
The Early Dynamic Change in Cardiac Enzymes and Renal Function Is Associated with Mortality in Patients with Fulminant Myocarditis on Extracorporeal Membrane Oxygenation: Analysis of a Single Center’s Experience

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Device and Management
2.3. Data Collection and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cutpoint (%) | Sensitivity | Specificity | Correctly Classified | LR+ | LR− |
|---|---|---|---|---|---|
| (≥−3.49) | 100.00% | 0.00% | 31.58% | 1.0000 | |
| (≥−2.62) | 100.00% | 7.69% | 36.84% | 1.0833 | 0.0000 |
| (≥−0.87) | 100.00% | 15.38% | 42.11% | 1.1818 | 0.0000 |
| (≥−0.37) | 100.00% | 23.08% | 47.37% | 1.3000 | 0.0000 |
| (≥−0.21) | 100.00% | 30.77% | 52.63% | 1.4444 | 0.0000 |
| (≥−0.15) | 100.00% | 38.46% | 57.89% | 1.6250 | 0.0000 |
| (≥−0.1) | 100.00% | 46.15% | 63.16% | 1.8571 | 0.0000 |
| (≥−0.09) | 100.00% | 53.85% | 68.42% | 2.1667 | 0.0000 |
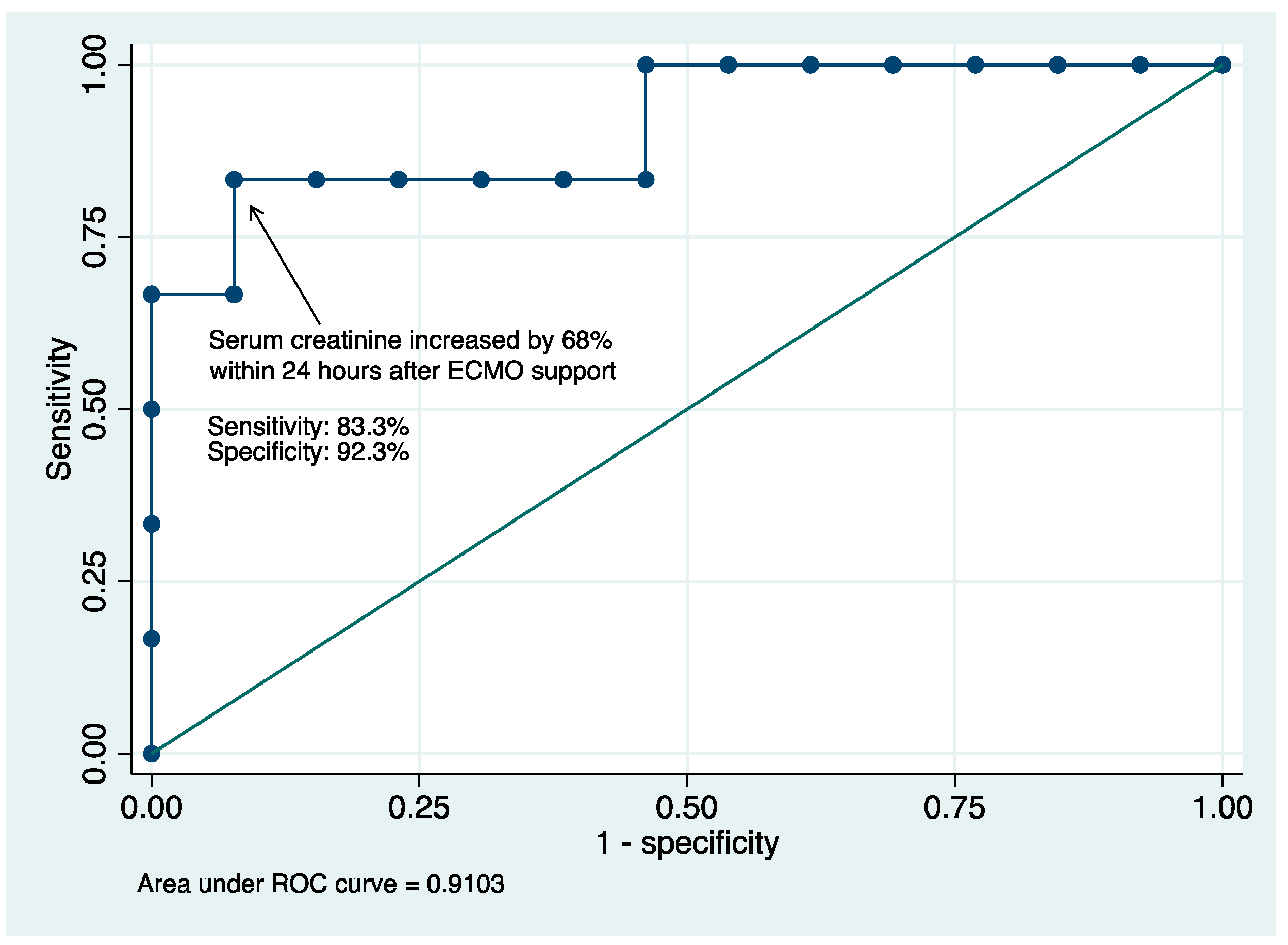
| (≥0.03) | 83.33% | 53.85% | 63.16% | 1.8056 | 0.3095 |
| (≥0.39) | 83.33% | 76.92% | 78.95% | 3.6111 | 0.2167 |
| (≥0.51) | 83.33% | 84.62% | 84.21% | 5.4167 | 0.1970 |
| (≥0.68) | 83.33% | 92.31% | 89.47% | 10.8333 | 0.1806 |
| (≥0.83) | 66.67% | 92.31% | 84.21% | 8.6667 | 0.3611 |
| (≥1.66) | 66.67% | 100.00% | 89.47% | 0.3333 | |
| (≥1.7) | 50.00% | 100.00% | 84.21% | 0.5000 | |
| (≥1.97) | 33.33% | 100.00% | 78.95% | 0.6667 | |
| (≥2.2) | 16.67% | 100.00% | 73.68% | 0.8333 | |
| (>2.2) | 0.00% | 100.00% | 68.42% | 1.0000 |
References
- Sharma, A.N.; Stultz, J.R.; Bellamkonda, N.; Amsterdam, E.A. Fulminant myocarditis: Epidemiology, pathogenesis, diagnosis, and management. Am. J. Cardiol. 2019, 124, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Kociol, R.D.; Cooper, L.T.; Fang, J.C.; Moslehi, J.J.; Pang, P.S.; Sabe, M.A.; Shah, R.V.; Sims, D.B.; Thiene, G.; Vardeny, O. Recognition and initial management of fulminant myocarditis: A scientific statement from the American Heart Association. Circulation 2020, 141, e69–e92. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.; Khalpey, Z.; Smith, R.; Burkhoff, D.; Kociol, R.D. Venoarterial extracorporeal membrane oxygenation for cardiogenic shock and cardiac arrest: Cardinal considerations for initiation and management. Circ. Heart Fail. 2018, 11, e004905. [Google Scholar] [CrossRef]
- Hsu, K.-H.; Chi, N.-H.; Yu, H.-Y.; Wang, C.-H.; Huang, S.-C.; Wang, S.-S.; Ko, W.-J.; Chen, Y.-S. Extracorporeal membranous oxygenation support for acute fulminant myocarditis: Analysis of a single center’s experience. Eur. J. Cardio-Thorac. Surg. 2011, 40, 682–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, T.; Ishida, K.; Taniguchi, Y.; Nakagawa, T.; Seguchi, M.; Wada, H.; Sugawara, Y.; Funayama, H.; Mitsuhashi, T.; Momomura, S.-I. Prognosis of patients with fulminant myocarditis managed by peripheral venoarterial extracorporeal membranous oxygenation support: A retrospective single-center study. J. Intensiv. Care 2015, 3, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, X.; Li, B.; Cheng, Z. Extracorporeal membrane oxygenation in adult patients with acute fulminant myocarditis. Herz 2018, 43, 728–732. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Asaumi, Y.; Nakamura, Y.; Nakatani, T.; Nagai, T.; Kanaya, T.; Kawakami, S.; Honda, S.; Kataoka, Y.; Nakajima, S. Clinical determinants of successful weaning from extracorporeal membrane oxygenation in patients with fulminant myocarditis. ESC Heart Fail. 2018, 5, 675–684. [Google Scholar] [CrossRef]
- Chao, C.M.; Sung, M.I.; Cheng, K.C.; Lai, C.C.; Chan, K.S.; Cheng, A.C.; Hsing, S.C.; Chen, C.M. Prognostic factors and outcomes of unplanned extubation. Sci. Rep. 2017, 7, 8636. [Google Scholar] [CrossRef] [Green Version]
- Asaumi, Y.; Yasuda, S.; Morii, I.; Kakuchi, H.; Otsuka, Y.; Kawamura, A.; Sasako, Y.; Nakatani, T.; Nonogi, H.; Miyazaki, S. Favourable clinical outcome in patients with cardiogenic shock due to fulminant myocarditis supported by percutaneous extracorporeal membrane oxygenation. Eur. Heart J. 2005, 26, 2185–2192. [Google Scholar] [CrossRef] [Green Version]
- Ishida, K.; Wada, H.; Sakakura, K.; Kubo, N.; Ikeda, N.; Sugawara, Y.; Ako, J.; Momomura, S.-I. Long-term follow-up on cardiac function following fulminant myocarditis requiring percutaneous extracorporeal cardiopulmonary support. Heart Vessel. 2013, 28, 86–90. [Google Scholar] [CrossRef]
- Chong, S.-Z.; Fang, C.-Y.; Fang, H.-Y.; Chen, H.-C.; Chen, C.-J.; Yang, C.-H.; Hang, C.-L.; Yip, H.-K.; Wu, C.-J.; Lee, W.-C. Associations with the in-hospital survival following extracorporeal membrane oxygenation in adult acute fulminant myocarditis. J. Clin. Med. 2018, 7, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diddle, J.W.; Almodovar, M.C.; Rajagopal, S.K.; Rycus, P.T.; Thiagarajan, R.R. Extracorporeal membrane oxygenation for the support of adults with acute myocarditis. Crit. Care Med. 2015, 43, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.S.C.; Tonna, J.E.; Nanjayya, V.; Nixon, P.; Abrams, D.C.; Raman, L.; Bernard, S.; Finney, S.J.; Grunau, B.; Youngquist, S.T. Extracorporeal cardiopulmonary resuscitation in adults. Interim guideline consensus statement from the extracorporeal life support organization. ASAIO J. 2021, 67, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Burrell, A.; Roberts, L.; Bailey, M.; Sheldrake, J.; Rycus, P.T.; Hodgson, C.; Scheinkestel, C.; Cooper, D.J.; Thiagarajan, R.R. Predicting survival after ECMO for refractory cardiogenic shock: The survival after veno-arterial-ECMO (SAVE)-score. Eur. Heart J. 2015, 36, 2246–2256. [Google Scholar] [CrossRef]
- Dennert, R.; Velthuis, S.; Schalla, S.; Eurlings, L.; van Suylen, R.-J.; van Paassen, P.; Tervaert, J.W.C.; Wolffs, P.; Goossens, V.J.; Bruggeman, C. Intravenous immunoglobulin therapy for patients with idiopathic cardiomyopathy and endomyocardial biopsy-proven high PVB19 viral load. Antivir. Ther. 2010, 15, 193–201. [Google Scholar] [CrossRef]
- Maisch, B.; Hufnagel, G.; Kölsch, S.; Funck, R.; Richter, A.; Rupp, H.; Herzum, M.; Pankuweit, S. Treatment of inflammatory dilated cardiomyopathy and (peri) myocarditis with immunosuppression and iv immunoglobulins. Herz 2004, 29, 624–636. [Google Scholar] [CrossRef]
- Mason, J.W.; O’Connell, J.B.; Herskowitz, A.; Rose, N.R.; McManus, B.M.; Billingham, M.E.; Moon, T.E. A clinical trial of immunosuppressive therapy for myocarditis. The Myocarditis Treatment Trial Investigators. N. Engl. J. Med. 1995, 333, 269–275. [Google Scholar] [CrossRef]
- McNamara, D.M.; Holubkov, R.; Starling, R.C.; Dec, G.W.; Loh, E.; Torre-Amione, G.; Gass, A.; Janosko, K.; Tokarczyk, T.; Kessler, P. Controlled trial of intravenous immune globulin in recent-onset dilated cardiomyopathy. Circulation 2001, 103, 2254–2259. [Google Scholar] [CrossRef] [Green Version]
- Isogai, T.; Yasunaga, H.; Matsui, H.; Tanaka, H.; Horiguchi, H.; Fushimi, K. Effect of intravenous immunoglobulin for fulminant myocarditis on in-hospital mortality: Propensity score analyses. J. Card. Fail. 2015, 21, 391–397. [Google Scholar] [CrossRef]
- Chou, H.-W.; Wang, C.-H.; Lin, L.-Y.; Chi, N.-H.; Chou, N.-K.; Yu, H.-Y.; Chen, Y.-S. Prognostic factors for heart recovery in adult patients with acute fulminant myocarditis and cardiogenic shock supported with extracorporeal membrane oxygenation. J. Crit. Care 2020, 57, 214–219. [Google Scholar] [CrossRef]
- Ricarte Bratti, J.P.; Cavayas, Y.A.; Noly, P.E.; Serri, K.; Lamarche, Y. Modalities of left ventricle decompression during VA-ECMO therapy. Membranes 2021, 11, 209. [Google Scholar] [CrossRef] [PubMed]
- Slottosch, I.; Liakopoulos, O.; Kuhn, E.; Scherner, M.; Deppe, A.-C.; Sabashnikov, A.; Mader, N.; Choi, Y.-H.; Wippermann, J.; Wahlers, T. Lactate and lactate clearance as valuable tool to evaluate ECMO therapy in cardiogenic shock. J. Crit. Care 2017, 42, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Mungan, İ.; Kazancı, D.; Bektaş, Ş.; Ademoglu, D.; Turan, S. Does lactate clearance prognosticates outcomes in ECMO therapy: A retrospective observational study. BMC Anesthesiol. 2018, 18, 152. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Lumlertgul, N. Acute kidney injury in ECMO patients. Annu. Update Intensive Care Emerg. Med. 2021, 2021, 207–222. [Google Scholar]
- Tanawuttiwat, T.; Trachtenberg, B.H.; Hershberger, R.E.; Hare, J.M.; Cohen, M.G. Dual percutaneous mechanical circulatory support as a bridge to recovery in fulminant myocarditis. ASAIO J. 2011, 57, 477–479. [Google Scholar] [CrossRef]
- Hori, T.; Iida, M.; Uchiyama, M.; Shimokawa, T. Successful cases of percutaneous left ventricular assist device “Impella” to fulminant myocarditis. J. Cardiothorac. Surg. 2022, 17, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Van Linthout, S.; Klein, O.; Mairinger, T.; Krackhardt, F.; Potapov, E.V.; Schmidt, G.; Burkhoff, D.; Pieske, B.; Spillmann, F. Mechanical unloading by fulminant myocarditis: LV-IMPELLA, ECMELLA, BI-PELLA, and PROPELLA concepts. J. Cardiovasc. Transl. Res. 2019, 12, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Non-Survivors (n = 6) | Survivors (n = 22) | p-Value | |
|---|---|---|---|
| Age, years | 44.7 ± 18.6 | 49.2 ± 11.9 | 0.47 |
| Female sex | 3 (50%) | 12 (54.5%) | 1 |
| Body mass index | 23 (23–27.2) | 23.9 (21.8–26.8) | 0.9 |
| Comorbidities | |||
| Diabetes Mellitus | 1 (16.7%) | 2 (9.1%) | 0.53 |
| Non-occlusive coronary artery disease | 1 (16.7%) | 0 | 0.21 |
| CKD stages 3–5 | 0 | 2 (9.1) | 0.61 |
| SAVE score | −4.3 ± 6.5 | −1.4 ± 5.8 | 0.29 |
| Time from ED triage to ECMO cannulation (min) | 681 (140–1260) | 315 (140–766) | 0.73 |
| Refractory ventricular tachycardia/fibrillation | 0 | 2 (9.1%) | 1 |
| ECMO during CPR | 1 (16.7%) | 3 (13.6%) | 1 |
| LVEF (%) b | 19.9 (13.9–30.5) | 23.1 (18–23.4) | 0.92 |
| Steroid use | 1 (16.7%) | 7 (31.8%) | 0.39 |
| Intravenous immunoglobin use | 1 (16.7%) | 1 (4.6%) | 0.64 |
| Laboratory data prior to ECMO support | |||
| WBC (K/uL) | 11.1 (8.2–14.2) | 10.9 (8.6–14.8) | 0.73 |
| Hb (g/dL) c | 15.4 (13.1–15.9) | 13.8 (12.6–14.8) | 0.25 |
| Platelet (K/uL) c | 201 (175–287) | 185 (112–270) | 0.58 |
| CK-MB (IU/L) | 108.9 (27.8–199) | 52.9 (29.2–70.3) | 0.56 |
| Troponin I (ng/mL) | 13.9 (5.5–32.3) | 14.1 (5.5–33.1) | 0.98 |
| CPK (IU/L) c | 620 (274–1171) | 788 (419–1096) | 0.84 |
| Lactate level (mmol/L) | 4.2 (3.7–16.3) | 5.6 (2.4–8.8) | 0.67 |
| BUN (mg/dL) | 21 (21–28) | 21 (14–33) | 0.99 |
| Creatinine (mg/dL) | 1.34 (1.23–1.53) | 1.35 (0.96–2.43) | 0.88 |
| Arterial PH | 7.25 (7.14–7.38) | 7.36 (7.3–42) | 0.29 |
| Peak CK-MB during hospitalization (IU/L) | 185.9 (83.5–727.2) | 70.3 (44.5–149) | 0.16 |
| Peak troponin I during hospitalization (ng/mL) | 66.6 (16.6–82) | 31.9 (10.9–47.6) | 0.15 |
| Non-Survivors (n = 6) | Survivors (n = 22) | p-Value | |
|---|---|---|---|
| Duration of ECMO (days) | 4.5 (4–9) | 8 (5–14) | 0.1 |
| ICU length of stay (days) | 5 (4–9) | 20 (11–45) | 0.002 * |
| Renal replacement therapy | 5 (83.3%) | 10 (45.5%) | 0.23 |
| Major complications | |||
| Limb ischemia | 1 (16.7%) | 0 | 0.21 |
| Bowel ischemia | 1 (16.7%) | 0 | 0.21 |
| Major GI bleeding | 1 (16.7%) | 4 (18.2%) | 1 |
| Major bleeding from cannula sites | 0 | 1 (4.6%) | 1 |
| ECMO cannula malposition or dislodgement | 0 | 0 | N/A |
| Ischemic stroke or intracranial bleeding | 0 | 0 | N/A |
| Non-Survivors (n = 6) | Survivors (n = 22) | p-Value 1 | |||
|---|---|---|---|---|---|
| Δ | Δ in % | Δ | Δ in % | ||
| WBC (K/uL) | 1.1 (0 to 4.1) | 6.9% (0 to 32.1) | 0.6 (−0.7 to 2) | 6.5% (−10 to 12.5) | 0.7 |
| Hb (g/dL) | −1.9 (−3.4 to −0.7) | −13.7% (−21.5 to −5.3) | −1.7 (−2.4 to −1.1) | −12.4% (−16.4 to −7.4) | 0.82 |
| Platelet (K/uL) | −92 (−138 to −47) | −38.4% (−52.5 to −16.4) | −49.5 (−76 to −8) | −28.3% (−37.6 to −1.9) | 0.49 |
| CK-MB (IU/L) | 49.5 (30.6 to 251) | 96.8% (23.3 to 144.1) | −10.2 (−20.4 to −1.6) | −23.7% (−41.5 to −10.4) | 0.022 * |
| Troponin I (ng/mL) | 42 (7.5 to 46.8) | 378% (145 to 1359.9) | −0.1 (−1.6 to 15.8) | 1.7% (−18 to 147.5) | 0.032 * |
| CPK (IU/L) | 1418 (486 to 18601) | 214% (41.5 to 2265) | 257 (−35 to 1160) | 41.6% (−11 to 190.7) | 0.1 |
| Lactate (mmol/L) | −1.8 (−3.1 to 2.4) | −18.7% (−25.4 to 54) | −2 (−4.4 to 0.5) | −32% (−64.5 to 29) | 0.44 |
| BUN (mg/dL) | 13 (10 to 13) | 46.4% (33.3 to 61.9) | 1.5 (−4.5 to 4) | 3.9% (−23.6 to 18.5) | 0.006 * |
| Creatinine (mg/dL) | 1.7 (0.7 to 2) | 108% (52.3 to 156.6) | −0.1 (−0.4 to 0.3) | −8.5% (−25.6 to 17.5) | 0.005 * |
| Arterial PH | 0.09 (−0.07 to 0.12) | 1.22% (−0.9 to 1.7) | 0.05 (−0.02 to 0.13) | 0.67% (−0.3 to 1.8) | 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, C.-L.; Ju, T.R.; Lee, C.C.; Lin, H.-T.; Wang, A.-L.; Chen, R.J.; Lin, Y.-C. The Early Dynamic Change in Cardiac Enzymes and Renal Function Is Associated with Mortality in Patients with Fulminant Myocarditis on Extracorporeal Membrane Oxygenation: Analysis of a Single Center’s Experience. Healthcare 2022, 10, 1063. https://doi.org/10.3390/healthcare10061063
Ho C-L, Ju TR, Lee CC, Lin H-T, Wang A-L, Chen RJ, Lin Y-C. The Early Dynamic Change in Cardiac Enzymes and Renal Function Is Associated with Mortality in Patients with Fulminant Myocarditis on Extracorporeal Membrane Oxygenation: Analysis of a Single Center’s Experience. Healthcare. 2022; 10(6):1063. https://doi.org/10.3390/healthcare10061063
Chicago/Turabian StyleHo, Ching-Lin, Teressa Reanne Ju, Chi Chan Lee, Hsin-Ti Lin, Alexander-Lee Wang, Robert Jeenchen Chen, and You-Cian Lin. 2022. "The Early Dynamic Change in Cardiac Enzymes and Renal Function Is Associated with Mortality in Patients with Fulminant Myocarditis on Extracorporeal Membrane Oxygenation: Analysis of a Single Center’s Experience" Healthcare 10, no. 6: 1063. https://doi.org/10.3390/healthcare10061063
APA StyleHo, C.-L., Ju, T. R., Lee, C. C., Lin, H.-T., Wang, A.-L., Chen, R. J., & Lin, Y.-C. (2022). The Early Dynamic Change in Cardiac Enzymes and Renal Function Is Associated with Mortality in Patients with Fulminant Myocarditis on Extracorporeal Membrane Oxygenation: Analysis of a Single Center’s Experience. Healthcare, 10(6), 1063. https://doi.org/10.3390/healthcare10061063