
User Engagement and Abandonment of mHealth: A Cross-Sectional Survey

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Items
2.2. Survey Participants
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
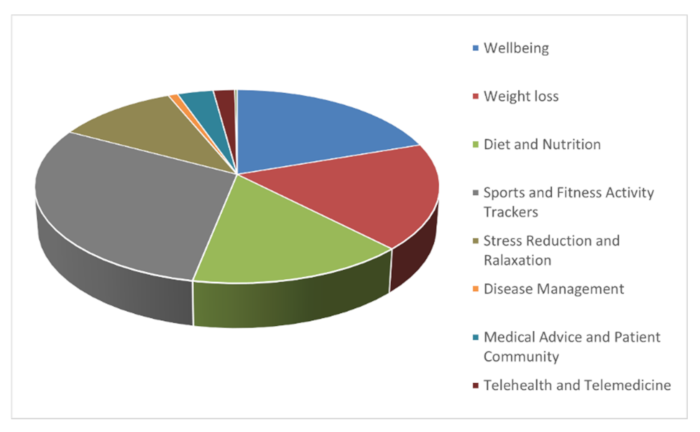
3.2. Characterizing Popular mHealth Apps
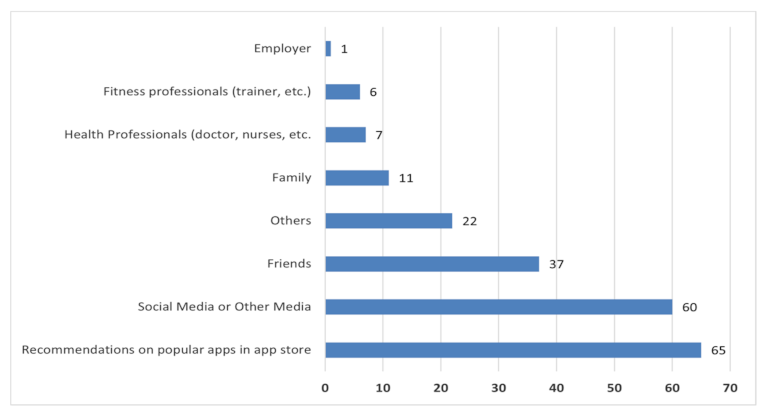
3.3. mHealth App Adoption
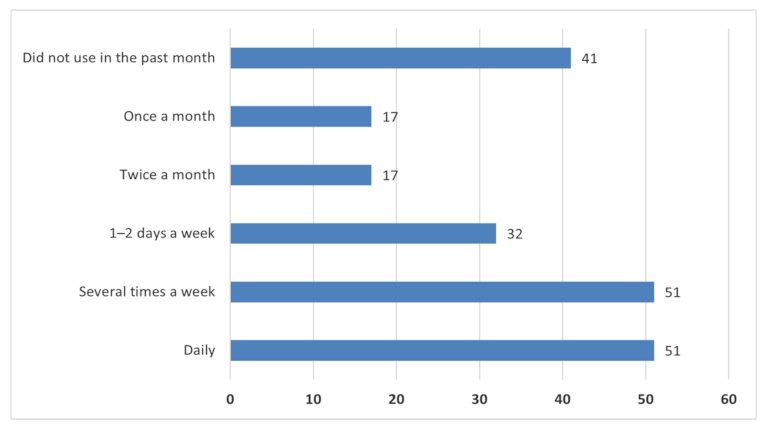
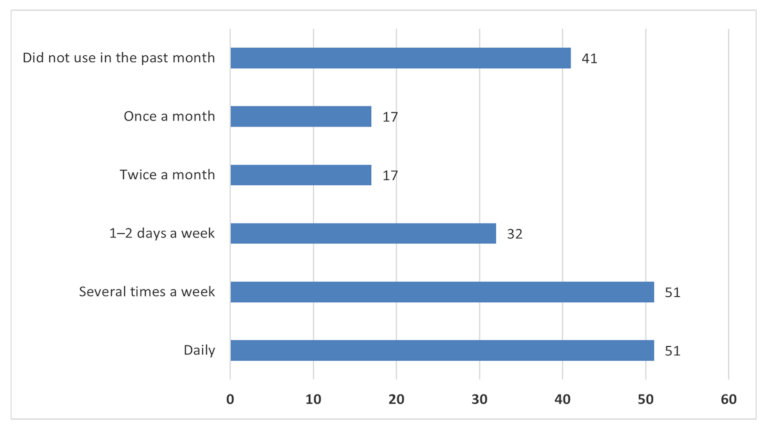
3.4. mHealth App Use
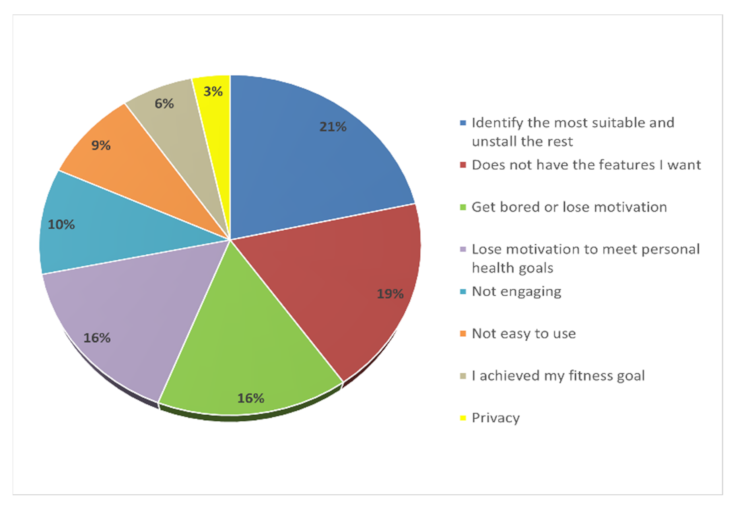
3.5. mHealth App Abandonment
3.6. Fitness App Motivation
3.7. Heavy vs. Light Fitness-App Users
- “More simplified, sometimes there’s too many things going on and too many things to track.”
- “Add personalized experiences and feedback”
- “I wish that more of them are free. Or at least less costly. As a student, I don’t really have the money to buy a subscription”
- “Add notifications and measure progress”
- “The thing that lacks in the existing apps is the motivation, it would be perfect to have something that will encourage to continue doing exercise and following the milestones without a break. For now, it is like I use an app for 1, 2, 3 days and then I lose my motivation to do exercise using app.”
4. Discussion
Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marston, H.R.; Hall, A.K. Gamification: Applications for health promotion and health information technology engagement. In Handbook of Research on Holistic Perspectives in Gamification for Clinical Practice Hershey; Novak, D., Tulu, B., Brendryen, H., Eds.; IGI Global: Hershey, PA, USA, 2015; pp. 78–104. [Google Scholar] [CrossRef]
- Aslam, A.S.; van Luenen, S.; Aslam, S.; van Bodegom, D.; Chavannes, N.H. A systematic review on the use of mHealth to increase physical activity in older people. Clin. eHealth 2020, 3, 31–39. [Google Scholar] [CrossRef]
- Xie, Z.; Nacioglu, A.; Or, C. Prevalence, Demographic Correlates, and Perceived Impacts of Mobile Health App Use Amongst Chinese Adults: Cross-Sectional Survey Study. JMIR mHealth uHealth 2018, 6, e103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.; Lou, M. Effects of mHealth-based interventions on health literacy and related factors: A systematic review. J. Nurs. Manag. 2020, 29, 385–394. [Google Scholar] [CrossRef]
- Rowland, S.P.; Fitzgerald, J.E.; Holme, T.; Powell, J.; McGregor, A. What is the clinical value of mHealth for patients? NPJ Digit. Med. 2020, 3, 4. [Google Scholar] [CrossRef]
- Liang, X.; Wang, Q.; Yang, X.; Cao, J.; Chen, J.; Mo, X.; Huang, J.; Wang, L.; Gu, D. Effect of mobile phone intervention for diabetes on glycaemic control: A meta-analysis. Diabet. Med. 2010, 28, 455–463. [Google Scholar] [CrossRef]
- Yoganathan, D.; Kajanan, S. What Drives Fitness Apps Usage? An Empirical Evaluation. In IFIP Advances in Information and Communication Technology; Springer: Berlin/Heidelberg, Germany, 2014; Volume 429, pp. 179–196. [Google Scholar] [CrossRef] [Green Version]
- Deterding, S.; Dixon, D.; Khaled, R.; Nacke, L. From Game Design Elements to Gamefulness: Defining ‘gamification’. In Proceedings of the International Academic MindTrek Conference: Envisioning Future Media Environments, Tampere, Finland, 28–30 September 2011; pp. 9–15. [Google Scholar] [CrossRef]
- Sailer, M.; Sailer, M. Gamification of in-class activities in flipped classroom lectures. Br. J. Educ. Technol. 2021, 52, 75–90. [Google Scholar] [CrossRef]
- Vanduhe, H.F.; Nat, V.Z.; Hasan, M. Continuance Intentions to Use Gamification for Training in Higher Education: Integrating the Technology Acceptance Model (TAM), Social Motivation, and Task Technology Fit (TTF). IEEE Access 2020, 8, 21473–21484. Available online: https://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=8957115 (accessed on 1 May 2021). [CrossRef]
- Patel, M.S.; Small, D.S.; Harrison, J.D.; Hilbert, V.; Fortunato, M.P.; Oon, A.L.; Rareshide, C.A.L.; Volpp, K.G. Effect of Behaviorally Designed Gamification with Social Incentives on Lifestyle Modification among Adults with Uncontrolled Diabetes: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2110255. [Google Scholar] [CrossRef] [PubMed]
- Corepal, R.; Best, P.; O’Neill, R.; Tully, M.A.; Edwards, M.; Jago, R.; Miller, S.J.; Kee, F.; Hunter, R.F. Exploring the use of a gamified intervention for encouraging physical activity in adolescents: A qualitative longitudinal study in Northern Ireland. BMJ Open 2018, 8, e019663. [Google Scholar] [CrossRef]
- Lee, A.M.; Chavez, S.; Bian, J.; Thompson, L.A.; Gurka, M.J.; Williamson, V.G.; Modave, F. Efficacy and Effectiveness of Mobile Health Technologies for Facilitating Physical Activity in Adolescents: Scoping Review. JMIR mHealth uHealth 2019, 7, e11847. [Google Scholar] [CrossRef]
- Swiatczak, M.D. Towards a neo-configurational theory of intrinsic motivation. Motiv. Emot. 2021, 45, 769–789. [Google Scholar] [CrossRef]
- Bai, S.; Hew, K.F.; Huang, B. Does gamification improve student learning outcome? Evidence from a meta-analysis and synthesis of qualitative data in educational contexts. Educ. Res. Rev. 2020, 30, 100322. [Google Scholar] [CrossRef]
- Priesterroth, L.; Grammes, J.; Holtz, K.; Reinwarth, A.; Kubiak, T. Gamification and Behavior Change Techniques in Diabetes Self-Management Apps. J. Diabetes Sci. Technol. 2019, 13, 954–958. [Google Scholar] [CrossRef] [PubMed]
- Mora-Gonzalez, J.; Pérez-López, I.J.; Esteban-Cornejo, I.; Delgado-Fernández, M. A Gamification-Based Intervention Program that Encourages Physical Activity Improves Cardiorespiratory Fitness of College Students: ‘The Matrix Refvolution Program’. Int. J. Environ. Res. Public Health 2020, 17, 877. [Google Scholar] [CrossRef] [Green Version]
- Johnson, D.; Deterding, S.; Kuhn, K.-A.; Staneva, A.; Stoyanov, S.; Hides, L. Gamification for health and wellbeing: A systematic review of the literature. Internet Interv. 2016, 6, 89–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murnane, E.L.; Huffaker, D.; Kossinets, G. Mobile health apps: Adoption, adherence, and abandonment. In Proceedings of the UbiComp/ISWC’15 Adjunct: Adjunct Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2015 ACM International Symposium on Wearable Computers, Osaka, Japan, 7–11 September 2015; pp. 261–264. [Google Scholar] [CrossRef]
- Huang, G.; Ren, Y. Linking technological functions of fitness mobile apps with continuance usage among Chinese users: Moderating role of exercise self-efficacy. Comput. Hum. Behav. 2020, 103, 151–160. [Google Scholar] [CrossRef]
- Armstrong, J.S.; Overton, T.S. Estimating Nonresponse Bias in Mail Surveys. J. Mark. Res. 1977, 14, 396. [Google Scholar] [CrossRef] [Green Version]
- Naimark, J.S.; Madar, Z.; Shahar, D.R.; Pojednic, R.; Janwantanakul, P. The Impact of a Web-Based App (eBalance) in Promoting Healthy Lifestyles: Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e56. [Google Scholar] [CrossRef] [Green Version]
- Deng, T.; Kanthawala, S.; Meng, J.; Peng, W.; Kononova, A.; Hao, Q.; Zhang, Q.; David, P. Measuring smartphone usage and task switching with log tracking and self-reports. Mob. Media Commun. 2019, 7, 3–23. [Google Scholar] [CrossRef]
- Sharma, S.; Kumar, R.; Krishna, C.R. A survey on analysis and detection of Android ransomware. Concurr. Comput. Pract. Exp. 2021, 33, e6272. [Google Scholar] [CrossRef]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Munson, S.; Consolvo, S. Exploring Goal-setting, Rewards, Self-monitoring, and Sharing to Motivate Physical Activity. In Proceedings of the 2012 6th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth) and Workshops, San Diego, CA, USA, 21–24 May 2012; pp. 25–32. [Google Scholar] [CrossRef] [Green Version]
- Ali, N.; Tretiakov, A.; Whiddett, D.; Hunter, I. Knowledge management systems success in healthcare: Leadership matters. Int. J. Med. Inform. 2016, 97, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Shani, R.; Omer, F. The Uninstall Threat: 2020 App Uninstall Benchmarks; AppsFlyer Ltd: Berlin, Germany, 2021; Available online: https://www.appsflyer.com/resources/reports/app-uninstall-benchmarks/ (accessed on 20 August 2021).
- Attig, C.; Franke, T. I Track, therefore I walk–Exploring the motivational costs of wearing activity trackers in actual users. Int. J. Hum. Comput. Stud. 2019, 127, 211–224. [Google Scholar] [CrossRef]
- Krebs, P.; Duncan, D.T. Health App Use among US Mobile Phone Owners: A National Survey. JMIR mHealth uHealth 2015, 3, e101. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Kraepelin, M.; Thiebes, S.; Stepanovic, S.; Mettler, T.; Sunyaev, A. Gamification in Health Behavior Change Support Systems A Synthesis of Unintended Side Effects. In Proceedings of the 14th International Conference on Wirtschaftsinformatik, Siegen, Germany, 24–27 February 2019; pp. 1032–1046. [Google Scholar]
- Hoffmann, A.; Christmann, A.C.; Bleser, G. Gamification in Stress Management Apps: A Critical App Review. JMIR Serious Games 2017, 5, e13. [Google Scholar] [CrossRef]
- König, L.M.; Attig, C.; Franke, T.; Renner, B. Barriers to and Facilitators for Using Nutrition Apps: Systematic Review and Conceptual Framework. JMIR mHealth uHealth 2021, 9, e20037. [Google Scholar] [CrossRef]
- Peng, W.; Kanthawala, S.; Yuan, S.; Hussain, S.A. A qualitative study of user perceptions of mobile health apps. BMC Public Health 2016, 16, 1158. [Google Scholar] [CrossRef] [Green Version]
- Mikulic, M. mHealth–Statistics & Facts; Statista: London, UK, 2020. [Google Scholar]
- Askari, M.; Klaver, N.S.; van Gestel, T.J.; van de Klundert, J. Intention to use Medical Apps Among Older Adults in the Netherlands: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e18080. [Google Scholar] [CrossRef]
- LaMonica, H.M.; Roberts, A.E.; Davenport, T.A.; Hickie, I.B. Evaluation of the Usability and Acceptability of the InnoWell Platform as Rated by Older Adults: Survey Study. JMIR Aging 2021, 4, e25928. [Google Scholar] [CrossRef] [PubMed]
- Kirkscey, R. mHealth Apps for Older Adults: A Method for Development and User Experience Design Evaluation. J. Tech. Writ. Commun. 2021, 51, 199–217. [Google Scholar] [CrossRef]
- Herrmann, L.K.; Kim, J. The fitness of apps: A theory-based examination of mobile fitness app usage over 5 months. mHealth 2017, 3, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsay, C.H.; Kofinas, A.K.; Trivedi, S.K.; Yang, Y. Overcoming the novelty effect in online gamified learning systems: An empirical evaluation of student engagement and performance. J. Comput. Assist. Learn. 2019, 36, 128–146. [Google Scholar] [CrossRef]
- Honary, M.; Bell, B.T.; Clinch, S.; Wild, S.E.; McNaney, R. Understanding the Role of Healthy Eating and Fitness Mobile Apps in the Formation of Maladaptive Eating and Exercise Behaviors in Young People. JMIR mHealth uHealth 2019, 7, e14239. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, A.S.; Ali, N.; Dhillon, J.S. A Systematic Review of the Integration of Motivational and Behavioural Theories in Game-Based Health Interventions. In Innovative Systems for Intelligent Health Informatics; Springer: Cham, Switzerland, 2021; Volume 7. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Measurements |
|---|---|
| Sociodemographic | What is your Gender? |
| What is your Age? | |
| Types of mHealth used and desired features | Which Smartphone Operating System (OS) do you use? |
| What kind of health and wellness apps have you downloaded over the past 12 months? | |
| How many health and fitness apps have you used over the last 12 months? | |
| What are the most important features for you in the health and fitness app? | |
| Adoption | What is the name of the health and fitness app that you use? |
| How do you usually know about the health and fitness apps you install on your phone? | |
| Adherence | What is the main reason you use health or fitness apps? |
| How often do you use a health and fitness app in a month? | |
| What is the main source of encouragement that you receive to use health and fitness apps? | |
| How many hours do you spend each day on your smartphone? | |
| Discontinued use | If you could change anything about the fitness apps you are using, what would it be? |
| Which of these better explains why you stop using the health and fitness apps? | |
| Motivational affordances | Using a health and fitness apps motivates me to exercise more. |
| Using a health and fitness apps motivates me to eat healthier. | |
| Using a health and fitness apps helps me to keep track of my goals. |
| Classification of User | Usage Frequency |
|---|---|
| Heavy user | Daily |
| Several times a day | |
| 1–2 days a week | |
| Light user | Twice a month |
| Once a month | |
| Did not use in the past month |
| App | Description | No. of Users | % |
|---|---|---|---|
| MyFitnessPal | Weight loss, calorie counter, and dieting app | 31 | 14.8 |
| Fitbit Health & Fitness | All-day activity, workouts, and sleep-tracking app | 15 | 7.2 |
| Nike Run Club & Training | Running app with GPS-guided run and challenges | 15 | 7.2 |
| Samsung Health | Supports healthier lifestyle, tacks sleep, dieting, and exercise | 15 | 7.2 |
| Strava | App tracking cycling and running with GPS and social networking | 12 | 5.7 |
| Leap Fitness | Full-body workout app | 9 | 4.3 |
| Life Sum Fitness | Personalized dieting, exercise, and calorie-tracking app | 8 | 3.8 |
| Apple Health | Workout, sleep, steps, and all-day activity-tracking app | 7 | 3.3 |
| Flo Fit | Women’s health and fitness and period-tracker app | 7 | 3.3 |
| Calm App | Meditation, sleep, and relaxation app | 6 | 2.9 |
| Themes Identified | Taxonomy |
|---|---|
| Cost (More affordable or free) | - |
| Less in-app advertising | - |
| Additional food and dieting options | BCT |
| More personalized (customization) | BCT, GT |
| Game-like features (combination of game elements) | GT |
| Use of leader board | GT |
| Increasing challenges | GT |
| Level of difficulty (levels) | GT |
| Social relatedness | GT |
| Improving motivation | BCT, GT |
| Syncing with other devices | GT |
| Improving user experience | BCT, GT |
| Goal-oriented (achievement) | BCT, GT |
| Quality of feedback (feedback) | BCT, GT |
| Characteristics | Heavy Users n = 51 | Light Users n = 41 |
|---|---|---|
| Male | 22 (43%) | 21 (51%) |
| Female | 29 (57%) | 20 (49%) |
| 18–25 age group | 19 | 12 |
| 26–35 age group | 20 | 20 |
| 36–46 age group | 11 | 8 |
| Android OS | 31 | 21 |
| Apple iOS | 20 | 20 |
| Popular category of fitness apps downloaded | Sports and fitness Wellbeing Diet Weight loss | Sports and Fitness Wellbeing Diet Weight loss |
| Popular fitness apps | MyFitnessPal, Fitbit, Samsung Health, and Strava. | MyFitnessPal, Samsung Health, Strava, Calm, and 30-day fitness at home. |
| Most important app features | Personalization, food tracker, game-like features, feedback | Personalization, game-like features, notifications, feedback |
| Primary motivation for engaging with fitness apps | To maintain or lose weight. To maintain or improve my level of physical fitness. To positively change my lifestyle or improve my quality of life. | To positively change my lifestyle or improve my quality of life. To maintain or lose weight. To maintain or improve my level of physical fitness. |
| Reasons for abandoning fitness apps | - | Not enjoyable. Does not have the features that I want. Bored or/and lose motivation. Does not meet their demand. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mustafa, A.S.; Ali, N.; Dhillon, J.S.; Alkawsi, G.; Baashar, Y. User Engagement and Abandonment of mHealth: A Cross-Sectional Survey. Healthcare 2022, 10, 221. https://doi.org/10.3390/healthcare10020221
Mustafa AS, Ali N, Dhillon JS, Alkawsi G, Baashar Y. User Engagement and Abandonment of mHealth: A Cross-Sectional Survey. Healthcare. 2022; 10(2):221. https://doi.org/10.3390/healthcare10020221
Chicago/Turabian StyleMustafa, Abdulsalam Salihu, Nor’ashikin Ali, Jaspaljeet Singh Dhillon, Gamal Alkawsi, and Yahia Baashar. 2022. "User Engagement and Abandonment of mHealth: A Cross-Sectional Survey" Healthcare 10, no. 2: 221. https://doi.org/10.3390/healthcare10020221
APA StyleMustafa, A. S., Ali, N., Dhillon, J. S., Alkawsi, G., & Baashar, Y. (2022). User Engagement and Abandonment of mHealth: A Cross-Sectional Survey. Healthcare, 10(2), 221. https://doi.org/10.3390/healthcare10020221