
Impact of Stress on Periodontal Health: Literature Revision

 ,
,  ,
,  , , ,
, , ,  ,
,  and
and 
Abstract
1. Introduction
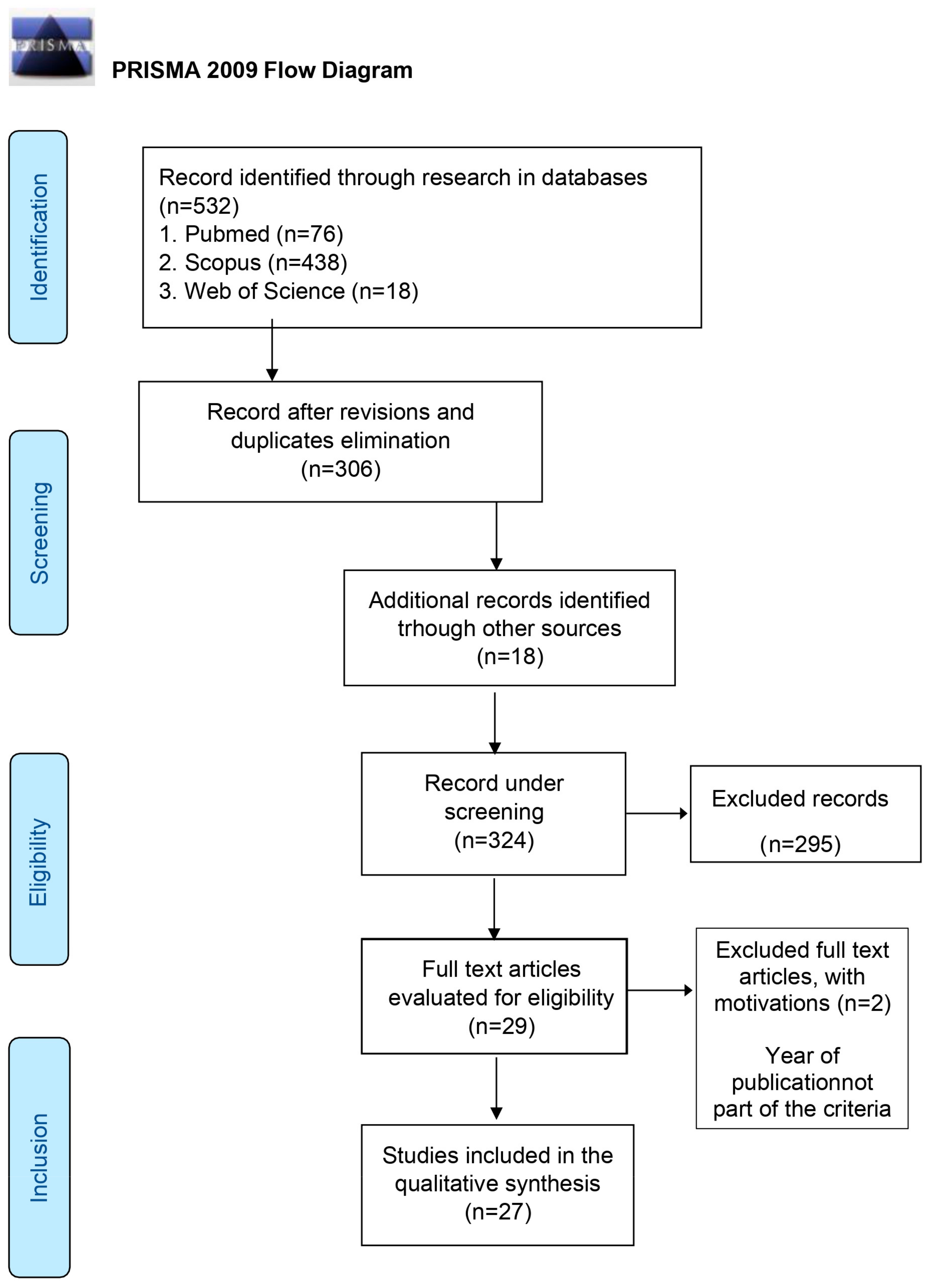
2. Materials and Methods
- -
- Population (P): human subjects with periodontal disease;
- -
- Exposure (E): psychological stress assessed by specialized questionnaires or biological biomarkers;
- -
- Comparison (C): periodontally healthy subjects not exposed to psychological stress;
- -
- Outcome/Results (O): association between psychological stress and the presence of periodontal disease.
3. Results

| Author, Year, Nation | Type of Study | Total Dimension of Sample (n of Case/Control) | Gender, -Age Range, Mean Age | Inclusion/Exclusion Criteria (C/EC) | Diagnosis of Periodontal Disease | Stress Measurement Tools | Conclusions |
|---|---|---|---|---|---|---|---|
| Wellappulli et al., 2019 Sri Lanka [38] | Case–control | 694 CP, 706 healthy | 680 F 720 M 30–60 | IC: 30–60 y.o. adults. Sri Lanka EC: n of teeth < 20; pregnant women; disability. | PD, CAL | GHQ-30 | Psychological distress is an independent risk factor for chronic periodontitis (CP) in the Sri Lankan population. |
| Varshini and Rajasekar 2020 India [16] | Clinical Observational | 100 dentistry students | NR NR | NR | Presence or absence of PD > 3 mm and loss of CAL | DAS | Dental students with severe levels of depression, anxiety and stress presented greater pocket depth and CAL. |
| Sudhakar et al., 2017 India [18] | Cohort study | 30 G1: 15 CP G2: 15 CP stress induced | Both sexes, 30–45 | EC: systemic diseases; antibiotic assumption, antioxidants; smokers. | BOP, PI, CAL, xray exam, ROM seric level measurement | Salivary and serological cortisol | The role of stress in the progression of periodontal disease was associated with increasing cortisol and ROM levels. |
| Islam et al., 2019 Japan [25] | Transversal | 738 Japanese workers | 92 F 646 M 19–65 40.7 ± 10.5 | EC: incomplete questionnaire. | Objective method: redness and/or swelling of the gingiva, with gingival recession and/or tooth mobility | Job stress and coping style questionnaire: Co-Labo57+ | Low coping style in relation to high job stress was significantly associated with periodontitis. |
| Develioglu et al., 2020 Turkey [27] | Transversal | 80 G1: 26 mild chronic periodontitis; G2: 39 moderate chronic periodontitis; G3: 15 severe chronic periodontitis | 37 F 43 M Group 1. 38.23 ± 3.55 (35–49) Group 2: 42.66 ± 7.65 (35–62) Group 3: 55.26 ± 6.94, (41–68) | IC: no dentures; not lactating. EC: diabetes; heart disease; allergies; smokers and alcohol users; periodontal treatment in the previous 6 months; anti-inflammatory or antioxidant drugs; antibiotics | PI, GI, CAL, PD, radiographic exam | STAI 1 and 2; pancreatic chromogranin A/statin, amylase alpha 1, beta-endorphin and salivary cortisol | Chronic periodontitis increased as salivary cortisol levels increased, and there was no correlation with the levels of other stress markers in saliva. |
| Obulareddy et al., 2018 India [19] | Transversal | 92 | 51 F 41 M NR | IC: age ≥ 30; muber of dental elements > 20; absence of systemic diseases, drug absumption and history of periodontal tratment over the last 6 months. EC: pregnant and nursing women | PD, CAL, BOP, PI | DASS-21, Salivar cortisol | Cortisol was associated with both chronic periodontitis (CP) and psychological stress. Cortisol levels were higher in subjects with CP associated with stress, compared with subjects with the presence of CP or stress alone. |
| Haririan et al., 2017 Austria [36] | Case-control | 56; 21 AgP,35 CP 44 healthy | 20 F 36 M 44; 21–64 | Control group IC: Healthy individuals; no PD ≥ 4 mm; no radiographic bone loss. | PD, CAL. | PSQ; Weariness scale; Warning Signals; SVF78; serum and salivary cortisol; serum levels of BDNF, SP, CGRP, VIP, NPY, ADM. | NPY and salivary VIP could be related to periodontal disease, regardless of stress levels or coping strategies. Salivary and serum cortisol levels did not differ between health and disease states. |
| Coelho et al., 2020 Brazil [37] | Transversal | 621 | 300 F 321 M 59.42 ± 10.91 (± SD) | IC: n of teeth > 4; not pregnant; no cancer or HIV-AIDS; no anti-inflammatory drugs; no periodontal treatment in the 6 months prior to study. EC: history of stroke; percutaneous coronary revascularization in the previous 6 months or surgical revascularization in the 2 months prior to the study. | PD, REC, CAL, BOP, PI e number of teeth | PSS | Positive association between stress exposure and presence of periodontitis. |
| Maruyama et al., 2022 Japan [26] | Cohort study-prospective | 40 | NR NR | IC: age ≥ 20 years. EC: systemic disease; periodontal treatment within 3 months; smokers; antibacterial, anti-inflammatory, or antiallergic medications within the past 2 weeks. | Oral status examinations-nato at T0 and follow-up. PD, BOP, PISA, PCR | Questionnaires completed at T0 and follow-up by self-reported questionnaires: PHQ-9, BDI and MIMOSYS to assess mental health status. | The change in psychological stress over 14 days was significantly correlated with changes in PD and the degree of periodontal inflammation. |
| Dubar et al., 2020 France [29] | Case-control | 60; 30 patients with periodontitis 30 patients without periodontitis | 34 F 26 M. Cases (38–65, mean age 55.0) Control (22–70, mean age 55.0) 34 F 26 M. Cases (38–65, mean age 55.0) Control (22–70, mean age 55.0) | IC: Case group: patients aged ≥ 18; moderate to severe chronic periodontitis; with at least two periodontal pockets (PD ≥ 5 mm) and one healthy site (PD ≤ 3 mm); without pathology; no history of taking antimicrobials, anti-inflammatory drugs; not pregnant; no periodontal treatment in the previous 6 months. -Control group: absence of periodontal disease; in good health; not pregnant. | Collection of parameters before and after nonsurgical periodontal treatment: PD, CAL, BOP, PI, GI, tooth mobility, radiographic examination, microbiological sample collection through crevicular fluid (GCF) | STAI-Y, PSS, salivary cortisol | Stress and anxiety in periodontal patients, appear to be associated with different bacterial colonization after SRP of Socransky orange or red complexes between stressed/anxious and non-stressed/anxious patients. Salivary cortisol concentrations would appear to be related to pocket depth, but not to self-reported stress/anxiety scores. |
| Deng et al., 2021 China [32] | Transversal | 460 | NR 45–46 | IC: age ≥ 18 years with a diagnosis of periodontitis. EC: inability to understand and independently complete questionnaires; aggressive systemic diseases. | CAL, PD | HADS, PSS-10 | The present study showed an increased prevalence of anxiety, depression, manifestations of distress and moderate to high stress among patients with periodontitis. |
| Bawankar et al., 2018 India [20] | Observational | 75 G1: 25 pcs periodontally healthy G2: 25 pcs non-smokers with moderate to severe untreated CP G3: 25 pcs smokers with moderate to severe untreated CP | 35 F 40 M 30–65 | IC: G1: periodontally healthy pcs with no history of smoking. G2: pcs without smoking history with severe untreated CP, PPD ≥ 5 mm and CAL ≥ 5 mm (30% affected teeth), radiographic alveolar bone loss. G3: pcs with smoking history (at least 10 cigarettes per day over the last 3 years). And Severe untreated CP, PPD ≥ 5 mm and CAL ≥ 5 mm (30% of teeth affected), radiographic alveolar bone loss. | PD, CAL, PI, GI, PBI | Serum and salivary cortisol, IL-1 | Strong correlation between emotional stress, smoking and CP. Smoking patients with CP show higher salivary cortisol, serum, IL-1, and stress levels than nonsmokers with CP, thus showing increased risk and severity of periodontal disease. |
| Tanveer et al., 2021 Saudi Arabia [39] | Transversal | 385 | F 15–30, M 31–45 | IC: age range 15–45 years. EC: absence of consent; pregnant, with history of diabetes mellitus; dementia and hypodontia/anodontia. | CPI, PD, only the central incisors and first and second perma-nent molars were recorded. | PPS | Significant association between psychosocial stress and periodontitis among socially disadvantaged women residing in group homes. |
| Folayan et al., 2021 Nigeria [40] | Transversal | 1.087 | 478 F 609 M 10–19 | EC: mental problems and critically ill. | GI | PHQ-9 | Mild depression was associated with higher probabilities of moderate/severe gingivitis in the study population and was a modifying factor for the association with plaque accumulation and refined carbohydrate consumption. |
| Naghsh et al., 2019 Iran [35] | Analytical-Transversal | 90: 45 CP, 45 N-CP | CP: 9 F, 36 M N-CP: 40 F, 5 M 20–55 CP: 37.1 ± 9.8 y.o. (range: 23–55 y.) N-CP: 34.8 ± 10.7 y.o. (range: 20–55 y) | IC: at least 5 natural teeth. EC: systemic diseases; or chronic immunosuppressant drugs, antidepressants, diuretics or psychoactive drugs, antihistamines, tricyclic antidepressants; smokers or alcohol users; pregnant or lactating; stressed patients undergoing treatment; orthodontic therapy; symptoms of acute disease or pulpal pain at the time of the study; history of periodontal treatment and antibiotic intake in the past 6 months. | PD, PI, BOP | STAI, salivary cortisol | Increased salivary cortisol levels in patients with CP. Therefore, the likelihood of occurrence of periodontitis is higher in subjects with increased cortisol levels. |
| Fenol et al., 2017 India [21] | Transversal | 70 G1: PD > 4 mm e < 6 mm G2: PD ≥ 6 mm G3: PD ≤ 3 mm | M 25–60 38.56 ± 10.878 | IC: n.teeth > 20. EC: corticosteroids or immunosuppressive drugs; Addison’s disease or Cushing’s syndrome; smokers; systemic diseases; history of psychiatric disorder; female sex; history of periodontal therapy in the past 6 months. | PD, CAL, OHI-S, GI. | Salivary cortisol levels, DASS | There is a positive relationship between stress and periodontal disease. |
| Karimi et al., 2017 Iran [34] | Case-control | 30 G1: 15 with periodontitis G2: 15 without periodontitis | 15 F 15 M 42–44 | IC: G1: no periodontal disease; G2: CAL ≥3 mm and BOP in upper teeth. | PD, CAL, PI, GI, BOP | DASS-42, IgA salivary | A total of 87% of subjects with periodontal disease were depressed compared with 60% without periodontal disease and depression. |
| Zhang et al., 2021 China [33] | Randomized, double-blind, prospective | 600 G1: 200 individuals with CP, history of smohaing and depression; G2: 200 with CP, no history of smoking and depression; G3: 200 individuals parodontalmente sani | 300 F 300 M 20–50 | EC: systemic diseases; drug intake; benign pituitary tumors including adenomas; cancerous pituitary tumors; benign and malignant adrenal gland tumors; Cushing syndrome, corticosteroids to treat asthma, arthritis, and some cancers; pregnant women. | GI, PI, PD, CAL, BOP, dental mobility, radiographic evidence | SCL-90, salivary cortisol | Strong relationship between depression, smoking history and CP. Smokers with CP show significantly higher cortisol levels in saliva than in serum. Subjects with elevated cortisol levels are at increased risk for periodontitis. |
| Wijayaa et al., 2020 Indonesia [41] | Transversal | 57 students | NR NR | IC: non-smokers for more than 6 months; no history of pregnancy, chronic diseases of the immune system, no use of antibiotics in the last 4 weeks; no use of immunomodulatory drugs, anti-inflammatory drugs, sodium antagonists and anticonvulsants; and no odotoiatric/orthodontic treatment. | Measurement of salivary and plaque flow rate (O’Leary) | SAAS | Academic stress in-fluences salivary flow rate but not directly on plaque score. A decrease in the salivary flow rate causes an increase in plaque score. |
| Petit et al., 2021 France [30] | Prospective | 54 | 56%F 51,2 y.o | IC: age > 18 years; diagnosis of severe chronic periodontitis; CAL > 4 mm; n. of teeth > 15 with at least 5% of sites with PPD > 5 mm and radiographic bone loss. EC: systemic diseases; history of taking anti-inflammatory, psychotropic and antibiotic drugs in the past 6 months; pregnancy; orthodontic therapy; history of periodontal treatment in the past 6 months. | PD, CAL, PI, and BOP recorded at T0 before SRP, at T3 and T6 | STAI, BDI | Depression and anxiety have been shown to be a risk factor of worsening SRP outcomes. |
| Petit et al., 2021 France [31] | Prospective | 71 at T0 58 at T3 54 at T6 | T0: 40 F, 31 M T3: 32 F, 26 M T6: 30 F, 24 M 29–74 mean age 51.3 | IC: age > 18 years; n. of teeth > 15; diagnosis of severe chronic parodontitis; with at least 5% of sites with PD > 5 mm and radiographic bone loss. EC: systemic diseases; history of taking anti-inflammatory drugs, psychotropic drugs, and antibiotics in the past 6 months; pregnancy; orthodontic therapy; history of periodontal treatment in the past 6 months. | PI, BOP, PD, CAL (collected at T0, before SRP and at 3 months) Complete periodontal examination performed at 6 months | DASS-42, TCS, At T0 and T6 from the SRP, plasma levels of cortisol and chromogranin-A were collected | Patients with increased stress, anxiety and depression scores, who use negative coping strategies, show worse SRP scores. |
| Khalil et al., 2020 United Arab Emirates [1] | Comparative-observational | 150 | 56 F 94 M 20–40 | IC: male and female patients attending the dental clinics of Ajman University; age between 20 and 65; any nationality. EC: people not attending Ajman University dental clinics; age below 20 or above 65. | NR | Questionnaire adapted from Barreca and Hepler (2000) | Stress-related oral manifestations. Among the different manifestations, chronic periodontal disease had an incidence of 24%, with a greater impact in older and male patients. |
| Gomaa et al., 2020 Canada [42] | Transversal | 102 | 52% di F 20–59 | EC: chronic, autoimmune or inflammatory diseases; history of taking corticosteroid, antibiotic, probiotic or prescription drugs; hair treatments/coloring; hair length < 3 cm; dental procedures and periodontal treatment within the past 3 months. | OPMN, OIL, PD, BOP, CAL | PSS, FSS, hair cortisol concentration, salivary alpha-Amylase | Psychosocial stress may contribute to pro-inflammatory immunity, implicated in the pathobiology of periodontal disease. |
| Rahate et al., 2021 India [22] | Transversal | 90 G1: periodontally healthy pcs G2: pcs diagnosed with stage III periodontitis and non-smokers G3: pcs diagnosed with stage III periodontitis and smokers | 34 F 56 M G1: 18 F, 12 M G2: 14 F, 16 M G3: 5 F, 25 M 30–65 G1: 49.03 G2: 51.93 G3: 52.23 | IC: G1: healthy, non-fumatorial pcs. G2: non-fumatorial pcs; diagnosis of periodontitis, stage III with PD ≥ 6 mm and CAL ≥ 5 mm; radiographic loss of alveolar bone. G3: pcs with smoking history (n ≥10 cigarettes per day); diagnosis of periodontitis, stage III with PD ≥ 6 mm and CAL ≥ 5 mm; ra-diographic loss of alveolar bone. EC: reported psychiatric disorders or psychotic medications; systemic diseases; pregnant, lactating, and menopausal; history of taking antibiotics or hormone therapy; acute diseases; immunosuppressive therapy; history of periodontal treatment over the past 6 months | PD, CAL, PI, GI, PBI | Serum and salivary levels of ghrelin and cortisol | Positive association between stress, smoking and stage III periodontitis. In patients with stage III periodontitis, stress and smoking habit increase the severity of destruction of the periodontal tissues. Serum and salivary ghrelin levels were lowest, while serum and salivary cortisol levels were higher in group 3, revealing an inverse relationship between the two parameters. |
| Yarkac et al., 2018 Turkey [28] | Randomized–controlled trial | 60: 30 pregnant women (Pr) 30 non-pregnant women (N-Pr) | F 20–45 N-Pr (27.93 ± 6.61) Pr (28.93 ± 4.04) | IC: presence of gingivitis; PD ≤ 3 mm in all four quadrants; with at least 20 teeth. EC: history of anti-inflammatory, antimicrobial, and hormone therapy in the previous 6 months; systemic diseases; mental disorders; female smokers; breastfeeding; pregnant or menstruating | Clinical and radiographic criteria (clinical criteria for PR only) recorded at baseline time T0 and 3 weeks after nonsurgical periodontal treatment. PD, PI, GI; collection of gingival crevicular fluid (GCF) for evaluation of IL-10 e IL-6. | PSS-10; salivary cortisol (at T0 and T3) | Pregnant women with stress had higher salivary cortisol levels after nonsurgical periodontal treatment than nonpregnant women. |
| Rajhans et al., 2017 India [23] | Case-control | 60-G 1: chronic periodontitis with DM; G 2: chronic periodontitis without DM; G3: systemically and periodontally healthy individuals. | NR 35–50 | EC: systemic diseases; pregnant women; history of taking drugs. | PI, GI, PD, CAL | PSS, SRRS | There seems to be a strong correlation between periodontal destruction, DM stress, and serum cortisol levels. |
| Ramesh et al., 2018 India [24] | Transversal | 27 G1: 10 generalized chronic periodontitis G2: 7 generalized aggressive periodontitis G3: 10 periodontally healthy subjects | Both sexes 19–60 | EC: periodontal treatment within the previous 3 months; smokers and alcohol users; systemic diseases and history of taking immunosuppressive drugs. | GI, PD, CAL | PHQ-9 | Clinical depression could be a risk factor in the development of periodontal disease. No significant association with chronic periodontitis. |
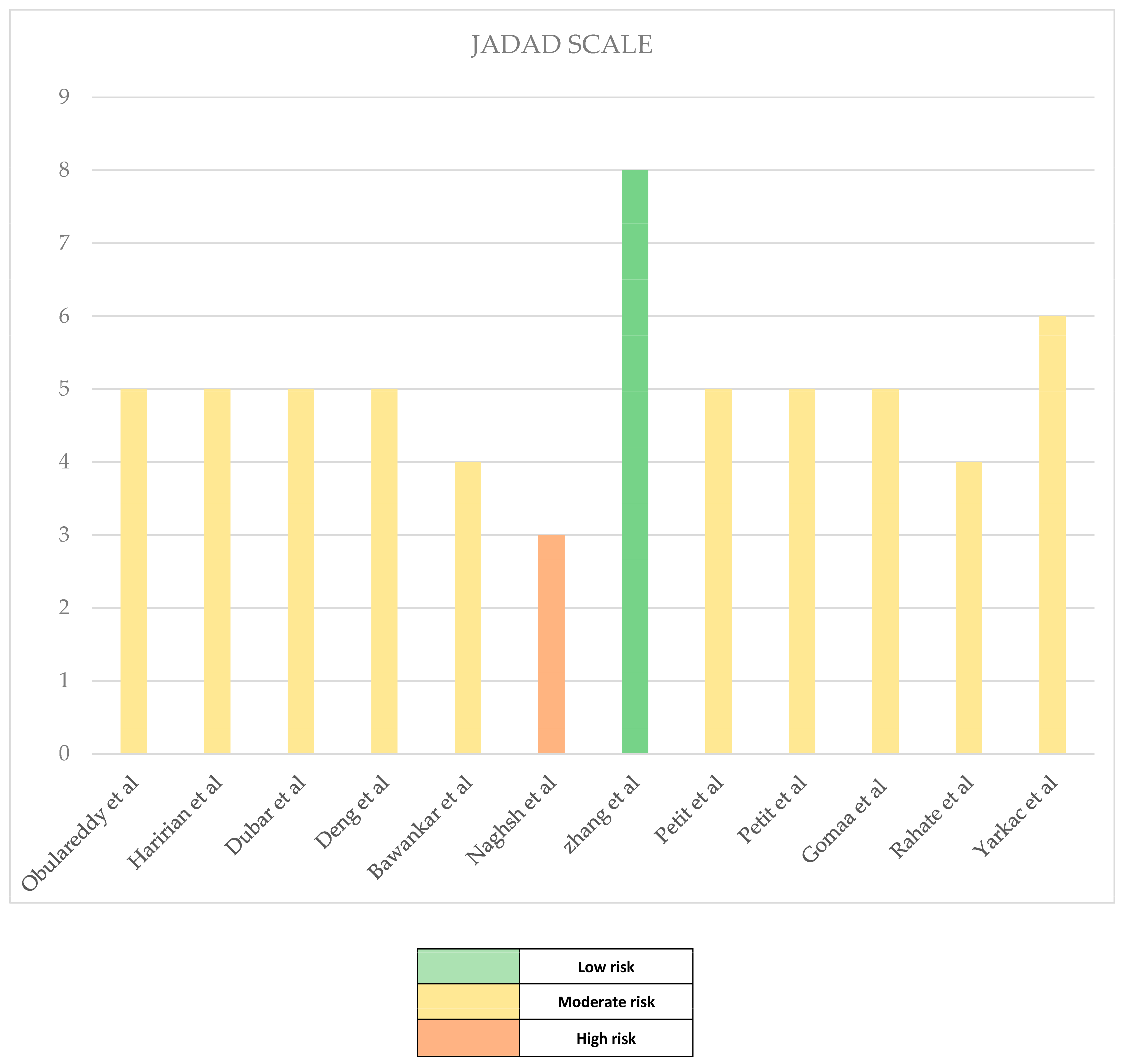
Risk of Bias in Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khalil, E.; Ibrahim, N.A.; Al Shayeb, M.; Kuduruthullah, S.; Hassan, M. Stress-Related Oral Manifestations Disorders in A Population Sample of Patients Attending Ajman University Dental Clinics. J. Int. Dent. Med. Res. 2020, 13, 577–586. [Google Scholar]
- Cortesi Ardizzone, V.; Abbinante, A. (Eds.) Igienista Orale: Teoria E Pratica Professionale; Edra: Milano, Italy, 2013. [Google Scholar]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Allen, G. Producing guidance for the management of patients with chronic periodontal disease in general dental practice. Br. Dent. J. 2015, 218, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontology 2000 2013, 62, 59–94. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Gupta, G.; Thomas, B.; Bhat, K.M.; Bhat, G.S. Stress and periodontal disease: The link and logic! Ind. Psychiatry J. 2013, 22, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Lang, N.P.; Karring, T. Clinical Periodontology and Implant Dentistry; Wiley: Hoboken, NJ, USA, 2009; ISBN 1444313045, 9781444313048. [Google Scholar]
- D’Ambrosio, F.; Caggiano, M.; Schiavo, L.; Savarese, G.; Carpinelli, L.; Amato, A.; Iandolo, A. Chronic Stress and Depression in Periodontitis and Peri-Implantitis: A Narrative Review on Neurobiological, Neurobehavioral and Immune-Microbiome Interplays and Clinical Management Implications. Dent. J. 2022, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Deinzer, R.; Granrath, N.; Spahl, M.; Linz, S.; Waschul, B.; Herforth, A. Stress, oral health behaviour and clinical outcome. Br. J. Health Psychol. 2005, 10 Pt 2, 269–283. [Google Scholar] [CrossRef]
- Ravishankar, T.L.; Ain, T.S.; Gowhar, O. Effect of academic stress on plaque and gingival health among dental students of Moradabad, India. J. Int. Acad. Periodontol. 2014, 16, 115–120. [Google Scholar]
- Hugo, F.N.; Hilgert, J.B.; Bozzetti, M.C.; Bandeira, D.R.; Gonçalves, T.R.; Pawlowski, J.; de Sousa, M.d.L.R. Chronic stress, depression and cortisol levels as risk indicators of elevated plaque and gingivitis levels in individuals aged 50 years and older. J. Periodontol. 2006, 77, 1008–1014. [Google Scholar] [CrossRef]
- Pedersen, A.M.L.; Sørensen, C.E.; Proctor, G.B.; Carpenter, G.H.; Ekström, J. Salivary secretion in health and disease. J. Oral Rehabil. Sep. 2018, 45, 730–746. [Google Scholar] [CrossRef]
- Guyton & Hall. Fisiologia Medica, 13th ed.; Aicardi, P.B.G., Ed.; Edra: Milano, Italy, 2017. [Google Scholar]
- Sherwood, L. Fondamenti di Fisiologia Umana; Piccin: Padova, Italy, 2012. [Google Scholar]
- Carpenter, G.H. The secretion, components, and properties of saliva. Annu. Rev. Food Sci. Technol. 2013, 4, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Vindhiya Varshini, V.; Arvina, R. Effect of Stress on Periodontal Health: A Clinical Study. J. Res. Med. Dent. Sci. 2020, 8, 259–263. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2014; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 17 February 2014).
- Sudhakar, U.; Thyagarajan, R.; Jeyapal, B.; Jagadeesh, S.; Jayakumar, P. Indagation of serum and salivary reactive oxygen metabolite and cortisol levels in chronic periodontitis and stress-induced chronic periodontitis patients. J. Indian Soc. Periodontol. 2017, 21, 371–375. [Google Scholar] [PubMed]
- Obulareddy, V.T.; Chava, V.K.; Nagarakanti, S. Association of Stress, Salivary Cortisol, and Chronic Periodontitis: A Clinico-biochemical Study. Contemp. Clin. Dent. 2018, 9 (Suppl. 2), S299–S304. [Google Scholar]
- Bawankar, P.V.; Kolte, A.P.; Kolte, R.A. Evaluation of stress, serum and salivary cortisol, and interleukin-1β levels in smokers and non-smokers with chronic periodontitis. J. Periodontol. 2018, 89, 1061–1068. [Google Scholar] [CrossRef]
- Fenol, A.; Jebi, S.; Krishnan, S.; Perayil, J.; Vyloppillil, R.; Bhaskar, A.; Menon, S.M.; Mohandas, A. Association of stress, salivary cortisol level, and periodontitis among the inmates of a central prison in Kerala. Dent. Res. J. 2017, 14, 288–292. [Google Scholar] [CrossRef]
- Rahate, P.S.; Kolte, R.A.; Kolte, A.P.; Lathiya, V.N.; Gupta, M.; Chari, S. Evaluation of stress, serum, and salivary ghrelin and cortisol levels in smokers and non- smokers with Stage III periodontitis: A cross-sectional study. J. Periodontol. 2022, 93, 1131–1140. [Google Scholar] [CrossRef]
- Rajhans, N.S.; Byakod, G.; Kumar, R.; Sable, D. Assessment of Psychological Stress and Serum Cortisol in Patients having Chronic Periodontitis with and witho Type II Diabetes Mellitus: A Clinicobiochemical Study. World J. Dent. 2017, 8, 378–381. [Google Scholar]
- Ramesh, A.; Malaiappan, S.; Prabhakar, J. Relationship between clinical depression and the types of periodontitis—A cross-sectional study. Drug Invent. Today 2018, 10, 659–663. [Google Scholar]
- Islam, M.M.; Ekuni, D.; Yoneda, T.; Yokoi, A.; Morita, M. Influence of Occupational Stress and Coping Style on Periodontitis among Japanese Workers: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 3540. [Google Scholar] [CrossRef]
- Maruyama, T.; Ekuni, D.; Higuchi, M.; Takayama, E.; Tokuno, S.; Morita, M. Relationship between Psychological Stress Determined by Voice Analysis and Periodontal Status: A Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 9489. [Google Scholar] [CrossRef] [PubMed]
- Develioglu, H.; Korkmaz, S.; Dundar, S.; Schlagenhauf, U. Investigation of the levels of different salivary stress markers in chronic periodontitis patients. J. Oral Biol. Craniofacial Res. 2020, 10, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Yarkac, F.U.; Gokturk, O.; Demir, O. Interaction between stress, cytokines, and salivary cortisol in pregnant and non-pregnant women with gingivitis. Clin. Oral Investig. 2021, 25, 1677–1684. [Google Scholar] [CrossRef]
- Dubar, M.; Clerc-Urmès, I.; Baumann, C.; Clément, C.; Alauzet, C.; Bisson, C. Relations of Psychosocial Factors and Cortisol with Periodontal and Bacterial Parameters: A Relations of psychosocial factors and cortisol with periodontal and bacterial parameters: A prospective clinical study in 30 patients with periodontitis before and after non-surgical treatment. Int. J. Environ. Res. Public Health 2020, 17, 7651. [Google Scholar] [PubMed]
- Petit, C.; Anadon-Rosinach, V.; Rettig, L.; Schmidt-Mutter, C.; Tuzin, N.; Davideau, J.L.; Huck, O. Influence of psychological stress on non-surgical periodontal treatment outcomes in patients with severe chronic periodontitis. J. Periodontol. 2021, 92, 186–195. [Google Scholar] [CrossRef]
- Petit, C.; Anadon-Rosinach, V.; Tuzin, N.; Davideau, J.L.; Huck, O. Influence of Depression and Anxiety on Non-Surgical Periodontal Treatment Outcomes: A 6-Month Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 9394. [Google Scholar] [CrossRef]
- Deng, Y.; He, S.; Wang, J. Validation of the Hospital Anxiety and Depression Scale and the Perceived Stress Scale and psychological features in patients with periodontitis. J. Periodontol. 2021, 92, 1601–1612. [Google Scholar] [CrossRef]
- Zhang, H.; Chen, B.; Pan, C.; Zhang, A. To evaluate the serum cortisol, salivary cortisol, and serum interleukin-1 B level in patients of chronic periodontitis with smoking and stress and without smoking and stress. Medicine 2021, 100, e26757. [Google Scholar] [CrossRef]
- Karimi, M.; Elyahoo, S.; Golchin, L.; Kermani, T. Relationship between stress, anxiety, depression and salivary IgA with periodontal disease. Biosci. Biotech. Res. Comm. 2017, 10, 88–92. [Google Scholar] [CrossRef]
- Naghsh, N.; Mogharehabed, A.; Karami, E.; Yaghini, J. Comparative evaluation of the cortisol level of unstimulated saliva in patients with and without chronic periodontitis. Dent. Res. J. 2019, 16, 421–427. [Google Scholar]
- Haririan, H.; Andrukhov, O.; Böttcher, M.; Pablik, E.; Wimmer, G.; Moritz, A.; Rausch-Fan, X. Salivary neuropeptides, stress, and periodontitis. J. Periodontol. 2018, 89, 9–18. [Google Scholar] [CrossRef]
- Coelho, J.; Miranda, S.S.; da Cruz, S.S.; Trindade, S.C.; Passos-Soares, J.S.; Cerqueira, E.; Costa, M.; Figueiredo, A.; Hintz, A.M.; Barreto, M.L.; et al. Is there association between stress and periodontitis? Clin. Oral Investig. 2020, 24, 2285–2294. [Google Scholar] [CrossRef]
- Wellappulli, N.; Ekanayake, L. Association between psychological distress and chronic periodontitis in Sri Lankan adults. Community Dent. Health 2019, 36, 293–297. [Google Scholar] [PubMed]
- Tanveer, A.S.; Afaq, A.; Alqutub, M.N.; Aldahiyan, N.; AlMubarak, A.M.; Shaikh, A.C.; Naseem, M.; Vohra, F.; Abduljabbar, T. Association of Self-Perceived Psychological Stress with the Periodontal Health of Socially Deprived Women in Shelter Homes. Int. J. Environ. Res. Public Health 2021, 18, 5160. [Google Scholar] [CrossRef] [PubMed]
- Folayan, M.O.; Tantawi, M.E.; Chukwumah, N.M.; Alade, M.; Mapayi, B.; Oginni, O.; Arowolo, O.; Sam-Agudu, N.A. Associations between depression and gingivitis among adolescents resident in semi-urban South-West Nigeria. BMC Oral Health 2021, 21, 55. [Google Scholar] [CrossRef] [PubMed]
- Wijayaa, D.; Ismalayanib; Zainurc, R.A.; Anggrainid, V.P. The Effect of Academic Stress on Salivary Flow Rate and Plaque Score in Dental Nursing Students of Palembang Health Polytechnic. Int. J. Innovation. 2020, 13, 2. [Google Scholar]
- Gomaa, N.; Glogauer, M.; Nicolau, B.; Tenenbaum, H.; Siddiqi, A.; Fine, N.; Quiñonez, C. Stressed-Out Oral Immunity: A Gateway from Socioeconomic Adversity to Periodontal Disease. Psychosom. Med. 2020, 82, 126–137. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Database | Search Format |
|---|---|
| PUMBED | (“Stress, Psychological” [Mesh]) AND “Periodontitis” [Mesh]); (“Stress, Psychological” [Mesh]) AND “Periodontal Diseases” [Mesh]. |
| SCOPUS | ALL(“Psychological stress”) AND ALL(“Periodontal Diseases”); ALL(“Psychological stress”) AND ALL(“Periodontitis”); TITLE-ABS-KEY(“Psychological stress”) AND TITLE-ABS-KEY(“Periodontal Diseases”); TITLE-ABS-KEY(“Psychological stress”) AND TITLE-ABS-KEY(“Periodontitis”). |
| WEB OF SCIENCE | TS = (“Psychological stress”) AND TS = (“Periodontal Diseases”); TS = (“Psychological stress”) AND TS = (“Periodontitis”) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corridore, D.; Saccucci, M.; Zumbo, G.; Fontana, E.; Lamazza, L.; Stamegna, C.; Di Carlo, G.; Vozza, I.; Guerra, F. Impact of Stress on Periodontal Health: Literature Revision. Healthcare 2023, 11, 1516. https://doi.org/10.3390/healthcare11101516
Corridore D, Saccucci M, Zumbo G, Fontana E, Lamazza L, Stamegna C, Di Carlo G, Vozza I, Guerra F. Impact of Stress on Periodontal Health: Literature Revision. Healthcare. 2023; 11(10):1516. https://doi.org/10.3390/healthcare11101516
Chicago/Turabian StyleCorridore, Denise, Matteo Saccucci, Giulia Zumbo, Erika Fontana, Luca Lamazza, Claudio Stamegna, Gabriele Di Carlo, Iole Vozza, and Fabrizio Guerra. 2023. "Impact of Stress on Periodontal Health: Literature Revision" Healthcare 11, no. 10: 1516. https://doi.org/10.3390/healthcare11101516
APA StyleCorridore, D., Saccucci, M., Zumbo, G., Fontana, E., Lamazza, L., Stamegna, C., Di Carlo, G., Vozza, I., & Guerra, F. (2023). Impact of Stress on Periodontal Health: Literature Revision. Healthcare, 11(10), 1516. https://doi.org/10.3390/healthcare11101516