
Validation of the Spanish Version of the Questionnaire on Environmental Awareness in Nursing (NEAT)

 , , and
, , and
Abstract
:1. Introduction
Theoretical Foundation: Nursing, Awareness, and Sustainability
2. Materials and Methods
2.1. Study Design
2.2. Sample
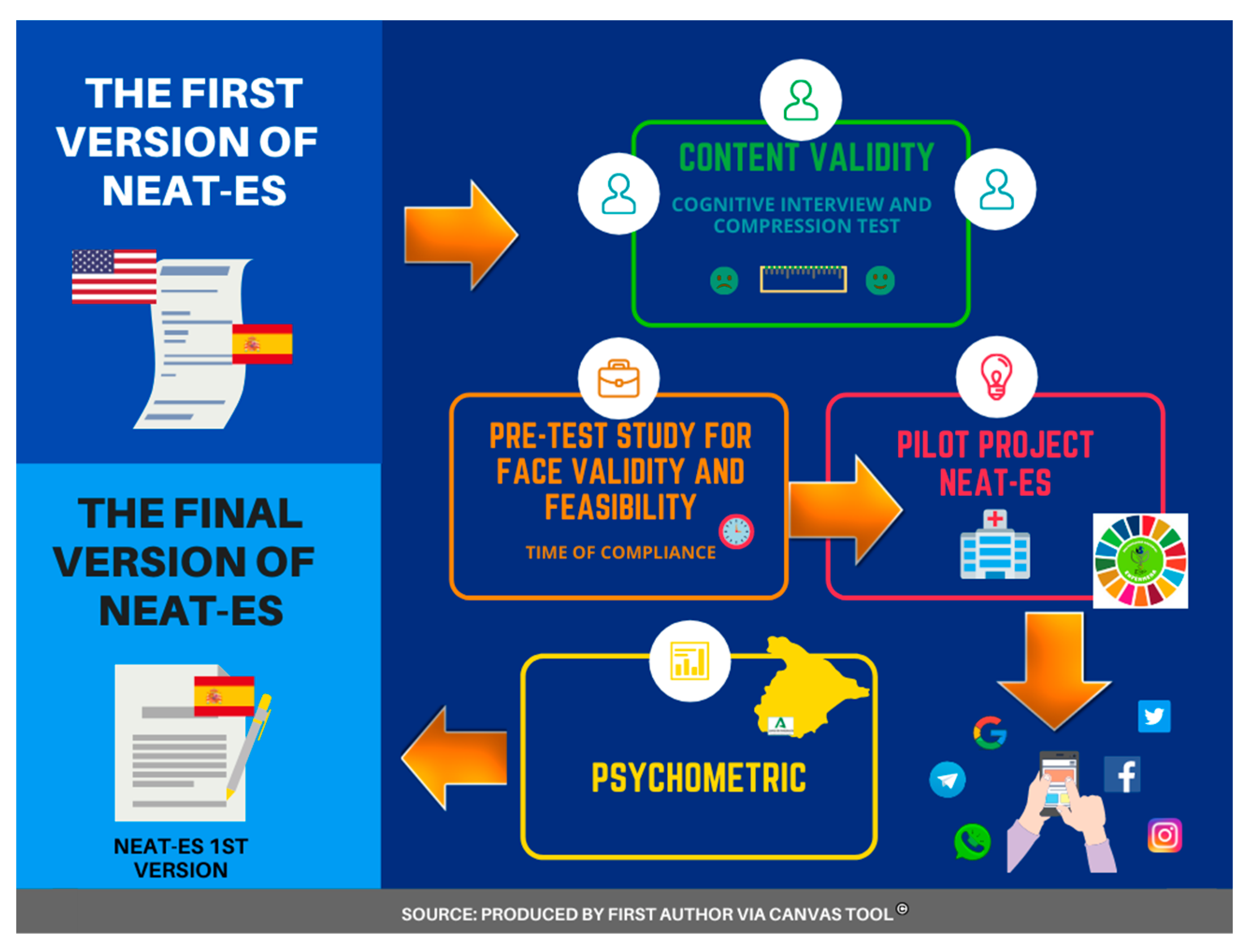
2.3. Validation Process
2.3.1. Translation and Back Translation
2.3.2. Participants of Cognitive Interview (CI)
2.3.3. Participants in End-Users Group Analysis and Pre-Test
2.3.4. Participants of the Pilot Study and Final Sample
2.4. Nurse’s Environmental Awareness Tool
2.5. Data Analysis
2.5.1. Qualitative Study: Cognitive Interview
2.5.2. Pre-Test Study and Pilot Study
2.5.3. Statistical Analysis: Descriptive and Psychometrics for Final Validation
2.6. Ethical Considerations
3. Results
3.1. Qualitative Study: Cognitive Interview
3.2. Pre-Test and Pilot Study
3.3. Result Psychometric for Final Validation: Reliability and Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA)
3.3.1. NAS-es Scale: Reliability, EFA, and CFA
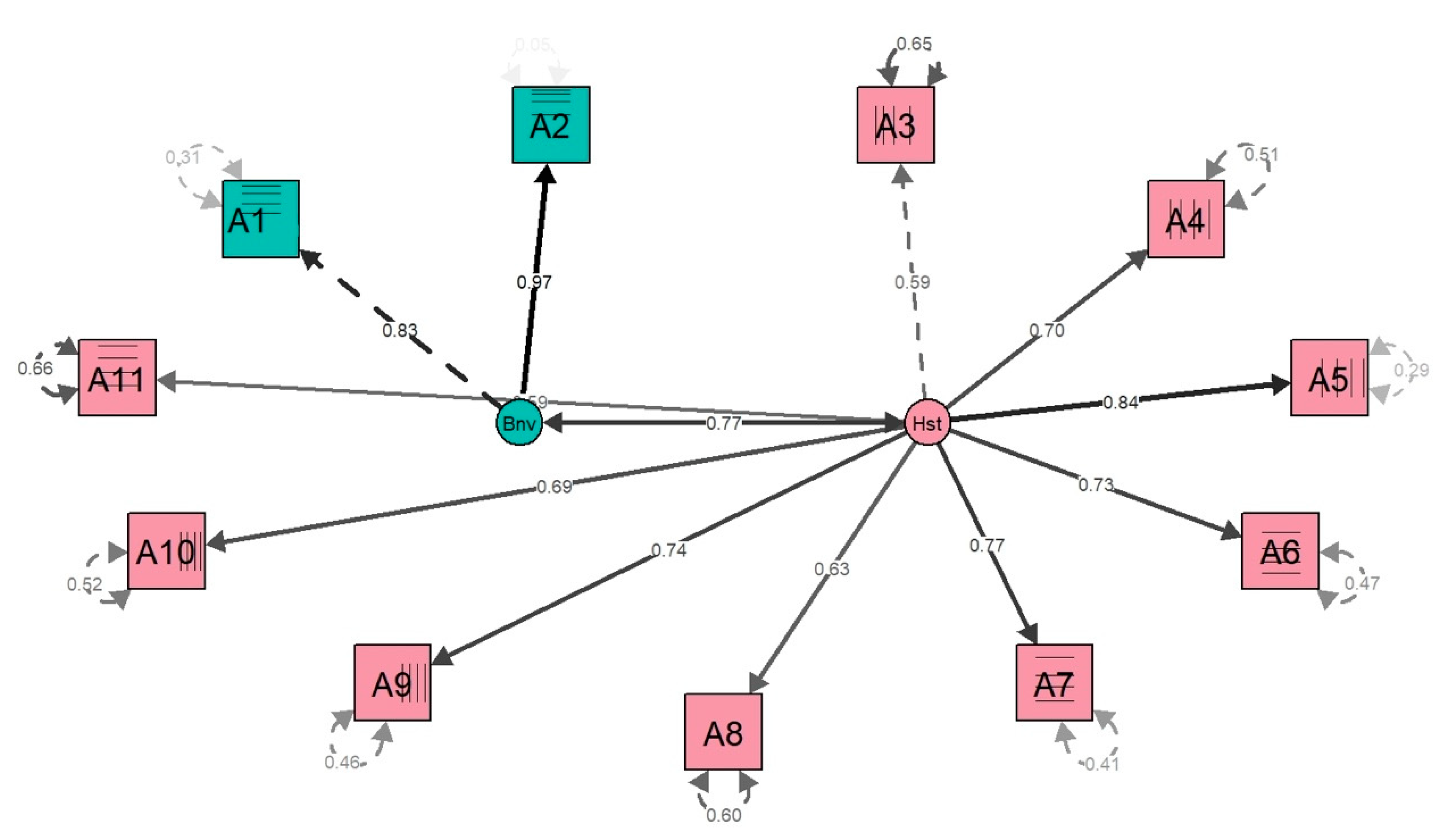
3.3.2. NPEB-es Scale: Reliability and Exploratory and Confirmatory Factor Analysis
3.3.3. PEB-es Scale: Reliability and Exploratory and Confirmatory Factor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| 1.-NAS: Escala de conciencia del personal enfermero. | |||
| Ítems | Por favor. lea las afirmaciones y conteste: Responda con la escala de la derecha. | ¿Ha oído hablar antes de esta información? Escala likert: 1.-No. nunca he oído hablar. 5.-Sí. definitivamente he oído hablar. | ¿Cómo cree que esto impacta sobre la salud? Escala likert: 1.-Nunca 5.-Mucho |
| A1 | De acuerdo con el Ministerio de Energía. la atención sanitaria se sitúa como el cuarto mayor consumidor de la energía dentro del sector servicios. | ||
| A2 | Los hospitales y centros de salud usan un 2% del consumo energético total. lo que supone un 30% respecto el sector de los edificios. | ||
| A3 | La mayor parte de la energía consumida en España. incluida la del sector sanitario. se basa en fuentes no renovables. | ||
| A4 | Cerca del 80% de los españoles se desplaza en vehículo privado (coche o moto). La energía utilizada puede igualar o exceder la energía requerida para el funcionamiento de un edificio de oficinas (incluyendo un hospital). | ||
| A5 | La energía utilizada en el transporte de productos médicos. alimentos y suministros representa una parte significativa de la energía total utilizada en la asistencia sanitaria. | ||
| A6 | Los hospitales españoles y centros de salud producen más de 700 toneladas de residuos al día. | ||
| A7 | Los productos químicos tóxicos usados en la asistencia sanitaria han contribuido a la acumulación de Mercurio. Dioxinas y Ftalatos en nuestro medio ambiente. | ||
| A8 | En las analíticas de sangre y orina. el personal enfermero puede mostrar niveles de algún agente químico tóxico. | ||
| A9 | Algunos plastificantes que ablandan los plásticos para facilitar su uso (por ejemplo en tubos para muestras sangre) son disruptores hormonales. | ||
| A10 | El Triclosán. una sustancia antibacteriana presente. por ejemplo jabones. está siendo objeto de estudio por su posible alteración hormonal. | ||
| A11 | La comida servida de manera convencional en hospitales puede contener restos de pesticidas y herbicidas. | ||
| 2.-NPEB: Escala de comportamientos ecológicos profesional del personal enfermero. | |||
| Ítems | Por favor. lea las afirmaciones y conteste: Responda con la escala de la derecha. | ¿Con qué frecuencia lo hace? Escala Likert: 1.-Nunca 5.-Siempre | ¿Cómo de difícil o de fácil le resulta hacerlo? Escala Likert: 1.-Muy Difícil 5.-Siempre |
| B1 | En el trabajo. apago las luces conscientemente cuando no están en uso. | ||
| B2 | En el trabajo. apago los monitores del ordenador cuando no están en uso. | ||
| B3 | En el trabajo. reciclo. | ||
| B4 | En el trabajo. motivo a mis compañeros/as para reciclar. | ||
| B5 | Trabajo para reducir el uso de los agentes químicos tóxicos en el hospital (tales como el Mercurio. DEHP o Triclosán). | ||
| B6 | Hago búsquedas en la literatura o en la web sobre agentes químicos tóxicos utilizados en la asistencia sanitaria. | ||
| B7 | En el trabajo. informo a otros miembros del personal sobre agente químicos tóxicos. | ||
| B8 | En el trabajo. educo a los/as pacientes sobre riesgos de exposiciones ambientales tales como los productos químicos tóxicos o la contaminación. | ||
| B9 | En el trabajo. animo al servicio de hostelería a servir alimentos locales. | ||
| 3.-PEB: Escalas de comportamientos ecológicos personales | |||
| Ítems | Por favor. lea las afirmaciones y conteste: Responda con la escala de la derecha. | Con qué frecuencia lo hace? Escala likert: 1.-Nunca 5.-Siempre | ¿Cómo de difícil o de fácil le resulta hacerlo? Escala likert: 1.-Muy Difícil 5.-Siempre |
| C1 | En casa. calculo cuántos kWh de electricidad consumo. | ||
| C2 | Periódicamente. realizo el mantenimiento de mis tuberías para comprobar las fugas de agua y hago las reparaciones necesarias. | ||
| C3 | En casa. compro productos reciclados. | ||
| C4 | En casa. tomo decisiones en las compras teniendo en cuenta evitar la producción de residuos. | ||
| C5 | En casa. no uso pesticidas ni herbicidas. | ||
| C6 | En casa. compro productos ecológicos. | ||
| C7 | En casa. evito el uso de productos de cuidado personal que contengan productos químicos. | ||
| C8 | En casa. uso productos de limpieza respetuosos con el medioambiente. | ||
| C9 | Leo sobre temas relacionados con el medio ambiente y salud en los medios de comunicación. | ||
| C10 | Soy voluntario/a en acciones para apoyar un medio ambiente saludable (participo en Asociaciones. Organizaciones No Gubernamentales (ONG). etc). | ||
| C11 | Como enfermera/o. debato cuestiones sobre medio ambiente y salud con mis amistades y familiares. | ||
References
- Al Huraimel, K.; Alhosani, M.; Kunhabdulla, S.; Stietiya, M.H. SARS-CoV-2 in the Environment: Modes of Transmission, Early Detection and Potential Role of Pollutions. Sci. Total Environ. 2020, 744, 140946. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Wang, X.; Sarkar, B.; Ok, Y.S. The COVID-19 Pandemic Necessitates a Shift to a Plastic Circular Economy. Nat. Rev. Earth Environ. 2021, 2, 659–660. [Google Scholar] [CrossRef] [PubMed]
- Paavola, J. Health Impacts of Climate Change and Health and Social Inequalities in the UK. Environ. Health 2017, 16, 113. [Google Scholar] [CrossRef] [PubMed]
- Harris, C.; Green, S.; Ramsey, W.; Allen, K.; King, R. Sustainability in Health Care by Allocating Resources Effectively (SHARE) 1: Introducing a Series of Papers Reporting an Investigation of Disinvestment in a Local Healthcare Setting. BMC Health Serv. Res. 2017, 17, 323. [Google Scholar] [CrossRef] [PubMed]
- Persaud, D.D. Enhancing Learning, Innovation, Adaptation, and Sustainability in Health Care Organizations: The ELIAS Performance Management Framework. Health Care Manag. (Frederick) 2014, 33, 183–204. [Google Scholar] [CrossRef]
- Álvarez-Nieto, C.; Richardson, J.; Navarro-Perán, M.Á.; Tutticci, N.; Huss, N.; Elf, M.; Anåker, A.; Aronsson, J.; Baid, H.; López-Medina, I.M. Nursing Students’ Attitudes towards Climate Change and Sustainability: A Cross-Sectional Multisite Study. Nurse Educ. Today 2022, 108, 105185. [Google Scholar] [CrossRef]
- Dossey, B.M.; Rosa, W.E.; Beck, D.-M. Nursing and the Sustainable Development Goals: From Nightingale to Now. AJN Am. J. Nurs. 2019, 119, 44–49. [Google Scholar] [CrossRef]
- Kiang, K.M.; Behne, C. Delivering Environmental Sustainability in Healthcare for Future Generations: Time to Clean up Our Own Cubby House. J. Paediatr. Child Health 2021, 57, 1767–1774. [Google Scholar] [CrossRef]
- Wyssusek, K.H.; Keys, M.T.; van Zundert, A.A.J. Operating Room Greening Initiatives–the Old, the New, and the Way Forward: A Narrative Review. Waste Manag. Res. 2019, 37, 3–19. [Google Scholar] [CrossRef]
- International Council of Nurses International Council of Nurses Calls for Increased Nursing Leadership to Combat Effects of Climate Change on Health. Available online: https://www.icn.ch/system/files/2021-10/ICN_Code-of-Ethics_EN_Web_0.pdf (accessed on 21 April 2019).
- Nhamo, L.; Ndlela, B. Nexus Planning as a Pathway towards Sustainable Environmental and Human Health Post COVID-19. Environ. Res. 2021, 192, 110376. [Google Scholar] [CrossRef]
- Perez, H.L.R. Sostenibilidad ambiental de la práctica clínica, una nueva visión para enfermería. Acc Cietna 2020, 7, 116–125. [Google Scholar] [CrossRef]
- Osingada, C.P.; Porta, C.M. Nursing and Sustainable Development Goals (SDGs) in a COVID-19 World: The State of the Science and a Call for Nursing to Lead. Public Health Nurs. 2020, 37, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Kitt-Lewis, E.; Adam, M.; Buckland, P.; Clark, D.; Hockenberry, K.; Jankura, D.; Knott, J. Creating a Generation of Sustainable Nurses: Sustainability Efforts in Nursing Education. Nurs. Clin. N. Am. 2020, 55, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lilienfeld, E.; Nicholas, P.K.; Breakey, S.; Corless, I.B. Addressing Climate Change through a Nursing Lens within the Framework of the United Nations Sustainable Development Goals. Nurs. Outlook 2018, 66, 482–494. [Google Scholar] [CrossRef] [PubMed]
- United Nations Open Working Group Proposal for Sustainable Development Goals. Available online: https://sustainabledevelopment.un.org/focussdgs.html (accessed on 12 April 2021).
- Capolongo, S.; Bottero, M.C.; Lettieri, E.; Buffoli, M.; Bellagarda, A.; Birocchi, M.; Cavagliato, E.; Dervishaj, A.; di Noia, M.; Gherardi, G.; et al. Healthcare Sustainability Challenge. In Improving Sustainability During Hospital Design and Operation: A Multidisciplinary Evaluation Tool; Capolongo, S., Bottero, M.C., Buffoli, M., Lettieri, E., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 1–9. ISBN 978-3-319-14036-0. [Google Scholar]
- Sarkodie, S.A.; Owusu, P.A. Impact of COVID-19 Pandemic on Waste Management. Environ. Dev. Sustain. 2021, 23, 7951–7960. [Google Scholar] [CrossRef]
- Baker, N.; Bromley-Dulfano, R.; Chan, J.; Gupta, A.; Herman, L.; Jain, N.; Taylor, A.L.; Lu, J.; Pannu, J.; Patel, L.; et al. COVID-19 Solutions Are Climate Solutions: Lessons from Reusable Gowns. Front. Public Health 2020, 8, 590275. [Google Scholar] [CrossRef]
- Gök, N.D.; Firat Kiliç, H. Environmental Awareness and Sensitivity of Nursing Students. Nurse Educ. Today 2021, 101, 104882. [Google Scholar] [CrossRef]
- Febles, M. Sobre la Necesidad de la Formación de una Conciencia Ambiental; Facultad de Psicología, Universidad de La Habana: Havana, Cuba, 2004. [Google Scholar]
- International Council of Nurses. The Icn Code of Ethics for Nurses; International Council of Nurses: Geneva, Switzerland, 2021; p. 32. [Google Scholar]
- Goodman, B. Developing the Concept of Sustainability in Nursing. Nurs. Philos. 2016, 17, 298–306. [Google Scholar] [CrossRef]
- Leonard, A.; Power, N.; Mayet, S.; Coetzee, M.; North, N. Engaging Nurses in Research Awareness Using a New Style of Hospital Journal Club—A Descriptive Evaluation. Nurse Educ. Today 2022, 108, 105123. [Google Scholar] [CrossRef]
- Workman, M.; Darch, G.; Dooley, K.; Lomax, G.; Maltby, J.; Pollitt, H. Climate Policy Decision Making in Contexts of Deep Uncertainty-from Optimisation to Robustness. Environ. Sci. Policy 2021, 120, 127–137. [Google Scholar] [CrossRef]
- Schwerdtle, P.N.; Maxwell, J.; Horton, G.; Bonnamy, J. 12 Tips for Teaching Environmental Sustainability to Health Professionals. Med. Teach. 2020, 42, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Rosa, W.E.; Catton, H.; Davidson, P.M.; Hannaway, C.J.; Iro, E.; Klopper, H.C.; Madigan, E.A.; McConville, F.E.; Stilwell, B.; Kurth, A.E. Nurses and Midwives as Global Partners to Achieve the Sustainable Development Goals in the Anthropocene. J. Nurs. Scholarsh. 2021, 53, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Pollitt, P.; Sattler, B.; Butterfield, P.; Anderko, L.; Brody, C.; Mood, L.; Huffling, K.; Schenk, E.; Cook, K. Environmental Nursing: Leaders Reflect on the 50th Anniversary of Earth Day. Public Health Nurs. 2020, 37, 614–625. [Google Scholar] [CrossRef] [PubMed]
- Orts-Cortés, M.I.; Moreno-Casbas, T.; Squires, A.; Fuentelsaz-Gallego, C.; Maciá-Soler, L.; González-María, E. Content Validity of the Spanish Version of the Practice Environment Scale of the Nursing Work Index. Appl. Nurs. Res. 2013, 26, e5–e9. [Google Scholar] [CrossRef] [PubMed]
- Schenk, E.C.; Cook, C.; Demorest, S.; Burduli, E. CHANT: Climate, Health, and Nursing Tool: Item Development and Exploratory Factor Analysis. Annu. Rev. Nurs. Res. 2019, 38, 97–112. [Google Scholar] [CrossRef]
- Schenk, E.; Butterfield, P.; Postma, J.; Barbosa-Leiker, C.; Corbett, C. Creating the Nurses’ Environmental Awareness Tool (NEAT). Workplace Health Saf. 2015, 63, 381–391. [Google Scholar] [CrossRef]
- Schenk, E.C.; Cook, C.; Demorest, S.; Burduli, E. Climate, Health, and Nursing Tool (CHANT): Initial Survey Results. Public Health Nurs. 2021, 38, 152–159. [Google Scholar] [CrossRef]
- Fuentelsaz-Gallego, C.; Moreno-Casbas, M.T.; González-María, E. Validation of the Spanish Version of the Questionnaire Practice Environment Scale of the Nursing Work Index. Int. J. Nurs. Stud. 2013, 50, 274–280. [Google Scholar] [CrossRef]
- García, O.; Lin, A. Extending Understandings of Bilingual and Multilingual Education. In Bilingual and Multilingual Education. Encyclopedia of Language and Education, 3rd ed.; García, O., Lin, A.M.Y., May, S., Eds.; Springer International Publishing: Cham, Switzerland; New York, NY, USA, 2017; pp. 1–20. ISBN 978-3-319-02257-4. [Google Scholar]
- Wolcott, M.; Lobczowski, N. Using Cognitive Interviews and Think-Aloud Protocols to Understand Thought Processes. Curr. Pharm. Teach. Learn. 2020, 13, 181–188. [Google Scholar] [CrossRef]
- Bolarinwa, O. Principles and Methods of Validity and Reliability Testing of Questionnaires Used in Social and Health Science Researches. Niger. Postgrad. Med. J. 2016, 22, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Schenk, E.; Corbett, C.; Barbosa-Leiker, C.; Postma, J.; Butterfield, P. Psychometric Properties of the Nurses’ Environmental Awareness Tool. J. Nurs. Meas. 2016, 24, 55E–71E. [Google Scholar] [CrossRef]
- Tucker, L.R.; Lewis, C. A Reliability Coefficient for Maximum Likelihood Factor Analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications; Sage Publications: Newbury Park, CA, USA, 2021; ISBN 1-5443-7935-8. [Google Scholar]
- Pérez, M.I.; Hervada Vidal, X.; Naveira-Barbeito, G.; Silva, L.C.; Fariñas, H.; Vázquez, E.; Bacallao, J.; Mujica, O. El Programa Epidat: Usos y Perspectivas. Rev. Panam. Salud Publica-Pan Am. J. Public Health Rev. Panam Salud Publica 2010, 27, 80–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauffer, A.; Solé, L.; Bernstein, S.; Lopes, M.H.; Francisconi, C.F. Cómo Minimizar Errores al Realizar La Adaptación Transcultural y la Validación de los Cuestionarios Sobre Calidad de Vida: Aspectos Prácticos. Rev. Gastroenterol. México 2013, 78, 159–176. [Google Scholar] [CrossRef] [Green Version]
- Sousa, V.; Rojjanasrirat, W. Translation, Adaptation and Validation of Instruments or Scales for Use in Cross-Cultural Health Care Research: A Clear and User-Friendly Guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- Rowen, D.; Carlton, J.; Elliott, J. PROM Validation Using Paper-Based or Online Surveys: Data Collection Methods Affect the Sociodemographic and Health Profile of the Sample. Value Health 2019, 22, 845–850. [Google Scholar] [CrossRef]
- Çabuk, B.; Karacaglu, C. Investigation of University Students’ Environmental Sensitivity. Ank. Univ. J. Fac. Educ. Sci. 2003, 36, 189–198. [Google Scholar]
- Fox, J. The R Commander: A Basic-Statistics Graphical User Interface to R. J. Stat. Soft. 2005, 14, 1–42. [Google Scholar] [CrossRef] [Green Version]
- María Isabel, O.-C.; Moreno-Casbas, T.; Squires, A.; Fuentelsaz-Gallego, C.; Maciá-Soler, L.; González-María, E. Validation of a Spanish Version of the Practice Environment Scale of the Nursing Work Index in the Colombian Context. Hisp. Health Care Int. 2014, 12, 34–42. [Google Scholar]
- López-Aguado, M.; Gutiérrez-Provecho, L. Cómo realizar e interpretar un análisis factorial exploratorio utilizando SPSS. REIRE 2019, 12, 1–14. [Google Scholar] [CrossRef]
- Shakil, M.H.; Munim, Z.H.; Tasnia, M.; Sarowar, S. COVID-19 and the Environment: A Critical Review and Research Agenda. Sci. Total Environ. 2020, 745, 141022. [Google Scholar] [CrossRef] [PubMed]
- Rosa, W.E.; Fitzgerald, M.; Davis, S.; Farley, J.E.; Khanyola, J.; Kwong, J.; Moreland, P.J.; Rogers, M.; Sibanda, B.; Turale, S. Leveraging Nurse Practitioner Capacities to Achieve Global Health for All: COVID-19 and Beyond. Int. Nurs. Rev. 2020, 67, 554–559. [Google Scholar] [CrossRef] [PubMed]
- United Nations Educational, Scientific and Cultural Organization (UNESCO). Anthropocene: The Vital Challenges of a Scientific Debate. Available online: https://en.unesco.org/courier/2018-2/anthropocene-vital-challenges-scientific-debate (accessed on 20 October 2019).
- Cruz, J.P.; Alshammari, F.; Felicilda-Reynaldo, R. Predictors of Saudi Nursing Students’ Attitudes towards Environment and Sustainability in Health Care. Int. Nurs. Rev. 2018, 65, 408–416. [Google Scholar] [CrossRef] [PubMed]
- González, A.G.; Sanz-Calcedo, J.; Salgado, D. A Quantitative Analysis of Final Energy Consumption in Hospitals in Spain. Sustain. Cities Soc. 2017, 36, 169–175. [Google Scholar] [CrossRef]
- Fitriani, I.; Sangadji, S.; Kristiawan, S. Energy Efficiency Evaluation of Hospital Building Office. J. Phys. Conf. Ser. 2017, 795, 012067. [Google Scholar] [CrossRef] [Green Version]
- Haines, A.; Dora, C. How the Low Carbon Economy Can Improve Health. BMJ 2012, 344, e1018. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Pilot Project (N = 63) | Final Sample (N = 376) | |
|---|---|---|
| Age | 40.76 (13.78) | 37.7 (0.62) |
| Gender | ||
| Female | 39 (61.9%) | 275 (73.1%) |
| Male | 24 (38.1%) | 101 (26.9%) |
| Non-binary | 0 | 0 |
| Working experience (years in the field) | ||
| More than 20 years | 29 (46.0%) | 142 (37.8%) |
| Between 11 and 20 years | 9 (14.3%) | 65 (17.3%) |
| Between 10 and 5 years | 3 (4.8%) | 51 (13.5%) |
| Less than 5 years | 22 (34.9%) | 118 (31.4%) |
| Occupation | ||
| Nursing Assistant | 4 (6.3%) | 23 (6.1%) |
| Nursing of Assistant Student | 1 (1.6%) | 1 (0.3%) |
| Nurse with Certificate from University | 41 (65.1%) | 267 (71.0%) |
| Nursing Student to Obtain University Certificate | 15 (23.8%) | 72 (19.1%) |
| Nursing Specialist Students | 2 (3.2%) | 13 (3.5%) |
| Workplace | ||
| Local Hospital | 28 (44.4%) | 139 (37.0%) |
| Local Primary Health Care | 10 (16.0%) | 68 (18.1%) |
| Regional Hospital | 14 (22.2%) | 124 (33.0%) |
| Regional Primary Health Care | 2 (3.2%) | 12 (3.2%) |
| Socio-Sanitary (i.e., hospice) | 5 (7.9%) | 14 (3.7%) |
| Others | 4 (6.3%) | 19 (5.0%) |
| Center Financial status | ||
| Public | 48 (76.2%) | 330 (87.9%) |
| Private | 8 (12.7%) | 20 (5.2%) |
| In Collaboration with Public and Private entities | 7 (11.1%) | 26 (6.9%) |
| Work shift | ||
| Only Morning | 30 (47.6%) | 185 (49.2%) |
| Only Afternoons | 4 (6.3%) | 18 (4.8%) |
| Only Nights | 2 (3.2%) | 11 (2.9%) |
| Rotating Shift (switch between other shifts) | 24 (38.1%) | 160 (42.6%) |
| Others | 3 (4.8%) | 2 (0.5%) |
| NAS-es SCALE | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Validation EFA | |||||||||
| NAS-e | Awareness | Health | |||||||
| Items | Loadings | ||||||||
| Factor | Pattern | Structure | Pattern | Structure | |||||
| 1 | 2 | 1 | 2 | 1 | 2 | 1 | 2 | ||
| A1 | −0.119 | 1.0 | 0.565 | 0.995 | 0.979 | −0.176 | 0.869 | 0.431 | |
| A2 | 0.154 | 0.659 | 0.575 | 0.757 | 0.957 | −0.128 | 0.877 | 0.466 | |
| A3 | 0.457 | 0.119 | 0.533 | 0.410 | 0.586 | 0.186 | 0.701 | 0.549 | |
| A4 | 0.614 | 0.008 | 0.619 | 0.400 | 0.368 | 0.396 | 0.614 | 0.625 | |
| A5 | 0.585 | 0.263 | 0.752 | 0.636 | 0.607 | 0.231 | 0.751 | 0.608 | |
| A6 | 0.263 | 0.149 | 0.653 | 0.505 | 0.351 | 0.386 | 0.590 | 0.603 | |
| A7 | 0.767 | −0.002 | 0.766 | 0.487 | 0.210 | 0.537 | 0.543 | 0.667 | |
| A8 | 0.661 | −0.010 | 0.655 | 0.412 | 0.028 | 0.602 | 0.401 | 0.619 | |
| A9 | 0.720 | −0.071 | 0.675 | 0.389 | 0.008 | 0.688 | 0.436 | 0.693 | |
| A10 | 0.608 | 0.014 | 0.617 | 0.403 | −0.036 | 0.832 | 0.480 | 0.809 | |
| A11 | 0.601 | −0.024 | 0.585 | 0.359 | −0.159 | 0.740 | 0.300 | 0.641 | |
| Kaiser–Meyer–Olkin measure of sampling adequacy | 0.879 | 0.892 | |||||||
| Bartlett’s Sphericity Test | Statistic | 1217.385 | 1404.342 | ||||||
| p-value | <0.001 | <0.001 | |||||||
| Cronbach’s Alpha | 0.886 | 0.891 | |||||||
| NAS-es SCALE | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Validation CFA | |||||||||
| NAS-es | Awareness | Health | |||||||
| Items | Loadings | ||||||||
| Factor | Pattern | Structure | Pattern | Structure | |||||
| 1 | 2 | 1 | 2 | 1 | 2 | 1 | 2 | ||
| A1 | 0.979 | −0.176 | 0.869 | 0.431 | 0.944 | −0.155 | 0.853 | 0.401 | |
| A2 | 0.957 | −0.128 | 0.877 | 0.466 | 0.940 | −0.131 | 0.862 | 0.422 | |
| A3 | 0.586 | 0.186 | 0.701 | 0.549 | 0.621 | 0.134 | 0.699 | 0.499 | |
| A4 | 0.368 | 0.396 | 0.614 | 0.625 | 0.460 | 0.272 | 0.621 | 0.543 | |
| A5 | 0.607 | 0.231 | 0.751 | 0.608 | 0.648 | 0.187 | 0.757 | 0.568 | |
| A6 | 0.351 | 0.386 | 0.590 | 0.603 | 0.291 | 0.419 | 0.538 | 0.590 | |
| A7 | 0.210 | 0.537 | 0.543 | 0.667 | 0.163 | 0.535 | 0.478 | 0.631 | |
| A8 | 0.028 | 0.602 | 0.401 | 0.619 | −0.013 | 0.638 | 0.363 | 0.631 | |
| A9 | 0.008 | 0.688 | 0.436 | 0.693 | 0.042 | 0.681 | 0.443 | 0.706 | |
| A10 | −0.036 | 0.832 | 0.480 | 0.809 | −0.016 | 0.774 | 0.440 | 0.765 | |
| A11 | −0.159 | 0.740 | 0.300 | 0.641 | −0.141 | 0.743 | 0.296 | 0.660 | |
| Comparative Fit Index (CFI) | 0.98 | 0.98 | |||||||
| RMSEA | Statistic | 0.049 | 0.068 | ||||||
| p-value | 0.48 | 0.123 | |||||||
| Cronbach’s Alpha | 0.891 | 0.886 | |||||||
| NPEB-es SCALE | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Validation EFA | |||||||||||
| Behavior | Difficulty | ||||||||||
| Items | Loadings | ||||||||||
| Factor | Pattern | Structure | Pattern | Structure | |||||||
| 1 | 2 | 1 | 2 | 1 | 2 | 3 | 1 | 2 | 3 | ||
| B1 | 0.113 | 0.408 | 0.338 | 0.471 | 0.109 | 0.445 | 0.052 | 0.297 | 0.502 | 0.258 | |
| B2 | 0.247 | 0.206 | 0.361 | 0.342 | −0.045 | 10.0 | −0.129 | 0.268 | 0.989 | 0.201 | |
| B3 | −0.004 | 0.677 | 0.369 | 0.675 | 0.104 | 0.109 | −0.234 | 0.022 | 0.068 | −0.144 | |
| B4 | −0.046 | 0.881 | 0.440 | 0.855 | 0.048 | 0.062 | 0.796 | 0.482 | 0.348 | 0.842 | |
| B5 | 0.552 | 0.226 | 0.677 | 0.530 | 0.449 | 0.027 | 0.258 | 0.592 | 0.276 | 0.499 | |
| B6 | 0.769 | −0.075 | 0.728 | 0.349 | 0.722 | −0.010 | −0.200 | 0.615 | 0.184 | 0.169 | |
| B7 | 0.805 | −0.004 | 0.803 | 0.439 | 0.837 | −0.032 | −0.088 | 0.780 | 0.241 | 0.333 | |
| B8 | 0.593 | −0.007 | 0.589 | 0.320 | 0.665 | 0.060 | −0.065 | 0.653 | 0.278 | 0.298 | |
| B9 | 0.350 | 0.055 | 0.380 | 0.248 | 0.458 | 0.023 | 0.146 | 0.542 | 0.238 | 0.390 | |
| Kaiser–Meyer–Olkin measure of sampling adequacy | 0.826 | 0.774 | |||||||||
| Bartlett’s Sphericity Test | Statistic | 600.988 | 481.724 | ||||||||
| p-value | <0.001 | <0.001 | |||||||||
| Cronbach’s Alpha | 0.799 | 0.730 | |||||||||
| NPEB-es SCALE | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Validation CFA | |||||||||
| Behavior | Difficulty | ||||||||
| Items | Loadings | ||||||||
| Factor | Pattern | Structure | Pattern | Structure | |||||
| 1 | 2 | 1 | 2 | 1 | 2 | 1 | 2 | ||
| B1 | 0.131 | 0.350 | 0.300 | 0.413 | 0.074 | 0.580 | 0.328 | 0.612 | |
| B2 | 0.271 | 0.233 | 0.384 | 0.364 | −0.009 | 0.776 | 0.331 | 0.772 | |
| B3 | −0.085 | 0.639 | 0.224 | 0.598 | −0.039 | 0.194 | 0.046 | 0.177 | |
| B4 | 0.021 | 0.809 | 0.412 | 0.820 | 0.370 | 0.194 | 0.455 | 0.356 | |
| B5 | 0.504 | 0.222 | 0.611 | 0.466 | 0.520 | 0.082 | 0.556 | 0.310 | |
| B6 | 0.797 | −0.080 | 0.758 | 0.305 | 0.679 | −0.067 | 0.649 | 0.231 | |
| B7 | 0.812 | −0.054 | 0.785 | 0.338 | 0.830 | −0.089 | 0.791 | 0.275 | |
| B8 | 0.594 | 0.006 | 0.597 | 0.293 | 0.682 | −0.013 | 0.676 | 0.286 | |
| B9 | 0.388 | 0.059 | 0.417 | 0.246 | 0.484 | 0.051 | 0.507 | 0.264 | |
| Comparative Fit Index (CFI) | 0.966 | 0.953 | |||||||
| RMSEA | Statistic | 0.061 | 0.06 | ||||||
| p-value | 0.259 | 0.219 | |||||||
| Cronbach’s Alpha | 0.780 | 0.744 | |||||||
| PEB-es SCALE | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Validation EFA | |||||||||||||
| Behavior | Difficulty | ||||||||||||
| Items | Loadings | ||||||||||||
| Factor | Pattern | Structure | Pattern | Structure | |||||||||
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | ||
| C1 | −0.005 | −0.037 | 1.0 | 0.413 | 0.364 | 0.999 | 0.077 | 0.122 | 0.487 | 0.351 | 0.272 | 0.547 | |
| C2 | 0.012 | 0.120 | 0.450 | 0.286 | 0.307 | 0.503 | 0.050 | −0.037 | 0.879 | 0.400 | 0.184 | 0.892 | |
| C3 | 0.518 | 0.297 | −0.007 | 0.709 | 0.633 | 0.337 | 0.702 | −0.041 | 0.026 | 0.690 | 0.360 | 0.312 | |
| C4 | 0.368 | 0.430 | 0.021 | 0.658 | 0.679 | 0.352 | 0.708 | −0.010 | 0.070 | 0.732 | 0.404 | 0.366 | |
| C5 | 0.274 | 0.090 | 0.050 | 0.355 | 0.289 | 0.205 | 0.321 | 0.081 | 0.019 | 0.375 | 0.266 | 0.172 | |
| C6 | 0.668 | −0.001 | −0.071 | 0.637 | 0.407 | 0.219 | 0.398 | 0.354 | −0.079 | 0.565 | 0.561 | 0.167 | |
| C7 | 0.868 | −0.125 | 0.052 | 0.809 | 0.463 | 0.380 | −0.131 | 10.0 | 0.100 | 0.499 | 0.993 | 0.274 | |
| C8 | 0.767 | −0.045 | 0.020 | 0.747 | 0.464 | 0.336 | 0.392 | 0.499 | −0.118 | 0.623 | 0.694 | 0.156 | |
| C9 | 0.052 | 0.704 | 0.030 | 0.525 | 0.750 | 0.333 | 0.457 | −0.030 | 0.108 | 0.485 | 0.251 | 0.293 | |
| C10 | 0.266 | 0.272 | −0.050 | 0.423 | 0.427 | 0.174 | 0.311 | 0.118 | 0.008 | 0.381 | 0.295 | 0.165 | |
| C11 | −0.129 | 0.823 | 0.029 | 0.421 | 0.751 | 0.301 | 0.079 | 0.067 | 0.019 | 0.125 | 0.115 | 0.067 | |
| Kaiser–Meyer–Olkin measure of sampling adequacy | 0.861 | 0.811 | |||||||||||
| Bartlett’s Sphericity Test | Statistic | 913.469 | 671.674 | ||||||||||
| p-value | <0.001 | <0.001 | |||||||||||
| Cronbach’s Alpha | 0.831 | 0.783 | |||||||||||
| PEB-es SCALE | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Validation CFA | |||||||||||
| Behavior | Difficulty | ||||||||||
| Items | Loadings | ||||||||||
| Factor | Pattern | Structure | Pattern | Structure | |||||||
| 1 | 2 | 1 | 2 | 1 | 2 | 3 | 1 | 2 | 3 | ||
| C1 | 0.191 | 0.324 | 0.405 | 0.450 | 0.021 | −0.035 | 0.699 | 0.270 | 0.336 | 0.689 | |
| C2 | 0.115 | 0.273 | 0.295 | 0.349 | −0.020 | 0.083 | 0.644 | 0.278 | 0.401 | 0.679 | |
| C3 | 0.363 | 0.401 | 0.628 | 0.641 | −0.033 | 0.704 | 0.011 | 0.387 | 0.690 | 0.359 | |
| C4 | 0.194 | 0.587 | 0.581 | 0.714 | 0.025 | 0.718 | 0.020 | 0.457 | 0.743 | 0.398 | |
| C5 | 0.248 | 0.153 | 0.349 | 0.317 | 0.169 | 0.200 | 0.022 | 0.295 | 0.311 | 0.189 | |
| C6 | 0.550 | 0.102 | 0.617 | 0.465 | 0.367 | 0.361 | −0.072 | 0.552 | 0.541 | 0.255 | |
| C7 | 0.878 | −0.105 | 0.808 | 0.474 | 0.990 | −0.148 | 0.068 | 0.928 | 0.471 | 0.374 | |
| C8 | 0.718 | 0.030 | 0.738 | 0.504 | 0.545 | 0.317 | −0.081 | 0.701 | 0.597 | 0.292 | |
| C9 | −0.013 | 0.752 | 0.483 | 0.744 | 0.000 | 0.374 | 0.236 | 0.312 | 0.495 | 0.428 | |
| C10 | 0.233 | 0.276 | 0.414 | 0.429 | 0.143 | 0.202 | 0.179 | 0.331 | 0.378 | 0.337 | |
| C11 | −0.116 | 0.756 | 0.383 | 0.679 | 0.013 | 0.009 | 0.025 | 0.028 | 0.029 | 0.035 | |
| Comparative Fit Index (CFI) | 0.943 | 0.94 | |||||||||
| RMSEA | Statistic | 0.066 | 0.07 | ||||||||
| p-value | 0.06 | 0.055 | |||||||||
| Cronbach’s Alpha | 0.825 | 0.774 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luque-Alcaraz, O.M.; Gomera, A.; Ruíz, Á.; Aparicio-Martinez, P.; Vaquero-Abellan, M. Validation of the Spanish Version of the Questionnaire on Environmental Awareness in Nursing (NEAT). Healthcare 2022, 10, 1420. https://doi.org/10.3390/healthcare10081420
Luque-Alcaraz OM, Gomera A, Ruíz Á, Aparicio-Martinez P, Vaquero-Abellan M. Validation of the Spanish Version of the Questionnaire on Environmental Awareness in Nursing (NEAT). Healthcare. 2022; 10(8):1420. https://doi.org/10.3390/healthcare10081420
Chicago/Turabian StyleLuque-Alcaraz, Olga María, Antonio Gomera, África Ruíz, Pilar Aparicio-Martinez, and Manuel Vaquero-Abellan. 2022. "Validation of the Spanish Version of the Questionnaire on Environmental Awareness in Nursing (NEAT)" Healthcare 10, no. 8: 1420. https://doi.org/10.3390/healthcare10081420
APA StyleLuque-Alcaraz, O. M., Gomera, A., Ruíz, Á., Aparicio-Martinez, P., & Vaquero-Abellan, M. (2022). Validation of the Spanish Version of the Questionnaire on Environmental Awareness in Nursing (NEAT). Healthcare, 10(8), 1420. https://doi.org/10.3390/healthcare10081420