) | 32 (17) | 191 | ||
| Nationality | Saudi | 178 (35) | 270 (53) | 57 (11) | 505 | 0.519 |
| Non-Saudi | 57 (33) | 90 (52) | 25 (14) | 172 | ||
| Geographical location | Central region | 115 (31) | 208 (56) | 48 (13) | 371 | 0.069 |
| Eastern region | 26 (50) | 18 (35) | 8 (15) | 52 | ||
| Northern region | 17 (29) | 32 (55) | 9 (15) | 58 | ||
| Southern region | 18 (45) | 19 (47) | 3 (7) | 40 | ||
| Western region | 59 (38) | 83 (53) | 14 (9) | 156 | ||
| Educational level | Intermediate school | 5 (18) | 21 (75) | 2 (7) | 28 | 0.061 |
| High school diploma | 48 (29) | 96 (57) | 23 (14) | 167 | ||
| Undergraduate | 159 (38) | 213 (51) | 46 (11) | 418 | ||
| Postgraduate degree | 23 (36) | 30 (47) | 11 (17) | 64 | ||
| Employment status | Employed | 123 (34) | 197 (54) | 45 (12) | 365 | 0.001 |
| Not employed | 100 (45) | 92 (42) | 28 (13) | 220 | ||
| Student | 12 (13) | 71 (77) | 9 (10) | 92 | ||
| Marital status | Married | 146 (38) | 199 (52) | 38 (10) | 383 | 0.008 |
| Single | 73 (28) | 149 (57) | 41 (16) | 263 | ||
| Separated | 16 (52) | 12 (39) | 3 (10) | 31 | ||
| Family income | Less than SAR 5000 | 51 (35) | 67 (46) | 27 (19) | 145 | 0.060 |
| SAR 5000–10,000 | 74 (36) | 112 (55) | 18 (9) | 204 | ||
| More than SAR 10,000 | 110 (33) | 181 (55) | 37 (11) | 328 | ||
| Chronic diseases status | Yes | 35 (29) | 69 (57) | 18 (15) | 122 | 0.255 |
| No | 200 (36) | 291 (52) | 64 (11) | 555 | ||
| Use of prescription drugs | Yes | 31 (26) | 68 (58) | 19 (16) | 118 | 0.069 |
| No | 204 (36) | 292 (52) | 63 (11) | 559 | ||
| Commitment to MOH instructions for COVID-19 | Fully commitment | 133 (33) | 218 (54) | 54 (13) | 405 | 0.658 |
| Committed to some extent | 97 (38) | 135 (52) | 27 (10) | 259 | ||
| Not committed at all | 5 (39) | 7 (54) | 1 (8) | 13 | ||
| Variables | Options | NP Use Status for COVID-19 [n (%)] | Total (677) | p Value * | ||
|---|---|---|---|---|---|---|
| Yes | No | Not Applicable | ||||
| Age | 18–25 | 66 (37) | 57 (32) | 56 (31) | 179 | 0.033 |
| 26–40 | 152 (45) | 73 (22) | 111 (33) | 336 | ||
| More than 40 years | 82 (51) | 33 (20) | 47 (29) | 162 | ||
| Gender | Female | 223 (46) | 113 (23) | 150 (31) | 486 | 0.417 |
| Male | 77 (40) | 50 (26) | 64 (34) | 191 | ||
| Nationality | Saudi | 217 (43) | 126 (25) | 162 (32) | 505 | 0.454 |
| Non-Saudi | 83 (48) | 37 (22) | 52 (30) | 172 | ||
| Geographical location | Central region | 163 (44) | 89 (24) | 119 (32) | 371 | 0.083 |
| Eastern region | 19 (37) | 13 (25) | 20 (39) | 52 | ||
| Northern region | 23 (40) | 23 (40) | 12 (21) | 58 | ||
| Southern region | 18 (45) | 6 (15) | 16 (40) | 40 | ||
| Western region | 77 (49) | 32 (21) | 47 (30) | 156 | ||
| Educational level | Intermediate school | 14 (50) | 4(14) | 10(36) | 28 | 0.136 |
| High school diploma | 63(38) | 47 (28) | 57 (34) | 167 | ||
| Undergraduate | 201 (48) | 95 (23) | 122 (29) | 418 | ||
| Postgraduate degree | 22(34) | 17 (27) | 25 (39) | 64 | ||
| Employment status | Employed | 160 (44) | 84 (23) | 121 (33) | 365 | 0.021 |
| Not employed | 110 (50) | 46 (21) | 64 (29) | 220 | ||
| Student | 30 (33) | 33 (36) | 29 (32) | 92 | ||
| Marital status | Married | 186 (49) | 79 (21) | 118 (31) | 383 | 0.002 |
| Single | 94 (36) | 78 (30) | 91 (35) | 263 | ||
| Separated | 20 (65) | 6 (19) | 5 (16) | 31 | ||
| Family income | Less than SAR 5000 | 64 (44) | 30 (21) | 51 (35) | 145 | 0.608 |
| SAR 5000–10,000 | 96 (47) | 50 (25) | 58 (28) | 204 | ||
| More than SAR 10,000 | 140 (43) | 83 (25) | 105 (32) | 328 | ||
| Chronic diseases status | Yes | 51 (42) | 32 (26) | 39 (32) | 122 | 0.777 |
| No | 249 (45) | 131 (24) | 175 (32) | 555 | ||
| Use of prescription drugs | Yes | 48 (41) | 29 (25) | 41 (35) | 118 | 0.642 |
| No | 252 (45) | 134 (24) | 173 (31) | 559 | ||
| Commitment to MOH instructions for COVID-19 | Fully commitment | 181 (45) | 89(22) | 135(33) | 405 | 0.558 |
| Committed to some extent | 114 (44) | 70(27) | 75 (29) | 259 | ||
| Not committed at all | 5 (38) | 4(31) | 4 (31) | 13 | ||
| Variables | NP Use Status for COVID-19 [n (%)] | p Value * | |||
|---|---|---|---|---|---|
| Yes | No | Not Applicable | Total (677) | ||
| Vaccination status | 0.307 | ||||
| Yes | 290 (44) | 161 (24) | 210 (32) | 661 | |
| No | 10 (62) | 2 (12) | 4 (25) | 16 | |
| Severity of COVID-19 | 0.001 | ||||
| Mild | 144 (70) | 51 (25) | 10 (50) | 205 | |
| Moderate | 92 (72) | 31 (24) | 4 (3) | 127 | |
| Severe | 6 (60) | 3 (30) | 1 (10) | 10 | |
| Hospitalization/home | 0.001 | ||||
| Hospital | 8 (57) | 5 (36) | 1 (7) | 14 | |
| Home | 238 (71) | 84 (25) | 14 (4) | 336 | |
| NP use before COVID-19 | 0.001 | ||||
| Always | 140 (60) | 33 (14) | 60 (26) | 233 | |
| Never | 11 (14) | 36 (46) | 31 (40) | 78 | |
| Sometimes | 149 (43) | 93 (27) | 107 (31) | 349 | |
| Combination of NP with other drugs | 0.001 | ||||
| Yes | 243 (52) | 89 (19) | 138 (29) | 470 | |
| No | 57 (27) | 74 (36) | 76 (37) | 207 | |
| Use of NP for immunity | 0.001 | ||||
| Yes | 259 (50) | 94 (18) | 161 (31) | 514 | |
| No | 41 (25) | 69 (42) | 35 (32) | 163 | |
| Variables | NP Use Status for COVID-19 [n (%)] | Total (677) | p Value * | ||
|---|---|---|---|---|---|
| Yes | No | Not Applicable | |||
| Priority for NP use | |||||
| Always | 115 (60) | 21 (11) | 56 (29) | 192 | 0.001 |
| Never | 28 (24) | 51 (44) | 37 (32) | 116 | |
| Sometimes | 157 (43) | 91 (25) | 121 (33) | 369 | |
| NP use by family for COVID-19 | 0.001 | ||||
| Yes | 284 (64) | 58 (13) | 99 (22) | 441 | |
| No | 16 (7) | 105 (45) | 115 (49) | 236 | |
| Status of relief from symptoms | 0.001 | ||||
| Yes | 272 (65) | 68 (16) | 78 (19) | 418 | |
| No | 14 (32) | 29 (66) | 1 (2) | 44 | |
| Side effects | 0.001 | ||||
| Yes | 8 (53) | 3 (20) | 4 (27) | 15 | |
| No | 280 (62) | 101 (22) | 72 (16) | 453 | |
| Coefficients a | ||||||||||
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95% Confidence Interval for B | Collinearity Statistics | ||||
| B | Std. Error | Beta | Lower Bound | Upper Bound | Tolerance | VIF | ||||
| 5 | (Constant) | 0.267 | 0.037 | 7.294 | 0.001 | 0.195 | 0.339 | |||
| NP use before COVID | 0.497 | 0.014 | 0.790 | 36.399 | 0.001 | 0.470 | 0.524 | 0.787 | 1.271 | |
| Priority for NP use always | 0.098 | 0.019 | 0.106 | 5.243 | 0.001 | 0.061 | 0.135 | 0.898 | 1.113 | |
| Combination of NPs with other drugs COVID-19 | 0.041 | 0.015 | 0.054 | 2.706 | 0.007 | 0.011 | 0.071 | 0.922 | 1.084 | |
| NP use by family | 0.059 | 0.021 | 0.059 | 2.741 | 0.006 | 0.017 | 0.100 | 0.799 | 1.251 | |
| Regions of Saudi Arabia | 0.032 | 0.013 | 0.046 | 2.393 | 0.017 | 0.006 | 0.059 | 0.996 | 1.004 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almuqbil, M.; Alshaikh, S.; Alrumayh, N.; Alnahdi, F.; Fallatah, E.; Almutairi, S.; Imran, M.; Kamal, M.; Almehmadi, M.; Alsaiari, A.A.; et al. Role of Natural Products in the Management of COVID-19: A Saudi Arabian Perspective. Healthcare 2023, 11, 1584. https://doi.org/10.3390/healthcare11111584
Almuqbil M, Alshaikh S, Alrumayh N, Alnahdi F, Fallatah E, Almutairi S, Imran M, Kamal M, Almehmadi M, Alsaiari AA, et al. Role of Natural Products in the Management of COVID-19: A Saudi Arabian Perspective. Healthcare. 2023; 11(11):1584. https://doi.org/10.3390/healthcare11111584
Chicago/Turabian StyleAlmuqbil, Mansour, Sarah Alshaikh, Nura Alrumayh, Fay Alnahdi, Eiman Fallatah, Shahad Almutairi, Mohd Imran, Mehnaz Kamal, Mazen Almehmadi, Ahad Amer Alsaiari, and et al. 2023. "Role of Natural Products in the Management of COVID-19: A Saudi Arabian Perspective" Healthcare 11, no. 11: 1584. https://doi.org/10.3390/healthcare11111584
APA StyleAlmuqbil, M., Alshaikh, S., Alrumayh, N., Alnahdi, F., Fallatah, E., Almutairi, S., Imran, M., Kamal, M., Almehmadi, M., Alsaiari, A. A., Alqarni, W. A. A., Alasmari, A. M., Alwarthan, S., Rabaan, A. A., Almadani, M. E., & Asdaq, S. M. B. (2023). Role of Natural Products in the Management of COVID-19: A Saudi Arabian Perspective. Healthcare, 11(11), 1584. https://doi.org/10.3390/healthcare11111584