
Analysing the Effects of Different Types of Exercise on Dyspnoea and Fatigue in Adults through COPD-Systematic Review and Meta-Analysis of Randomised Clinical Trials

 ,
,  , ,
, ,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Study Identification
2.3. Data Extraction
2.4. Quality of Study and Risk of Bias
2.5. GRADE Assessment
2.6. Data Synthesis and Analysis
3. Results
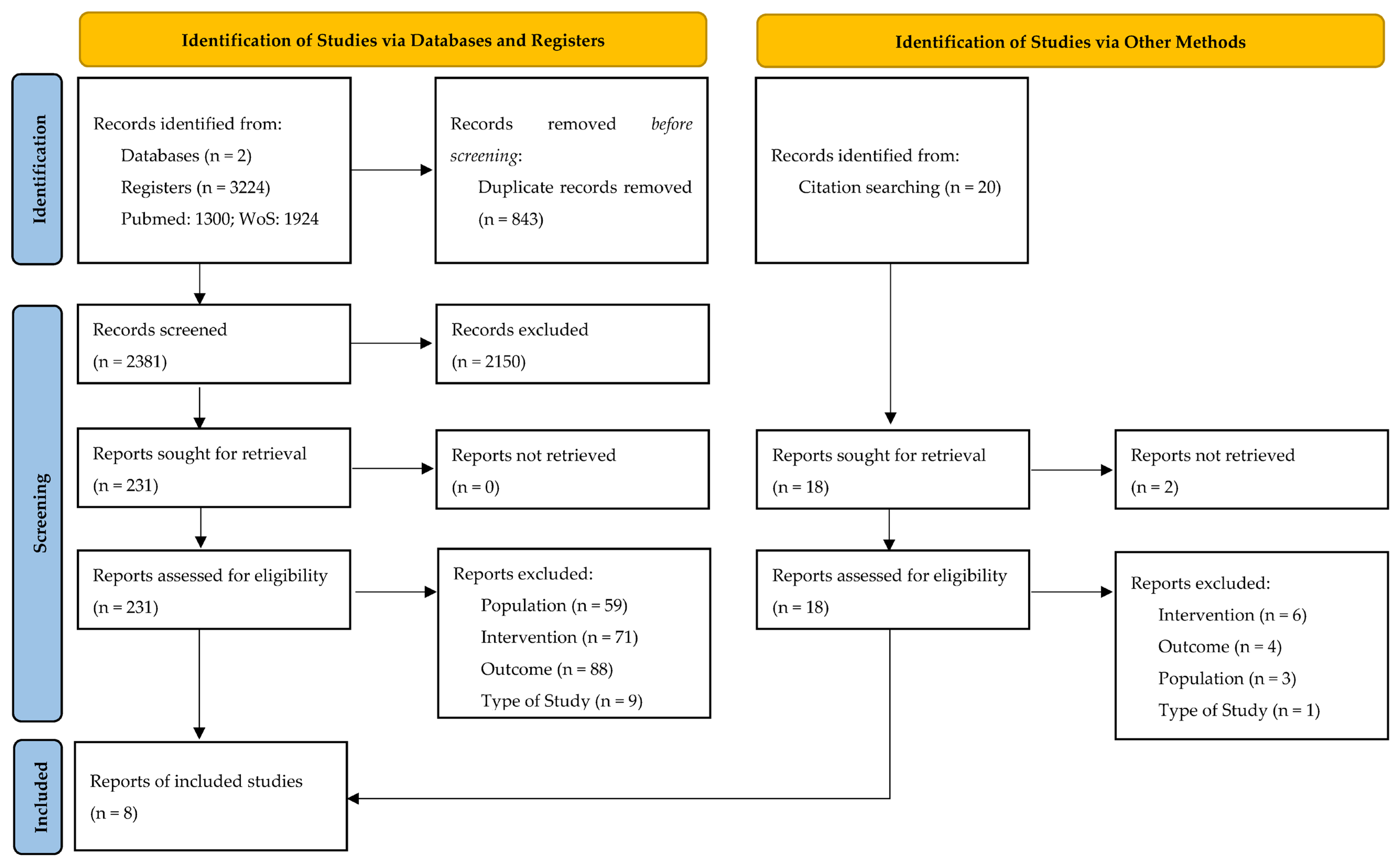
3.1. Results of the Systematic Literature Search Are Summarised in the PRISMA Flowchart (Figure 1)

3.2. Study Characteristics
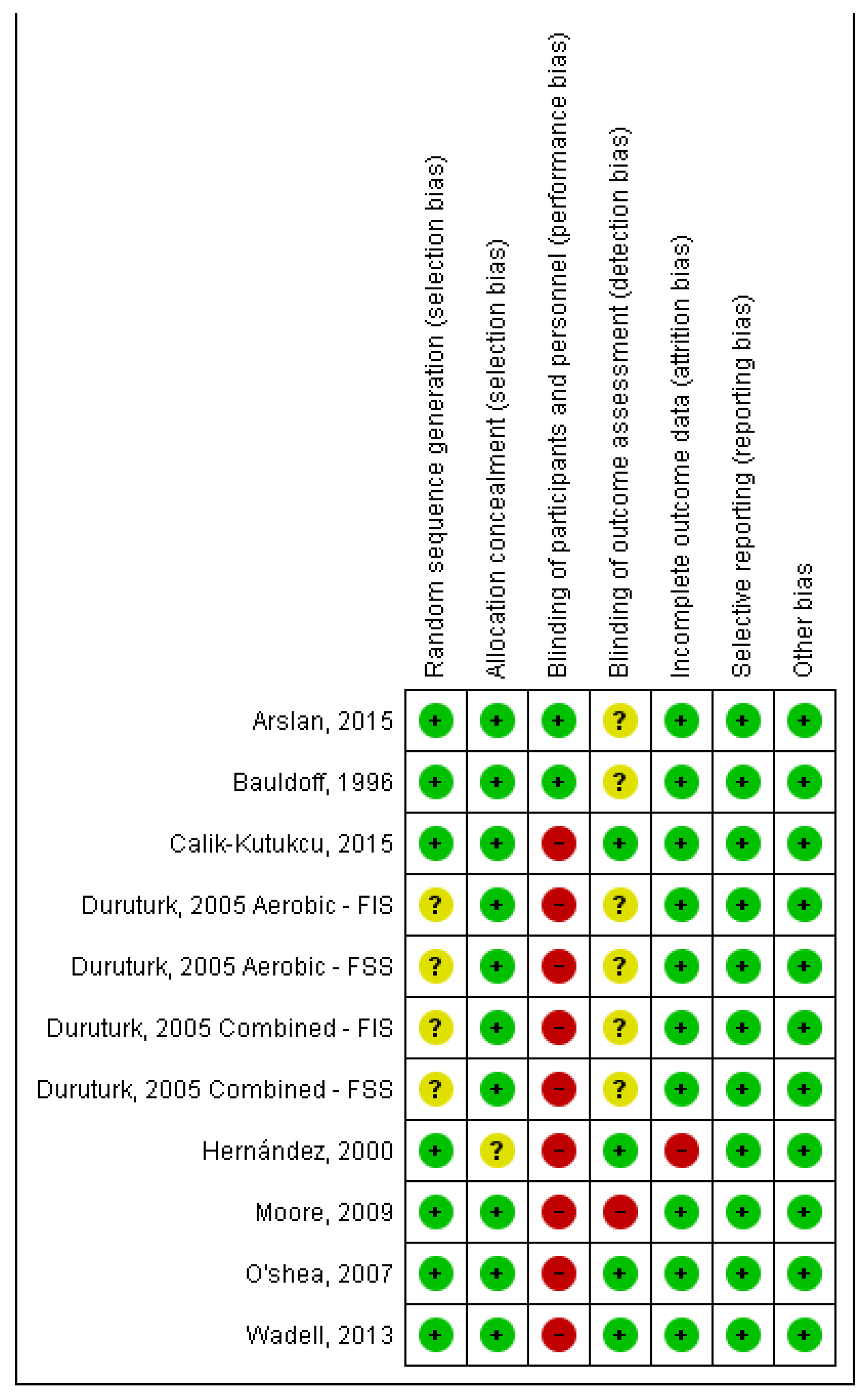
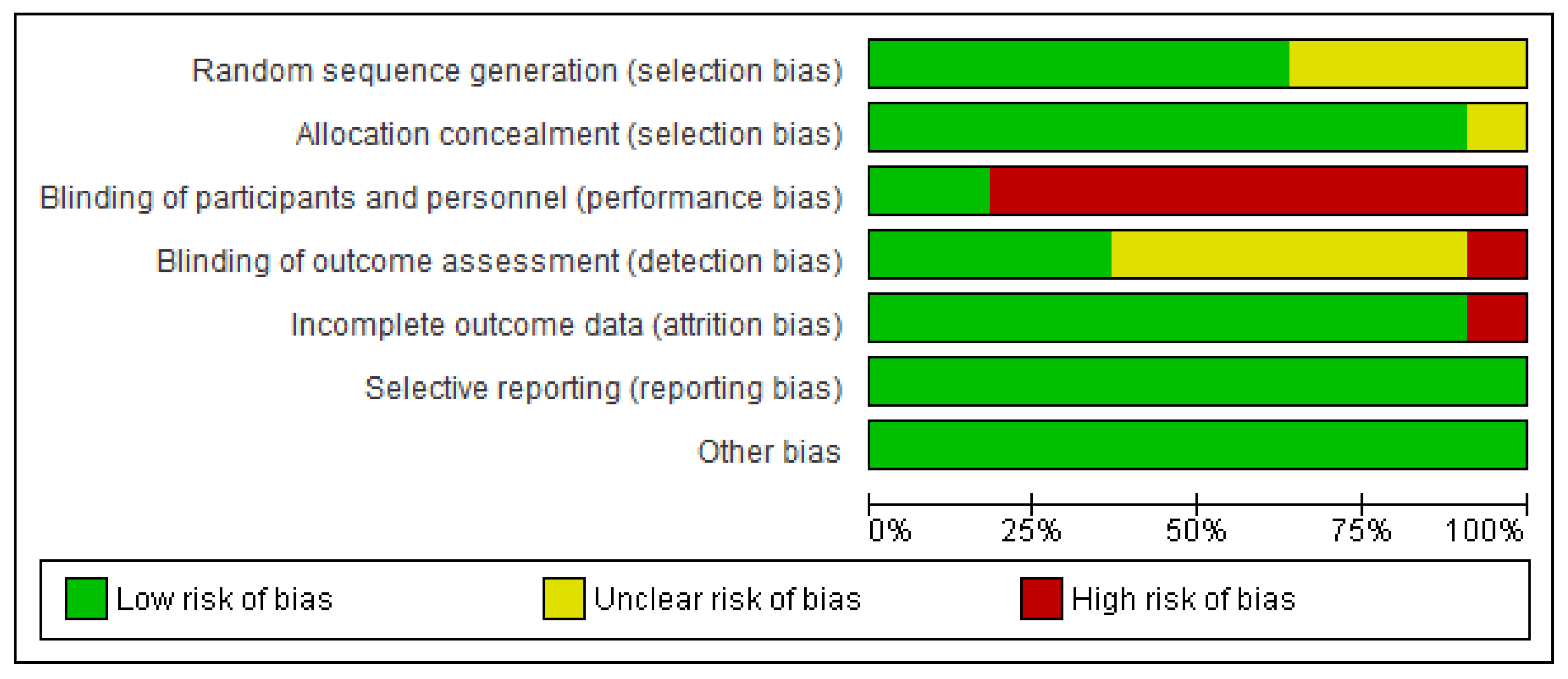
3.3. Quality of Studies and Risk of Bias (Figure 2 and Figure 3)


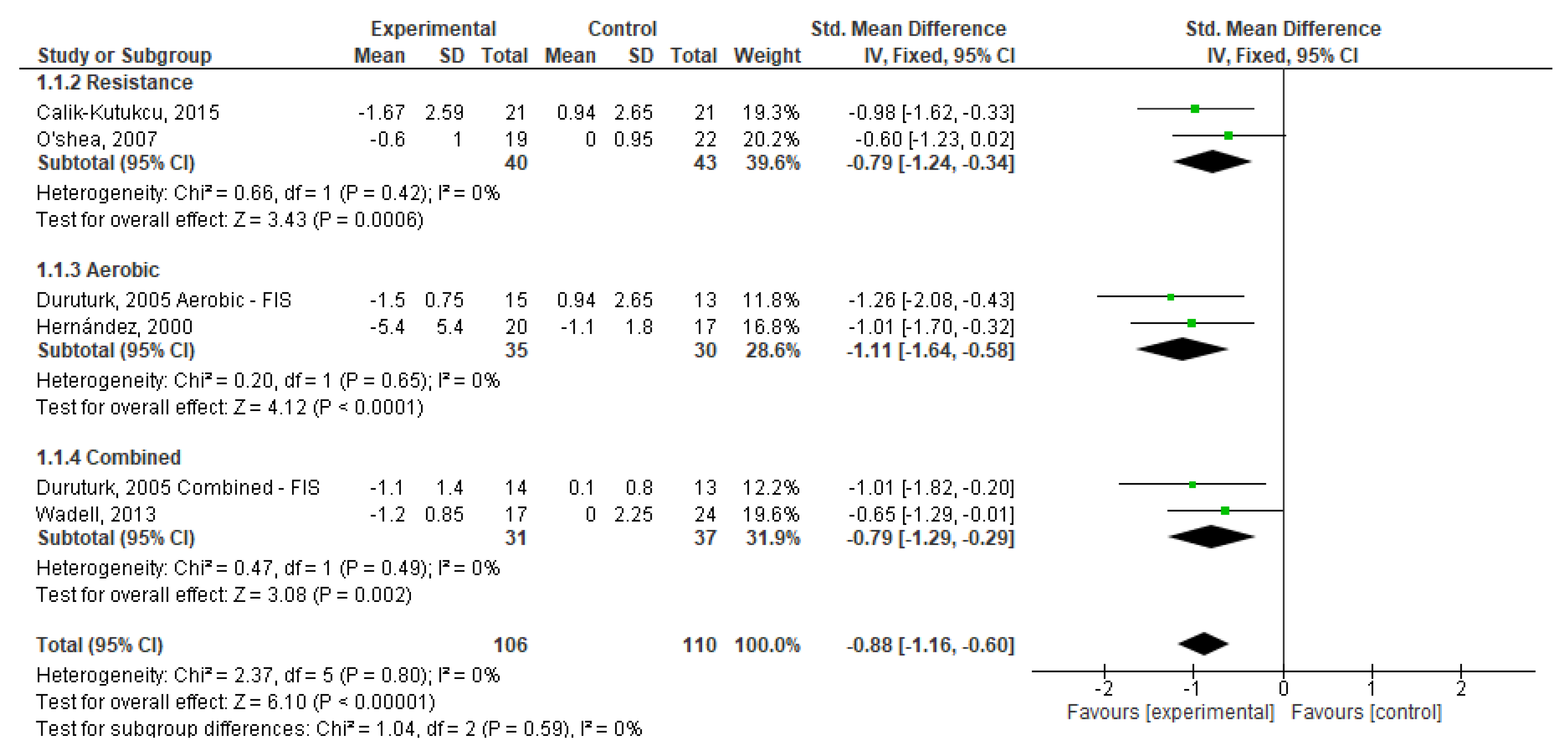
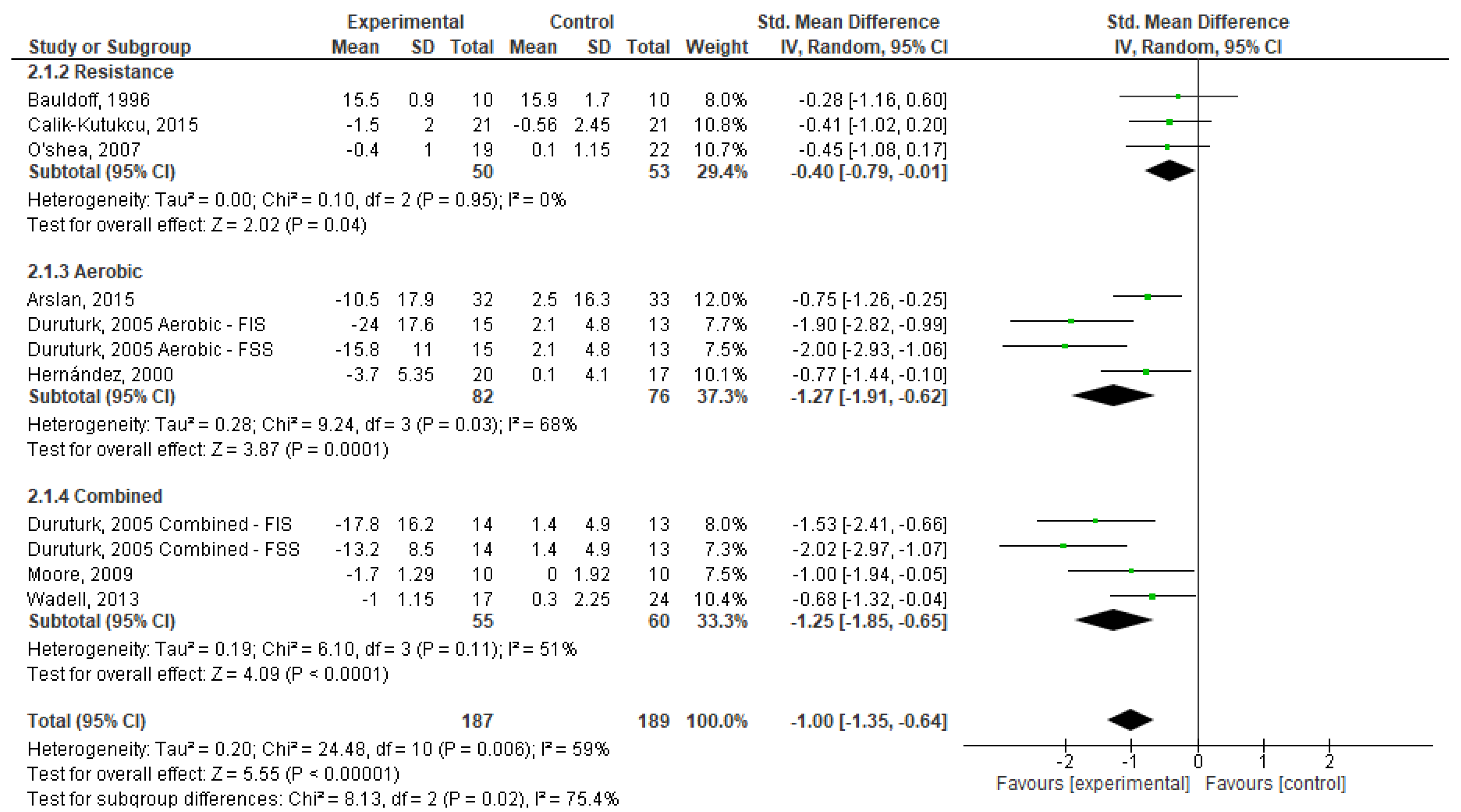
3.4. Meta-Analysis
3.5. Certainty of Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease. 2023. Available online: https://goldcopd.org/wp-content/uploads/2022/12/GOLD-2023-ver-1.1-2Dec2022_WMV.pdf (accessed on 12 February 2023).
- World Health Organization. Chronic Obstructive Pulmonary Disease (COPD); World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Goërtz, Y.M.J.; Looijmans, M.; Prins, J.B.; Janssen, D.J.A.; Thong, M.S.Y.; Peters, J.B.; Burtin, C.; Meertens-Kerris, Y.; Coors, A.; Muris, J.W.M.; et al. Fatigue in patients with chronic obstructive pulmonary disease: Protocol of the Dutch multicentre, longitudinal, observational FAntasTIGUE study. BMJ Open 2018, 8, e021745. [Google Scholar] [CrossRef] [PubMed]
- Arandelović, M.; Stanković, I.; Nikolić, M. Swimming and persons with mild persistant asthma. Sci. World J. 2007, 7, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- Burr, J.F.; Davidson, W.; Shephard, R.J.; Eves, N. Physical activity in chronic respiratory conditions: Assessing risks for physical activity clearance and prescription. Can. Fam. Physician 2012, 58, 761–764. [Google Scholar]
- Gloeckl, R.; Marinov, B.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Lake, F.R.; Henderson, K.; Briffa, T.; Openshaw, J.; Musk, A.W. Upper-limb and lower-limb exercise training in patients with chronic airflow obstruction. Chest 1990, 97, 1077–1082. [Google Scholar] [CrossRef]
- Salcedo, P.A.; Lindheimer, J.B.; Klein-Adams, J.C.; Stotolongo, A.M.; Falvo, M.J. Effects of Exercise Training on Pulmonary Function in Adults with Chronic Lung Disease: A Meta-Analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2018, 99, 2561–2569. [Google Scholar] [CrossRef]
- Bolton, C.E.; Singh, S.J.; Walker, P.P. British Thoracic Society Pulmonary Rehabilitation Guideline Group. Commentary: The British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax 2013, 68, 887–888. [Google Scholar] [CrossRef]
- Lim, W.S.; Smith, D.L.; Wise, M.P.; Welham, S.A. British Thoracic Society. British Thoracic Society community acquired pneumonia guideline and the NICE pneumonia guideline: How they fit together. Thorax 2015, 70, 698–700. [Google Scholar] [CrossRef]
- Schneider, A.; Gantner, L.; Maag, I.; Borst, M.M.; Wensing, M.; Szecsenyi, J. Are ICD-10 codes appropriate for performance assessment in asthma and COPD in general practice? Results of a cross sectional observational study. BMC Health Serv. Res. 2005, 5, 11. [Google Scholar] [CrossRef]
- Cooke, C.R.; Joo, M.J.; Anderson, S.M.; Lee, T.A.; Udris, E.M.; Johnson, E.; Au, D.H. The validity of using ICD-9 codes and pharmacy records to identify patients with chronic obstructive pulmonary disease. BMC Health Serv. Res. 2011, 11, 37. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2021; ISBN 197515018X/978-1975150181. [Google Scholar]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. ATS/ERS Task Force on Pulmonary Rehabilitation. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Paixão, C.; Rocha, V.; Brooks, D.; Marques, A. Unsupervised physical activity interventions for people with COPD: A systematic review and meta-analysis. Pulmonology 2022. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Paneroni, M.; Vitacca, M.; Venturelli, M.; Simonelli, C.; Bertacchini, L.; Scalvini, S.; Schena, F.; Ambrosino, N. The impact of exercise training on fatigue in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Pulmonology 2020, 26, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.W.M.; McKeough, Z.; Alison, J.; Dennis, S.; Hamer, M.; Stamatakis, E. Associations of total and type-specific physical activity with mortality in chronic obstructive pulmonary disease: A population-based cohort study. BMC Public Health 2018, 18, 268. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Nang, C.; Piano, B.; Lewis, A.; Lycett, K.; Woodhouse, M. Using The PICOS Model to Design and Conduct a Systematic Search: A Speech Pathology Case Study. In Proceedings of the ECU Research Week, Perth, Australia, 14–18 September 2015; p. 51. [Google Scholar]
- Arslan, S.; Öztunç, G. The Effects of a Walking Exercise Program on Fatigue in the Person with COPD. Rehabil. Nurs. 2016, 41, 303–312. [Google Scholar] [CrossRef]
- Bauldoff, G.S.; Hoffman, L.A.; Sciurba, F.; Zullo, T.G. Home-based, upper-arm exercise training for patients with chronic obstructive pulmonary disease. Heart Lung 1996, 25, 288–294. [Google Scholar] [CrossRef]
- Calik-Kutukcu, E.; Arikan, H.; Saglam, M.; Vardar-Yagli, N.; Oksuz, C.; Inal-Ince, D.; Savci, S.; Duger, T.; Coplu, L. Arm strength training improves activities of daily living and occupational performance in patients with COPD. Clin. Respir. J. 2017, 11, 820–832. [Google Scholar] [CrossRef]
- Duruturk, N.; Arıkan, H.; Ulubay, G.; Tekindal, M.A. A comparison of calisthenic and cycle exercise training in chronic obstructive pulmonary disease patients: A randomized controlled trial. Expert Rev. Respir. Med. 2016, 10, 99–108. [Google Scholar] [CrossRef]
- Hernández, M.T.; Rubio, T.M.; Ruiz, F.O.; Riera, H.S.; Gil, R.S.; Gómez, J.C. Results of a home-based training program for patients with COPD. Chest 2000, 118, 106–114. [Google Scholar] [CrossRef]
- Moore, J.; Fiddler, H.; Seymour, J.; Grant, A.; Jolley, C.; Johnson, L.; Moxham, J. Effect of a home exercise video programme in patients with chronic obstructive pulmonary disease. J. Rehabil. Med. 2009, 41, 195–200. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, S.D.; Taylor, N.F.; Paratz, J.D. A predominantly home-based progressive resistance exercise program increases knee extensor strength in the short-term in people with chronic obstructive pulmonary disease: A randomised controlled trial. Aust. J. Physiother. 2007, 53, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Wadell, K.; Webb, K.A.; Preston, M.E.; Amornputtisathaporn, N.; Samis, L.; Patelli, J.; Guenette, J.A.; O’Donnell, D.E. Impact of pulmonary rehabilitation on the major dimensions of dyspnea in COPD. COPD 2013, 10, 425–435. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.C.; Schünemann, H.J.; Oxman, A.D.; Pottie, K.; Meerpohl, J.J.; Coello, P.A.; Rind, D.; Montori, V.M.; Brito, J.P.; Norris, S.; et al. GRADE guidelines: 15. Going from evidence to recommendation-determinants of a recommendation’s direction and strength. J. Clin. Epidemiol. 2013, 66, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988; ISBN 0805802835/978-0805802832. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Group on behalf of the, C.S.M. Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2019; pp. 241–284. ISBN 978-1-119-53660-4. [Google Scholar]
- Rücker, G.; Schwarzer, G.; Carpenter, J.R.; Schumacher, M. Undue reliance on I(2) in assessing heterogeneity may mislead. BMC Med. Res. Methodol. 2008, 8, 79. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.H.; Chen, J.W.; Chen, X.; Lin, L.; Yan, H.Y.; Zhou, Y.Q.; Chen, R. Impact of Resistance Training in Subjects With COPD: A Systematic Review and Meta-Analysis. Respir. Care 2015, 60, 1130–1145. [Google Scholar] [CrossRef]
- Kruapanich, C.; Tantisuwat, A.; Thaveeratitham, P.; Lertmaharit, S.; Ubolnuar, N.; Mathiyakom, W. Effects of Different Modes of Upper Limb Training in Individuals with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Ann. Rehabil. Med. 2019, 43, 592–614. [Google Scholar] [CrossRef]
- Pereira, A.M.; Santa-Clara, H.; Pereira, E.; Simões, S.; Remédios, I.; Cardoso, J.; Brito, J.; Cabri, J.; Fernhall, B. Impact of combined exercise on chronic obstructive pulmonary patients’ state of health. Rev. Port. Pneumol. 2010, 16, 737–757. [Google Scholar] [CrossRef]
- Rinaldo, N.; Bacchi, E.; Coratella, G.; Vitali, F.; Milanese, C.; Rossi, A.; Schena, F.; Lanza, M. Effects of Combined Aerobic-Strength Training vs Fitness Education Program in COPD Patients. Int. J. Sport. Med. 2017, 38, 1001–1008. [Google Scholar] [CrossRef]
- Pauwels, R.A.; Buist, A.S.; Ma, P.; Jenkins, C.R.; Hurd, S.S.; GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: National Heart, Lung, and Blood Institute and World Health Organization Global Initiative for Chronic Obstructive Lung Disease (GOLD): Executive summary. Respir. Care 2001, 46, 798–825. [Google Scholar] [PubMed]
- Ottenheijm, C.A.; Heunks, L.M.; Sieck, G.C.; Zhan, W.Z.; Jansen, S.M.; Degens, H.; de Boo, T.; Dekhuijzen, P.N. Diaphragm dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 172, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Putt, M.T.; Watson, M.; Seale, H.; Paratz, J.D. Muscle stretching technique increases vital capacity and range of motion in patients with chronic obstructive pulmonary disease. Arch. Phys. Med. Rehabil. 2008, 89, 1103–1107. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Subjects aged 18 years old or older, diagnosed with COPD at moderate and severe stage of severity, in a stable phase of the disease (i.e., four weeks without hospital admissions or exacerbations, nor changes in medication), according to Gold [1]. |
| Intervention | Randomised control trials (RCTs) with interventions based on one of the following types of exercise: aerobic (AE), resistance (RE), stretching (ST) or combined (CE). |
| Comparison | All studies including a comparison of subjects that performed at least one type of exercise (i.e., AE, RE, ST, and CE), with others who maintained their daily activities with standard care for COPD. |
| Outcomes | Studies assessing the effects of exercise on dyspnoea or fatigue. |
| Type of Study | RCTs comparing AE, RE, ST or CE with a control group receiving no treatment or standard care were included. |
| Author/Year | Participants | Age (Years) (M ± SD) | Intervention | Outcomes | Conclusions |
|---|---|---|---|---|---|
| Arslan and Oztunc 2015 [20] | AE: 32 subjects CG: 33 subjects | AE = 56.9 ± 6.6 years CG * | Intervention: AE. Patients walked three days a week with low to moderate intensity. Comparison: treatment-as-usual (CG). Duration: 45 min. three times a week for 14 weeks. | Fatigue-Modified Borg Scale | Compared to CG, walking exercise programme applied to patients with COPD affected the fatigue symptom positively. |
| Bauldoff et al., 1996 [21] | RE: 10 subjects CG: 10 subjects | RE = 61 ± 14 years CG = 63 ± 13 years | Intervention: RE. Patients performed three sets of six repetitions of arms and shoulders exercises. The training level (weight used, sets, and repetitions) for the muscle groups began at a low stage and progressed, according to subject tolerance. Comparison: treatment-as-usual (CG). Duration: five times a week for eight weeks. | Fatigue-BFS | A home-based, upper-arm exercise programme can reduce perceptions of fatigue for patients with COPD. |
| Calik-Kutukcu et al., 2015 [22] | CE: 28 subjects SE: 28 subjects | RE = 58.38 ± 9.32 years CG = 59.71 ± 9.3 years | Intervention: RE. Exercise was conducted with free weights at 40–50% 1 RM, three sets/session, three times/week, with 8–12 reps loading for a total 23 supervised sessions over an eight-week period. Comparation: treatment-as-usual (CG). Duration: three times a week for eight weeks. | Fatigue-Modified Borg Scale Dyspnoea-BDI | Muscle strength exercise decreases dyspnoea and arm fatigue perception during supported arm exercises, and dyspnoea perception during daily living activities. |
| Duruturk et al., 2005 [23] | CE: 16 subjects AE: 16 subjects CG: 15 subjects | CE = 61.2 ± 5.1 years AE = 61.2 ± 5.0 years CG = 63.8 ± 5.7 years | Intervention: CE. The subjects performed 16 different rhythmical, and calisthenic exercises that included strengthening and stretching of the lower and upper extremity muscles. The intensity of the calisthenics was adjusted using the Modified Borg Scale to maintain a perceived difficulty level of between 4 and 7. The intensity of the aerobic exercise intensity was also adjusted based on the subjects’ Modified Borg Scale rated dyspnoea or leg fatigue. The intensity was increased if the Borg rate was <4, and decreased if it was >7. Comparation: treatment-as-usual (CG). Duration: three times a week for six weeks. Intervention: AE. The subjects performed cycle ergometer exercise (Dunlop Sport 1696 Cycle Ergometer, Japan) consisting of 20–30 min of continuous cycling at 50–70% of the VO2max obtained from the cycle ergometer exercise testing. Comparation: treatment-as-usual (CG). Duration: three times a week for six weeks. | Dyspnoea-MMRCDS Fatigue-FIS; FSS | The dyspnoea and fatigue changed significantly in exercise groups. There were no significant improvements in control group. |
| Hernández et al., 2000 [24] | AE: 30 subjects CG: 30 subjects | AE = 64.3 ± 8.3 years CG = 63.1 ± 6.9 years | Intervention: AE. The intensity of walking was set at 70% of the maximum speed attained on the shuttle walking test (SWT). Comparison: treatment-as-usual (CG). Duration: AE: six times per week (60 min) for 12 weeks. | Dyspnoea-BDI | AE exercise achieved improvement in dyspnoea and quality of life in COPD patients. |
| Moore et al., 2009 [25] | CE: 10 subjects CG: 10 subjects | CE = 70 ± 13 years CG = 70.5 ± * years | Intervention: CE. Warm-up, high-intensity interval exercises (upper and lower limb strengthening and aerobic exercise) and a cool-down including stretches. Free weights and body weight were used for strengthening. The subjects were educated to achieve the status of intensity “somewhat severely out of breath” and “somewhat severely tired”, corresponding to a Borg score of four. Comparison: treatment-as-usual (CG). Duration: four times a week (30 min) for six weeks. | Dyspnoea-CRQ-D Fatigue-CRQ-F | The experimental group had improved on dyspnoea and fatigue. |
| O’Shea et al., 2007 [26] | RE: 27 subjects CG: 27 subjects | RE = 66.9 ± 7.0 years CG = 68.4 ± 9.9 years | Intervention: RE. Progressive resistance exercise of three sets of eight to 12 repetition maximum progressed against elasticised bands. Comparison: treatment-as-usual (CG). Duration: three times a week for 12 weeks. | Dyspnoea-CRQ-D Fatigue-CRQ-F | The experimental group had improved on dyspnoea and fatigue. |
| Wadell et al., 2013 [27] | CE: 20 subjects CG: 20 subjects | CE = 68 ± 6.0 years CG = 66 ± 7.0 years | Intervention: CE. Sessions included graduated exercise for upper and lower limbs-walking on treadmill and in corridor, cycle ergometer, arm ergometer, strength/resistance exercises for upper and lower limbs. Subjects worked at their highest attainable work rate for the longest tolerable duration by targeting at least a “moderate” intensity of breathing discomfort on the modified 10-point Borg scale. Comparison: treatment-as-usual (CG). Duration: programme consisted of three supervised 2.5 h sessions per week over an 8-week period. | Dyspnoea-CRQ-D Fatigue-CRQ-F | The experimental group had improved on dyspnoea and fatigue. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Couto, N.; Cid, L.; Alves, S.; Brito, J.P.; Pimenta, N.; Bento, T. Analysing the Effects of Different Types of Exercise on Dyspnoea and Fatigue in Adults through COPD-Systematic Review and Meta-Analysis of Randomised Clinical Trials. Healthcare 2023, 11, 1449. https://doi.org/10.3390/healthcare11101449
Couto N, Cid L, Alves S, Brito JP, Pimenta N, Bento T. Analysing the Effects of Different Types of Exercise on Dyspnoea and Fatigue in Adults through COPD-Systematic Review and Meta-Analysis of Randomised Clinical Trials. Healthcare. 2023; 11(10):1449. https://doi.org/10.3390/healthcare11101449
Chicago/Turabian StyleCouto, Nuno, Luís Cid, Susana Alves, João Paulo Brito, Nuno Pimenta, and Teresa Bento. 2023. "Analysing the Effects of Different Types of Exercise on Dyspnoea and Fatigue in Adults through COPD-Systematic Review and Meta-Analysis of Randomised Clinical Trials" Healthcare 11, no. 10: 1449. https://doi.org/10.3390/healthcare11101449
APA StyleCouto, N., Cid, L., Alves, S., Brito, J. P., Pimenta, N., & Bento, T. (2023). Analysing the Effects of Different Types of Exercise on Dyspnoea and Fatigue in Adults through COPD-Systematic Review and Meta-Analysis of Randomised Clinical Trials. Healthcare, 11(10), 1449. https://doi.org/10.3390/healthcare11101449