Alcohol Consumption by Italian and Spanish University Students in Relation to Adherence to the Mediterranean Diet and to the Food Neophobia: A Pilot Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Recruitment, and Data Collection
2.2. Validated Questionnaires Data Analysis
2.3. Statistical Analysis
3. Results
3.1. Participants
3.2. Consumption of Alcohol and Caffeinated Beverages
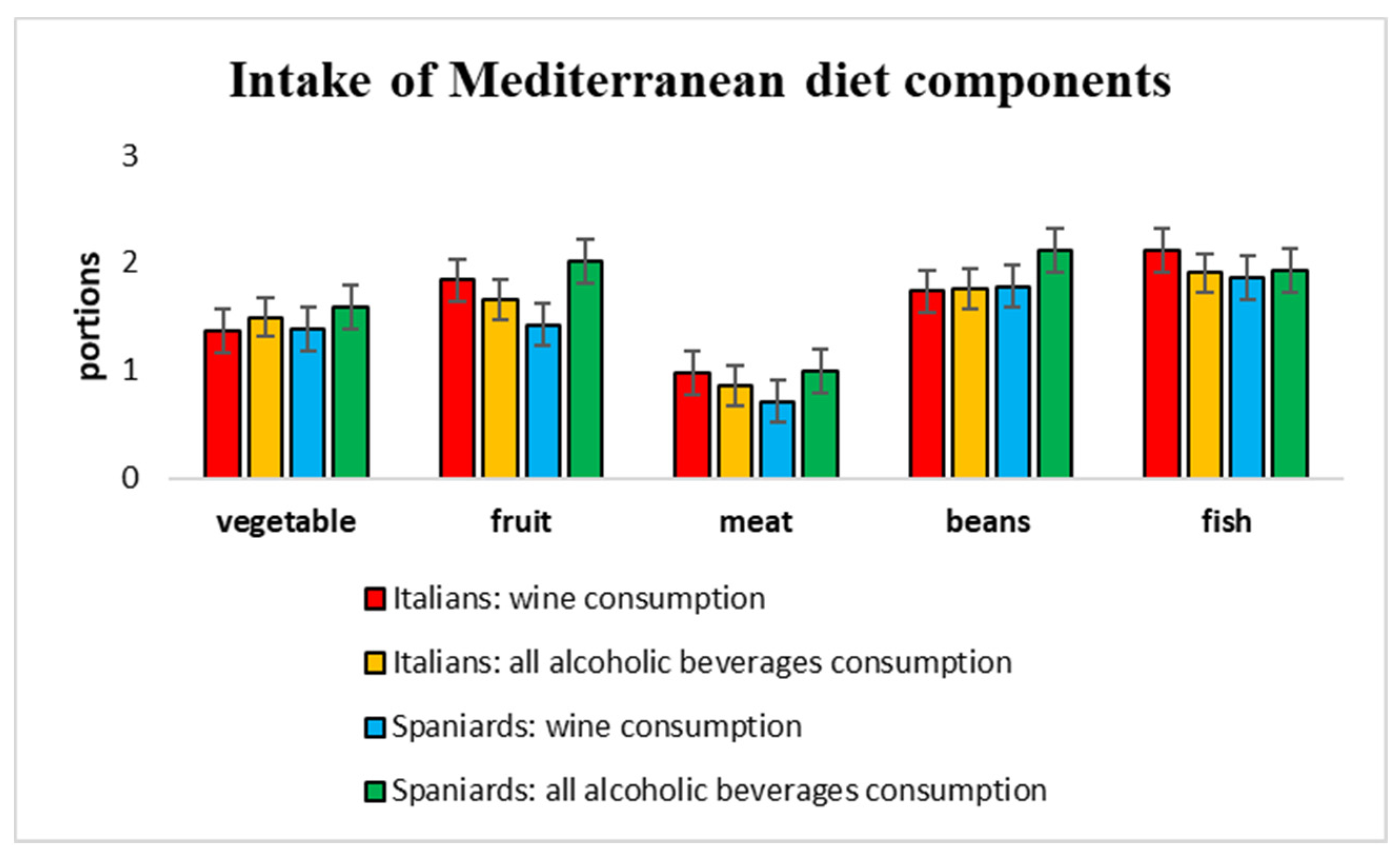
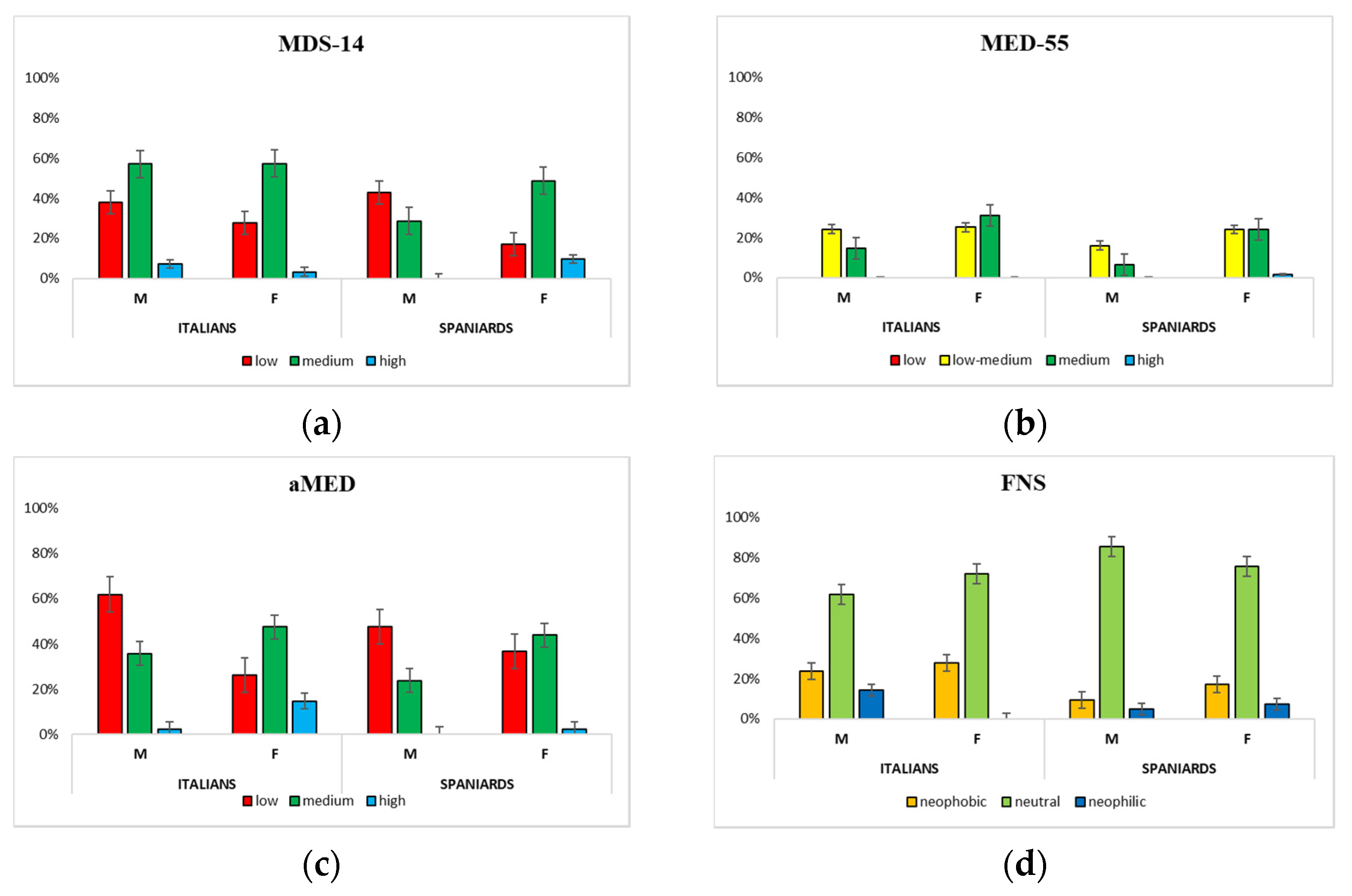
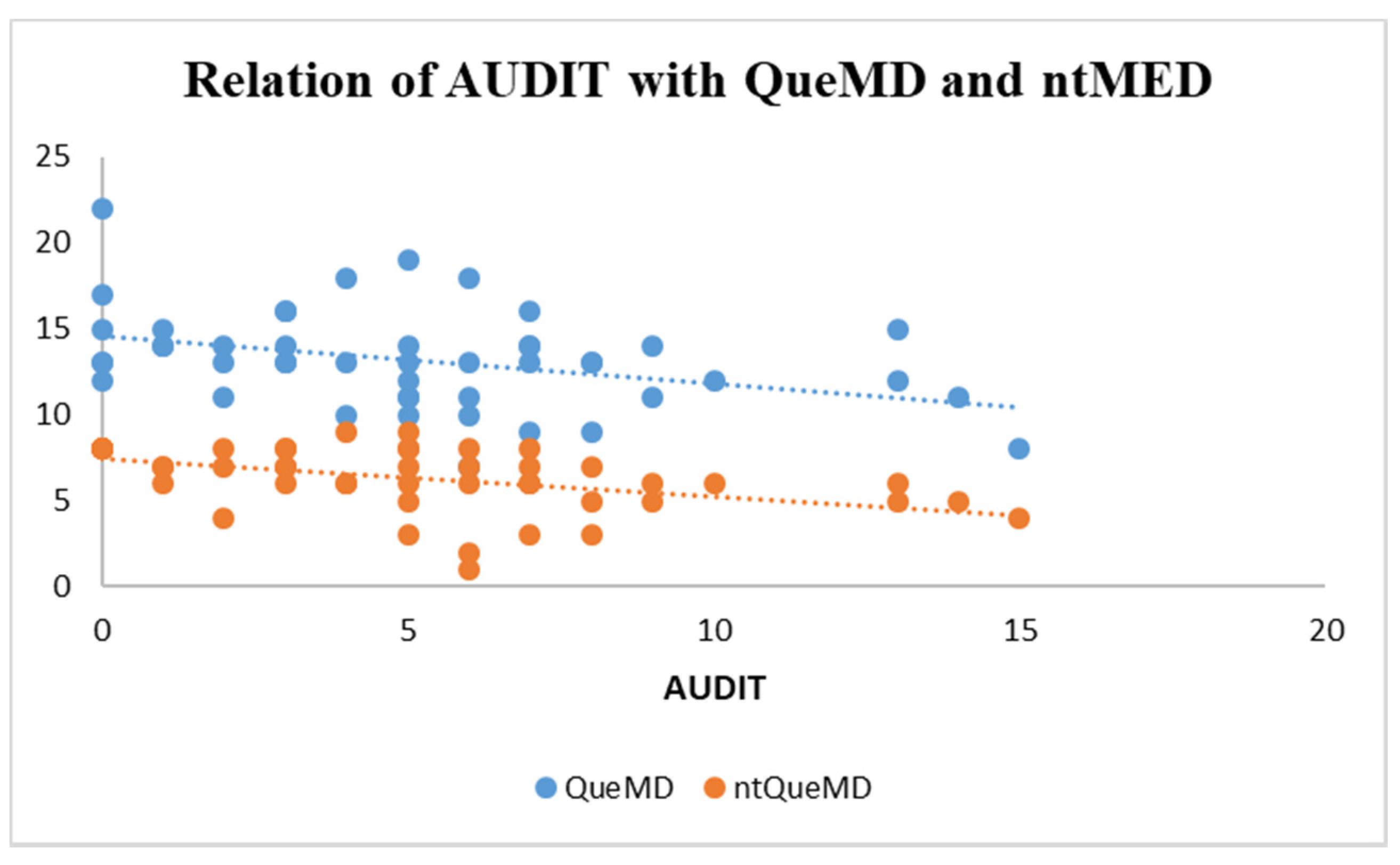
3.3. Dietary Habits and Adherence to Mediterranean Diet (MD)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- White, A.; Hingson, R. The burden of alcohol use: Excessive alcohol consumption and related consequences among college students. Alcohol. Res. 2013, 35, 201–218. [Google Scholar] [PubMed]
- Arria, A.M.; Caldeira, K.M.; Allen, H.K.; Vincent, K.B.; Bugbee, B.A.; O’Grady, K.E. Drinking Like an Adult? Trajectories of Alcohol Use Patterns Before and After College Graduation. Alcohol. Clin. Exp. Res. 2016, 40, 583–590. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Alcohol and Health. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/312318/WHO-MSD-MSB-18.2-eng.pdf (accessed on 3 November 2021).
- Ministero della Salute. Relazione del Ministro Della Salute Al Parlamento Sugli Interventi Realizzati ai Sensi della Legge 30.3.2001 n. 125 Legge Quadro in Materia di Alcol e Problemi Alcol Correlati. 2016. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2589_allegato.pdf (accessed on 3 November 2021).
- Organisation for Economic Co-Operation and Development. Tackling Harmful Alcohol Use. 2021. Available online: https://www.oecd.org/health/tackling-harmful-alcohol-use-9789264181069-en.htm (accessed on 15 January 2022).
- Yockey, R.A.; King, K.A.; Vidourek, R.A. The Epidemiology of Recent Alcohol Use Among a National Sample of Middle Eastern College Students. J. Drug Educ. 2020, 49, 30–42. [Google Scholar] [CrossRef]
- ISTAT. Il Consumo di Alcol in Italia. 2017. Available online: https://www.istat.it/it/files/2017/04/Consumo_alcol_in_Italia_2016.pdf (accessed on 4 November 2021).
- Davoren, M.P.; Cronin, M.; Perry, I.J.; O’Connor, K. Alcohol consumption among university students: A typology of consumption to aid the tailoring of effective public health policy. BMJ Open 2016, 6, e011815. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organization. Global Alcohol Report. 2016. Available online: https://www.who.int/substance_abuse/publications/global_alcohol_report/profiles/esp.pdf (accessed on 15 January 2022).
- Forouzanfar, M.H.; Alexander, L.; Anderson, H.R.; Bachman, V.F.; Biryukov, S.; Brauer, M.; Burnett, R.; Casey, D.; Coates, M.M.; Cohen, A.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–3023. [Google Scholar] [CrossRef]
- Santos-Buelga, C.; González-Manzano, S.; González-Paramás, A.M. Wine, Polyphenols, and Mediterranean Diets. What Else Is There to Say? Molecules 2021, 26, 5537. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, A.; Vecchio, R.; Mariani, A. Alcohol Warnings and Moderate Drinking Patterns among Italian University Students: An Exploratory Study. Nutrients 2017, 9, 628. [Google Scholar] [CrossRef]
- Bracale, R.; Vaccaro, C.M.; Coletta, V.; Cricelli, C.; Gamaleri, F.C.; Parazzini, F.; Carruba, M. Nutrition behaviour and compliance with the Mediterranean diet pyramid recommendations: An Italian survey-based study. Eat Weight Disord. 2020, 25, 1789–1798. [Google Scholar] [CrossRef]
- Carlos, M.; Elena, B.; Teresa, I.M. Are Adherence to the Mediterranean Diet, Emotional Eating, Alcohol Intake, and Anxiety Related in University Students in Spain? Nutrients 2020, 12, 2224. [Google Scholar] [CrossRef]
- López-Moreno, M.; Garcés-Rimón, M.; Miguel, M.; Iglesias López, M.T. Adherence to Mediterranean Diet, Alcohol Consumption and Emotional Eating in Spanish University Students. Nutrients 2021, 13, 3174. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, P.M.; Carmona-Torres, J.M.; Rivera-Picón, C.; Morales-Cané, I.; Fabbian, F.; Manfredini, R.; Rodríguez-Borrego, M.A.; López-Soto, P.J. Risky Behaviours of Spanish University Students: Association with Mediterranean Diet, Sexual Attitude and Chronotype. Nutrients 2021, 13, 4042. [Google Scholar] [CrossRef] [PubMed]
- Ramón-Arbués, E.; Granada-López, J.M.; Martínez-Abadía, B.; Echániz-Serrano, E.; Antón-Solanas, I.; Jerue, B.A. Factors Related to Diet Quality: A Cross-Sectional Study of 1055 University Students. Nutrients 2021, 13, 3512. [Google Scholar] [CrossRef] [PubMed]
- Lupi, S.; Bagordo, F.; Stefanati, A.; Grassi, T.; Piccinni, L.; Bergamini, M.; De Donno, A. Assessment of lifestyle and eating habits among undergraduate students in northern Italy. Ann. Ist. Super. Sanita. 2015, 51, 154–161. [Google Scholar] [PubMed]
- De Toffoli, A.; Spinelli, S.; Monteleone, E.; Arena, E.; Di Monaco, R.; Endrizzi, I.; Gallina Toschi, T.; Laureati, M.; Napolitano, F.; Torri, L.; et al. Influences of Psychological Traits and PROP Taster Status on Familiarity with and Choice of Phenol-Rich Foods and Beverages. Nutrients 2019, 11, 1329. [Google Scholar] [CrossRef]
- Guidetti, M.; Carraro, L.; Cavazza, N.; Roccato, M. Validation of the revised Food Neophobia Scale (FNS-R) in the Italian context. Appetite 2018, 128, 95–99. [Google Scholar] [CrossRef]
- Predieri, S.; Sinesio, F.; Monteleone, E.; Spinelli, S.; Cianciabella, M.; Daniele, G.M.; Dinnella, C.; Gasperi, F.; Endrizzi, I.; Torri, L.; et al. Gender, Age, Geographical Area, Food Neophobia and Their Relationships with the Adherence to the Mediterranean Diet: New Insights from a Large Population Cross-Sectional Study. Nutrients 2020, 12, 1778. [Google Scholar] [CrossRef]
- Rodriguez-Tadeo, A.; Patiño-Villena, B.; González Martínez-La Cuesta, E.; Urquídez-Romero, R.; Ros-Berruezo, G. Food neophobia, Mediterranean diet adherence and acceptance of healthy foods prepared in gastronomic workshops by Spanish students. Nutr. Hosp. 2018, 35, 642–649. [Google Scholar]
- Allen, J.P.; Litten, R.Z.; Fertig, J.B.; Babor, T. A review of research on the Alcohol Use Disorders Identification Test (AUDIT). Alcohol. Clin. Exp. Res. 1997, 21, 613–619. [Google Scholar] [CrossRef]
- Babor, T.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. AUDIT—The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Health Care, 2nd ed.; World Health Organisation: Geneva, Switzerland, 2001. [Google Scholar]
- Reinert, D.F.; Allen, J.P. The alcohol use disorders identification test: An update of research findings. Alcohol. Clin. Exp. Res. 2007, 31, 185–199. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Milias, G.A.; Pitsavos, C.; Stefanadis, C. MedDietScore: A computer program that evaluates the adherence to the Mediterranean dietary pattern and its relation to cardiovascular disease risk. Comput. Methods Programs Biomed. 2006, 83, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Chrysohoou, C.; Stefanadis, C.; Toutouzas, P. Risk stratification of coronary heart disease in Greece: Final results from the CARDIO2000 Epidemiological Study. Prev. Med. 2002, 35, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Gnagnarella, P.; Dragà, D.; Misotti, A.M.; Sieri, S.; Spaggiari, L.; Cassano, E.; Baldini, F.; Soldati, L.; Maisonneuve, P. Validation of a short questionnaire to record adherence to the Mediterranean diet: An Italian experience. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed]
- Teleman, A.A.; de Waure, C.; Soffiani, V.; Poscia, A.; Di Pietro, M.L. Nutritional ha-bits in Italian university students. Ann. dell’Ist. Super. Sanita. 2015, 51, 99–101. [Google Scholar]
- Travé, T.D.; Gandarias, A.C. Adherencia a la dieta Mediterránea en la población universitaria Adherence to a Mediterranean diet in a college population. Nutr. Hosp. 2011, 26, 602–608. (In Spanish) [Google Scholar]
- Organisation for Economic Co-Operation and Development. Health at a Glance: Europe. OECD. 2014. Available online: https://read.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-europe-2014_health_glance_eur-2014-en (accessed on 20 November 2021).
- Rao, M.; Afshin, A.; Singh, G.; Mozaffarian, D. Do healthier foods and diet patterns cost more than less healthy options? A systematic review and meta-analysis. BMJ Open 2013, 3, e004277. [Google Scholar] [CrossRef]
- Rehm, C.D.; Monsivais, P.; Drewnowski, A. Relation between diet cost and Healthy Eating Index 2010 scores among adults in the United States 2007–2010. Prev. Med. 2015, 73, 619. [Google Scholar] [CrossRef]
- Scholz, A.; Navarrete-Muñoz, E.M.; Garcia de la Hera, M.; Gimenez-Monzo, D.; Gonzalez-Palacios, S.; Valera-Gran, D.; Torres-Collado, L.; Vioque, J. Alcohol consumption and Mediterranean Diet adherence among health science students in Spain: The DiSA-UMH Study. Gac Sanit. 2016, 30, 126–132. [Google Scholar] [CrossRef][Green Version]
- Minzer, S.; Estruch, R.; Casas, R. Wine Intake in the Framework of a Mediterranean Diet and Chronic Non-Communicable Diseases: A Short Literature Review of the Last 5 Years. Molecules 2020, 25, 5045. [Google Scholar] [CrossRef]
- Vitiello, V.; Germani, A.; Capuzzo Dolcetta, E.; Donini, L.M.; Del Balzo, V. The New Modern Mediterranean Diet Italian Pyramid. Ann Ig 2016, 28, 179–186. [Google Scholar]
- Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2915_allegato.pdf (accessed on 21 January 2022).
- Aranceta-Bartrina, J.; Partearroyo, T.; López-Sobaler, A.M.; Ortega, R.M.; Varela-Moreiras, G.; Serra-Majem, L.; Pérez-Rodrigo, C.; The Collaborative Group for the Dietary Guidelines for the Spanish Population. Updating the Food-Based Dietary Guidelines for the Spanish Population: The Spanish Society of Community Nutrition (SENC) Proposal. Nutrients 2019, 11, 2675. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Gómez, C.; Romaguera-Bosch, D.; Tauler-Riera, P.; Bennasar-Veny, M.; Per-icas-Beltran, J.; Martinez-Andreu, S.; Aguilo-Pons, A. Clustering of lifestyle factors in Spanish university students: The relationship between smoking, alcohol consumption, phys-ical activity and diet quality. Public Health Nutr. 2012, 15, 2131–2139. [Google Scholar] [CrossRef] [PubMed]
- Wansink, B.; Cao, Y.; Saini, P.; Shimizu, M.; Just, D.R. College cafeteria snack food purchases become less healthy with each passing week of the semester. Public Health Nutr. 2013, 16, 1291–1295. [Google Scholar] [CrossRef] [PubMed]
- El Ansari, W.; Stock, C.; Mikolajczyk, R.T. Relationships between food consumption and living arrangements among university students in four European countries—A cross-sectional study. Nutr. J. 2012, 11, 28. [Google Scholar] [CrossRef]
- La Fauci, V.; Alessi, V.; Assefa, D.Z.; Lo Giudice, D.; Calimeri, S.; Ceccio, C.; Anto-nuccio, G.M.; Genovese, C.; Squeri, R. Mediterranean diet: Knowledge and adherence in Ita-lian young people. Clin. Ter. 2020, 171, e437–e443. [Google Scholar] [PubMed]
- White, H.R.; Stevens, A.K.; Hayes, K.; Jackson, K.M. Changes in Alcohol Con-sumption Among College Students Due to COVID-19: Effects of Campus Closure and Resi-dential Change. J. Stud. Alcohol. Drugs 2020, 81, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, A.E.; Kumar, S.A.; Ramirez, J.J.; DiLillo, D. Is the COVID-19 Pandemic a High-Risk Period for College Student Alcohol Use? A Comparison of Three Spring Semes-ters. Alcohol. Clin. Exp. Res. 2021, 45, 854–863. [Google Scholar] [CrossRef]
- Lechner, W.V.; Laurene, K.R.; Patel, S.; Anderson, M.; Grega, C.; Kenne, D.R. Changes in alcohol use as a function of psychological distress and social support fol-lowing COVID-19 related University closings. Addict. Behav. 2020, 110, 106527. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Italians (n = 108) | Spaniards (n = 86) | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| Sex (%) | 42.6 | 57.4 | 40.7 | 59.3 |
| Age | 26.1 ± 3.7 | 25.6 ± 3.4 | 25.3 ± 2.8 | 24.5 ± 3.7 |
| BMI | ||||
| Underweight | - | 17.7 ± 0.4 | 16.3 ± 0.0 | 17.6 ± 1.2 |
| Normal weight | 22.5 ± 1.5 | 20.9 ± 1.6 ††† | 23.2 ± 1.4 | 22.2 ± 2.0 ## |
| Overweight | 27.2 ± 1.5 | 27.1 ± 1.56 | 27.9 ± 2.4 | 27.1 ± 1.1 |
| Obese | 32.5 ± 2.2 | 33.9 ± 4.6 | - | 32.7 ± 0.0 |
| Weekday | Italians | Spaniards | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| (n = 38) | (n = 54) | (n = 20) | (n = 27) | |
| Beer (bottle 33 cl) | % | % | % | % |
| 1, 2 portions | 63.2, 5.3 | 51.9, 3.7 | 60.0, 5.0 | 48.2, 18.5 |
| 3, 4 portions | - | - | 5.0, 5.0 | 11.1, - |
| 8 portions | - | - | 3.7 | |
| Total | 68.5 | 55.6 | 75 | 81.5 |
| Wine (glass 125 mL) | % | % | % | % |
| 1, 2 portions | 47.4, 7.9 | 57.4, 11.1 | 40.0, 5.0 | 40.7, 7.4 |
| 3, 4 portions | 2.6 | - | - | -, 3.7 |
| Total | 57.9 | 68.5 | 45 | 51.8 |
| Hard liquor (glass 40 mL) | % | % | % | % |
| 1, 2 portions | 21.1, 2.6 | 24.1, - | 30.0, 5.0 | 22.2, 7.4 |
| 3, 4 portions | - | - | 5.0, - | 7.4, 3.7 |
| Total | 23.7 | 24.1 | 40 | 40.7 |
| Cocktail (glass 40 mL) | % | % | % | % |
| 1, 2 portions | 21.1, 2.6 | 35.2, 1.9 | 20.0, 5.0 | 14.8, 11.1 |
| 8 portions | - | - | - | 7.4, 3.7 |
| Total | 23.7 | 37.1 | 25 | 37 |
| Saturday night | ||||
| Beer (bottle 33 cl) | % | % | % | % |
| 1, 2 portions | 57.9, 18.4 | 35.2, 13.0 | 25.0, 10.0 | 14.8, 29.6 |
| 3, 4 portions | 5.3, - | 1.9, - | 20.0, 5.0 | 25.9, 3.7 |
| 8 portions | - | - | 5 | 3.7 |
| Total | 81.6 | 50.1 | 65 | 77.7 |
| Wine (glass 125 mL) | % | % | % | % |
| 1, 2 portions | 29.0, 21.1 | 44.4, 14.8 | 30.0, 5.0 | 22.2, 3.7 |
| 3, 4 portions | 5.3, 2.6 | 3.7, 1.9 | -- | 7.4, - |
| Total | 58 | 64.8 | 35% | 33.30% |
| Hard liquor (glass 40 mL) | % | % | % | % |
| 1, 2 portions | 36.8, 7.9 | 24.1, - | 15.0, 20.0 | 7.4, 11.1 |
| 3, 4 portions | - | - | 15.0, 5.0 | 7.4, 7.4 |
| Total | 44.7 | 24.1 | 55 | 33.3 |
| Cocktail (glass 40 mL) | % | % | % | % |
| 1, 2 portions | 29.0, 10.5 | 35.2, 7.4 | 25.0, 15.0 | -, 22.2 |
| 3, 4 portions | - | - | 5.0, - | 11.1, 3.7 |
| 8, >8 portions | - | - | - | 3.7, 3.7 |
| Total | 39.5 | 42.6 | 45 | 44.4 |
| Beverage Portions (n) | Italians | Spaniards | ||
|---|---|---|---|---|
| Weekday | Resident Students (n = 80) | Non-Resident Students (n = 12) | Resident Students (n = 31) | Non-Resident Students (n = 16) |
| Beer (bottle 33 cl) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.5) | 1.0 (1.0–2.8) |
| Wine (glass 125 mL) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.5) |
| Hard liquor (glass 40 mL) | 1.0 (1.0–1.0) ## | - | 1.0 (1.0–3.0) | 1.0 (1.0–2.0) |
| Cocktail (glass 40 mL) | 1.0 (1.0–1.0) ## | - | 1.0 (1.0–3.5) | 1.0 (1.0–2.0) |
| Saturday night | ||||
| Beer (bottle 33 cl) | 1.0 (1.0–2.0) ### | 1.0 (1.0–1.0) | 2.5 (1.3–3.0) | 2.0 (1.0–3.0) |
| Wine (glass 125 mL) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–1.3) | 1.0 (1.0–3.0) |
| Hard liquor (glass 40 mL) | 1.0 (1.0–1.0) ### | 2.0 (2.0–2.0) | 2.47 ± 1.06 | 2.00 ± 0.89 |
| Cocktail (glass 40 mL) | 1.0 (1.0–1.0) ### | 1.5 (1.0–2.0) | 2.0 (1.0–3.0) | 1.83 ± 0.75 |
| MD Components | Italians | Spaniards | ||
|---|---|---|---|---|
| Male (n = 45) % | Female (n = 62) % | Male (n = 25) % | Female (n = 48) % | |
| Vegetable | 26.7 | 48.4 | 40.0 | 47.9 |
| Fruit | 22.2 | 16.1 | 36.0 | 27.1 |
| Red meat | 40.0 | 41.9 | 20.0 | 31.3 |
| Beans | 20.0 | 22.6 | 32.0 | 31.3 |
| Fish | 31.1 | 22.6 | 32.0 | 29.2 |
| Resident students (n = 80) % | Non-resident students (n = 12) % | Resident students (n = 31) % | Non-resident students (n = 16) % | |
| Vegetable | 39.0 ## | 33.3 | 43.8 | 48.0 |
| Fruit | 19.0 ## | 16.7 | 33.3 | 24.0 |
| Red meat | 42.1 ## | 33.3 | 22.9 | 32.0 |
| Beans | 12.6 ## | 8.3 | 39.6 | 36.0 |
| Fish | 21.1 ## | 25.0 | 47.9 | 36.0 |
| Questionnaires | Italians | Spaniards | ||
|---|---|---|---|---|
| Male (n = 46) | Female (n = 62) | Male (n = 35) | Female (n = 51) | |
| FNS ** | 22.0 (15.0–27.0) | 22.0 (19.0–29.5) ## | 19.5 (14.3–22.8) | 19.0 (14.0–23.5) |
| MDS-14 | 6.0 (5.0–7.0) | 7.0 (5.0–8.0) | 7.0 (4.0–8.0) † | 7.0 (6.0–8.0) |
| MED-55 | 32.7 ± 4.5 ‡ | 34.5 ± 4.2 § | 31.4 ± 5.8 § | 33.6 ± 7.3 |
| QueMD | 13.0 ± 3.1 | 13.4 ± 2.7 | 13.3 ± 2.8 | 12.9 ± 2.8 |
| aMED * | 3.0 (2.0–5.0) | 5.0 (3.0–6.0) ††† | 3.0 (2.0–4.0) † | 4.0 (3.0–5.0) ## |
| ntMED | 6.0 (4.0–8.0) | 6.0 (4.8–8.0) | 7.0 (5.8–8.0) | 6.0 (5.0–8.0) |
| AUDIT ** | 3.0 (2.0–5.0) | 3.0 (2.0–4.0) ## | 3.5 (0.8–8.0) | 5.0 (2.5–7.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aiello, P.; Peluso, I.; Villaño Valencia, D. Alcohol Consumption by Italian and Spanish University Students in Relation to Adherence to the Mediterranean Diet and to the Food Neophobia: A Pilot Study. Healthcare 2022, 10, 393. https://doi.org/10.3390/healthcare10020393
Aiello P, Peluso I, Villaño Valencia D. Alcohol Consumption by Italian and Spanish University Students in Relation to Adherence to the Mediterranean Diet and to the Food Neophobia: A Pilot Study. Healthcare. 2022; 10(2):393. https://doi.org/10.3390/healthcare10020393
Chicago/Turabian StyleAiello, Paola, Ilaria Peluso, and Débora Villaño Valencia. 2022. "Alcohol Consumption by Italian and Spanish University Students in Relation to Adherence to the Mediterranean Diet and to the Food Neophobia: A Pilot Study" Healthcare 10, no. 2: 393. https://doi.org/10.3390/healthcare10020393
APA StyleAiello, P., Peluso, I., & Villaño Valencia, D. (2022). Alcohol Consumption by Italian and Spanish University Students in Relation to Adherence to the Mediterranean Diet and to the Food Neophobia: A Pilot Study. Healthcare, 10(2), 393. https://doi.org/10.3390/healthcare10020393