
The Dose-Response Efficacy of Physical Training on Frailty Status and Physical Performance in Community-Dwelling Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Methods
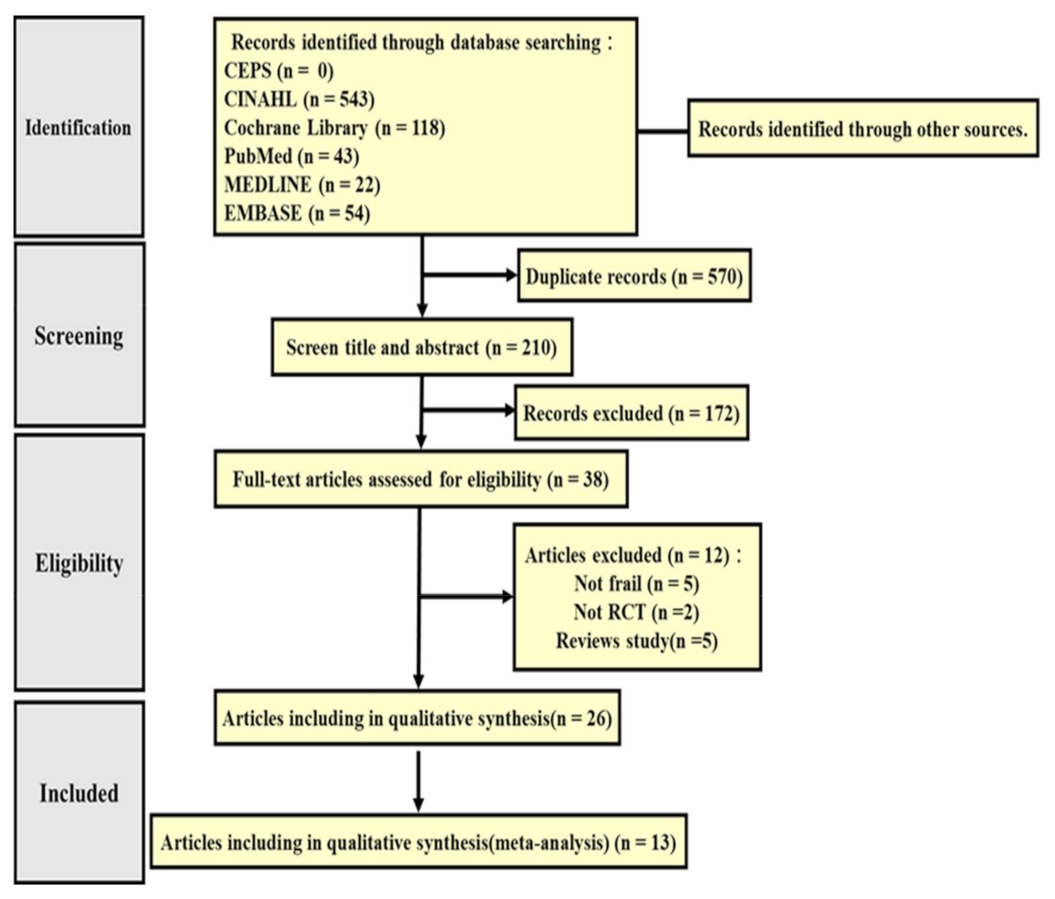
2.1. Literature Search
2.2. Study Selection
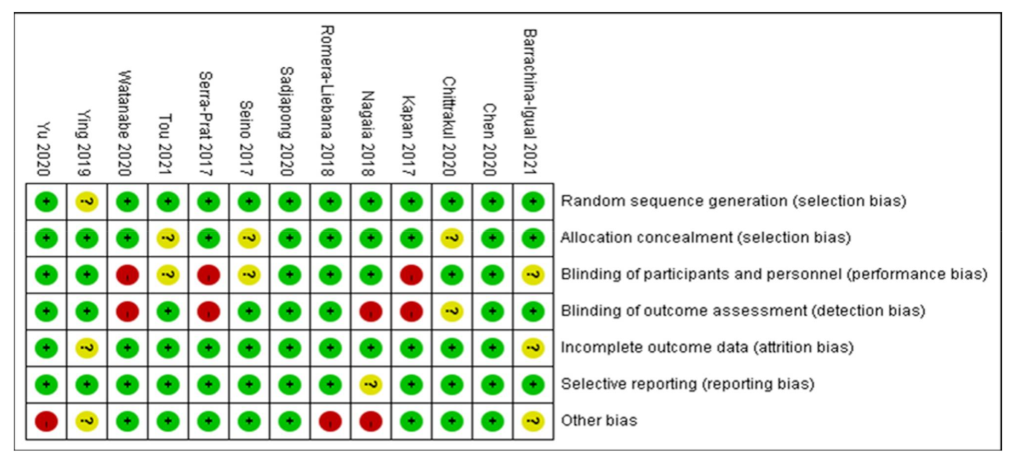
2.3. Risk of Bias Appraisal
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Selected Studies
3.2. Risk of Bias Assessment
3.3. Study Characteristics
3.3.1. Intervention Design
3.3.2. Types of Physical Training
3.3.3. Dose-Response of Physical Training: Dose
3.3.4. Dose-Response of Physical Training: Frequency
3.3.5. Dose-Response of Physical Training: Duration
3.3.6. Adverse Events
3.4. Outcome Measures
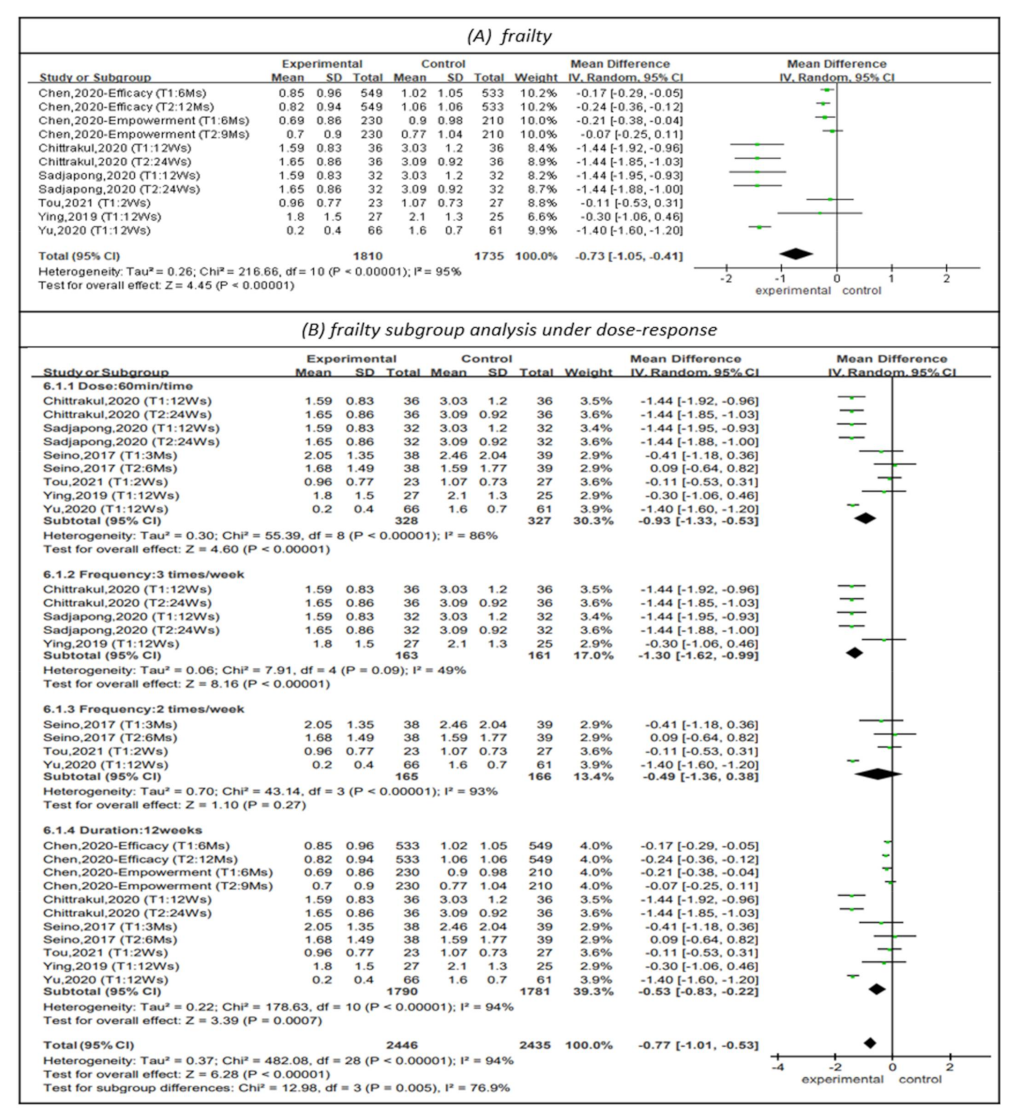
3.4.1. Effectiveness on Frailty
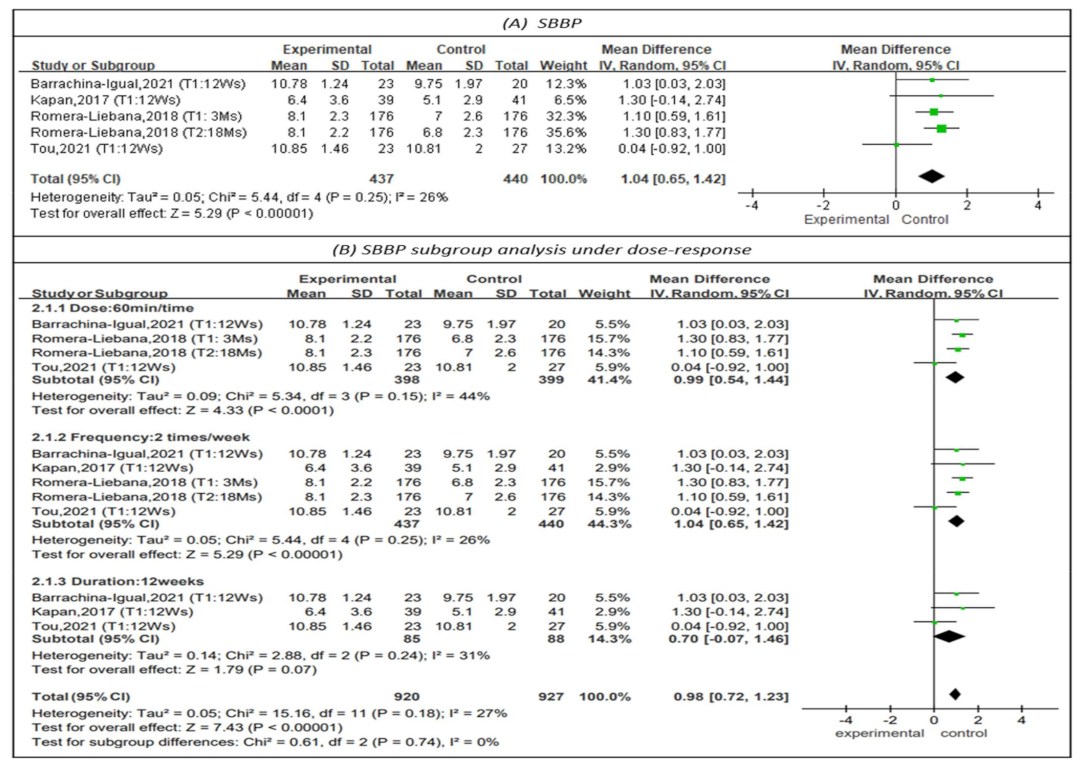
3.4.2. Effectiveness on Physical Performance
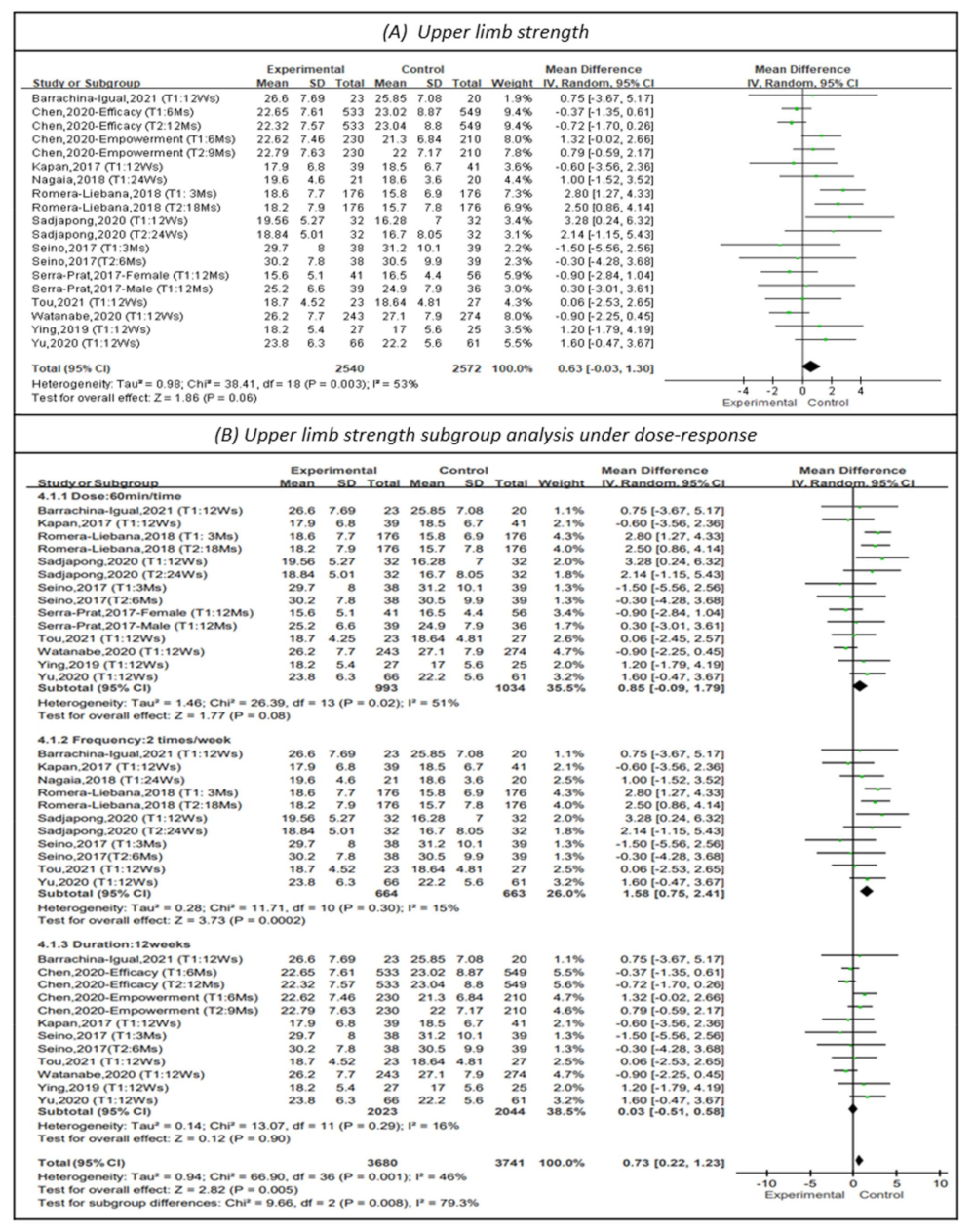
3.4.3. Effectiveness on Upper Limb Strength
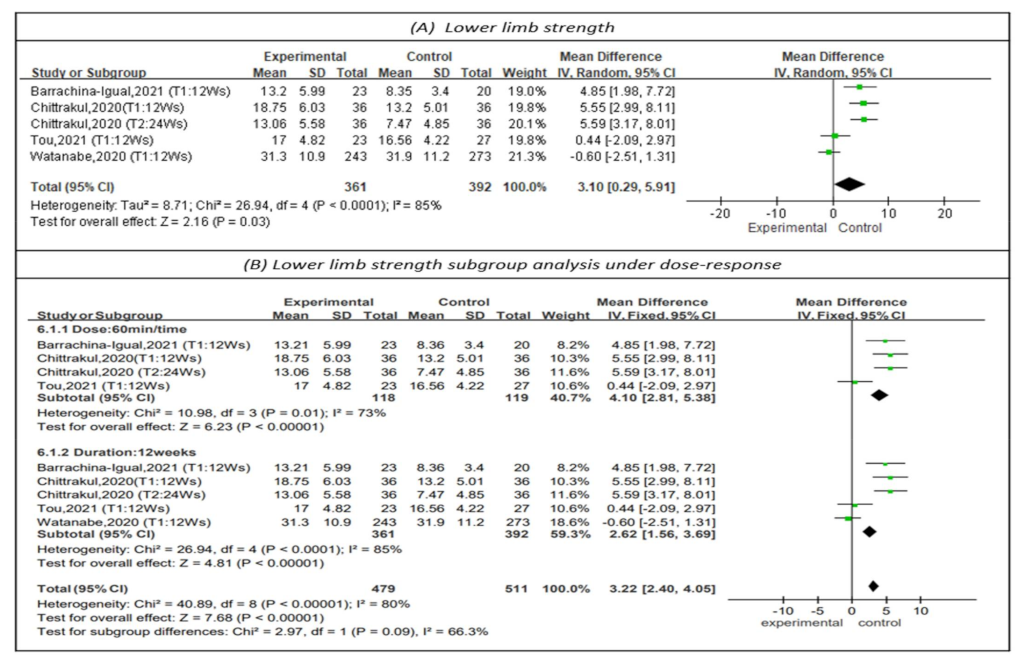
3.4.4. Effectiveness on Lower Limb Strength
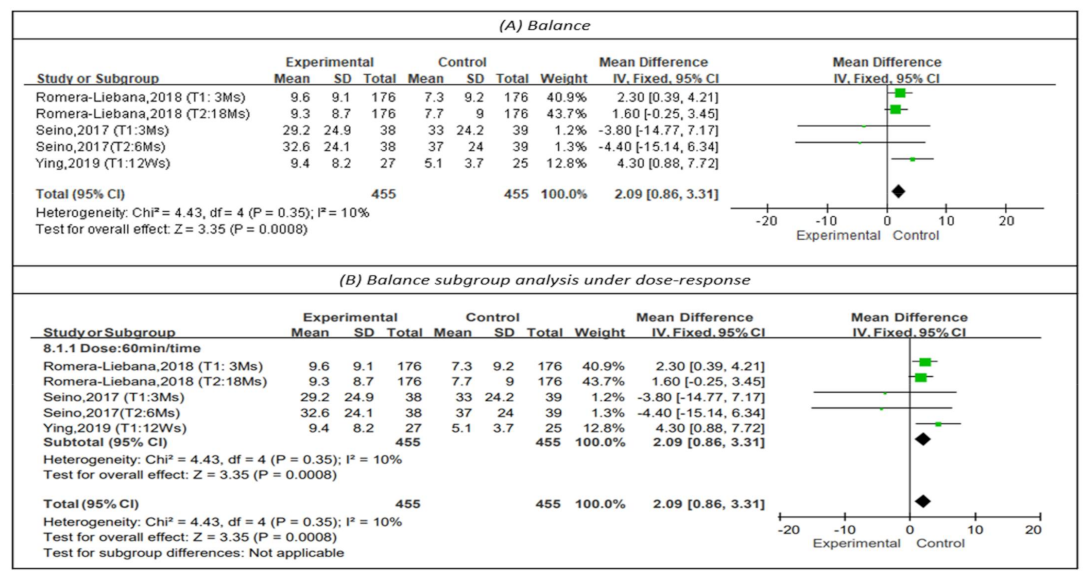
3.4.5. Effectiveness on Balance
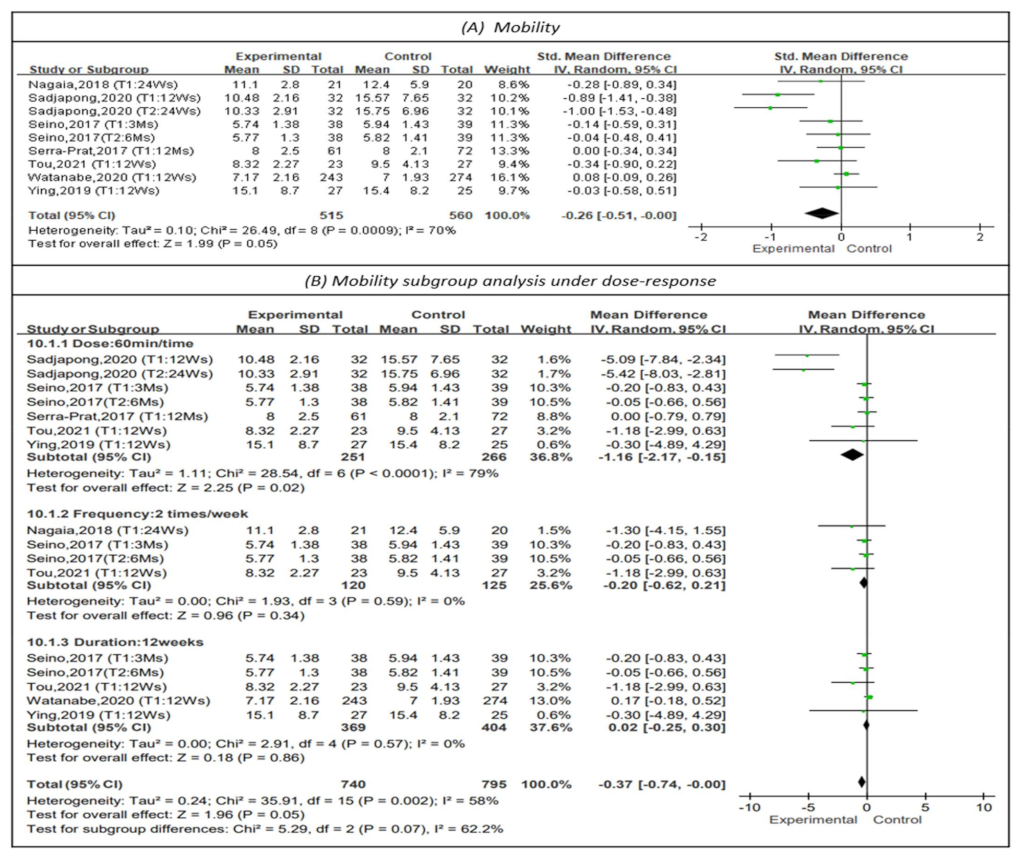
3.4.6. Effectiveness on Mobility
4. Discussion
4.1. The Efficacy of Physical Training in the Community-Dwelling Elderly
4.2. Dose-Response Efficacy of Physical Training on Frailty Status
4.3. Dose-Response Efficacy of Physical Training on Physical Performance
4.3.1. Dose-Response Efficacy on Physical Performance
4.3.2. Dose-Response Efficacy on Muscular Strength
4.3.3. Dose-Response Efficacy on Balance
4.3.4. Dose-Response Efficacy on Mobility
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Hamedanchi, A.; Zanjari, N.; Khankeh, H.R.; Momtaz, Y.A. Phenomenology in Gerontology: From Philosophy to Method. Curr. Psychiatry Res. Rev. 2021, 17, 220–230. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, G.M.; Olson, R.D. The physical activity guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Lien, C.; Lim, W.S.; Wong, W.C.; Wong, C.H.; Ng, T.P.; Woo, J.; Dong, B.; de la Vega, S.; Poi, P.J.H.; et al. The Asia-Pacific clinical practice guidelines for the management of frailty. J. Am. Med. Dir. Assoc. 2017, 18, 564–575. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.S.; Pinheiro, M.B.; Fairhall, N.; Walsh, S.; Franks, T.C.; Kwok, W.; Bauman, A.; Sherrington, C. Evidence on physical activity and the prevention of frailty and sarcopenia among older people: A systematic review to inform the World Health Organization physical activity guidelines. J. Phys. Act. Health. 2020, 17, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Dipietro, L.; Campbell, W.W.; Buchner, D.M.; Erickson, K.I.; Powell, K.E.; Bloodgood, B.; Hughes, T.; Day, K.R.; Piercy, K.L.; Vaux-Bjerke, A.; et al. Physical activity, injurious falls, and physical function in aging: An umbrella review. Med. Sci. Sports Exerc. 2019, 51, 1303–1313. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, Y.; Du, S.; Wang, Q.; Xia, H.; Sun, R. Exercise interventions for improving physical function, daily living activities and quality of life in community-dwelling frail older adults: A systematic review and meta-analysis of randomized controlled trials. Geriatr. Nurs. 2020, 41, 261–273. [Google Scholar] [CrossRef]
- Haider, S.; Grabovac, I.; Dorner, T.E. Effects of physical activity interventions in frail and prefrail community-dwelling people on frailty status, muscle strength, physical performance and muscle mass—A narrative review. Wien. Klin. Wochenschr. 2019, 131, 244–254. [Google Scholar] [CrossRef] [Green Version]
- Falck, R.S.; Davis, J.C.; Best, J.R.; Crockett, R.A.; Liu-Ambrose, T. Impact of exercise training on physical and cognitive function among older adults: A systematic review and meta-analysis. Neurobiol. Aging. 2019, 79, 119–130. [Google Scholar] [CrossRef]
- Kidd, T.; Mold, F.; Jones, C.; Ream, E.; Grosvenor, W.; Sund-Levander, M.; Tingström, P.; Carey, N. What are the most effective interventions to improve physical performance in pre-frail and frail adults? A systematic review of randomised control trials. BMC Geriatr. 2019, 19, 184. [Google Scholar] [CrossRef] [Green Version]
- Apóstolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; D’Avanzo, B.; Gwyther, H.; et al. Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 140–232. [Google Scholar] [CrossRef]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef]
- De Souto Barreto, P.; Rolland, Y.; Maltais, M.; Vellas, B.; MAPT Study Group. Associations of Multidomain Lifestyle Intervention with Frailty: Secondary Analysis of a Randomized Controlled Trial. Am. J. Med. 2018, 131, 1382.e7–1382.e13. [Google Scholar] [CrossRef] [PubMed]
- Romera-Liebana, L.; Orfila, F.; Segura, J.M.; Real, J.; Fabra, M.L.; Möller, M.; Lancho, S.; Ramirez, A.; Marti, N.; Cullell, M.; et al. Effects of a Primary Care-Based Multifactorial Intervention on Physical and Cognitive Function in Frail, Elderly Individuals: A Randomized Controlled Trial. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Ožić, S.; Vasiljev, V.; Ivković, V.; Bilajac, L.; Rukavina, T. Interventions aimed at loneliness and fall prevention reduce frailty in elderly urban population. Medicine 2020, 99, e19145. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Yamada, Y.; Yoshida, T.; Yokoyama, K.; Miyake, M.; Yamagata, E.; Yamada, M.; Yoshinaka, Y.; Kimura, M.; Kyoto-Kameoka Study Group. Comprehensive geriatric intervention in community-dwelling older adults: A cluster-randomized controlled trial. J. Cachexia Sarcopenia Muscle 2020, 11, 26–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaushal, N.; Langlois, F.; Desjardins-Crépeau, L.; Hagger, M.S.; Bherer, L. Investigating dose-response effects of multimodal exercise programs on health-related quality of life in older adults. Clin. Interv. Aging 2019, 14, 209–271. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Review Manager (RevMan) [Computer Program]. Version 5.4.1. Copenhagen: The Nordic Cochrane Centre. The Cochrane Collaboration. 2020. Available online: https://training-cochrane-org.vgharpa.vghtpe.gov.tw/online-learning/core-software-cochrane-reviews/revman (accessed on 10 March 2022).
- Chen, L.K.; Hwang, A.C.; Lee, W.J.; Peng, L.N.; Lin, M.H.; Neil, D.L.; Shih, S.F.; Loh, C.H.; Chiou, S.T.; Taiwan Health Promotion Intervention Study for Elders research group. Efficacy of multidomain interventions to improve physical frailty, depression and cognition: Data from cluster-randomized controlled trials. J. Cachexia Sarcopenia Muscle 2020, 11, 650–662. [Google Scholar] [CrossRef] [Green Version]
- Chittrakul, J.; Siviroj, P.; Sungkarat, S.; Sapbamrer, R. Multi-System Physical Exercise Intervention for Fall Prevention and Quality of Life in Pre-Frail Older Adults: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 3102. [Google Scholar] [CrossRef]
- Kapan, A.; Luger, E.; Haider, S.; Titze, S.; Schindler, K.; Lackinger, C.; Dorner, T. Fear of falling reduced by a lay led home-based program in frail community-dwelling older adults: A randomised controlled trial. Arch. Gerontol. Geriatr. 2017, 68, 25–32. [Google Scholar] [CrossRef]
- Nagai, K.; Miyamato, T.; Okamae, A.; Tamaki, A.; Fujioka, H.; Wada, Y.; Uchiyama, Y.; Shinmura, K.; Domen, K. Physical activity combined with resistance training reduces symptoms of frailty in older adults: A randomized controlled trial. Arch. Gerontol. Geriatr. 2018, 76, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Sadjapong, U.; Yodkeeree, S.; Sungkarat, S.; Siviroj, P. Multicomponent Exercise Program Reduces Frailty and Inflammatory Biomarkers and Improves Physical Performance in Community-Dwelling Older Adults: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 3760. [Google Scholar] [CrossRef] [PubMed]
- Serra-Prat, M.; Sist, X.; Domenich, R.; Jurado, L.; Saiz, A.; Roces, A.; Palomera, E.; Tarradelles, M.; Papiol, M. Effectiveness of an intervention to prevent frailty in pre-frail community-dwelling older people consulting in primary care: A randomised controlled trial. Age Ageing 2017, 46, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, Y.Y.; Chen, I.H.; Wang, R.Y. Effects of Kinect-based exergaming on frailty status and physical performance in prefrail and frail elderly: A randomized controlled trial. Sci Rep. 2019, 9, 9353. [Google Scholar] [CrossRef]
- Yu, R.; Tong, C.; Ho, F.; Woo, J. Effects of a Multicomponent Frailty Prevention Program in Prefrail Community-Dwelling Older Persons: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2020, 19, 30640–30641. [Google Scholar] [CrossRef]
- Barrachina-Igual, J.; Martínez-Arnau, F.M.; Pérez-Ros, P.; Flor-Rufino, C.; Sanz-Requena, R.; Pablos, A. Effectiveness of the PROMUFRA program in pre-frail, community-dwelling older people: A randomized controlled trial. Geriatr. Nurs. 2021, 42, 582–591. [Google Scholar] [CrossRef]
- Seino, S.; Nishi, M.; Murayama, H.; Narita, M.; Yokoyama, Y.; Nofuji, Y.; Taniguchi, Y.; Amano, H.; Kitamura, A.; Shinkai, S. Effects of a multifactorial intervention comprising resistance exercise, nutritional and psychosocial programs on frailty and functional health in community-dwelling older adults: A randomized, controlled, cross-over trial. Geriatr. Gerontol. Int. 2017, 17, 2034–2045. [Google Scholar] [CrossRef]
- Tou, N.X.; Wee, S.-L.; Seah, W.T.; Ng, D.H.M.; Pang, B.W.J.; Lau, L.K.; Ng, T.P. Effectiveness of Community-Delivered Functional Power Training Program for Frail and Pre-frail Community-Dwelling Older Adults: A Randomized Controlled Study. Prev. Sci. 2021, 22, 1048–1059. [Google Scholar] [CrossRef]
- Jadczak, A.D.; Makwana, N.; Luscombe-Marsh, N.; Visvanathan, R.; Schultz, T.J. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 752–775. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample (I/C) | Experimental Group | Control Group | Follow Time | Outcome Measures |
|---|---|---|---|---|---|
| Barrachina-Igual, 2021 | 43 (23/20) | Resistance training combined with self-massage for myofascial release. Dose-response: about 60 min/time (dose), 2 times/week (frequency), total 12 weeks (duration). | Unclear | T1: 12 Wk | Physical frailty Muscle function Functional performance |
| Chen, 2020 | Efficacy: 1082 (549/533) Empowerment: 440 (230/210) | Efficacy Study: physical exercise, cognitive training and nutritional counseling. Dose-response: 45 min/time (dose). The sessions were curtailed and home practiced alone (frequency), total 12 weeks (duration). Empowerment Study: Efficacy version redesigned and additionally empowered. Dose-response: 45 min/time (dose), the sessions were completed at home and curtailed and monitored for amount of practice (frequency), total 12 weeks (duration). | The Efficacy Study compared telephone consultation. The Empowerment Study compared the standard Efficacy Study. | Efficacy T1: 6 Mo T2: 12 Mo Empowerment T1: 6 Mo T2: 9 Mo | CHS frailty score, Gait speed Grip strength |
| Chittrakul, 2020 | 72 (36/36) | Proprioception training, muscle strength training, reaction time exercise training with auditory cues, and postural balance training. Dose-response: 60 min/time (dose), 3 times/week (frequency), total 12 weeks (duration). | The control group received flexibility exercise training three times each week of the program. | T1: 12 Wk T2: 24 Wk | Knee extension strength |
| Kapan, 2017 | 80 (39/41) | Strength exercise programs supplemented with a nutrition. Dose-response: 35 min/time (dose), 2 times/week (frequency), total 12 weeks (duration). | The control group engaged in cognitive practice. | T1: 12 Wk | Physical functioning Handgrip strength Physical activity level |
| Nagaia, 2018 | 41 (21/20) | Resistance training. Dose-response: 2 times/week (frequency), total 24 weeks (duration). | The control group received resistance training. | T1: 24 Wk | Frailty status Physical function Muscle strength |
| Romera-Liebana, 2018 | 352 (176/176) | Physical activity, high-protein nutritional shake, memory workshops and medication review. Dose-response: 60 min/time (dose), 2 times/week (frequency), total 6 weeks (duration). | The control group received usual care. | T1: 3 Mo T2: 18 Mo | SPPB Strength by handgrip Functional reach Balance |
| Sadjapong, 2020 | 64 (32/32) | Aerobic training, resistance training, balance training and home practice. Dose-response: 60 min/time (dose), 3 times/week (frequency), total 24 weeks (duration). | The control group received usual care. | T1: 12 Wk T2: 24 Wk | Physical performance Hand strength Balance Endurance Frailty scores |
| Seino, 2017 | 77 (38/39) | Resistance exercise, nutritional or psychosocial programs and home practice. Dose-response: 60 min/time (dose), 2 times/week (frequency), total 12 weeks (duration). | The control group continued with their daily activities. | T1: 3 Mo T2: 6 Mo | Frailty status Physical function |
| Serra-Prat, 2017 | 172 (80/92) | Nutritional assessment and physical activity program (strength, balance and coordination exercises). Dose-response: about 60 min/time (dose), 4 times/week (frequency), total 12 months (duration). | The control group received usual care. | T1: 12 Mo | Frailty status Hand grip |
| Tou, 2021 | 57 (27/30) | Progressive power, balance exercises and home practice). Dose-response: 60 min/time (dose), 2 times/week (frequency), total 12 weeks (duration). | The control group continued with the exercise program. | T1: 12 Wk | Physical Function Frailty Status |
| Watanabe, 2020 | 517 (243/274) | Low-load resistance exercises, 2500 steps/day, oral functional care, a nutritional guide and home monitored practice. Dose-response: 90 min/time (dose), 1 time/week (frequency), total 12 weeks (duration). | The control group carried out the program by themself at home. | T1: 12 Wk | Physical functions: grip strength, knee extension strength, walking speeds, TUG, five-time chair standing test, 30 s chair stands, functional reach test, chair stepping test and a vertical jump index Physical activity |
| Ying-Yi, 2019 | 52 (25/27) | Tai-Chi, resistance and aerobic combination training and balance training. Dose-response: 60 min/time (dose), 3 times/week (frequency), total 12 weeks (duration). | The control group received a combined exercise program. | T1: 12 Wk | Frailty status SPPB Back scratch Chair sit and reach 30-s sit-to-stand 2-min step Single leg stance Functional reach Timed up and go Walking speed Grip strength |
| Yu, Tong, 2020 | 127 (66/61) | Multicomponent Frailty Prevention Program combined with exercise, computer-assisted cognitive training, and board game activities. Dose-response: 60 min/time (dose), 2 times/week (frequency), total 12 weeks (duration). | The control group received usual care. | T1: 12 Wk | Frailty Hand-grip strength Muscle endurance Balance Gait speed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, P.-S.; Hsieh, C.-J.; Tallutondok, E.B.; Peng, H.-J. The Dose-Response Efficacy of Physical Training on Frailty Status and Physical Performance in Community-Dwelling Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare 2022, 10, 586. https://doi.org/10.3390/healthcare10030586
Li P-S, Hsieh C-J, Tallutondok EB, Peng H-J. The Dose-Response Efficacy of Physical Training on Frailty Status and Physical Performance in Community-Dwelling Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare. 2022; 10(3):586. https://doi.org/10.3390/healthcare10030586
Chicago/Turabian StyleLi, Pei-Shan, Chia-Jung Hsieh, Eva Berthy Tallutondok, and Hsuan-Ju Peng. 2022. "The Dose-Response Efficacy of Physical Training on Frailty Status and Physical Performance in Community-Dwelling Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Healthcare 10, no. 3: 586. https://doi.org/10.3390/healthcare10030586
APA StyleLi, P.-S., Hsieh, C.-J., Tallutondok, E. B., & Peng, H.-J. (2022). The Dose-Response Efficacy of Physical Training on Frailty Status and Physical Performance in Community-Dwelling Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare, 10(3), 586. https://doi.org/10.3390/healthcare10030586