Abstract
Background: Total Hip Arthroplasty (THA) is an effective method for relieving pain and improving gait function. However, THA patients demonstrate slow gait speed at discharge. Rehabilitation programs after THA require the immediate improvement of gait speed early in the postoperative period. To examine the immediate effects of seated side tapping training (SSTT), which focuses on lateral trunk movement and movement velocity, on gait function in early postoperative THA patients, the methods were as follows: The SSTT group performed five repetitions of a task in which they moved their trunks laterally to alternately touch markers to their left and right side as quickly as possible 10 times in a seated position. One set of SSTT lasted approximately 3 min. The control group rested in a seated position for 10 min. Results: Significant interactions were observed for gait speed, stride time, and stride time coefficient of variability. The SSTT group demonstrated significant pre-post-intervention improvement in gait speed, stride time, and coefficient of variability. Conclusions: SSTT improved both gait speed and gait stability and can be performed easily and safely. Therefore, single-session high-velocity trunk training may be an effective method to improve gait function immediately in early postoperative THA patients.
1. Introduction
Total hip arthroplasty (THA) is an effective method for relieving pain and improving function, and activities of daily living [1,2]. The duration of hospitalization after THA has been shortened by the development of minimally invasive procedures, reductions in medical fees, and intensive physical therapy starting shortly after surgery [3,4]. However, THA patients demonstrate a very slow gait speed of 0.19–0.43 m/s at discharge [5] and improving gait function after THA by traditional rehabilitation programs requires a period of 6 to 12 weeks [6,7,8,9,10]. Since a gait speed of 1.0 m/s or more is necessary to live safely [11], rehabilitation programs after THA require the immediate improvement of gait speed early in the postoperative period.
Gait speed is more closely related to muscle power (strength × velocity) than muscle strength [12]. Some previous studies have indicated that high-velocity training increased muscle power in the very short term [13,14,15]. Therefore, high-velocity training of hip joint muscles might have immediate effects on gait speed in patients with THA. However, high-velocity training of the hip joint is difficult for early postoperative patients with THA due to pain or fear of movement. Seated side tapping training (SSTT), which focuses on high-velocity movement of the trunk, has been shown to improve gait speed in the early postoperative period of total knee arthroplasty (TKA) [16]. SSTT consists of side trunk movements in a seated position and does not require a great degree of hip joint motion. As trunk function is closely associated with gait function in community-dwelling older adults [17], SSTT has the potential to immediately improve gait speed for early postoperative THA patients.
As with gait speed, gait stability is an important assessment for gait function. Stride-time coefficient of variability (CV) is an indicator of gait stability and a useful predictor of fall risk [18]. The stride time CV of patients with THA one year after surgery does not improve compared to its preoperative level [19], and 36% of THA patients suffer a fall within 1 year after surgery [20]. Trunk function is critical for dynamic stability during gait [21] and the SST test primarily evaluates mobility function of the trunk. Therefore, SSTT also may improve the gait stability of THA patients.
This study aimed to examine the immediate effects of SSTT on gait function in early postoperative THA patients. The primary hypothesis was that SSTT would improve gait speed and stride time CV in patients undergoing THA. The secondary hypothesis was that SSTT does not change lower-extremity muscle strength despite improved gait function.
2. Materials and Methods
2.1. Participants
The participants were patients who underwent THA for unilateral hip osteoarthritis at a hospital between July and September 2018. In all participants, THA was performed with a direct anterior approach. Inclusion criteria were as follows: women with the ability to walk ≥20 m without assistance at measurement time, no medical or neurological diseases, and discharge on a clinical pathway (at 13 days). The study design was a quasi-randomized controlled trial. Participants were allocated into an intervention (SSTT) group or a control group in the order of the performed surgeries. Participants received an explanation of the aim of the study and provided written consent. The present study was conducted with the approval of the Institutional Review Board of university (approval no: 2018-102).
2.2. Measurement
To eliminate the effects of surgery as much as possible, immediate effects were assessed the day before discharge (post-operative day 12). The primary outcome measure was gait function, and the secondary outcome measure was lower-extremity muscle strength. Gait function and lower extremity muscle strength were measured before and after the interventions. The basic characteristics of the participants included age, height, body weight, body mass index, hip pain (visual analog scale), and Kellgren–Lawrence grade. The Kellgren–Lawrence grade was used to determine the degree of hip osteoarthritis [22]. Hip pain during gait was assessed with a visual analog scale; patients recorded their level of hip pain by drawing a vertical line between the ends of a 10 cm horizontal line [23]. Gait function was assessed by measuring comfortable gait speed, stride time, and stride time CV. Comfortable gait speed was measured on a 13 m walkway, and the initial and final 1.5 m sections were acceleration and deceleration zones. Measurement of stride time was based on a previous study; specifically, stride time was measured during a straight 20 m walk with angular rate sensors attached to affected limbs [24]. Stride time CV was calculated based on mean stride time and its standard deviation/mean × 100 (%) during the middle 15 m [25]. Comfortable gait speed and stride time were both measured twice, and the faster time of the two trials was recorded. Lower-extremity muscle strength was assessed by measuring hip abduction and knee extension using a handheld dynamometer. Hip abductor strength was measured in the supine position with both lower limbs in a neutral position [26]. The sensor pad of the handheld dynamometer was placed at the lateral femoral condyles. Knee extension strength was measured at a hip angle of 90° and with the knee flexed to 60° in the sitting position [26]. A strap was attached between the chair and a point on the patient’s ankle 5 cm above the lateral malleolus. The sensor pad was then placed at the front of the ankle under the strap to measure knee extension strength. Muscle strength measurement was performed twice, with a one-minute interval between trials, and the maximum value was used.
2.3. Interventions
The intervention was based on a previous study [16]. Figure 1 shows the movements of SSTT. Briefly, participants abducted their shoulders 90° in a seated position and moved as quickly as possible to alternately touch markers located 10 cm from their fingertips to their left and right 10 times; participants performed 5 sets of this task. The SSTT group performed a single session of SSTT. The control group rested in a seated position for 10 min.
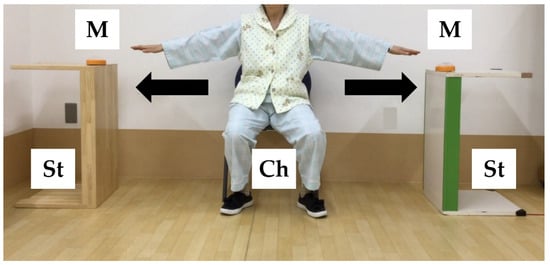
Figure 1.
Movements of seated side tapping training. M: marker (diameter, 10 cm); Ch: chair (height, 41 cm from the floor); St: stand (height, 72 cm).
2.4. Statistical Analysis
Using G*Power 3.1, we calculated the sample size with an α of 0.05 and a Power (1 − β) of 0.80 with reference to the method described by Cohen et al. [27] and the effect size as stated in a previous study [16]. We assumed a dropout rate of 20%, and the necessary sample size for the present study was calculated as 20 participants per group. Student’s t-test, the chi-square test, or the Mann–Whitney U test was used to assess for significant differences in basic characteristics between the SSTT group and the control group. Pre–post-intervention comparisons were made by 2-way ANOVA. If an interaction was observed, the Bonferroni correction was used to correct for multiple comparisons. Effect sizes were calculated for items which demonstrated a significant difference. A p-value of <0.05 was considered to be statistically significant. All data were analyzed using IBM SPSS Statistics ver. 24.0 (IBM, Armonk, NY, USA).
3. Results
3.1. Basic Characteristics
Figure 2 shows the flow diagram of the process for enrollment in this study. The final analysis set consisted of 20 participants in the SSTT group and 16 participants in the control group. The basic characteristics of both groups are shown in Table 1. The mean ages of the participants in the SSTT and control groups were 66.5 ± 7.0 years and 62.6 ± 9.1 years, respectively. The two groups did not demonstrate any significant differences in basic characteristics.
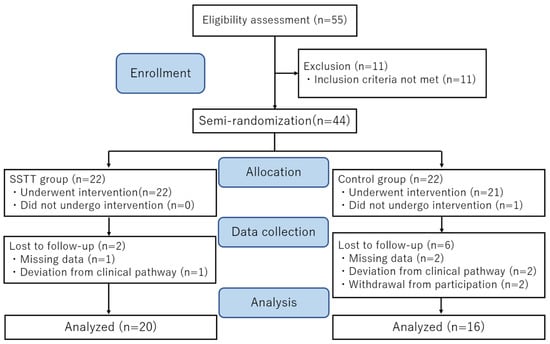
Figure 2.
CONSORT flow diagram showing the enrollment and progress of the study participants.

Table 1.
Comparison of basic characteristics between SSTT and control groups.
3.2. Gait Function and Lower Extremity Muscle Strength
In total, 95% (19/20) of participants in the SSTT group showed improved gait speed (Figure 3). Table 2 shows indicators of gait function and lower-extremity muscle strength. Interactions were observed among gait speed, stride time, and stride time CV; for all of these, the SSTT group showed significant pre–post-intervention improvement. In addition, gait speed, stride time, and stride time CV all demonstrated moderate to large effect sizes. No interaction was observed between hip abductor strength and knee extensor strength.
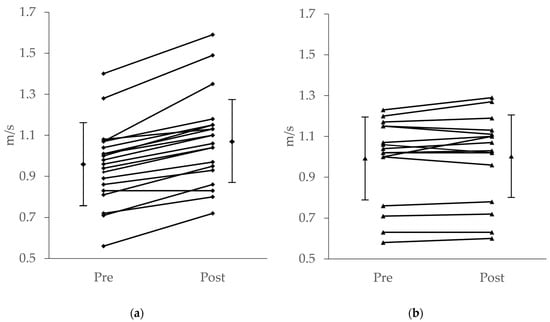
Figure 3.
Gait speed of SSTT group (a) and control group (b) before and after the intervention. Group average and standard deviation (vertical bars). Individual data (solid lines).
Table 2.
Comparison of gait function and lower extremity muscle strength between SSTT and control groups.
4. Discussion
In the present study, we aimed to examine whether a single-session SSTT, which focuses on high-velocity lateral trunk movement, immediately improves gait speed for in patients with THA. Although we observed no effect on lower-extremity muscle strength or pain, we did observe improvement in comfortable gait speed, stride time, and stride time CV. SSTT improved gait speed by 0.12 m/s. This improvement is considered a clinically relevant difference [28]. Thus, SSTT is an effective intervention for the improvement of gait speed for early postoperative THA patients.
The significant improvement in gait function of the THA patients may be mainly attributable to three factors. First, lateral trunk movement is a common determinant of gait and SSTT. Lateral trunk movement is necessary for maintaining balance during walking [17]. Similarly, quick lateral trunk movement in a seated position is related to gait speed [29]. Gait pattern in patients after THA is characterized by a lower lateral force rate and slow output of force, and this force output leads to a longer double support phase and slow gait speed [30]. Hodt-Billington et al. reported that trunk exercises in addition to the hip abductors may contribute to improving lateral stability during gait [31]. Trunk muscle exercises have been reported to improve gait speed in the elderly [32], patients with stroke [33], and patients after TKA [16]. The above suggests that SSTT, which consists of lateral movement of the trunk in a seated position, might help to improve lateral stability and gait function.
Second, movement velocity is important for gait speed. In general, increased muscle power is more closely associated with improved performance than increased muscle strength or muscle cross-sectional area [34]. Muscle power is expressed as the product of muscle strength and movement velocity. The fibers responsible for rapid contraction are selectively lost with age [35]. Muscle power is also reduced in patients undergoing THA for hip osteoarthritis, which is an age-related disease [36]. A study that focused on movement velocity found that unloaded high-velocity training yielded the same improvements in performance as conventional loaded training [37]. High-velocity training of hip muscles was also shown to improve gait speed and cadence in patients with hip osteoarthritis [38]. In the present study, SSTT was performed as quickly as possible post THA; consequently, lateral trunk movement velocity was significantly higher after the intervention. SSTT mainly focuses on the movement velocity of the trunk, and so this may have led to the improvement in gait speed.
Third, SSTT includes not only trunk movement but also hip movement. In our previous study of TKA patients, the SSTT group demonstrated a gait speed 0.11 m/s faster than that of the control group by three weeks of SSTT training [16]. We observed an immediate improvement in gait speed of 0.12 m/s in this study. Comparing the two studies, SSTT is likely to be more effective for patients undergoing THA than TKA. Based on these findings, because SSTT includes hip movements, it is considered that SSTT might improve hip movements and lead to enhancement of the speed.
On the other hand, CV—which is an indicator of gait regularity and pattern [39]—is believed to reflect adaptability to better forms of movement and reduced balance control [40]. It has been shown that CV is not improved following THA. For instance, in a previous study, CV was found to be high both preoperatively (3.3%) and at 3 months postoperative (2.8%) [18]. However, in the present study CV improved significantly from 2.3% before intervention to 1.8% after intervention. This result indicates that SSTT immediately improved not only gait speed, but also gait stability. Patients who underwent THA showed abnormal balance control, reflecting sensory and motor abnormalities [41]. SSTT, including head movement, may have contributed to sensory functions, including vestibular function [42] and improved gait stability.
The present study was limited in several ways. First, we did not evaluate trunk function during trunk training. Thus, it was unknown how the trunk function changed. Second, it assessed hip function in terms of abductor strength and did not assess other hip functions, such as range of motion and other aspects of hip muscle strength. Third, the study did not examine step length and cadence, which are determinants of gait speed, or changes in range of motion during gait, which are considered to affect stride time CV. Fourth, while SSTT demonstrated an immediate intervention effect, the absence of sufficient follow up means that the long-term effects of SSTT are unknown. It is necessary to verify the long-term effect and investigate the occurrence of possible adverse events, such as pain, if SSTT is used regularly.
5. Conclusions
In the present study, we examined the immediate effects of SSTT in early postoperative THA patients. Consequently, although there was no difference in hip pain and no improvement in muscle strength, significant improvements were observed in gait speed, stride time, and CV. These results suggest that SSTT may improve gait function immediately, easily, and safely in patients after THA.
Author Contributions
Conceptualization, K.H. and A.I.; methodology, S.Y. and A.I.; validation, Y.Y., T.O. and K.S.; formal analysis, A.K.; investigation, K.H.; data curation, H.W.; writing—original draft preparation, K.H. and A.I.; writing—review and editing, A.I.; supervision, H.O.; project administration, A.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the ethics committees of Osaka Prefecture University (approval No. 2018-102).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Data available on request due to restrictions, e.g., privacy or ethical concerns. The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors thank the study participants and their families. The authors would also like to thank all of the staff who were involved in this project.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Singh, J.A.; Lewallen, D.G. Patient-level clinically meaningful improvements in activities of daily living and pain after total hip arthroplasty: Data from a large US institutional registry. Rheumatology 2013, 52, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Vissers, M.M.; Bussmann, J.B.; Verhaar, J.A.; Arends, L.R.; Furlan, A.D.; Reijman. Recovery of physical functioning after total hip arthroplasty: Systematic review and meta-analysis of the literature. Phys. Ther. 2011, 91, 615–629. [Google Scholar] [CrossRef] [PubMed]
- Zawadsky, M.W.; Paulus, M.C.; Murray, P.J.; Johansen, M.A. Early outcome comparison between the direct anterior approach and the mini-incision posterior approach for primary total hip arthroplasty: 150 consecutive cases. J. Arthroplast. 2014, 29, 1256–1260. [Google Scholar] [CrossRef] [PubMed]
- Stambough, J.B.; Nunley, R.M.; Curry, M.C.; Steger-May, K.; Clohisy, J.C. Rapid recovery protocols for primary total hip arthroplasty can safely reduce length of stay without increasing readmissions. J. Arthroplast. 2015, 30, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Morri, M.; Natali, E.; Tosarelli, D. At discharge gait speed and independence of patients provides a challenges for rehabilitation after total joint arthroplasty: An observational study. Arch. Physiother. 2016, 29, 6. [Google Scholar] [CrossRef]
- Mahomed, N.M.; Davis, A.M.; Hawker, G.; Badley, E.; Syed, K.A.; Coyte, P.C.; Gandhi, R.; Wright, J. Inpatient compared with home-based rehabilitation following primary unilateral total hip or knee replacement: A randomized controlled trial. J. Bone Joint Surg. Am. 2008, 90, 1673–1680. [Google Scholar] [CrossRef]
- Galea, M.P.; Levinger, P.; Lythgo, N.; Cimoli, C.; Weller, R.; Tully, E.; McMeeken, J.; Westh, R. A targeted home- and center-based exercise program for people after total hip replacement: A randomized clinical trial. Arch. Phys. Med. Rehabil. 2008, 89, 1442–1447. [Google Scholar] [CrossRef]
- Jan, M.H.; Hung, J.Y.; Lin, J.C.; Wang, S.F.; Liu, T.K.; Tang, P.F. Effects of a home program on strength, walking speed, and function after total hip replacement. Arch. Phys. Med. Rehabil. 2004, 85, 1943–1951. [Google Scholar] [CrossRef]
- Unlu, E.; Eksioglu, E.; Aydog, E.; Atay, G. The effect of exercise on hip muscle strength, gait speed and cadence in patients with total hip arthroplasty: A randomized controlled study. Clin. Rehabil. 2007, 21, 706–711. [Google Scholar] [CrossRef]
- Rahmann, A.E.; Brauer, S.G.; Nitz, J.C. A specific inpatient aquatic physiotherapy program improves strength after total hip or knee replacement surgery: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2009, 90, 745–755. [Google Scholar] [CrossRef]
- Kyrdalen, I.L.; Thingstad, P.; Sandvik, L.; Ormstad, H. Associations between gait speed and well-knowen fall risk factors among community-dwelling older adults. Physiother. Res. Int. 2019, 24, e1743. [Google Scholar] [CrossRef] [PubMed]
- Cuoco, A.; Callahan, D.M.; Sayers, S.; Frontera, W.R.; Bean, J.; Fielding, B.A. Impact of muscle power and force on gait speed in disabled older men and women. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.; Whitehurst, M. The effect of short-term isokinetic training on force and rate of velocity development. J. Strength Cond. Res. 2003, 17, 88–94. [Google Scholar] [PubMed]
- Prevost, M.; Nelson, A.; Maraj, B.K. The effect of two days of velocity-specific isokinetic training on torque production. J. Strength Cond. Res. 1999, 13, 35–39. [Google Scholar]
- Coburn, J.W.; Housh, T.J.; Malek, M.H.; Weir, J.P.; Cramer, J.T.; Bec, T.W.; Johnson, G.O. Neuromuscular responses to three days of velocity-specific isokinetic training. J. Strength Cond. Res. 2006, 20, 892–898. [Google Scholar]
- Sano, Y.; Iwata, A.; Wanaka, H.; Matsui, M.; Yamamoto, S.; Koyanagi, J.; Iwata, H. An easy and safe training method for trunk function improves mobility in total knee arthroplasty patients: A quasi-randomized controlled trial. PLoS ONE 2018, 13, e0204884. [Google Scholar] [CrossRef]
- Helbostad, J.L.; Moe-Nilssen, R. The effect of gait speed on lateral barance control during walking in healthy elderly. Gait Posture 2003, 18, 27–36. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef]
- Lindemann, U.; Becker, C.; Unnewehr, I.; Muche, R.; Aminin, K.; Dejnabadi, H.; Nikolaus, T.; Puhl, W.; Huch, K.; Dreinhöfer, K.E. Gait analysis and WOMAC are complementary in assessing functional outcome in total hip replacement. Clin. Rehabil. 2006, 20, 413–420. [Google Scholar] [CrossRef]
- Ikutomo, H.; Nagai, K.; Nakagawa, N.; Masuhara, K. Falls in patients after total hip arthroplasty in Japan. J. Orthop. Sci. 2015, 20, 663–668. [Google Scholar] [CrossRef]
- Kang, H.G.; Dingwell, J.B. Dynamic stability of superior vs. inferior segments during walking in young and older adults. Gait Posture 2009, 30, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.; Huskisson, E.C. Graphic representation of pain. Pain 1976, 2, 175–184. [Google Scholar] [CrossRef]
- Salarian, A.; Russmann, H.; Vingerhoets, F.J.; Dehollain, C.; Blanc, Y.; Burkhard, P.R.; Aminian, K. Gait assessment in Parkinson’s disease: Toward an ambulatory system for long-term monitoring. IEEE Trans. Biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Dubost, V.; Aminian, K.; Gonthier, R.; Kressig, R.W. Dual-task-related gait changes in the elderly: Does the type of cognitive task matter? J. Mot. Behav. 2005, 37, 259–264. [Google Scholar]
- Hayashi, K.; Kako, M.; Suzuki, K.; Hattori, K.; Fukuyasu, S.; Sato, K.; Kadono, I.; Sakai, T.; Hasegawa, Y.; Nishida, Y. Associations among pain catastrophizing, muscle strength, and physical performance after total knee and hip arthroplasty. World J. Orthop. 2017, 8, 336–341. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Iwata, A.; Higuchi, Y.; Kimura, D.; Okamoto, K.; Arai, S.; Iwata, H.; Fuchioka, S. Quick lateral movements of the trunk in a seated position reflect mobility and activities of daily living (ADL) function in frail elderly individuals. Arch. Gerontol. Geriatr. 2013, 56, 482–486. [Google Scholar] [CrossRef]
- Perron, M.; Malouin, F.; Moffet, H.; McFadyen, B.J. Three-dimensional gait analysis in women with a total hip arthroplasty. Clin. Biomech. 2000, 15, 504–515. [Google Scholar] [CrossRef]
- Hodt-Billington, C.; Helbostad, J.L.; Vervaat, W.; Rognsvåg, T.; Moe-Nilssen, R. Changes in gait symmetry, gait velocity and self-reported function following total hip replacement. J. Rehabil. Med. 2011, 43, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.J.; Kim, J.S.; Wang, J.S.; Park, J.H.; Choi, J.H. The effects of isometric trunk exercises and dynamic trunk exercises on gait in elderly people. J. Phys. Ther. Sci. 2015, 27, 1685–1689. [Google Scholar] [CrossRef] [PubMed]
- Karthikbabu, S.; Rao, B.K.; Manikandan, N.; Solomon, J.M.; Chakrapani, M.; Nayak, A. Role of Trunk Rehabilitation on Trunk Control, Balance and Gait in Patients with Chronic Stroke: A Pre-Post Design. Neurosci. Med. 2011, 2, 61–67. [Google Scholar] [CrossRef]
- McKinnon, N.B.; Connelly, D.M.; Rice, C.L.; Hunter, S.W.; Doherty, T.J. Neuromuscular contributions to the age-related reduction in muscle power: Mechanisms and potential role of high velocity power training. Ageing Res. Rev. 2017, 35, 147–154. [Google Scholar] [CrossRef]
- Mosole, S.; Carraro, U.; Kern, H.; Loefler, S.; Fruhmann, H.; Vogelauer, M.; Burggraf, S.; Mayr, W.; Krenn, M.; Paternostro-Sluga, T.L.; et al. Long-term high-level exercise promotes muscle reinnervation with age. J. Neuropathol. Exp. Neurol. 2014, 73, 284–294. [Google Scholar] [CrossRef]
- Friesenbichler, B.; Casartelli, N.C.; Wellauer, V.; Item-Glatthorn, J.F.; Ferguson, S.T.; Leunig, M.; Maffiuletti, N.A. Explosive and maximal strength before and 6 months after total hip arthroplasty. J. Orthop. Res. 2017, 36, 425–431. [Google Scholar]
- Glenn, J.M.; Gray, M.; Binns, A. The effects of loaded and unloaded high-velocity resistance training on functional fitness among community-dwelling older adults. Age Ageing 2015, 44, 926–931. [Google Scholar] [CrossRef][Green Version]
- Fukumoto, Y.; Tateuchi, H.; Tsukagoshi, R.; Okita, Y.; Akiyama, H.; So, K.; Kuroda, Y.; Ichihashi, N. Effects of High- and Low-Velocity Resistance Training on Gait Kinematics and Kinetics in Individuals with Hip Osteoarthritis: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2017, 96, 417–423. [Google Scholar] [CrossRef]
- Gabell, A.; Nayak, U.S. The effect of age on variability in gait. J. Gerontol. 1984, 39, 662–666. [Google Scholar] [CrossRef]
- Moe-Nilssen, R.; Helbostad, J.L. Estimation of gait cycle characteristics by trunk accelerometry. J. Biomech. 2004, 37, 121–126. [Google Scholar] [CrossRef]
- Labanca, L.; Ciardulli, F.; Bonsanto, F.; Sommella, N.; Martino, A.D.; Benedetti, M.G. Balance and proprioception impairment, assessment tools, and rehabilitation training in patients with total hip arthroplasty: A systematic review. BMC Musculoskelet. Disord. 2021, 22, 1055. [Google Scholar] [CrossRef] [PubMed]
- Schweigart, G.; Chien, R.D.; Mergner, T. Neck proprioception compensates for age-related deterioration of vestibular self-motion perception. Exp. Brain Res. 2002, 147, 89–97. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).