
Use of Netnography to Understand GoFundMe® Crowdfunding Profiles Posted for Individuals and Families of Children with Osteogenesis Imperfecta


Abstract
:1. Introduction
2. Materials and Methods
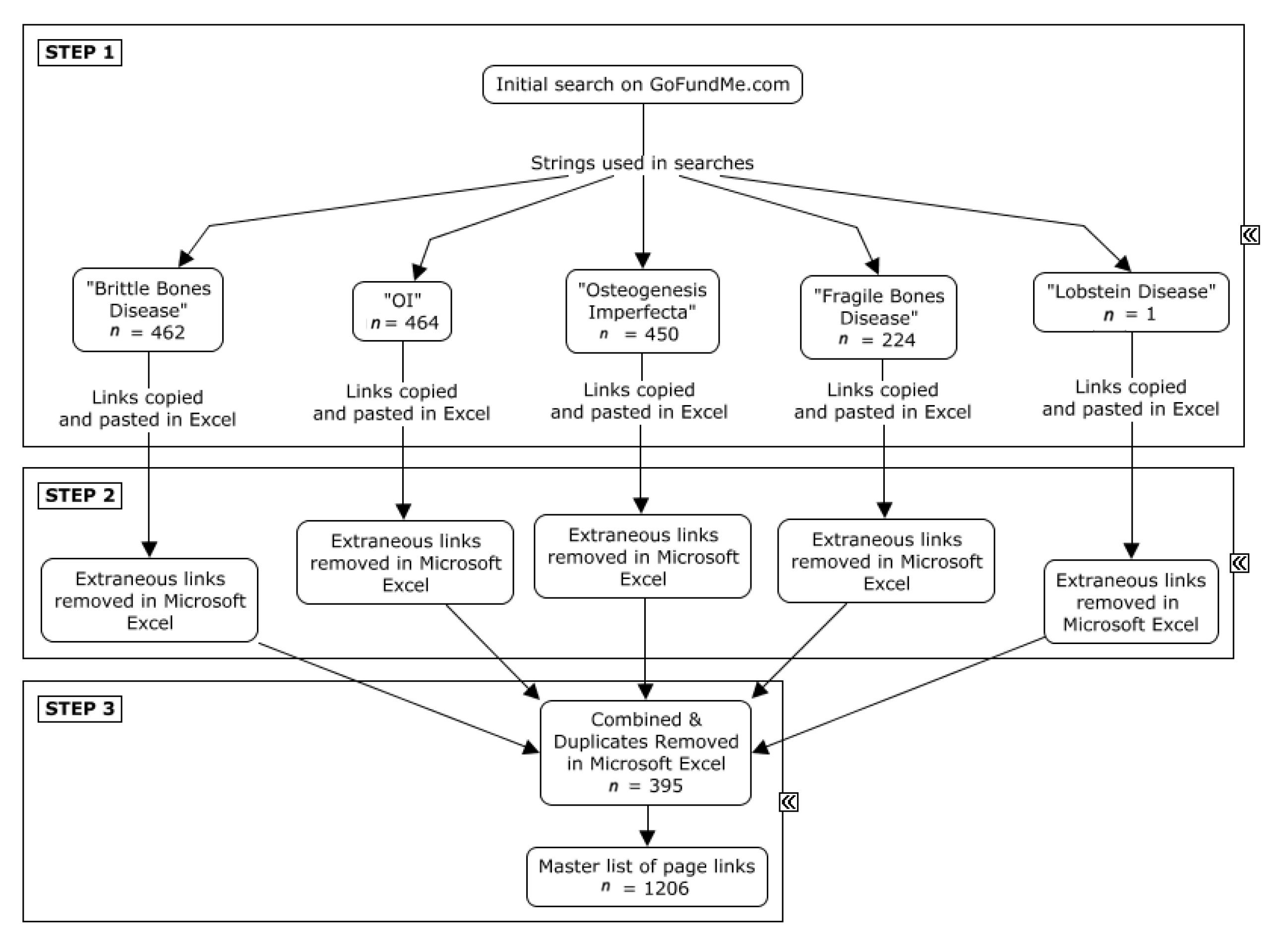
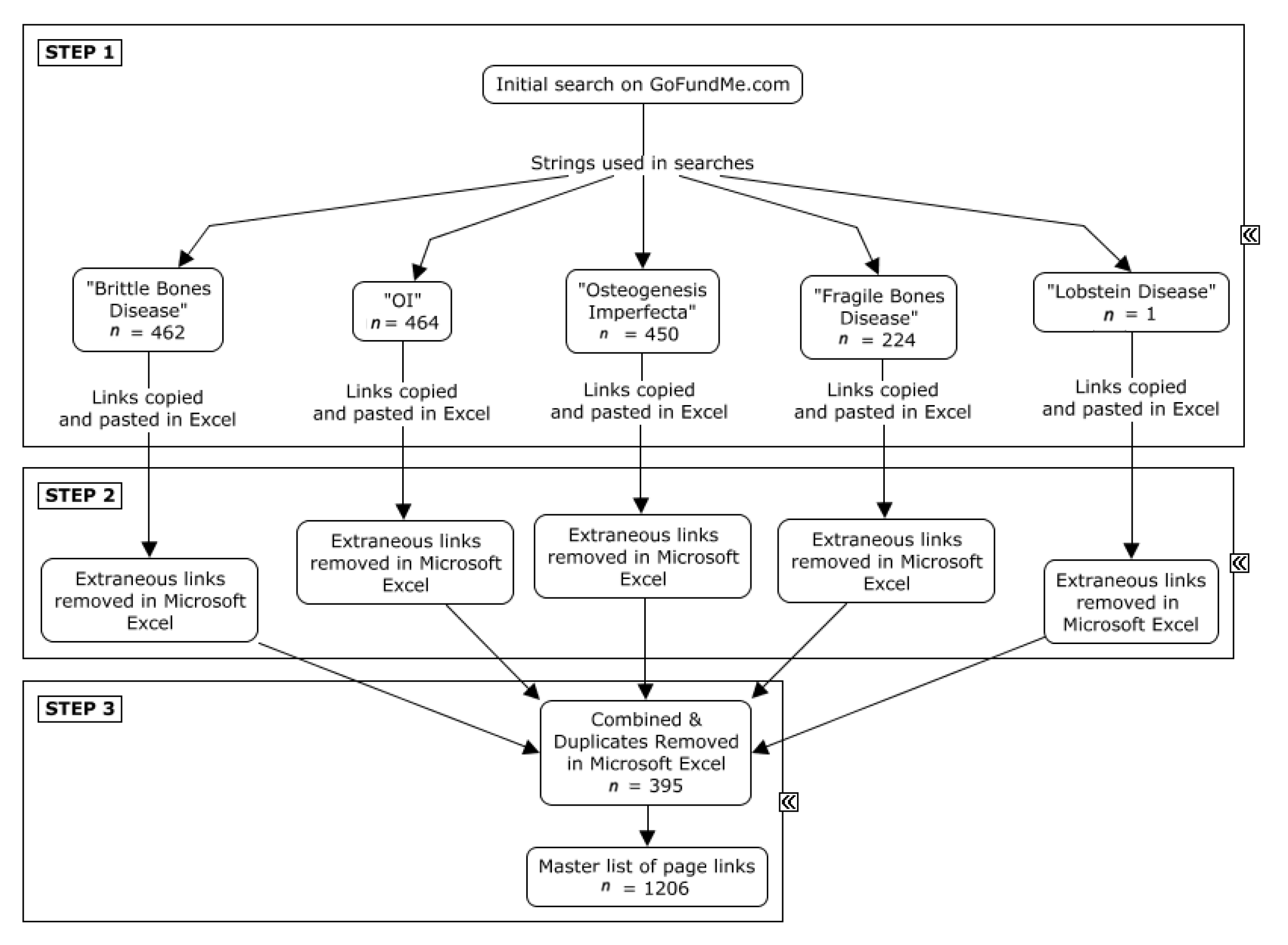
- Step 2: Extraneous links, which discussed legal information, common user questions, and other material unrelated to donation pages, were removed from the spreadsheets (Figure 2, Step 2).
- Step 3: The five spreadsheets were merged into one master list (n = 1601 links), and 395 duplicate links were subsequently removed (Figure 2, Step 3).
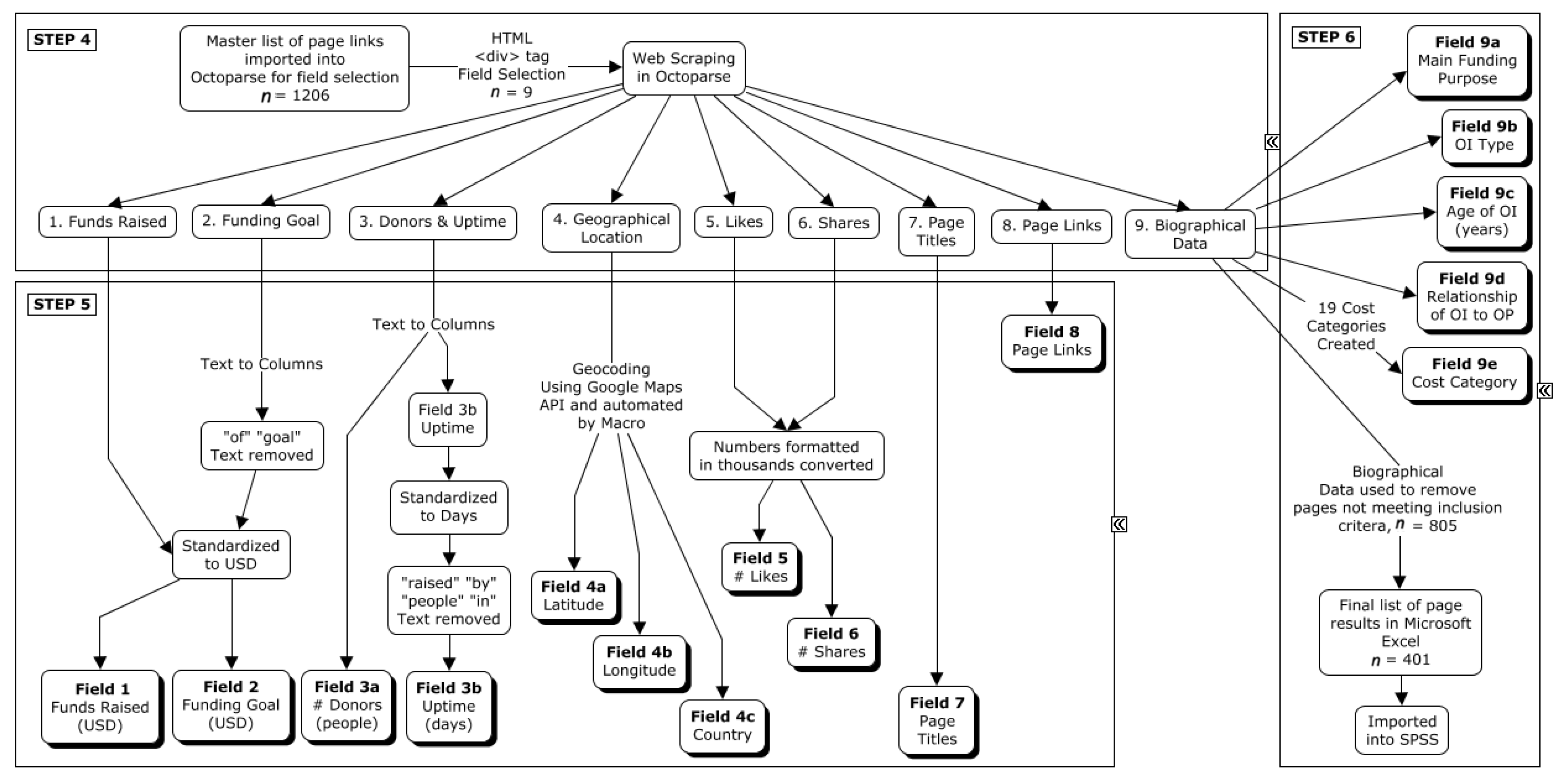
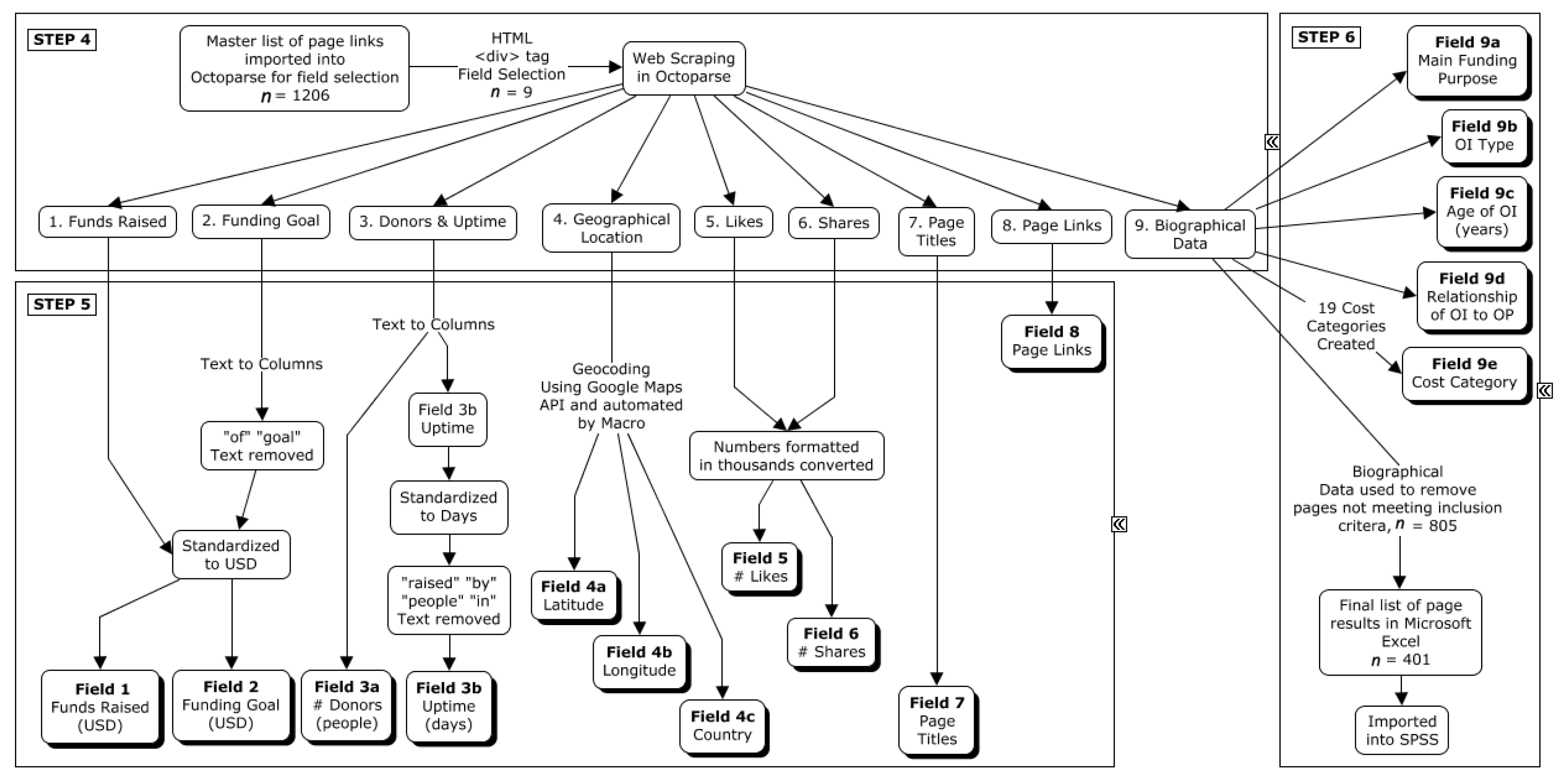
- Step 5: The dataset was cleaned prior to statistical analysis. MapMakerApp.com, 1 May 2022 [28], which uses the Google Maps Application Program Interface (API), was used to provide a geocoded location based on the civic addresses of individuals with OI. MacroRecorder [29] was used to automate the process of searching for the GPS coordinates (Figure 3, Step 5).
- Step 6: After combining the search results and removing duplicates, all biographical data were screened for eligibility. Included webpages were active donation pages on GoFundMe® posted in English, French, or Spanish that were raising funds for an individual diagnosed with OI. Webpages were excluded if there were no indications that the person for whom the webpage was created had OI, or if the funds were intended for the family of a person with OI rather than the person who has OI. Excluded webpages also included those referring to “OI” as British/Australian slang for “Hi”, “Hi” in Portuguese, and/or describing individuals with “brittle bones” due to other medical conditions (e.g., side effects of chemotherapy). The content of included biographies was extrapolated to create Fields 9a, 9b, 9c, and 9d, corresponding with the main funding purpose, the OI type, the age of the individual with OI (child was less than 18 years), and the relationship of the individual with OI to the donation page creator, respectively (Figure 3, Step 6). Field 9e contained a total of 19 different cost categories.
3. Experimental Results
3.1. Description of the GoFundMe® Web Profiles Created for Individuals with Osteogenesis Imperfecta
3.2. Description of the 19 Cost Categories Requested for Funding by the Osteogenesis Imperfecta Community on GoFundMe®
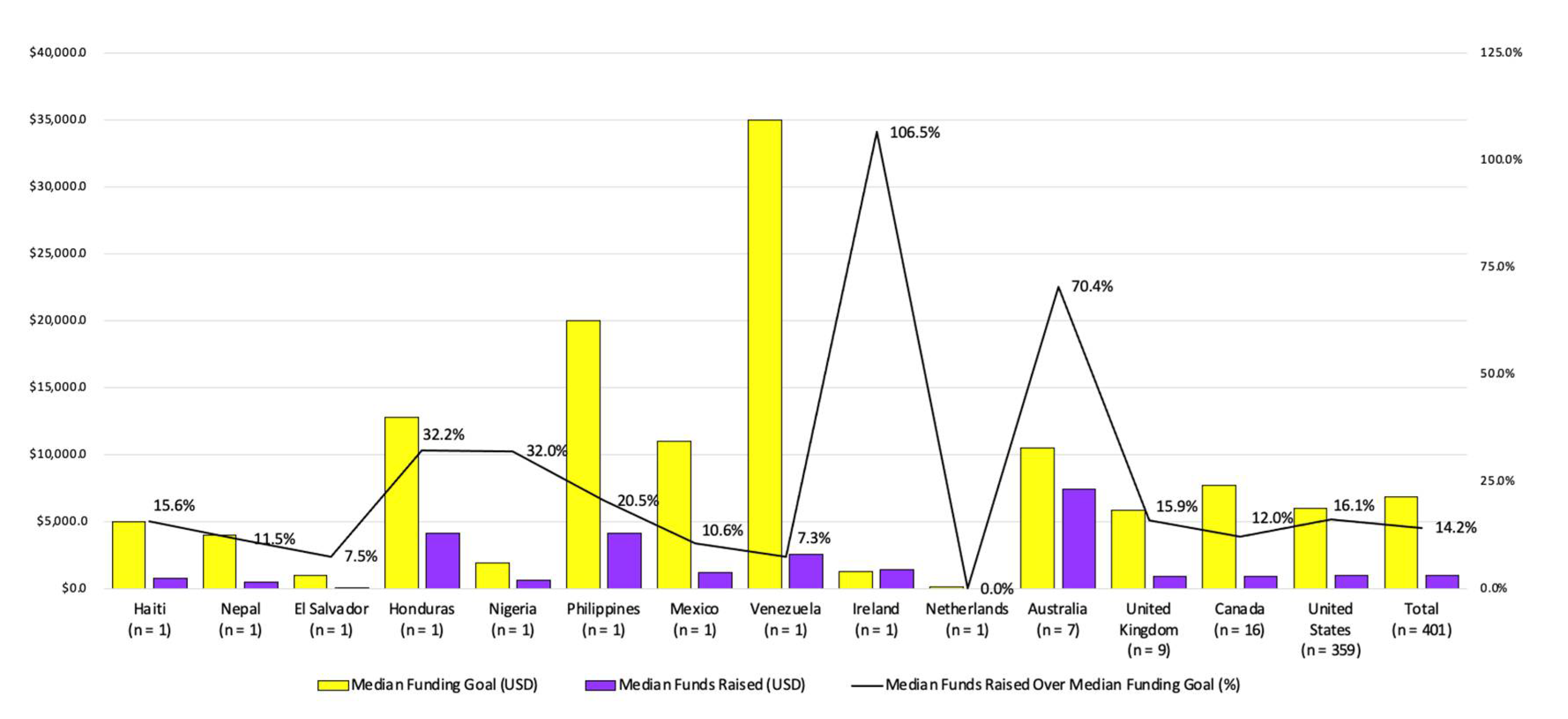
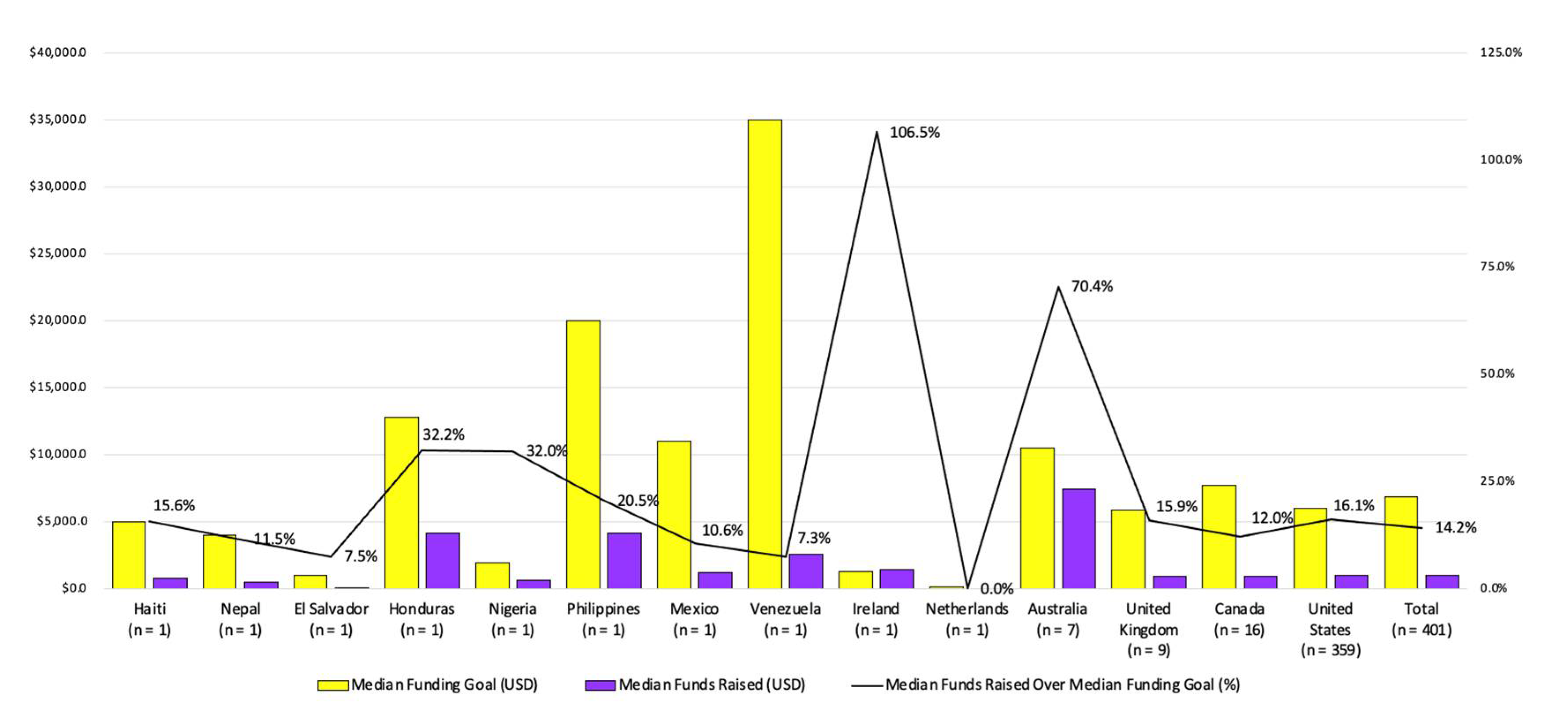
3.3. Funding Goals against Received Funding
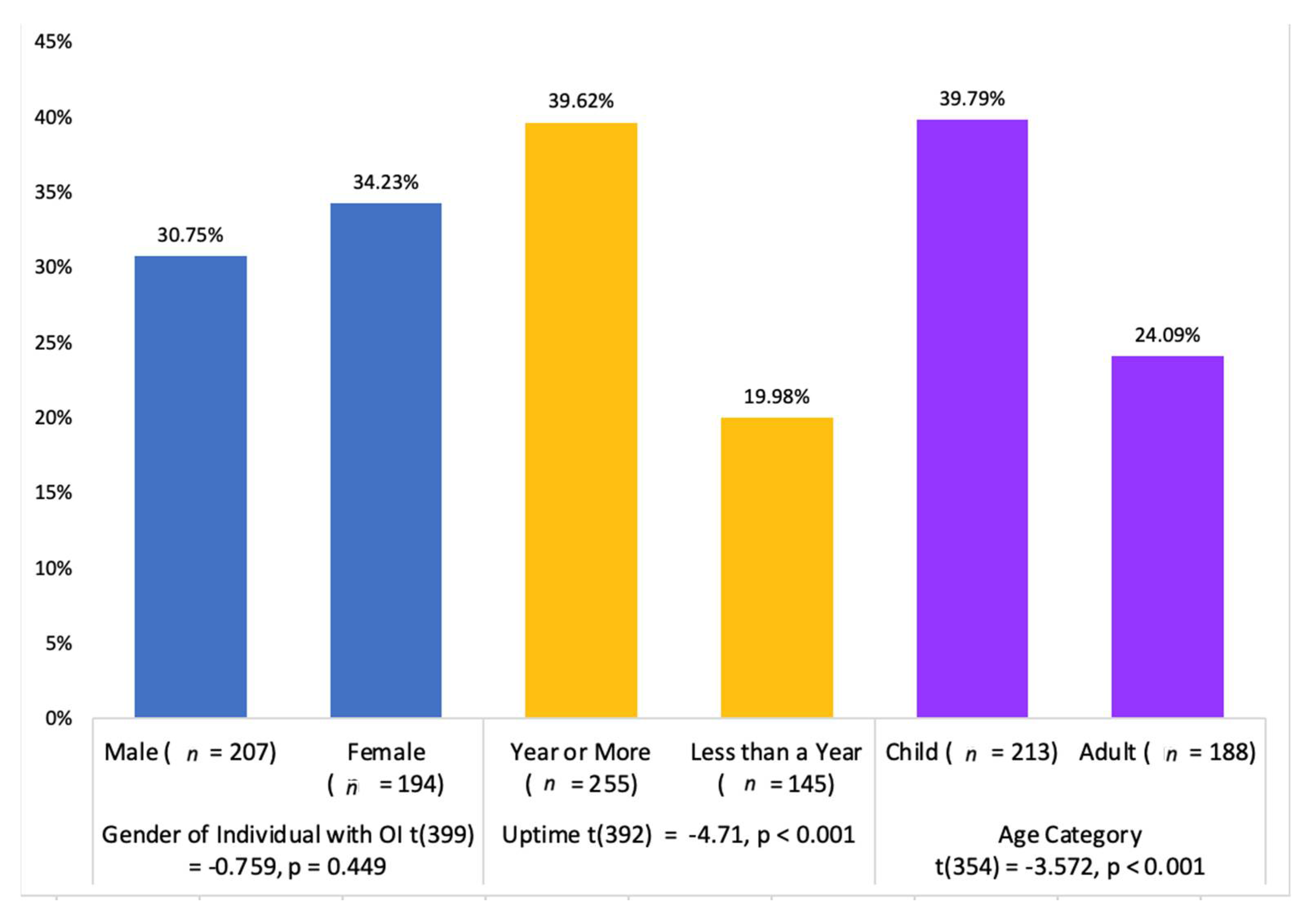
3.4. Contributing Factors to Selecting and Achieving Funding Goals and Specific Items or Requests That Increase Likelihood of Receiving Funding
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forlino, A.; Marini, J.C. Osteogenesis Imperfecta. Lancet 2016, 387, 1657–1671. [Google Scholar] [CrossRef]
- Van Dijk, F.S.; Cobben, J.M.; Kariminejad, A.; Maugeri, A.; Nikkels, P.G.; van Rijn, R.R.; Pals, G. Osteogenesis Imperfecta: A Review with Clinical Examples. Mol. Syndromol. 2011, 2, 1–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folkestad, L.; Hald, J.D.; Ersbøll, A.K.; Gram, J.; Hermann, A.P.; Langdahl, B.; Abrahamsen, B.; Brixen, K. Fracture Rates and Fracture Sites in Patients With Osteogenesis Imperfecta: A Nationwide Register-Based Cohort Study. J. Bone Miner. Res. 2017, 32, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dogba, M.J.; Bedos, C.; Durigova, M.; Montpetit, K.; Wong, T.; Glorieux, F.H.; Rauch, F. The Impact of Severe Osteogenesis Imperfecta on the Lives of Young Patients and Their Parents—A Qualitative Analysis. BMC Pediatrics 2013, 13, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dye, D.E.; Brameld, K.J.; Maxwell, S.; Goldblatt, J.; Bower, C.; Leonard, H.; Bourke, J.; Glasson, E.J.; O’Leary, P. The Impact of Single Gene and Chromosomal Disorders on Hospital Admissions of Children and Adolescents: A Population-Based Study. PHG 2011, 14, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczepaniak-Kubat, A.; Kurnatowska, O.; Jakubowska-Pietkiewicz, E.; Chlebna-Sokół, D. Assessment of Quality of Life of Parents of Children with Osteogenesis Imperfecta. Adv. Clin. Exp. Med. 2012, 21, 99–104. [Google Scholar] [PubMed]
- Claesson, I.B.; Brodin, J. What Families with Children with Brittle Bones Want to Tell. Child Care Health Dev. 2002, 28, 309–315. [Google Scholar] [CrossRef]
- Forestier-Zhang, L.; Watts, L.; Turner, A.; Teare, H.; Kaye, J.; Barrett, J.; Cooper, C.; Eastell, R.; Wordsworth, P.; Javaid, M.K.; et al. Health-Related Quality of Life and a Cost-Utility Simulation of Adults in the UK with Osteogenesis Imperfecta, X-Linked Hypophosphatemia and Fibrous Dysplasia. Orphanet J. Rare Dis. 2016, 11, 160. [Google Scholar] [CrossRef] [Green Version]
- Tsimicalis, A.; Stevens, B.; Ungar, W.J.; McKeever, P.; Greenberg, M. The Cost of Childhood Cancer from the Family’s Perspective: A Critical Review. Pediatric Blood Cancer 2011, 56, 707–717. [Google Scholar] [CrossRef]
- Morand, M.; Chougui, K.; Westerheim, K.; Thorstad, K.; Dubé, C.; Wong, T.; Hamdy, R.C.; Semler, O.; Carnevale, F.A.; Rauch, F. The Costs Incurred by Individuals Living with Osteogenesis Imperfecta (OI) and Their Families. In Proceedings of the International Conference on the Quality of Life for Osteogenesis Imperfecta, Amsterdam, The Netherlands, 22–25 November 2019. [Google Scholar]
- Anderson, D.; Dumont, S.; Jacobs, P.; Azzaria, L. The Personal Costs of Caring for a Child with a Disability: A Review of the Literature. Public Health Rep. 2007, 122, 3–16. [Google Scholar] [CrossRef]
- Jo, C. Cost-of-Illness Studies: Concepts, Scopes, and Methods. Clin. Mol. Hepatol. 2014, 20, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A.; Howard, A.; Sochett, E.; Harrington, J. Financial Burden in Families of Children with Osteogenesis Imperfecta (OI). Bone Abstr. 2017, 6. [Google Scholar] [CrossRef]
- Pelentsov, L.J.; Fielder, A.L.; Laws, T.A.; Esterman, A.J. The Supportive Care Needs of Parents with a Child with a Rare Disease: Results of an Online Survey. BMC Fam. Pract. 2016, 17, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, J.; Raghupathi, V.; Raghupathi, W. Understanding the Dimensions of Medical Crowdfunding: A Visual Analytics Approach. J. Med. Internet Res. 2020, 22, e18813. [Google Scholar] [CrossRef] [PubMed]
- Okediji, P.T.; Ojo, A.O.; Ojo, A.I.; Ojo, A.S.; Ojo, O.E.; Abioye-Kuteyi, E.A. The Economic Impacts of Chronic Illness on Households of Patients in Ile-Ife, South-Western Nigeria. Cureus 2017, 9, e1756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Website Analysis for December 2017. Available online: http://www.seogorillatactics.com/?s=analysis (accessed on 4 April 2022).
- Kozinets, R.V. Netnography: Redefined; SAGE: London, UK, 2015. [Google Scholar]
- Wolf, Z.R. Ethnography: The Method. In Nursing Research: A Qualitative Perspective; Munhall, P., Ed.; Jones and Barlett Publishers: Sudbury, MA, USA, 2012; pp. 285–338. [Google Scholar]
- Pittman, J.W.; Bennett, M.E.; Koroluk, L.D.; Robinson, S.G.; Phillips, C.L. Characterizing the Orthodontic Patient’s Purchase Decision: A Novel Approach Using Netnography. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Diniz, M.V.; Sun, S.Y.; Barsottini, C.; Viggiano, M.; Filho, R.C.S.; Pimenta, B.S.O.; Elias, K.M.; Horowitz, N.S.; Braga, A.; Berkowitz, R.S. Experience With the Use of an Online Community on Facebook for Brazilian Patients with Gestational Trophoblastic Disease: Netnography Study. J. Med. Internet Res. 2018, 20, e10897. [Google Scholar] [CrossRef] [Green Version]
- Witney, C.; Hendricks, J.; Cope, V. Variation of Kozinets’ Framework and Application to Nursing Research. Nurse Res. 2016, 23, 36–41. [Google Scholar] [CrossRef] [PubMed]
- About W3C. Available online: https://www.w3.org/Consortium/ (accessed on 4 April 2022).
- IBM Statistics for Windows, Version 20.0; IBM Corporation: New York, NY, USA, 2011.
- Roblin, G. Copy Links Advanced. 2018. Available online: https://www.crx4chrome.com/crx/231142/ (accessed on 1 May 2022).
- Lambert, J.; Frye, C. Microsoft Office 2016; Microsoft Press: Redmond, DC, USA, 2016. [Google Scholar]
- Octoparse; Octopus Datas Inc.: Diamond Bar, CA, USA, 2018.
- Ward, D. MapMakerApp.Com; My Maps Inc.: Boca Raton, FL, USA, 2018. [Google Scholar]
- MacroRecorder; Bartels Media GmbH: Dortmund, Germany, 2018.
- Akobundu, E.; Ju, J.; Blatt, L.; Mullins, C.D. Cost-of-Illness Studies. Pharmacoeconomics 2006, 24, 869–890. [Google Scholar] [CrossRef] [PubMed]
- Tsimicalis, A.; Stevens, B.; Ungar, W.J.; McKeever, P.; Greenberg, M.; Agha, M.; Guerriere, D.; Barr, R.; Naqvi, A.; Moineddin, R. A Prospective Study to Determine the Costs Incurred by Families of Children Newly Diagnosed with Cancer in Ontario. Psycho-Oncology 2012, 21, 1113–1123. [Google Scholar] [CrossRef]
- Tsimicalis, A.; Stevens, B.; Ungar, W.J.; McKeever, P.; Greenberg, M.; Agha, M.; Guerriere, D.; Naqvi, A.; Barr, R. A Mixed Method Approach to Describe the Out-of-Pocket Expenses Incurred by Families of Children with Cancer. Pediatric Blood Cancer 2013, 60, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Bodden, D.H.M.; van den Heuvel, M.W.H.; Engels, R.C.M.E.; Dirksen, C.D. Societal Costs of Subclinical Depressive Symptoms in Dutch Adolescents: A Cost-of-Illness Study. J. Child Psychol. Psychiatry 2022, 63, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Angelis, A.; Kanavos, P.; López-Bastida, J.; Linertová, R.; Serrano-Aguilar, P.; Serrano-Aguilar, P.; Linertová, R.; López-Bastida, J.; Oliva-Moreno, J.; de la Paz, M.P.; et al. Socioeconomic Costs and Health-Related Quality of Life in Juvenile Idiopathic Arthritis: A Cost-of-Illness Study in the United Kingdom. BMC Musculoskelet Disord. 2016, 17, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belova, A.; Fann, N.; Haskell, J.; Hubbell, B.; Narayan, T. Estimating Lifetime Cost of Illness. An Application to Asthma. Ann. ATS 2020, 17, 1558–1569. [Google Scholar] [CrossRef] [PubMed]
- Altalib, A.; Althomali, A.; Alshahrani, A.; Alfrayyan, A.; Aljughaiman, M.S. Osteogenesis Imperfecta and Child Abuse From a Forensic Point of View. Cureus 2021, 13, e12790. [Google Scholar] [CrossRef]
- D’Eufemia, P.; Palombaro, M.; Lodato, V.; Zambrano, A.; Celli, M.; Persiani, P.; De Bari, M.P.; Sangiorgi, L. Child Abuse and Osteogenesis Imperfecta: How Can They Be Still Misdiagnosed? A Case Report. Clin. Cases Min. Bone Metab. 2012, 9, 195–197. [Google Scholar]
- Nieke, J.P.; Van As, A.B. Child Abuse and/or Osteogenesis Imperfecta? The Challenging Management of Patients with Unclear Diagnosis. S. Afr. Med. J. 2021, 111, 386. [Google Scholar] [CrossRef]
- Chau, F.Y.; Wallace, D.; Vajaranant, T.; Herndon, L.; Lee, P.; Challa, P.; Allingham, R.; Maumenee, I. Chapter 31—Osteogenesis Imperfecta and the Eye. In Osteogenesis Imperfecta; Shapiro, J.R., Byers, P.H., Glorieux, F.H., Sponseller, P.D., Eds.; Academic Press: San Diego, GA, USA, 2014; pp. 289–303. [Google Scholar] [CrossRef]
- Roddy, Á. Income and Conversion Handicaps: Estimating the Impact of Child Chronic Illness/Disability on Family Income and the Extra Cost of Child Chronic Illness/Child Disability in Ireland Using a Standard of Living Approach. Eur. J. Health Econ. 2021, 23, 467–483. [Google Scholar] [CrossRef] [PubMed]
- Ralston, S.H.; Gaston, M.S. Management of Osteogenesis Imperfecta. Front. Endocrinol. 2020, 10, 924. [Google Scholar] [CrossRef] [Green Version]
- Disability Accommodation Cost Guides. Available online: https://www.homeadvisor.com/cost/disability-accommodation/ (accessed on 4 April 2022).
- Marr, C.; Seasman, A.; Bishop, N. Managing the Patient with Osteogenesis Imperfecta: A Multidisciplinary Approach. J. Multidiscip. Healthc. 2017, 10, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Angelis, A.; Tordrup, D.; Kanavos, P. Socio-Economic Burden of Rare Diseases: A Systematic Review of Cost of Illness Evidence. Health Policy 2015, 119, 964–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadić, V.; Hundt, G.L.; Keeley, S.; Rahi, J.S.; Vision-Related Quality of Life (VQoL) Group. Seeing It My Way: Living with Childhood Onset Visual Disability. Child Care Health Dev. 2015, 41, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.M.; Corrêa, J.C.F.; Pereira, G.S.; Corrêa, F.I. Social Participation Following a Stroke: An Assessment in Accordance with the International Classification of Functioning, Disability and Health. Disabil. Rehabil. 2019, 41, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Squires, M.E.; Burnell, B.A.; McCarty, C.; Schnackenberg, H. Emerging Adults: Perspectives of College Students with Disabilities. J. Postsecond. Educ. Disabil. 2018, 31, 121–134. [Google Scholar]
- Bezyak, J.L.; Sabella, S.A.; Gattis, R.H. Public Transportation: An Investigation of Barriers for People with Disabilities. J. Disabil. Policy Stud. 2017, 28, 52–60. [Google Scholar] [CrossRef]
- Schreuer, N.; Plaut, P.; Golan, L.; Sachs, D. The Relations between Walkable Neighbourhoods and Active Participation in Daily Activities of People with Disabilities. J. Transp. Health 2019, 15, 100630. [Google Scholar] [CrossRef]
- Finfgeld-Connett, D. Clarification of Social Support. J. Nurs. Scholarsh. 2005, 37, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Tsimicalis, A.; Stevens, B.; Ungar, W.J.; Greenberg, M.; McKeever, P.; Agha, M.; Guerriere, D.; Barr, R.; Naqvi, A.; Moineddin, R. Determining the Costs of Families’ Support Networks Following a Child’s Cancer Diagnosis. Cancer Nurs. 2013, 36, E8. [Google Scholar] [CrossRef]
- Small, D.A.; Verrochi, N.M. The Face of Need: Facial Emotion Expression on Charity Advertisements. J. Mark. Res. 2009, 46, 777–787. [Google Scholar] [CrossRef]
- Erlandsson, A.; Nilsson, A.; Västfjäll, D. Attitudes and Donation Behavior When Reading Positive and Negative Charity Appeals. J. Nonprofit Public Sect. Mark. 2018, 30, 444–474. [Google Scholar] [CrossRef] [Green Version]
- Ridic, G.; Gleason, S.; Ridic, O. Comparisons of Health Care Systems in the United States, Germany and Canada. Mater Sociomed 2012, 24, 112–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bickenbach, J.; Rubinelli, S.; Stucki, G. Being a Person with Disabilities or Experiencing Disability: Two Perspectives on the Social Response to Disability. J. Rehabil. Med. 2017, 49, 543–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tips for Finding Financial Aid. Available online: https://rarediseases.info.nih.gov/Guides/pages/149/tips-for-finding-financial-aid (accessed on 4 April 2022).
- Lee, S.; Lehdonvirta, V. New Digital Safety Net or Just More ‘Friendfunding’? Institutional Analysis of Medical Crowdfunding in the United States; SSRN Scholarly Paper ID 3559901; Social Science Research Network: Rochester, NY, USA, 2020. [Google Scholar] [CrossRef] [Green Version]
- Snyder, J.; Mathers, A.; Crooks, V.A. Fund My Treatment!: A Call for Ethics-Focused Social Science Research into the Use of Crowdfunding for Medical Care. Soc. Sci. Med. 2016, 169, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Kenworthy, N.; Dong, Z.; Montgomery, A.; Fuller, E.; Berliner, L. A Cross-Sectional Study of Social Inequities in Medical Crowdfunding Campaigns in the United States. PLoS ONE 2020, 15, e0229760. [Google Scholar] [CrossRef]
- ICT Facts and Figures. Available online: https://www.itu.int/en/ITU-D/Statistics/Pages/facts/default.aspx (accessed on 5 April 2022).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cost Category | Cost Description | Median Funds Raised (USD) | Median Funding Goal (USD) | Funds Raised Over Funding Goal (%) | # of Donors | # of Uptime (Days) |
|---|---|---|---|---|---|---|
| Direct Costs | ||||||
| Direct Healthcare Costs | ||||||
| Any dental care costs incurred as a result of OI | 1580 | 7250 | 21.8% | 19.00 | 608 |
| Eye care or surgery related to OI | 110 | 1000 | 11.0% | 2.00 | 304 |
| Audiology services or American Sign Language lessons that are needed as a result of OI | 1120 | 7000 | 16.0% | 18.00 | 7301 |
| Costs associated with a hospital stay (imaging, laboratory tests, registration) | 1530 | 10,000 | 15.3% | 27.00 | 821 |
| Surgeries for fracture repairs, surgeries to prevent or palliate future fractures | 827 | 10,000 | 8.3% | 11.00 | 700 |
| Difficulty with affording medications such as Forteo or Pamidronate | 900 | 10,000 | 9.0% | 10.00 | 274 |
| Costs of repairing or obtaining wheelchairs, scooters, portable oxygen, walkers | 1427 | 5000 | 28.5% | 22.00 | 791 |
| Costs associated with physical therapy equipment and services | 2574 | 9000 | 28.6% | 22.50 | 1034 |
| Support for personal life elements such as in vitro fertilization, genetic counseling | 878 | 7000 | 12.5% | 18.00 | 1049 |
| Direct Non-healthcare Costs | ||||||
| Modifying, obtaining, or repairing a vehicle that is wheelchair adapted | 1135 | 20,000 | 5.7% | 13.00 | 669 |
| Home renovations such as lifts, ramps, kitchen adaptations, bathroom adaptations, or any attempt to improve wheelchair mobility within the home | 800 | 10,000 | 8.0% | 15.00 | 578 |
| Household bills, rent, utilities, furniture | 467 | 3500 | 13.3% | 4.00 | 319 |
| Legal expenses due to OI | 13 | 5500 | 0.2% | 0.50 | 380 |
| Food, groceries, clothing | 440 | 3000 | 14.7% | 6.00 | 335 |
| Adaptive software, computer, education costs, travel for work/internship, adaptive devices, support for professional sports | 648 | 5500 | 11.8% | 9.00 | 639 |
| The cost of traveling for health care services, including lodging, plane tickets, gas, ambulances, moving expenses | 780 | 5000 | 15.6% | 13.00 | 669 |
| The need for funding for family vacations, holiday presents, concerts | 353 | 3750 | 9.4% | 10.00 | 669 |
| Funeral costs associated with relatives who have passed on as a result of OI | 975 | 30,000 | 32.5% | 25.00 | 760 |
| Indirect Costs | ||||||
| Lost wages as a result of OI or caring for someone with OI | 14,500 | 8000 | 18.1% | 16.00 | 608 |
| Total (n = 401) | 965 | 6812 | 14.2% | 14.00 | 669 | |
| Cost Category | Cost Description | Median Funds Raised (USD) | Median Funding Goal (USD) | Funds Raised Over Funding Goal (%) | Median # of Donors | Median # of Uptime (Days) |
|---|---|---|---|---|---|---|
| Direct Costs | ||||||
| Direct Healthcare Costs | ||||||
| Costs associated with a hospital stay (imaging, laboratory tests, registration) | 9175 | 5000 | 183.5% | 33.00 | 121.67 |
| Surgeries for fracture repairs, surgeries to prevent or palliate future fractures | 3100 | 3000 | 103.3% | 57.00 | 699.59 |
| Costs of repairing or obtaining wheelchairs, scooters, portable oxygen, walkers | 5777 | 5306 | 108.9% | 96.00 | 958.14 |
| Direct Non-healthcare Costs | ||||||
| Modifying, obtaining, or repairing a vehicle that is wheelchair adapted | 5000 | 500 | 100.0% | 13.00 | 851.68 |
| Home renovations such as lifts, ramps, kitchen adaptations, bathroom adaptations, or any attempt to improve wheelchair mobility within the home | 7560 | 6000 | 126.0% | 100.00 | 912.51 |
| Household bills, rent, utilities, furniture | 3895 | 2700 | 144.3% | 44.00 | 577.92 |
| Adaptive software, computer, education costs, travel for work/internship, adaptive devices, support for professional sports | 7535 | 5500 | 137.0% | 157.00 | 912.51 |
| The cost of traveling for health care services, including lodging, plane tickets, gas, ambulances, moving expenses | 9670 | 4000 | 241.8% | 147.00 | 425.84 |
| The need for funding for family vacations, holiday presents, concerts | 838 | 800 | 104.7% | 16.50 | 486.67 |
| Funeral costs associated with relatives who have passed on as a result of OI | 4285 | 4000 | 107.1% | 46.00 | 790.84 |
| Indirect Costs | ||||||
| Lost wages as a result of OI or caring for someone with OI | 2125 | 2000 | 106.3% | 16.00 | 760.43 |
| Total (n = 37) | 4285 | 3500 | 122.4% | 57.00 | 760.43 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsimicalis, A.; Gasse, M.; Morand, M.; Rauch, F. Use of Netnography to Understand GoFundMe® Crowdfunding Profiles Posted for Individuals and Families of Children with Osteogenesis Imperfecta. Healthcare 2022, 10, 1451. https://doi.org/10.3390/healthcare10081451
Tsimicalis A, Gasse M, Morand M, Rauch F. Use of Netnography to Understand GoFundMe® Crowdfunding Profiles Posted for Individuals and Families of Children with Osteogenesis Imperfecta. Healthcare. 2022; 10(8):1451. https://doi.org/10.3390/healthcare10081451
Chicago/Turabian StyleTsimicalis, Argerie, Michael Gasse, Marilyn Morand, and Frank Rauch. 2022. "Use of Netnography to Understand GoFundMe® Crowdfunding Profiles Posted for Individuals and Families of Children with Osteogenesis Imperfecta" Healthcare 10, no. 8: 1451. https://doi.org/10.3390/healthcare10081451
APA StyleTsimicalis, A., Gasse, M., Morand, M., & Rauch, F. (2022). Use of Netnography to Understand GoFundMe® Crowdfunding Profiles Posted for Individuals and Families of Children with Osteogenesis Imperfecta. Healthcare, 10(8), 1451. https://doi.org/10.3390/healthcare10081451