

Association between Locomotive Syndrome and Physical Activity in Long-Term Inpatients of Psychiatric Care Wards in Japan: A Preliminary Study
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Basic Information
2.3. Physical Activity and Sedentary Behavior
2.4. Locomotive Syndrome Stage Tests
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Physical Activity Levels of the Participants
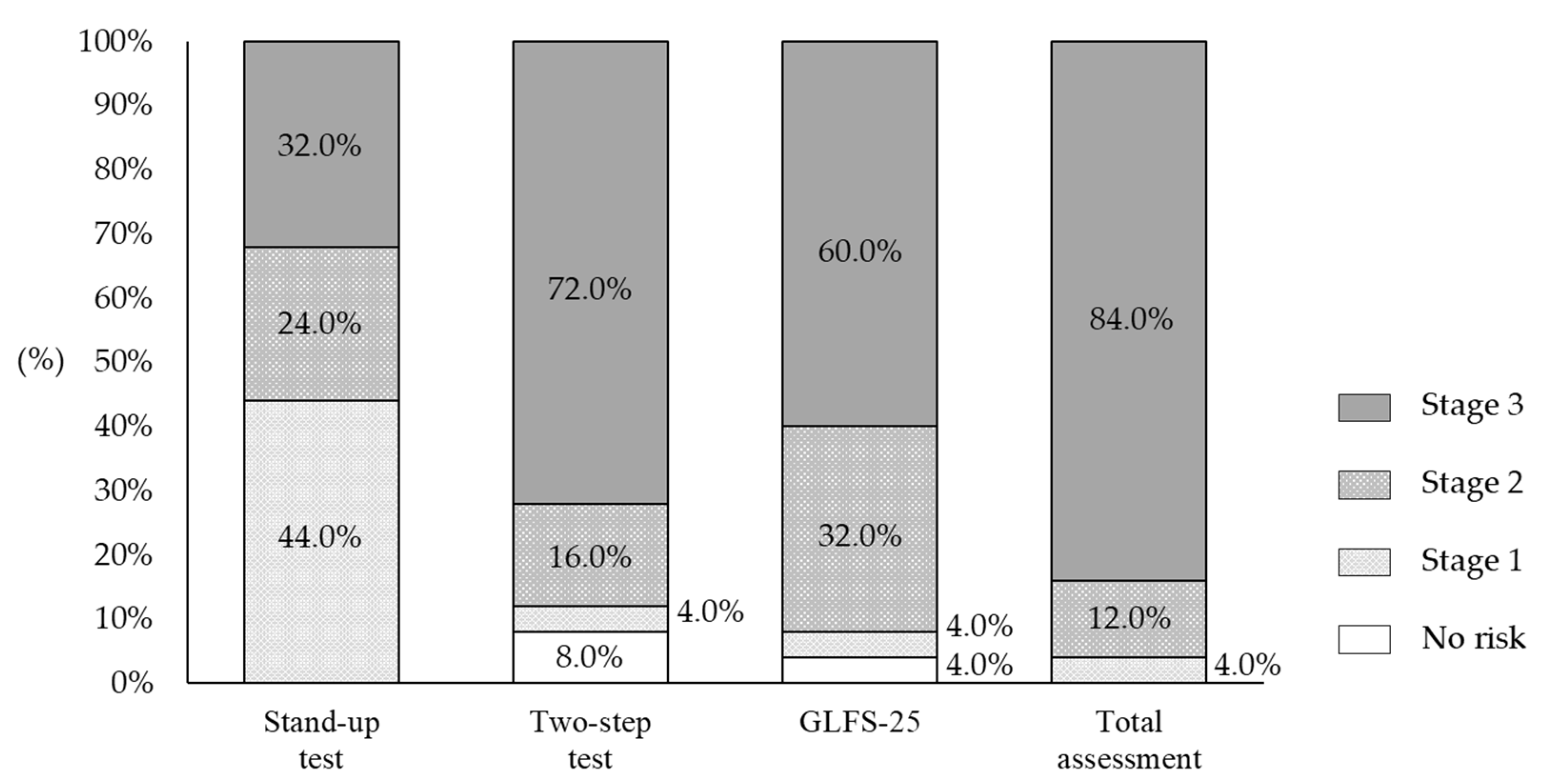
3.3. Distribution of Risk Levels for Locomotive Syndrome
3.4. Association between Locomotive Syndrome and Measured Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health, Labour and Welfare. Patient Survey 2017. 2017. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/kanja/17/index.html (accessed on 22 November 2021). (In Japanese).
- Ministry of Health, Labour and Welfare. Central Social Insurance Medical Council; 40th Result Verification Committee for Medical Fee Revision. 2014. Available online: https://www.mhlw.go.jp/stf/shingi/0000049078.html (accessed on 22 November 2021). (In Japanese).
- Robert, J.; Phillips, M.B. Physical disorder in 164 consecutive admissions to a mental hospital: The incidence and significance. BMJ 1937, 2, 363–366. [Google Scholar]
- Reininghaus, U.; Dutta, R.; Dazzan, P.; Doody, G.A.; Fearon, P.; Lappin, J.; Heslin, M.; Onyejiaka, A.; Donoghue, K.; Lomas, B.; et al. Mortality in schizophrenia and other psychoses: A 10-year follow-up of the ӔSOP first-episode cohort. Schizophr. Bull. 2015, 41, 664–673. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiovascular fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Rosenbaum, S.; Schuch, F.; Ward, P.B.; Richards, J.; Mugisha, J.; Probst, B. Cardiorespiratory fitness in severe mental illness: A systematic review and meta-analysis. Sports Med. 2017, 47, 343–352. [Google Scholar] [CrossRef]
- Vancampfort, D.; Probst, M.; Scheewe, T.; De Herdt, A.; Sweers, K.; Knapen, J.; van Winkel, R.; De Hert, M. Relationships between physical fitness, physical activity, smoking and metabolic and mental health parameters in people with schizophrenia. Psychiatry Res. 2013, 207, 25–32. [Google Scholar] [CrossRef]
- Vancampfort, D.; Sienaert, P.; Wyckaert, S.; Probst, M.; De Herbt, A.; De Hert, M.; Stubbs, B.; Buys, R. Cardiorespiratory fitness in outpatients with bipolar disorder versus matched controls: An exploratory study. J. Affect. Disord. 2016, 199, 1–5. [Google Scholar] [CrossRef][Green Version]
- Ishibashi, Y.; Arakawa, H.; Uezono, S.; Kitakaze, S.; Kota, M.; Daikuya, S.; Hirakawa, J.; Nakamura, T.; Chosa, E. Association between long-term hospitalization for mental illness and locomotive syndrome. J. Orthop. Sci. 2022, 27, 473–477. [Google Scholar] [CrossRef]
- Nakamura, K. A “super-aged” society and the “locomotive syndrome”. J. Orthop. Sci. 2008, 13, 1–2. [Google Scholar] [CrossRef]
- Vancampfort, D.; Firth, J.; Schuch, F.; Rosenbaum, S.; De Hert, M.; Mugisha, J.; Probst, M.; Stubbs, B. Physical activity and sedentary behavior in people with bipolar disorder: A systematic review and meta-analysis. J. Affect. Disord. 2016, 201, 145–152. [Google Scholar] [CrossRef]
- Schuch, F.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.; Reichert, T.; Bagatini, N.C.; Bgeginski, R.; Stubbs, B. Physical activity and sedentary behavior in people with major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2017, 210, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Williams, J.; Gaughran, F.; Craig, T. How sedentary are people with psychosis? A systematic review and meta-analysis. Schizophr. Res. 2016, 171, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Firth, J.; Berry, A.; Schuch, F.B.; Rosenbaum, S.; Gaughran, F.; Veronesse, N.; Williams, J.; Craig, T.; Yung, A.R.; et al. How much physical activity do people with schizophrenia engage in? A systematic review, comparative meta-analysis and meta-regression. Schizophr. Res. 2016, 176, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Firth, J.; Schuch, F.B.; Rosenbaum, S.; Mugisha, J.; Hallgren, M.; Probst, M.; Ward, P.B.; Gaughran, F.; De Hert, M.; et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: A global systematic review and meta-analysis. World Psychiatry 2017, 16, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Inada, T.; Inagaki, A. Psychoropic dose equivalence in Japan. Psychiatry Clin. Neurosci. 2015, 69, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Endicott, J.; Spitzer, R.L.; Fleiss, J.L.; Cohen, J. The Global Assessment Scale: A procedure for measuring overall severity of psychiatric disturbance. Arch. Gen. Psychiatry 1976, 33, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Suzuki, H.; Yasunaga, M.; Sugiyama, M.; Ijuin, M.; Sakuma, N.; Inagaki, H.; Iwasa, H.; Ura, C.; Yatomi, N.; et al. Brief screening tool for mild cognitive impairment in older Japanese: Validation of the Japanese version of the Montreal Cognitive Assessment. Geriatr. Gerontol. Int. 2010, 10, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Yokoyama, K.; Noriyasu, R.; Osaki, T.; Adachi, T.; Itoi, A.; Naito, Y.; Morimoto, T.; Kimura, M.; Oda, S. Light-intensity activities are important for estimating physical activity energy expenditure using uniaxial and triaxial accelerometers. Eur. J. Appl. Physiol. 2009, 105, 141–152. [Google Scholar] [CrossRef]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.W.; King, A.C.; et al. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995, 273, 402–407. [Google Scholar] [CrossRef]
- Japan Locomo Challenge Promotion Conference, The Japanese Orthopaedic Association 2018. 2018. Available online: https://locomo-joa.jp/check/judge (accessed on 22 November 2021). (In Japanese).
- Aoyagi, Y.; Park, H.; Watanabe, E.; Park, S.; Shephard, R.J. Habitual physical activity and physical fitness in older Japanese adults: The Nakanojo Study. Gerontology 2009, 55, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Park, S.; Shephard, R.J.; Aoyagi, Y. Yearlong physical activity and sarcopenia in older aduls: The Nakanojo Study. Eur. J. Appl. Physiol. 2010, 109, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Togo, F.; Watanabe, E.; Yasunaga, A.; Park, S.; Shephard, R.J.; Aoyagi, Y. Relationship of bone health to yearlong physical activity in older Japanese adults: Cross-sectional data from the Nakanojo Study. Osteoporos. Int. 2007, 18, 285–293. [Google Scholar] [CrossRef]
- Aoyagi, Y.; Park, H.; Kakiyama, T.; Park, S.; Yoshiuchi, K.; Shephard, R.J. Yearlong physical activity and regional stiffness of arteries in older adults: The Nakanojo Study. Eur. J. Appl. Physiol. 2010, 109, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, B.; Messias, E.; Harvey, P.D.; Fernandez-Egea, E.; Bowie, C.R. Is schizophrenia a syndrome of accelerated aging? Shizophr. Bull. 2008, 34, 1024–1032. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, N.; Muraki, S.; Nakamura, K.; Tanaka, S. Epidemiology of the locomotive syndrome: The research on osteoarthritis/osteoporosis against disability study 2005–2015. Mod. Rheumatol. 2017, 27, 1–7. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Sienaert, P.; Wyckaert, S.; De Hert, M.; Richards, J.; Kinyanda, E.; Probst, M. Depressive symptoms and muscular fitness contribute independently to the ability to perform daily life activities in people with bipolar disorder. Nord. J. Psychiatry 2016, 70, 477–482. [Google Scholar] [CrossRef]
- Vancampfort, D.; Sweers, K.; Probst, M.; Maurissen, K.; Knapen, J.; Minguet, P.; De Hert, M. Association of the metabolic syndrome with physical activity performance in patients with schizophrenia. Diabetes Metab. 2011, 37, 318–323. [Google Scholar] [CrossRef]
- Vancampfort, D.; Probst, M.; Scheewe, T.; Maurissen, K.; Sweers, K.; Knapen, J.; De Hert, M. Lack of physical activity during leisure time contribute to an impaired health related quality of life in patients with schizophrenia. Schizophr. Res. 2011, 129, 122–127. [Google Scholar] [CrossRef]
- Deenik, J.; Kruisdijk, F.; Tenback, D.; Braakman-Jansen, A.; Taal, E.; Hopman-Rock, M.; Beekman, A.; Tak, E.; Hendriksen, I.; van Harten, P. Physical activity and quality of life in long-term hospitalized patients with severe mental illness: A cross-sectional study. BMC Psychiatry 2017, 17, 298–307. [Google Scholar] [CrossRef]
- Zschucke, E.; Gaudlitz, K.; Ströhle, A. Exercise and physical activity in mental disorders: Clinical and experimental evidence. J. Prev. Med. Public Health 2013, 46, S12–S21. [Google Scholar] [CrossRef] [PubMed]
- Vera-Garcia, E.; Mayoral-Cleries, F.; Vancampfort, D.; Stubbs, B.; Cuesta-Vargas, A. A systematic review of the benefits of physical therapy within a multidisciplinary care approach for people with schizophrenia: An update. Psychiatry Res. 2015, 229, 828–839. [Google Scholar] [CrossRef] [PubMed]
- Silveira, H.; Moraes, H.; Oliveira, N.; Coutinho, E.; Laks, J.; Delandes, A. Physical exercise and clinically depressed patients: A systematic review and meta-analysis. Nueropsychobiology 2013, 67, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Kota, M.; Uezono, S.; Ishibashi, Y.; Kitakaze, S.; Arakawa, H. Relationship between whether the planned discharge destination is decided and locomotive syndrome for admitted patients in psychiatric long-term care wards. Phys. Ther. Res. 2020, 23, 180–187. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Overall (n = 25) | Male (n = 5) | Female (n = 20) |
|---|---|---|---|
| Age, y | 70.1 ± 9.3 | 67.0 ± 7.6 | 70.9 ± 9.7 |
| ≤59 y | 5 (20.0%) | 1 (20.0%) | 4 (20.0%) |
| 60–69 y | 7 (28.0%) | 2 (40.0%) | 5 (25.0%) |
| 70–79 y | 9 (36.0%) | 2 (40.0%) | 7 (35.0%) |
| ≥80 y | 4 (16.0%) | 0 (0.0%) | 4 (20.0%) |
| LOS, y | 16.2 ± 14.1 | 17.5 ± 16.9 | 15.8 ± 13.8 |
| ≥1y, <5y | 6 (24.0%) | 2 (40.0%) | 4 (20.0%) |
| ≥5y, <10y | 6 (24.0%) | 0 (0.0%) | 6 (30.0%) |
| ≥10y | 13 (52.0%) | 3 (60.0%) | 10 (50.0%) |
| BMI (kg/m2) | 22.5 ± 3.9 | 20.9 ± 4.1 | 22.9 ± 3.9 |
| CP dose (mg/day) | 646.9 ± 741.6 | 745.9 ± 611.3 | 621.1 ± 763.0 |
| Categories | Overall (n = 25) | Male (n = 5) | Female (n = 20) |
|---|---|---|---|
| F0 | 1 (4.0%) | 0 (0.0%) | 1 (5.0%) |
| F2 | 18 (72.0%) | 3 (60.0%) | 15 (75.0%) |
| F3 | 5 (20.0%) | 2 (40.0%) | 3 (15.0%) |
| F7 | 1 (4.0%) | 0 (0.0%) | 1 (5.0%) |
| Variables | Overall (n = 25) | Male (n = 5) | Female (n = 20) | |
|---|---|---|---|---|
| FIM-motor | 82.0 ± 9.1 | 83.8 ± 10.5 | 81.6 ± 8.9 | |
| FIM-cognitive | 27.4 ± 5.5 | 27.6 ± 7.5 | 27.4 ± 5.2 | |
| GAF | 11–20 | 1 (4.0%) | 1 (20.0%) | 0 (0.0%) |
| 21–30 | 16 (64.0%) | 3 (60.0%) | 13 (65.0%) | |
| 31–40 | 6 (24.0%) | 1 (20.0%) | 5 (25.0%) | |
| 41–50 | 1 (4.0%) | 0 (0.0%) | 1 (5.0%) | |
| 51–60 | 1 (4.0%) | 0 (0.0%) | 1 (5.0%) | |
| MoCA-J | 13.9 ± 6.8 | 15.0 ± 9.2 | 13.6 ± 6.6 | |
| Variables | Overall (n = 25) | Male (n = 5) | Female (n = 20) |
|---|---|---|---|
| Step counts (steps) | 3089.8 ± 2346.5 | 4243.3 ± 1685.3 | 2955.5 ± 2450.1 |
| Sedentary time (min) | 349.7 ± 68.6 | 366.3 ± 34.7 | 342.1 ± 74.7 |
| LPA time (min) | 122.4 ± 66.9 | 107.0 ± 32.1 | 129.8 ± 72.8 |
| MVPA time (min) | 9.2 ± 7.7 | 8.0± 9.2 | 9.3 ± 7.9 |
| Variables | Stand-Up Test | Two-Step Test | GLFS-25 |
|---|---|---|---|
| Age | −0.65 * | −0.59 | 0.65 ** |
| LOS | 0.02 | −0.12 | 0.27 |
| BMI | 0.42 | 0.30 | −0.33 |
| CP dose | 0.18 | 0.42 | −0.21 |
| FIM-motor | 0.78 ** | 0.73 ** | −0.68 ** |
| FIM-cognitive | 0.44 | 0.49 | −0.32 |
| GAF | 0.31 | 0.25 | −0.19 |
| MoCA-J | 0.21 | −0.06 | −0.15 |
| Step counts | 0.68 ** | 0.27 * | −0.41 |
| Sedentary time | −0.21 | 0.11 | 0.28 |
| LPA | 0.22 | −0.06 | −0.30 |
| MVPA | 0.35 | 0.11 | −0.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishibashi, Y.; Nishida, M.; Hirai, M.; Uezono, S.; Kitakaze, S.; Kota, M.; Nishimura, Y.; Tajima, F.; Arakawa, H. Association between Locomotive Syndrome and Physical Activity in Long-Term Inpatients of Psychiatric Care Wards in Japan: A Preliminary Study. Healthcare 2022, 10, 1741. https://doi.org/10.3390/healthcare10091741
Ishibashi Y, Nishida M, Hirai M, Uezono S, Kitakaze S, Kota M, Nishimura Y, Tajima F, Arakawa H. Association between Locomotive Syndrome and Physical Activity in Long-Term Inpatients of Psychiatric Care Wards in Japan: A Preliminary Study. Healthcare. 2022; 10(9):1741. https://doi.org/10.3390/healthcare10091741
Chicago/Turabian StyleIshibashi, Yusuke, Muneyoshi Nishida, Motoharu Hirai, Sae Uezono, Sosuke Kitakaze, Munetsugu Kota, Yukihide Nishimura, Fumihiro Tajima, and Hideki Arakawa. 2022. "Association between Locomotive Syndrome and Physical Activity in Long-Term Inpatients of Psychiatric Care Wards in Japan: A Preliminary Study" Healthcare 10, no. 9: 1741. https://doi.org/10.3390/healthcare10091741
APA StyleIshibashi, Y., Nishida, M., Hirai, M., Uezono, S., Kitakaze, S., Kota, M., Nishimura, Y., Tajima, F., & Arakawa, H. (2022). Association between Locomotive Syndrome and Physical Activity in Long-Term Inpatients of Psychiatric Care Wards in Japan: A Preliminary Study. Healthcare, 10(9), 1741. https://doi.org/10.3390/healthcare10091741