
A Comparison of Univariate and Multivariate Forecasting Models Predicting Emergency Department Patient Arrivals during the COVID-19 Pandemic

 , ,
, ,
Abstract
:1. Introduction
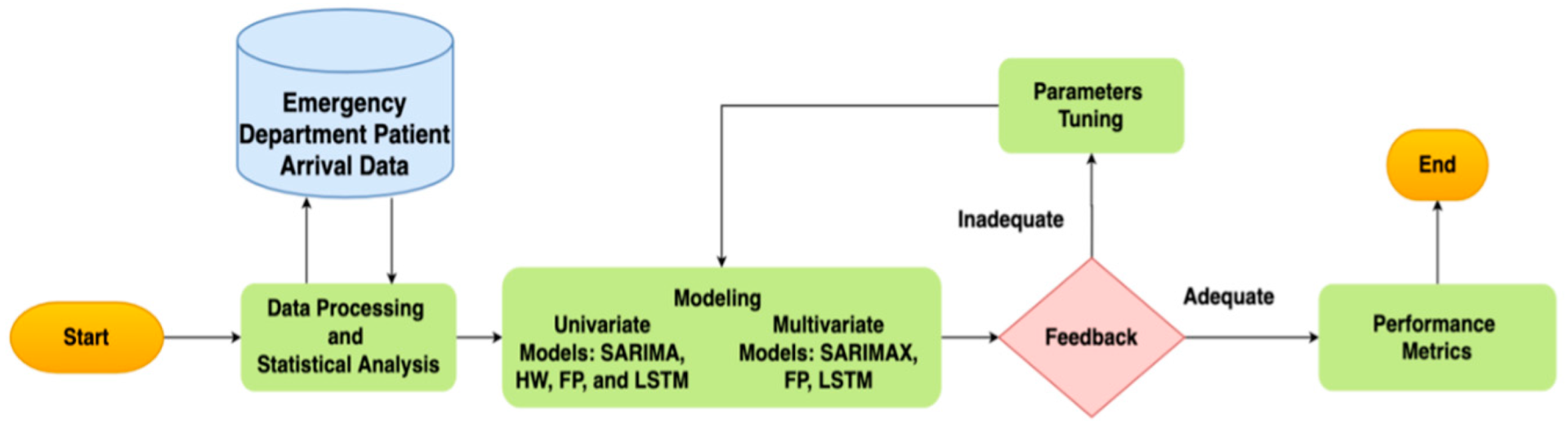
2. Materials and Methods
2.1. Study Design, Setting, and Selection of Participants
2.2. Data Processing and Statistical Analysis
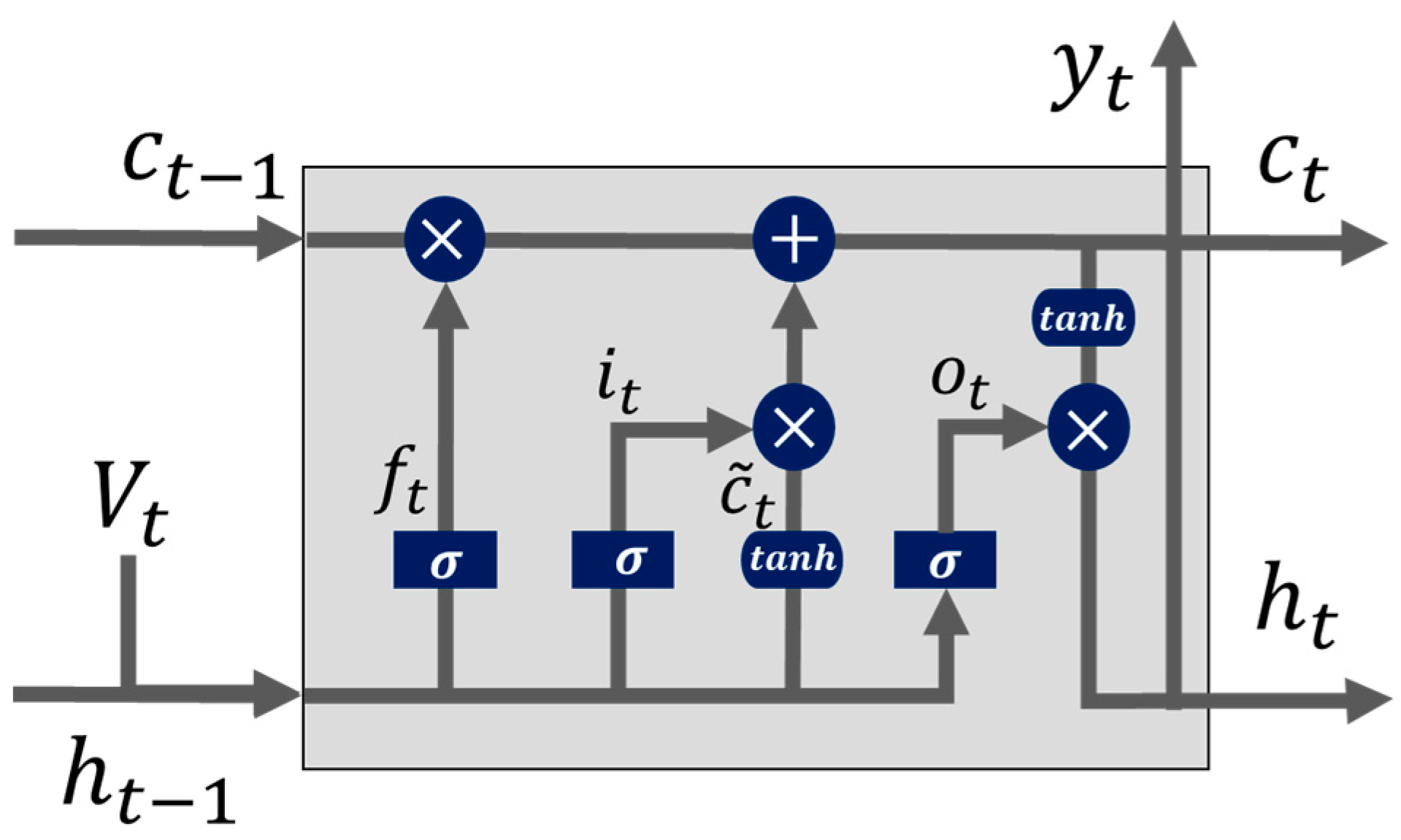
2.3. Forecasting Models
2.4. Model Evaluation Criteria
3. Results
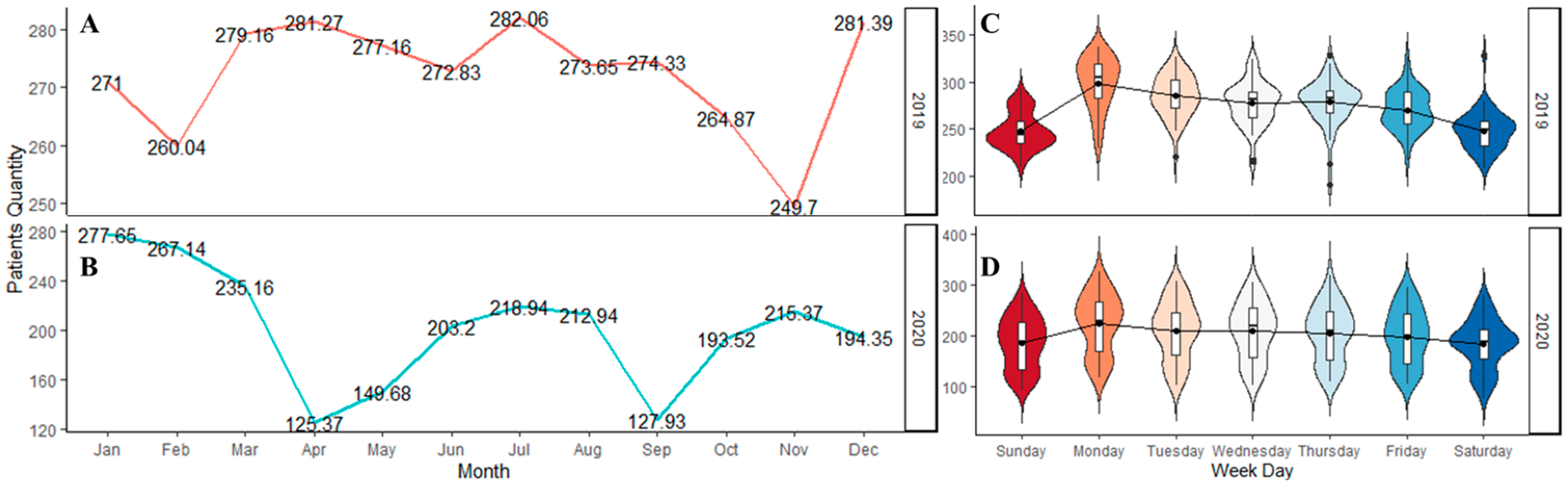
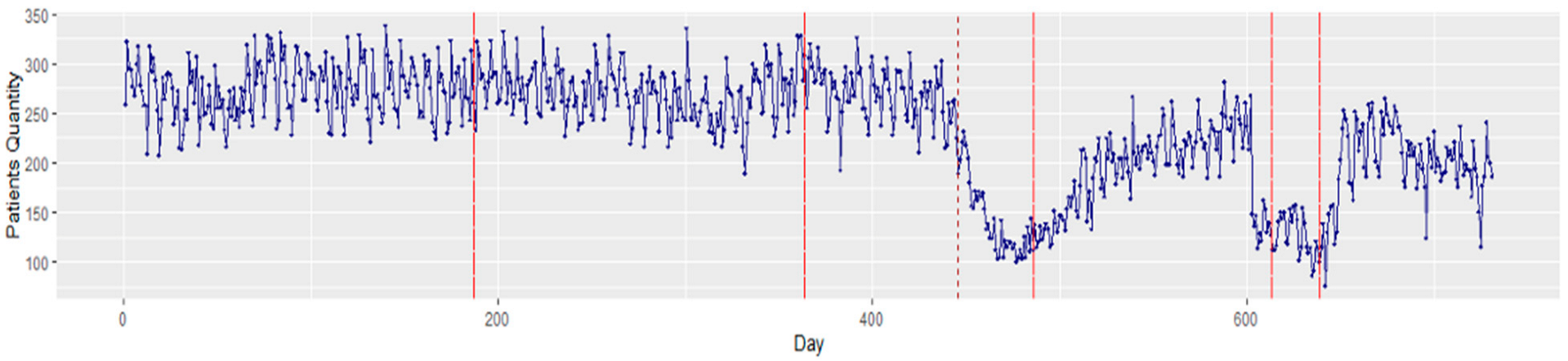
3.1. Statistical Data Analysis
3.2. Forecasting Models
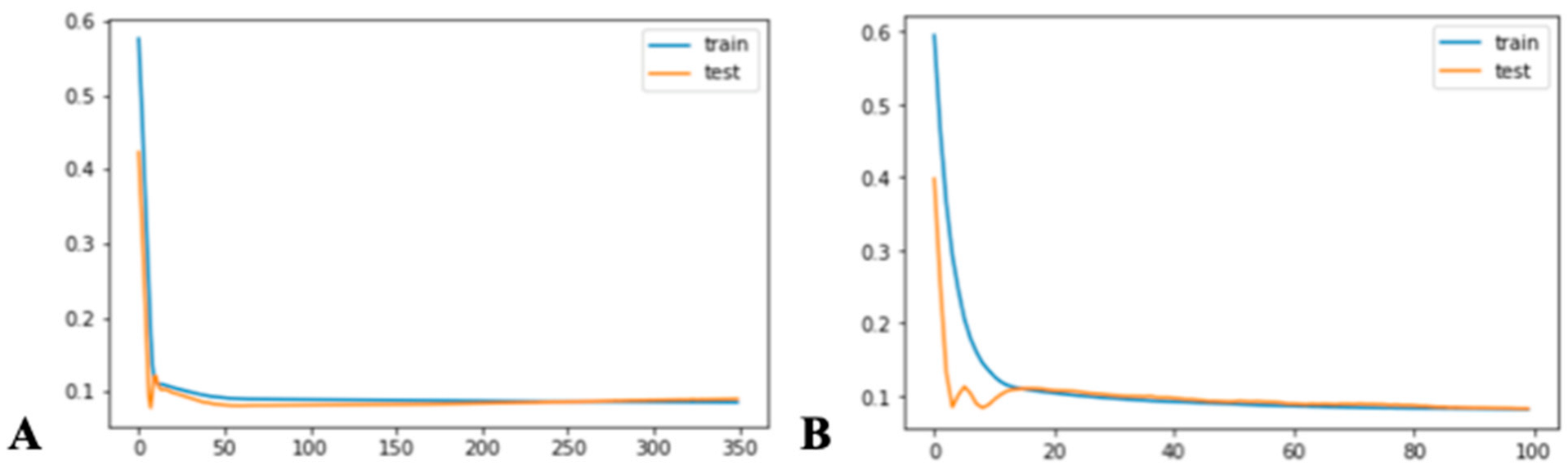
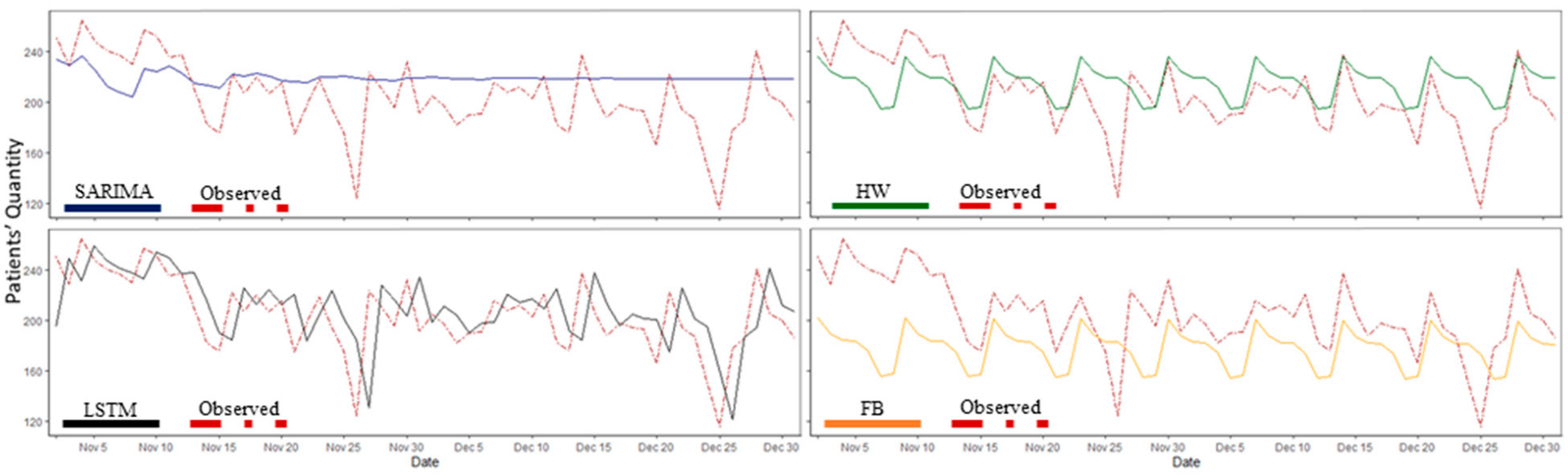
3.2.1. Univariate Models: SARIMA, FP, HW, and LSTM
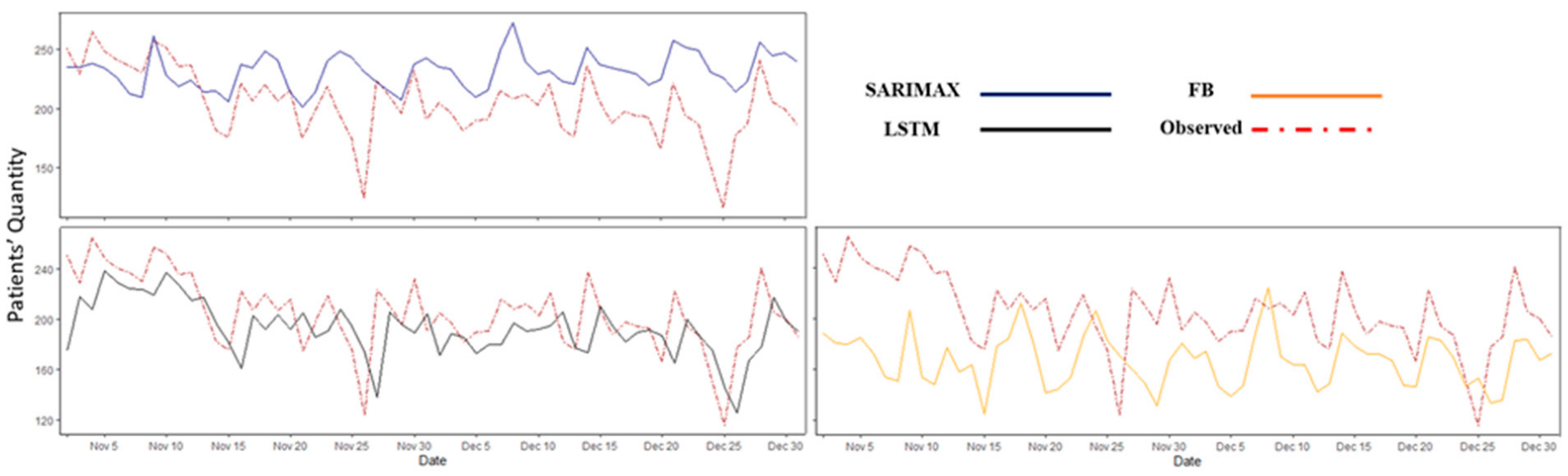
3.2.2. Multivariable Models: SARIMAX, FP, and LSTM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Forecasting Modeling Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Estimated Value | Standard Error | p-Value |
|---|---|---|---|
| Intercept | 0.000 | 0.002 | 0.940 |
| ar.L1 | −0.644 | 0.226 | 0.004 * |
| ar.L2 | 0.216 | 0.056 | 0.000 * |
| ma.L1 | 0.095 | 0.225 | 0.672 |
| ma.L2 | −0.662 | 0.159 | 0.000 * |
| ar.S.L7 | 0.999 | 0.001 | 0.000 * |
| ma.S.L7 | −0.857 | 0.039 | 0.000 * |
| ma.S.L14 | −0.114 | 0.040 | 0.004 * |
| Parameter | Estimated Value | Standard Error | p-Value |
|---|---|---|---|
| Lockdown | −104.845 | 8.061 | 0.000 * |
| Humidity | 0.078 | 0.089 | 0.382 |
| Max. Temp | −0.761 | 0.570 | 0.182 |
| Avg. Temp | 2.131 | 0.930 | 0.022 * |
| Min. Temp | −0.421 | 0.506 | 0.405 |
| Precipitation | 0.174 | 0.311 | 0.577 |
| ar.L1 | 1.490 | 0.035 | 0.000 * |
| ar.L2 | −0.493 | 0.031 | 0.000 * |
| ma.L1 | −0.999 | 0.280 | 0.000 * |
| ar.S.L7 | 0.418 | 0.039 | 0.000 * |
| ar.S.L14 | 0.173 | 0.040 | 0.000 * |
References
- Woodruff, A.; Frakt, A.B. COVID-19 Pandemic Leads to Decrease in Emergency Department Wait Times. Proc. JAMA Health Forum 2020, 1, e201172. [Google Scholar] [CrossRef]
- Dugas, A.F.; Morton, M.; Beard, R.; Pines, J.M.; Bayram, J.D.; Hsieh, Y.-H.; Kelen, G.; Uscher-Pines, L.; Jeng, K.; Cole, G. Interventions to mitigate emergency department and hospital crowding during an infectious respiratory disease outbreak: Results from an expert panel. PLoS Curr. 2013, 5, 23856917. [Google Scholar] [CrossRef]
- Sullivan, C.; Staib, A.; Khanna, S.; Good, N.M.; Boyle, J.; Cattell, R.; Heiniger, L.; Griffin, B.R.; Bell, A.J.; Lind, J. The National Emergency Access Target (NEAT) and the 4-hour rule: Time to review the target. Med. J. Aust. 2016, 204, 354. [Google Scholar] [CrossRef]
- Carr, B.G.; Kaye, A.J.; Wiebe, D.J.; Gracias, V.H.; Schwab, C.W.; Reilly, P.M. Emergency department length of stay: A major risk factor for pneumonia in intubated blunt trauma patients. J. Trauma Acute Care Surg. 2007, 63, 9–12. [Google Scholar] [CrossRef] [Green Version]
- Robertson, J.J.; Long, B. Suffering in silence: Medical error and its impact on health care providers. J. Emerg. Med. 2018, 54, 402–409. [Google Scholar] [CrossRef]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare staff wellbeing, burnout, and patient safety: A systematic review. PLoS ONE 2016, 11, e0159015. [Google Scholar]
- Gul, M.; Celik, E. An exhaustive review and analysis on applications of statistical forecasting in hospital emergency departments. Health Syst. 2020, 9, 263–284. [Google Scholar] [CrossRef]
- Marcilio, I.; Hajat, S.; Gouveia, N. Forecasting daily emergency department visits using calendar variables and ambient temperature readings. Acad. Emerg. Med. 2013, 20, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Batal, H.; Tench, J.; McMillan, S.; Adams, J.; Mehler, P.S. Predicting patient visits to an urgent care clinic using calendar variables. Acad. Emerg. Med. 2001, 8, 48–53. [Google Scholar] [CrossRef]
- Giannakeas, V.; Bhatia, D.; Warkentin, M.T.; Bogoch, I.; Stall, N.M. Estimating the maximum daily number of incident COVID-19 cases manageable by a healthcare system. MedRxiv 2020. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, J.; Tao, M.; Shu, J.; Zhu, D. Forecasting patient arrivals at emergency department using calendar and meteorological information. Appl. Intell. 2022, 1–12. [Google Scholar]
- Corcuera Hotz, I.; Hajat, S. The effects of temperature on accident and emergency department attendances in London: A time-series regression analysis. Int. J. Environ. Res. Public Health 2020, 17, 1957. [Google Scholar] [CrossRef] [Green Version]
- Chan, E.Y.; Goggins, W.B.; Yue, J.S.; Lee, P. Hospital admissions as a function of temperature, other weather phenomena and pollution levels in an urban setting in China. Bull. World Health Organ. 2013, 91, 576–584. [Google Scholar] [CrossRef]
- Linares, C.; Diaz, J. Impact of high temperatures on hospital admissions: Comparative analysis with previous studies about mortality (Madrid). Eur. J. Public Health 2008, 18, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Wargon, M.; Casalino, E.; Guidet, B. From model to forecasting: A multicenter study in emergency departments. Acad. Emerg. Med. 2010, 17, 970–978. [Google Scholar] [CrossRef]
- Sato, R.C. Disease management with ARIMA model in time series. Einstein 2013, 11, 128. [Google Scholar] [CrossRef] [Green Version]
- Qiu, M.; Song, Y. Predicting the direction of stock market index movement using an optimized artificial neural network model. PLoS ONE 2016, 11, e0155133. [Google Scholar] [CrossRef] [Green Version]
- Toharudin, T.; Pontoh, R.S.; Caraka, R.E.; Zahroh, S.; Lee, Y.; Chen, R.C. Employing long short-term memory and Facebook prophet model in air temperature forecasting. Commun. Stat.-Simul. Comput. 2020, 1–24. [Google Scholar] [CrossRef]
- Zhang, X.; Pang, Y.; Cui, M.; Stallones, L.; Xiang, H. Forecasting mortality of road traffic injuries in China using seasonal autoregressive integrated moving average model. Ann. Epidemiol. 2015, 25, 101–106. [Google Scholar] [CrossRef]
- Service, N.W. NOWDATA—NOAA Online Weather Data. Available online: https://www.weather.gov/wrh/Climate?wfo=dtx (accessed on 15 December 2021).
- Calegari, R.; Fogliatto, F.S.; Lucini, F.R.; Neyeloff, J.; Kuchenbecker, R.S.; Schaan, B.D. Forecasting daily volume and acuity of patients in the emergency department. Comput. Math. Methods Med. 2016, 2016, 3863268. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.S.; Thomas, A.; Evans, R.S.; Welch, S.J.; Haug, P.J.; Snow, G.L. Forecasting daily patient volumes in the emergency department. Acad. Emerg. Med. 2008, 15, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Romero, T. Americans Fear Hospital Visits Amid the COVID-19 Crisis. The Beach? Not So Much. Philly Voice Newspaper. Available online: https://www.phillyvoice.com/hospital-fear-covid-19-coronavirus-pandemic-beach-salons-survey/ (accessed on 29 May 2020).
- Michigan.gov. Coronavirus—Michigan Data. Available online: https://www.michigan.gov/coronavirus/0,9753,7-406-98163_98173---,00.html (accessed on 15 December 2021).
- Zhang, X.; Liu, Y.; Yang, M.; Zhang, T.; Young, A.A.; Li, X. Comparative study of four time series methods in forecasting typhoid fever incidence in China. PLoS ONE 2013, 8, e63116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kam, H.J.; Sung, J.O.; Park, R.W. Prediction of daily patient numbers for a regional emergency medical center using time series analysis. Healthc. Inform. Res. 2010, 16, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arunraj, N.S.; Ahrens, D.; Fernandes, M. Application of SARIMAX model to forecast daily sales in food retail industry. Int. J. Oper. Res. Inf. Syst. 2016, 7, 1–21. [Google Scholar] [CrossRef]
- Cools, M.; Moons, E.; Wets, G. Investigating the variability in daily traffic counts through use of ARIMAX and SARIMAX models: Assessing the effect of holidays on two site locations. Transp. Res. Rec. 2009, 2136, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.J.; Letham, B. Forecasting at scale. Am. Stat. 2018, 72, 37–45. [Google Scholar] [CrossRef]
- Champion, R.; Kinsman, L.D.; Lee, G.A.; Masman, K.A.; May, E.A.; Mills, T.M.; Taylor, M.D.; Thomas, P.R.; Williams, R.J. Forecasting emergency department presentations. Aust. Health Rev. 2007, 31, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Koehler, A.B.; Snyder, R.D.; Ord, J.K. Forecasting models and prediction intervals for the multiplicative Holt–Winters method. Int. J. Forecast. 2001, 17, 269–286. [Google Scholar] [CrossRef] [Green Version]
- Le, X.-H.; Ho, H.V.; Lee, G.; Jung, S. Application of long short-term memory (LSTM) neural network for flood forecasting. Water 2019, 11, 1387. [Google Scholar] [CrossRef] [Green Version]
- Zheng, J.; Xu, C.; Zhang, Z.; Li, X. Electric load forecasting in smart grids using long-short-term-memory based recurrent neural network. In Proceedings of the 2017 51st Annual Conference on Information Sciences and Systems (CISS), Baltimore, MD, USA, 22–24 March 2017; pp. 1–6. [Google Scholar]
- Masoud, S.; Mariscal, N.; Huang, Y.; Zhu, M. A Sensor-Based Data Driven Framework to Investigate PM 2.5 in the Greater Detroit Area. IEEE Sens. J. 2021, 21, 16192–16200. [Google Scholar] [CrossRef]
- Upshur, R.E.; Moineddin, R.; Crighton, E.; Kiefer, L.; Mamdani, M. Simplicity within complexity: Seasonality and predictability of hospital admissions in the province of Ontario 1988–2001, a population-based analysis. BMC Health Serv. Res. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, S.A.; Joy, M.P.; Pearson, J. Forecasting demand of emergency care. Health Care Manag. Sci. 2002, 5, 297–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downing, A.; Wilson, R. Temporal and demographic variations in attendance at accident and emergency departments. Emerg. Med. J. 2002, 19, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Duarte, D.; Walshaw, C.; Ramesh, N. A comparison of time-series predictions for healthcare emergency department indicators and the impact of COVID-19. Appl. Sci. 2021, 11, 3561. [Google Scholar] [CrossRef]
- Wargon, M.; Guidet, B.; Hoang, T.; Hejblum, G. A systematic review of models for forecasting the number of emergency department visits. Emerg. Med. J. 2009, 26, 395–399. [Google Scholar] [CrossRef]


| Models | Benefits | Limitations |
|---|---|---|
| SARIMA/ SARIMAX | Solid mathematical and statistical theory. Time-varying trends/seasonal patterns. Relatively few parameters. Handles exogenous variables. | Difficulty tuning the model parameters. Usually computationally expensive. Prone to overfitting. |
| FP | Supports seasonality with multiple periods. Robust to missing data. Does not require data interpolation. Handles outliers. Handles exogenous variables. | Does not consider multiplicative models. Strict formatting requirement Restricted to Gaussian noise distribution. Does not take autocorrelation into account. Does not assume a stochastic trend. |
| HW | Works best for data with trends and with seasonality that increases over time. The results are interpretable. Very easy to implement. | The presence of outliers distorts the results. Not expanded to multivariable approach. Accounts for only a single seasonal pattern. |
| LSTM | Learns information for an extended period. Mitigates the vanishing gradient problem. No specific assumptions. Handles exogenous variables. | Computationally time-consuming. Sensitive to random weight initializations. Prone to overfitting. |
| Factors | Variables | Explanation |
|---|---|---|
| Disease Outbreak | COVID lockdown | Denoting whether the COVID lockdown was in place or not in Michigan |
| Climatic | Average temperature | The average temperature (K) |
| Minimum temperature | The minimum temperature (K) | |
| Maximum temperature | The maximum temperature (K) | |
| Precipitation | Quantity of water deposited (i.e., rain, snow, or hail) | |
| Relative humidity | Percentage of relative humidity | |
| Pressure | Pressure within the earth atmosphere (Hg) |
| Models | Forecasting Horizon (in Days) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 7 | 14 | 21 | 30 | ||||||
| RMSE | MAE | RMSE | MAE | RMSE | MAE | RMSE | MAE | RMSE | MAE | |
| SARIMA | 33.57 | 26.58 | 32.73 | 26.03 | 28.81 | 22.28 | 47.59 | 39.97 | 96.20 | 89.92 |
| FP | 43.82 | 34.74 | 45.94 | 41.62 | 54.50 | 51.15 | 60.67 | 57.27 | 53.75 | 49.99 |
| HW | 28.42 | 21.29 | 28.19 | 21.32 | 30.20 | 23.07 | 38.47 | 32.34 | 89.74 | 84.09 |
| LSTM | 29.92 | 23.64 | 29.94 | 23.65 | 30.70 | 23.92 | 30.43 | 23.97 | 31.32 | 24.52 |
| Models | Forecasting Horizon (in days) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 7 | 14 | 21 | 30 | ||||||
| RMSE | MAE | RMSE | MAE | RMSE | MAE | RMSE | MAE | RMSE | MAE | |
| SARIMAX | 35.57 | 31.08 | 39.76 | 34.75 | 48.27 | 43.02 | 52.89 | 46.96 | 60.92 | 53.91 |
| FP | 48.68 | 43.25 | 58.27 | 53.37 | 70.07 | 65.56 | 80.34 | 76.13 | 78.00 | 72.39 |
| LSTM | 28.55 | 20.52 | 30.04 | 21.32 | 31.26 | 22.14 | 31.20 | 23.54 | 35.96 | 28.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Etu, E.-E.; Monplaisir, L.; Masoud, S.; Arslanturk, S.; Emakhu, J.; Tenebe, I.; Miller, J.B.; Hagerman, T.; Jourdan, D.; Krupp, S. A Comparison of Univariate and Multivariate Forecasting Models Predicting Emergency Department Patient Arrivals during the COVID-19 Pandemic. Healthcare 2022, 10, 1120. https://doi.org/10.3390/healthcare10061120
Etu E-E, Monplaisir L, Masoud S, Arslanturk S, Emakhu J, Tenebe I, Miller JB, Hagerman T, Jourdan D, Krupp S. A Comparison of Univariate and Multivariate Forecasting Models Predicting Emergency Department Patient Arrivals during the COVID-19 Pandemic. Healthcare. 2022; 10(6):1120. https://doi.org/10.3390/healthcare10061120
Chicago/Turabian StyleEtu, Egbe-Etu, Leslie Monplaisir, Sara Masoud, Suzan Arslanturk, Joshua Emakhu, Imokhai Tenebe, Joseph B. Miller, Tom Hagerman, Daniel Jourdan, and Seth Krupp. 2022. "A Comparison of Univariate and Multivariate Forecasting Models Predicting Emergency Department Patient Arrivals during the COVID-19 Pandemic" Healthcare 10, no. 6: 1120. https://doi.org/10.3390/healthcare10061120
APA StyleEtu, E.-E., Monplaisir, L., Masoud, S., Arslanturk, S., Emakhu, J., Tenebe, I., Miller, J. B., Hagerman, T., Jourdan, D., & Krupp, S. (2022). A Comparison of Univariate and Multivariate Forecasting Models Predicting Emergency Department Patient Arrivals during the COVID-19 Pandemic. Healthcare, 10(6), 1120. https://doi.org/10.3390/healthcare10061120