
Influence of Personal, Environmental, and Community Factors on Cigarette Smoking in Adolescents: A Population-Based Study from Taiwan


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.1.1. Data Source
2.1.2. Study Design
2.1.3. Study Population
2.2. Measures
2.2.1. Outcome
2.2.2. Potential Associated Factors
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Sample Characteristics
3.2. Factors Associated with Current Cigarette Smoking
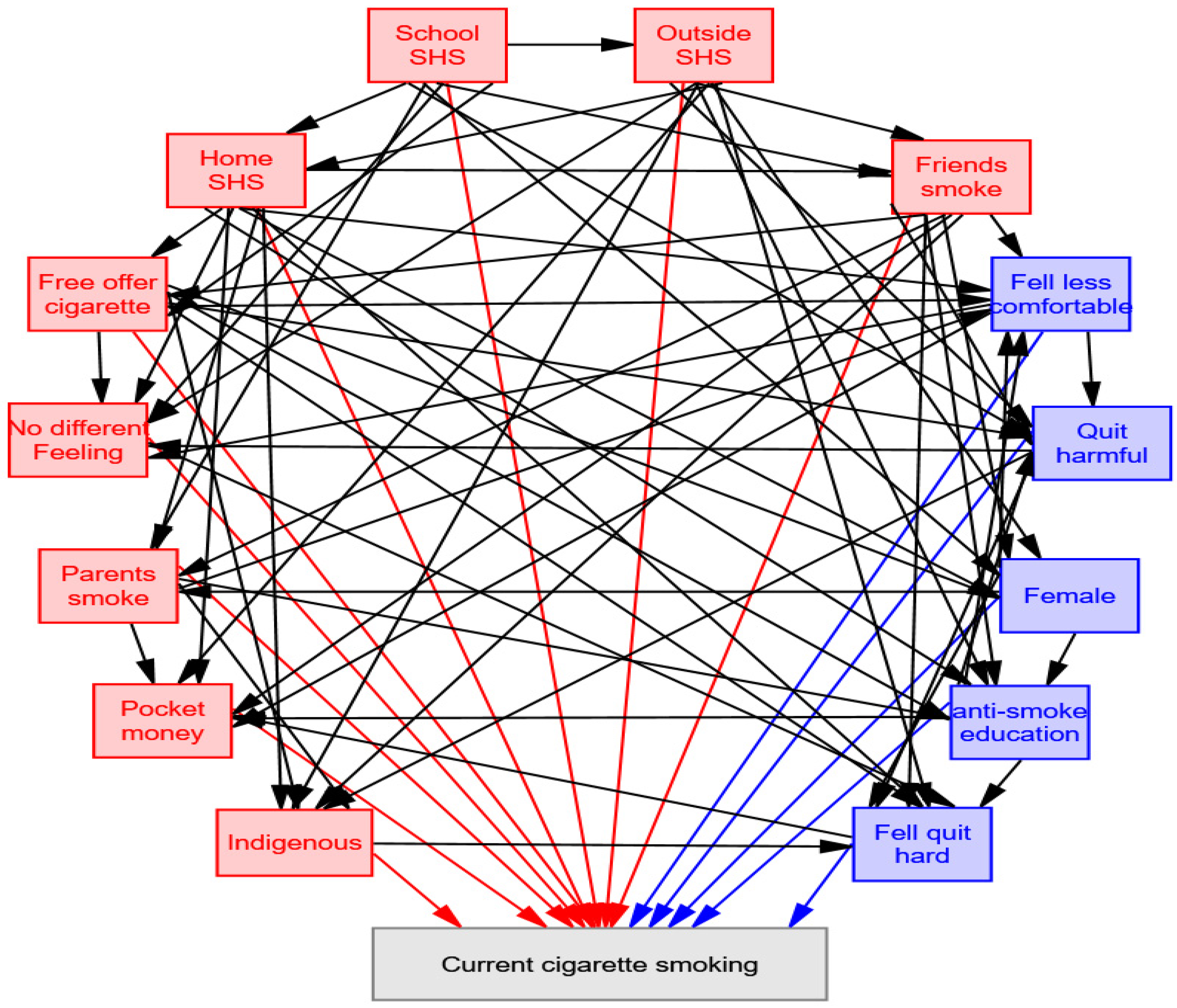
3.3. Effects of Associated Factors on Current Cigarette Smoking
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Center for Chronic Disease and Prevention; Department of Health and Human Services; Health Reports of the Surgeon General. The Health Consequences of Smoking-50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2014.
- Chiang, C.Y.; Chang, H.Y. A population study on the time trend of cigarette smoking, cessation, and exposure to secondhand smoking from 2001 to 2013 in Taiwan. Popul. Health Metr. 2016, 14, 38. [Google Scholar] [CrossRef] [PubMed]
- Tynan, M.A.; Polansky, J.R.; Driscoll, D.; Garcia, C.; Glantz, S.A. Tobacco Use in Top-Grossing Movies—United States, 2010–2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 974–978. [Google Scholar] [CrossRef]
- Nuyts, P.A.W.; Kuipers, M.A.G.; Willemsen, M.C.; Kunst, A.E. Trends in age of smoking initiation in the Netherlands: A shift towards older ages? Addiction 2018, 113, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yu, B.; Wang, Y. Initiation of Electronic Cigarette Use by Age Among Youth in the U.S. Am. J. Prev. Med. 2017, 53, 396–399. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, R.M. A new surgeon general’s report: Preventing tobacco use among adolescents and young adults. Public Health Rep. 2012, 127, 360–361. [Google Scholar] [CrossRef] [PubMed]
- Berg, C.J.; Haardorfer, R.; Vu, M.; Getachew, B.; Lloyd, S.A.; Lanier, A.; Childs, D.; Sandridge, Y.; Bierhoff, J.; Li, J.; et al. Cigarette use trajectories in young adults: Analyses of predictors across system levels. Drug Alcohol Depend. 2018, 188, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Palmer, P.; Li, Y.; Lin, C.; Johnson, C.A. Developmental trajectories of cigarette use and associations with multilayered risk factors among Chinese adolescents. Nicotine Tob. Res. 2013, 15, 1673–1681. [Google Scholar] [CrossRef]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Wongtongkam, N.; Ward, P.R.; Day, A.; Winefield, A.H. The influence of protective and risk factors in individual, peer and school domains on Thai adolescents’ alcohol and illicit drug use: A survey. Addict. Behav. 2014, 39, 1447–1451. [Google Scholar] [CrossRef]
- Cho, D.; Park, C.L. Smoking and sedentary behavior changes from adolescence to emerging adulthood: A multilevel modeling perspective. Prev. Med. 2017, 101, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Kasza, K.A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Taylor, K.; Goniewicz, M.L.; Cummings, K.M.; Sharma, E.; Pearson, J.L.; Green, V.R.; et al. Tobacco-Product Use by Adults and Youths in the United States in 2013 and 2014. N. Engl. J. Med. 2017, 376, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Creamer, M.R.; Wang, T.W.; Babb, S.; Cullen, K.A.; Day, H.; Willis, G.; Jamal, A.; Neff, L. Tobacco Product Use and Cessation Indicators Among Adults—United States, 2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1013–1019. [Google Scholar] [CrossRef]
- Lenk, K.M.; Erickson, D.J.; Forster, J.L. Trajectories of Cigarette Smoking From Teens to Young Adulthood: 2000 to 2013. Am. J. Health Promot. 2018, 32, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Forget, E.L.; Zhu, Y.; Torabi, M.; Oguzoglu, U. The effects of cigarette price and the amount of pocket money on youth smoking initiation and intensity in Canada. Can. J. Public Health. 2019, 110, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.L.; Tzeng, L.C.; Lu, K.Y.; Hsu, H.M. Factors related to tobacco use among adolescents in southern Taiwan. J. Nurs. Res. 2008, 16, 243–251. [Google Scholar] [CrossRef]
- Heydari, G.; Yousefifard, M.; Hosseini, M.; Ramezankhani, A.; Masjedi, M.R. Cigarette smoking, knowledge, attitude and prediction of smoking between male students, teachers and clergymen in tehran, iran, 2009. Int. J. Prev. Med. 2013, 4, 557–564. [Google Scholar]
- Mbongwe, B.; Tapera, R.; Phaladze, N.; Lord, A.; Zetola, N.M. Predictors of smoking among primary and secondary school students in Botswana. PLoS ONE 2017, 12, e0175640. [Google Scholar] [CrossRef] [PubMed]
- Albers, A.B.; Biener, L.; Siegel, M.; Cheng, D.M.; Rigotti, N. Household smoking bans and adolescent antismoking attitudes and smoking initiation: Findings from a longitudinal study of a Massachusetts youth cohort. Am. J. Public Health 2008, 98, 1886–1893. [Google Scholar] [CrossRef]
- Gorini, G.; Carreras, G.; Cortini, B.; Verdi, S.; Petronio, M.G.; Sestini, P.; Chellini, E. Smoke-Free Homes and Youth Smoking Behavior in Italy: Findings From the SIDRIAT Longitudinal Study. Nicotine Tob. Res. 2016, 18, 2075–2082. [Google Scholar] [CrossRef]
- Siegel, M.; Albers, A.B.; Cheng, D.M.; Hamilton, W.L.; Biener, L. Local restaurant smoking regulations and the adolescent smoking initiation process: Results of a multilevel contextual analysis among Massachusetts youth. Arch. Pediatr. Adolesc. Med. 2008, 162, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.W.; Cao, S.S.; Hu, R.Y. Smoking by family members and friends and electronic-cigarette use in adolescence: A systematic review and meta-analysis. Tob. Induc. Dis. 2018, 16, 5. [Google Scholar] [CrossRef] [PubMed]
- Kaur, J.; Kishore, J.; Kumar, M. Effect of Anti-Tobacco Audiovisual Messages on Knowledge and Attitude towards Tobacco Use in North India. Indian J. Community Med. 2012, 37, 227–231. [Google Scholar] [CrossRef]
- Liao, Y.; Huang, Z.; Huh, J.; Pentz, M.A.; Chou, C.P. Changes in friends’ and parental influences on cigarette smoking from early through late adolescence. J. Adolesc. Health 2013, 53, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Hiler, M.; Spindle, T.R.; Dick, D.; Eissenberg, T.; Breland, A.; Soule, E. Reasons for Transition From Electronic Cigarette Use to Cigarette Smoking Among Young Adult College Students. J. Adolesc. Health 2019, 66, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Kadobera, D.; Chaussard, M.; Lee, K.A.; Ayebazibwe, N.; Ndyanabangi, S. Changes in prevalence of tobacco use and the factors that may affect use among Uganda youth: The Global Youth Tobacco Survey (GYTS) 2007–2011. Pan. Afr. Med. J. 2016, 25, 152. [Google Scholar] [CrossRef] [PubMed]
- Chido-Amajuoyi, O.G.; Mantey, D.S.; Clendennen, S.L.; Perez, A. Association of tobacco advertising, promotion and sponsorship (TAPS) exposure and cigarette use among Nigerian adolescents: Implications for current practices, products and policies. BMJ Glob. Health 2017, 2, e000357. [Google Scholar] [CrossRef]
- Dawson, A.P.; Cargo, M.; Stewart, H.; Chong, A.; Daniel, M. Aboriginal health workers experience multilevel barriers to quitting smoking: A qualitative study. Int. J. Equity Health 2012, 11, 27. [Google Scholar] [CrossRef]
- Differences in worldwide tobacco use by gender: Findings from the Global Youth Tobacco Survey. J. Sch. Health 2003, 73, 207–215. [CrossRef]
- Huong, N.T.; Kien, N.T.; Giang, K.B.; Minh, H.V.; Hai, P.T.; Huyen, D.T.; Khue, L.N.; Linh, N.T.; Lam, N.T.; Nga, P.T. Knowledge and Attitude Towards Tobacco Smoking among 13–15 Year-Old School Children in Viet Nam—Findings from GYTS 2014. Asian Pac. J. Cancer Prev. 2016, 17, 37–42. [Google Scholar]
- Yan, Y.; Jacques-Tiura, A.J.; Chen, X.; Xie, N.; Chen, J.; Yang, N.; Gong, J.; Macdonell, K.K. Application of the protection motivation theory in predicting cigarette smoking among adolescents in China. Addict. Behav. 2014, 39, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Nazarzadeh, M.; Bidel, Z.; Ayubi, E.; Bahrami, A.; Jafari, F.; Mohammadpoorasl, A.; Delpisheh, A.; Taremian, F. Smoking status in Iranian male adolescents: A cross-sectional study and a meta-analysis. Addict. Behav. 2013, 38, 2214–2218. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Aslam, S.K.; Zaheer, S.; Shafique, K. Anti-smoking initiatives and current smoking among 19,643 adolescents in South Asia: Findings from the Global Youth Tobacco Survey. Harm. Reduct. J. 2014, 11, 8. [Google Scholar] [CrossRef] [PubMed]
- Tahlil, T.; Woodman, R.J.; Coveney, J.; Ward, P.R. Six-months follow-up of a cluster randomized trial of school-based smoking prevention education programs in Aceh, Indonesia. BMC Public Health 2015, 15, 1088. [Google Scholar] [CrossRef]
- Chen, L.; Chen, Y.; Hao, Y.; Gu, J.; Guo, Y.; Ling, W. Effectiveness of school-based smoking intervention in middle school students of Linzhi Tibetan and Guangzhou Han ethnicity in China. Addict. Behav. 2014, 39, 189–195. [Google Scholar] [CrossRef]
- Agaku, I.T.; Obadan, E.M.; Odukoya, O.O.; Olufajo, O. Tobacco-free schools as a core component of youth tobacco prevention programs: A secondary analysis of data from 43 countries. Eur. J. Public Health 2015, 25, 210–215. [Google Scholar] [CrossRef]
- Veeranki, S.P.; John, R.M.; Ibrahim, A.; Pillendla, D.; Thrasher, J.F.; Owusu, D.; Ouma, A.E.; Mamudu, H.M. Age of smoking initiation among adolescents in Africa. Int. J. Public Health 2017, 62, 63–72. [Google Scholar] [CrossRef]
- Global Youth Tobacco Survey (GYTS). Available online: https://www.who.int/tobacco/surveillance/gyts/en/ (accessed on 4 August 2019).
- Veeranki, S.P.; Mamudu, H.M.; Anderson, J.L.; Zheng, S. Worldwide never-smoking youth susceptibility to smoking. J. Adolesc. Health 2014, 54, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Leonardi-Bee, J.; Jere, M.L.; Britton, J. Exposure to parental and sibling smoking and the risk of smoking uptake in childhood and adolescence: A systematic review and meta-analysis. Thorax 2011, 66, 847–855. [Google Scholar] [CrossRef]
- Leshargie, C.T.; Alebel, A.; Kibret, G.D.; Birhanu, M.Y.; Mulugeta, H.; Malloy, P.; Wagnew, F.; Ewunetie, A.A.; Ketema, D.B.; Aderaw, A.; et al. The impact of peer pressure on cigarette smoking among high school and university students in Ethiopia: A systemic review and meta-analysis. PLoS ONE 2019, 14, e0222572. [Google Scholar] [CrossRef]
- Vitoria, P.; Pereira, S.E.; Muinos, G.; Vries, H.; Lima, M.L. Parents modelling, peer influence and peer selection impact on adolescent smoking behavior: A longitudinal study in two age cohorts. Addict. Behav. 2020, 100, 106131. [Google Scholar] [CrossRef] [PubMed]
- Veeranki, S.P.; Mamudu, H.M.; John, R.M.; Ouma, A.E. Prevalence and correlates of tobacco use among school-going adolescents in Madagascar. J. Epidemiol. Glob. Health 2015, 5, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Xi, B.; Liang, Y.; Liu, Y.; Yan, Y.; Zhao, M.; Ma, C.; Bovet, P. Tobacco use and second-hand smoke exposure in young adolescents aged 12–15 years: Data from 68 low-income and middle-income countries. Lancet Glob. Health 2016, 4, e795–e805. [Google Scholar] [CrossRef]
- Faber, T.; Been, J.V.; Reiss, I.K.; Mackenbach, J.P.; Sheikh, A. Smoke-free legislation and child health. NPJ Prim. Care Respir. Med. 2016, 26, 16067. [Google Scholar] [CrossRef] [PubMed]
- Tjelta, T.; Ritchie, D.; Amos, A. “It’s Easy to Get Fags”: A Qualitative Study of Disadvantaged Young People’s Perspectives on Cigarette Availability and Access. Nicotine Tob. Res. Off. J. Soc. Res. Nicotine Tob. 2017, 19, 1434–1440. [Google Scholar] [CrossRef]
- Sardana, M.; Goel, S.; Gupta, M.; Sardana, V.; Singh, B.S. Is Exposure to Tobacco Advertising, Promotion and Sponsorship Associated with Initiation of Tobacco Use among Current Tobacco Users in Youth in India? Asian Pac. J. Cancer Prev. 2015, 16, 6299–6302. [Google Scholar] [CrossRef] [PubMed]
- Lantz, P.M.; Jacobson, P.D.; Warner, K.E.; Wasserman, J.; Pollack, H.A.; Berson, J.; Ahlstrom, A. Investing in youth tobacco control: A review of smoking prevention and control strategies. Tob. Control 2000, 9, 47–63. [Google Scholar] [CrossRef]
- Hwang, J.H.; Park, S.W. Is there differential responsiveness to a future cigarette price increase depending on adolescents’ source of cigarette access? Medicine 2017, 96, e7311. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Non-Smoker | Smoker | p Value |
|---|---|---|---|
| n = 24,995 | n = 2529 | ||
| Personal factors | |||
| Gender, n (%) | |||
| Male | 11,896 (47.6) | 1816 (71.8) | <0.001 |
| Female | 13,099(52.4) | 713 (28.2) | |
| Age, n (%) | |||
| 12–15 years old | 12,571 (50.3) | 941 (37.2) | <0.001 |
| 16–18 years old | 12,424 (49.7) | 1588 (62.8) | |
| Pocket money, n (%) | |||
| none | 6065 (24.3) | 194 (7.7) | <0.001 |
| less than 500 NTD 1 | 7142 (28.6) | 445 (17.6) | |
| 500~1499 NTD 1 | 5714 (22.8) | 491 (19.4) | |
| 1500~2499 NTD 1 | 2647 (10.6) | 363 (14.4) | |
| 2500~3499 NTD 1 | 1450 (5.8) | 287 (11.3) | |
| 3500~4499 NTD 1 | 758 (3.0) | 173 (6.8) | |
| more than 4500 NTD 1 | 1219 (4.9) | 576 (22.8) | |
| Feel quitting hard, n (%) | |||
| No | 7180 (28.7) | 1054 (41.7) | <0.001 |
| Yes | 17815 (71.3) | 1475 (58.3) | |
| Feel comfortable when smoking at social occasions, n (%) | |||
| More comfortable | 1940 (7.8) | 638 (25.2) | <0.001 |
| Less comfortable | 12954 (51.8) | 580 (22.9) | |
| No difference, whether smoking or not | 10101 (40.4) | 1311 (51.9) | |
| Smoke then quit harmful, n (%) | |||
| No | 4517 (18.1) | 635 (25.1) | <0.001 |
| Yes | 20,478 (81.9) | 1894 (74.9) | |
| Feel SHS harmful, n (%) | |||
| No | 754 (3.0) | 131 (5.2) | <0.001 |
| Yes | 24,241 (97.0) | 2398 (94.8) | |
| Environmental factors | |||
| Parents’ smoking status, n (%) | |||
| None | 13,411 (53.7) | 867 (34.3) | <0.001 |
| Both | 1736 (6.9) | 465 18.4) | |
| Only father | 9464 (37.9) | 1122 (44.3) | |
| Only mother | 384 (1.5) | 75 (73.0) | |
| Friends’ smoking status, n (%) | |||
| None | 10,808 (43.2) | 57 (2.2) | <0.001 |
| Some | 13,021 (52.1) | 1375 (54.4) | |
| Most | 1077 (4.3) | 997 (39.4) | |
| All | 89 (0.4) | 100 (4.0) | |
| School anti-smoking education, n (%) | |||
| None | 3456 (13.8) | 493 (19.5) | <0.001 |
| This semester | 4769 (19.1) | 590 (23.3) | |
| The past semester | 8168 (32.7) | 757 (29.9) | |
| Two semesters ago | 4503 (18.0) | 313 (12.4) | |
| Three semesters ago | 1449 (5.8) | 118 (4.7) | |
| Two years or longer ago | 2650 (10.6) | 258 (10.2) | |
| School SHS past 7 days, n (%) | <0.001 | ||
| None | 20,890 (83.6) | 1199 (47.4) | |
| 1–2 days | 2124 (8.5) | 325 (12.9) | |
| 3–4 days | 730 (2.9) | 225 (8.9) | |
| >5 days | 1251 (5.0) | 780 (30.8) | |
| Home SHS past 7 days, n (%) | <0.001 | ||
| None | 15,492 (62.0) | 953 (37.7) | |
| 1–2 days | 2412 (9.6) | 224 (8.9) | |
| 3–4 days | 1526 (6.1) | 138 (5.4) | |
| >5 days | 5565 (22.3) | 1214 (48.0) | |
| Outside of home and school SHS past 7 days, n (%) | <0.001 | ||
| None | 8940 (35.8) | 202 (8.0) | |
| 1–2 days | 5761 (23.0) | 259 (10.2) | |
| 3–4 days | 3275 (13.1) | 300 (11.9) | |
| >5 days | 7019 (28.1) | 1768 (69.9) | |
| Community factors | |||
| where to receive free cigarettes offered by tobacco companies, n (%) | |||
| Never obtained | 24,089 (96.4) | 1927 (76.2) | <0.001 |
| Convenience store, supermarket, department store | 114 (0.5) | 96 (3.8) | |
| Tobacco sale | 54 (0.2) | 38 (1.5) | |
| Internet café | 108 (0.4) | 91 (3.6) | |
| KTV or MTV | 46 (0.2) | 69 (2.7) | |
| On the side of the road | 79 (0.3) | 42 (1.7) | |
| Wedding or funerals | 338 (1.3) | 140 (5.5) | |
| Other places | 167 (0.7) | 126 (5.0) | |
| Indigenous population, mean (95% CI) | 3.6 (3.6–3.8) | 5.7 (5.3–6.1) | <0.001 |
| Low-income population, mean (95% CI) | 1.6 (1.5–1.6) | 1.8 (1.7–1.8) | <0.001 |
| College/university, graduate population, mean (95% CI) | 85.5 (85.4–85.5) | 85.5 (85.4–8515) | 0.47 |
| Migrant population, mean (95% CI) | 3.9 (3.9–4.0) | 3.9 (3.9–4.0) | 0.83 |
| Temple density, mean (95% CI) | 0.7 (0.6–0.7) | 0.6 (0.6–0.7) | <0.001 |
| Criminal cases, mean (95% CI) | 3.8 (3.7–3.8) | 3.8 (3.7–3.8) | 0.47 |
| Fertility rate under 19 years old, mean (95% CI) | 4.6 (4.4–4.5) | 5.0 (4.9–5.0) | <0.001 |
| Divorce rate, mean (95% CI) | 2.3 (2.2–2.3) | 2.3 (2.3–2.3) | 0.003 |
| Communicable diseases, mean (95% CI) | 4.2 (4.1–4.2) | 4.2 (4.2–4.3) | 0.19 |
| Variables | Unadjusted Analysis | p Value | Adjusted Analysis | p Value |
|---|---|---|---|---|
| Odds Ratio (95% CI a) | Odds Ratio (95% CI a) | |||
| Personal factors | ||||
| Gender (female vs. male) | 0.36 (0.33–0.39) | <0.001 | 0.54 (0.48–0.60) | <0.001 |
| Age (16–18 years old vs. 13–15 years old) | 1.71 (1.57–1.86) | <0.001 | ||
| Pocket money | ||||
| Less than 500 NTD (vs. none) | 1.95 (1.64–2.31) | <0.001 | 2.12 (1.74–2.57) | <0.001 |
| 500–1499 NTD (vs. none) | 2.69 (2.27–3.18) | <0.001 | 2.30 (1.89–2.79) | <0.001 |
| 1500–2499 NTD (vs. none) | 4.29 (3.58–5.13) | <0.001 | 2.94 (2.39–3.62) | <0.001 |
| 2500–3499 NTD (vs. none) | 6.19 (5.11–7.50) | <0.001 | 3.01 (2.41–3.76) | <0.001 |
| 3500–4499 NTD (vs. none) | 7.14 (5.74–8.88) | <0.001 | 3.26 (2.52–4.22) | <0.001 |
| More than 4500 NTD (vs. none) | 14.77 (12.41–17.58) | <0.001 | 4.21 (3.43–5.18) | <0.001 |
| Feel quitting hard (yes vs. no) | 0.56 (0.52–0.61) | <0.001 | 0.65 (0.58–0.72) | <0.001 |
| Feel comfortable at social occasions | ||||
| Less comfortable (vs. more comfortable) | 0.14 (0.12–0.15) | <0.001 | 0.31 (0.26–0.35) | <0.001 |
| no difference (vs. more comfortable) | 0.40 (0.36–0.44) | <0.001 | 0.51 (0.45–0.58) | <0.001 |
| Smoked then quit harmful (yes vs. no) | 0.66 (0.60–0.72) | <0.001 | 0.82 (0.73–0.93) | 0.001 |
| Feel SHS is harmful (yes vs. no) | 0.57 (0.47–0.69) | <0.001 | ||
| Environmental factors | ||||
| Parents’ smoking status | ||||
| Both (vs. none) | 4.14 (3.66–4.69) | <0.001 | 1.65 (1.38–1.97) | <0.001 |
| Only father (vs. none) | 1.83 (1.67–2.01) | <0.001 | 1.12 (0.98–1.28) | 0.088 |
| Only mother (vs. none) | 3.02 (2.34–3.91) | <0.001 | 1.48 (1.07–2.05) | 0.019 |
| Friends’ smoking status | ||||
| Some (vs. none) | 20.02 (15.34–26.12) | <0.001 | 8.54 (6.51–11.21) | <0.001 |
| Most (vs. none) | 175.52 (133.43–230.89) | <0.001 | 36.27 (27.25–48.29) | <0.001 |
| All (vs. none) | 213.04 (144.76–313.54) | <0.001 | 30.12 (19.04–47.63) | <0.001 |
| School anti-smoking education and rules | ||||
| This semester (vs. none) | 0.87 (0.76–0.99) | 0.028 | 0.92 (0.79–1.08) | 0.335 |
| The past semester (vs. none) | 0.65 (0.58–0.73) | <0.001 | 0.82 (0.70–0.95) | 0.009 |
| Two semesters ago (vs. none) | 0.49 (0.42–0.57) | <0.001 | 0.74 (0.62–0.89) | 0.001 |
| Three semesters ago (vs. none) | 0.57 (0.46–0.70) | <0.001 | 0.80 (0.62–1.03) | 0.087 |
| Two years or longer ago (vs. none) | 0.68 (0.58–0.80) | <0.001 | 0.81 (0.67–0.99) | 0.038 |
| School SHS during the past 7 days | ||||
| 1–2 days (vs. none) | 2.67 (2.34–3.04) | <0.001 | 1.42 (1.22–1.65) | <0.001 |
| 3–4 days (vs. none) | 5.37(4.57–6.30) | <0.001 | 1.80 (1.49–2.19) | <0.001 |
| >5 days (vs. none) | 10.86 (9.76–12.09) | <0.001 | 2.37 (2.06–2.71) | <0.001 |
| Home SHS during the past 7 days | ||||
| 1–2 days (vs. none) | 1.51 (1.30–1.76) | <0.001 | 1.03 (0.85–1.25) | 0.751 |
| 3–4 days (vs. none) | 1.47 (1.22–1.77) | <0.001 | 0.89 (0.71–1.12) | 0.316 |
| >5 days (vs. none) | 3.55 (3.24–3.88) | <0.001 | 1.19 (1.03–1.37) | 0.016 |
| Outside SHS during the past 7 days | ||||
| 1–2 days (vs. none) | 1.99 (1.65–2.40) | <0.001 | 1.78 (1.45–2.18) | <0.001 |
| 3–4 days (vs. none) | 4.05 (3.38–4.87) | <0.001 | 2.60 (2.11–3.19) | <0.001 |
| >5 days (vs. none) | 11.15 (9.61–12.94) | <0.001 | 3.36 (2.82–4.00) | <0.001 |
| Community factors | ||||
| where to receive free cigarettes offeredby tobacco companies | ||||
| Convenience store, supermarket, department store (vs. never obtained) | 10.53 (7.99–13.87) | <0.001 | 3.94 (2.76–5.61) | <0.001 |
| Tobacco sale (vs. never obtained) | 8.80 (5.79–13.36) | <0.001 | 5.59 (3.26–9.59) | <0.001 |
| Internet café (vs. never obtained) | 10.53 (7.94–13.98) | <0.001 | 4.55 (3.15–6.58) | <0.001 |
| KTV or MTV (vs. never obtained) | 18.75 (12.88–27.31) | <0.001 | 4.90 (3.04–7.90) | <0.001 |
| On the side of the road (vs. never obtained) | 6.65 (4.56–9.69) | <0.001 | 3.38 (2.11–5.41) | <0.001 |
| Wedding or funerals (vs. never obtained) | 5.18 (4.23–6.34) | <0.001 | 2.32 (1.80–2.99) | <0.001 |
| Other places (vs. never obtained) | 9.43 (7.45–11.94) | <0.001 | 3.22 (2.39–4.34) | <0.001 |
| Indigenous population | 1.03 (1.02–1.03) | <0.001 | 1.01 (1.01–1.02) | <0.001 |
| Low-income population | 1.19 (1.15–1.23) | <0.001 | ||
| College/university graduate population | 0.99 (0.97–1.02) | 0.47 | ||
| Migrant population | 1.01 (0.96–1.05) | 0.836 | ||
| Temple density | 0.80 (0.74–0.86) | <0.001 | ||
| Criminal cases | 1.01 (0.98–1.04) | 0.472 | ||
| Fertility rate under 19 years old | 1.11 (1.09–1.13) | <0.001 | ||
| Divorce rate | 1.20 (1.06–1.33) | 0.003 | ||
| Communicable diseases | 1.02 (0.99–1.05) | 0.19 | ||
| Associated Factors | Direct Effect a | Indirect Effect a | Total Effect a | |
|---|---|---|---|---|
| Positive effect | ||||
| 1 | Free cigarettes offered by tobacco company (C) | 0.182 | 0.015 | 0.197 |
| 2 | Home SHS (E) | 0.153 | 0.077 | 0.230 |
| 3 | Friends smoking (E) | 0.104 | 0.069 | 0.173 |
| 4 | Pocket money (P) | 0.080 | 0.000 | 0.008 |
| 5 | Outside of home and school SHS (E) | 0.061 | 0.078 | 0.139 |
| 6 | School SHS (E) | 0.046 | 0.097 | 0.143 |
| 7 | Indigenous population (C) | 0.037 | 0.001 | 0.038 |
| 8 | Parents smoking (E) | 0.019 | 0.005 | 0.025 |
| Negative effect | ||||
| 1 | Feel less comfortable at social occasions while smoking (P) | −0.236 | −0.005 | −0.241 |
| 2 | Feel no difference whether smoking or not at social occasions (P) | −0.170 | 0.203 | 0.033 |
| 3 | Female (P) | −0.068 | −0.017 | −0.085 |
| 4 | Feel quitting is hard (P) | −0.047 | −0.001 | −0.048 |
| 5 | School anti-smoking education and rules (E) | −0.021 | 0.000 | −0.021 |
| 6 | Feel quitting after having smoked is harmful (P) | −0.015 | −0.011 | −0.026 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, Y.-C.; Liao, J.-Y.; Lee, C.T.-C.; Liu, C.-M. Influence of Personal, Environmental, and Community Factors on Cigarette Smoking in Adolescents: A Population-Based Study from Taiwan. Healthcare 2022, 10, 534. https://doi.org/10.3390/healthcare10030534
Liang Y-C, Liao J-Y, Lee CT-C, Liu C-M. Influence of Personal, Environmental, and Community Factors on Cigarette Smoking in Adolescents: A Population-Based Study from Taiwan. Healthcare. 2022; 10(3):534. https://doi.org/10.3390/healthcare10030534
Chicago/Turabian StyleLiang, Yu-Chun, Jung-Yu Liao, Charles Tzu-Chi Lee, and Chin-Mei Liu. 2022. "Influence of Personal, Environmental, and Community Factors on Cigarette Smoking in Adolescents: A Population-Based Study from Taiwan" Healthcare 10, no. 3: 534. https://doi.org/10.3390/healthcare10030534
APA StyleLiang, Y.-C., Liao, J.-Y., Lee, C. T.-C., & Liu, C.-M. (2022). Influence of Personal, Environmental, and Community Factors on Cigarette Smoking in Adolescents: A Population-Based Study from Taiwan. Healthcare, 10(3), 534. https://doi.org/10.3390/healthcare10030534