
Disparities in Health Financing Allocation among Infectious Diseases in Ebola Virus Disease (EVD)-Affected Countries, 2005–2017


Abstract
1. Introduction
2. Materials and Methods
2.1. Selected Countries and Study Period
2.2. Data
2.3. Data Analysis
3. Results
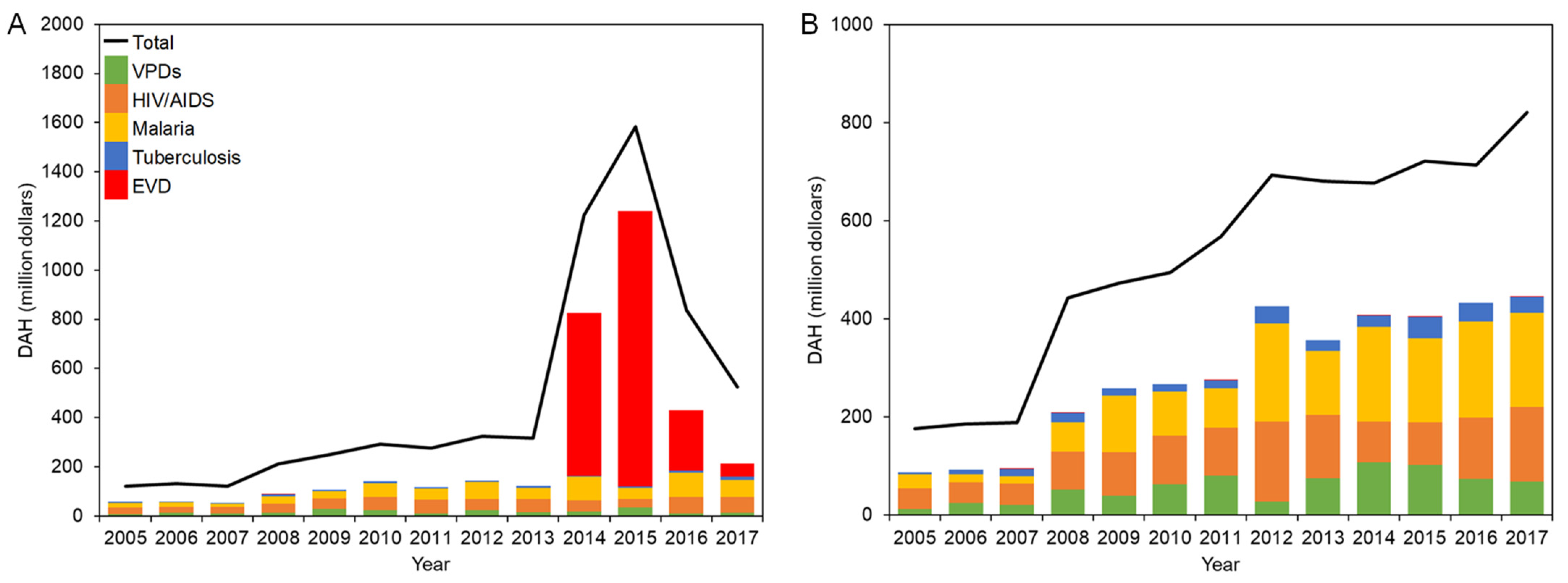
3.1. DAH for EVD-Affected Countries
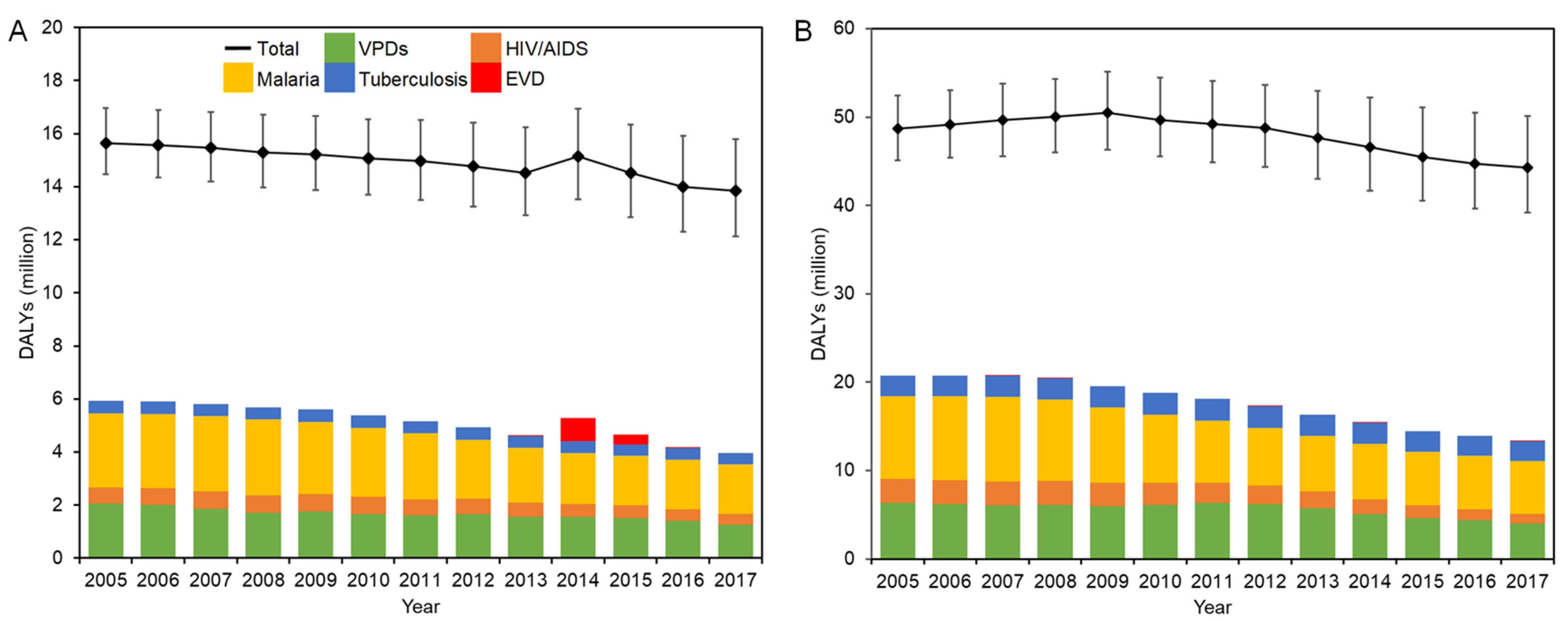
3.2. DALYs in EVD-Affected Countries
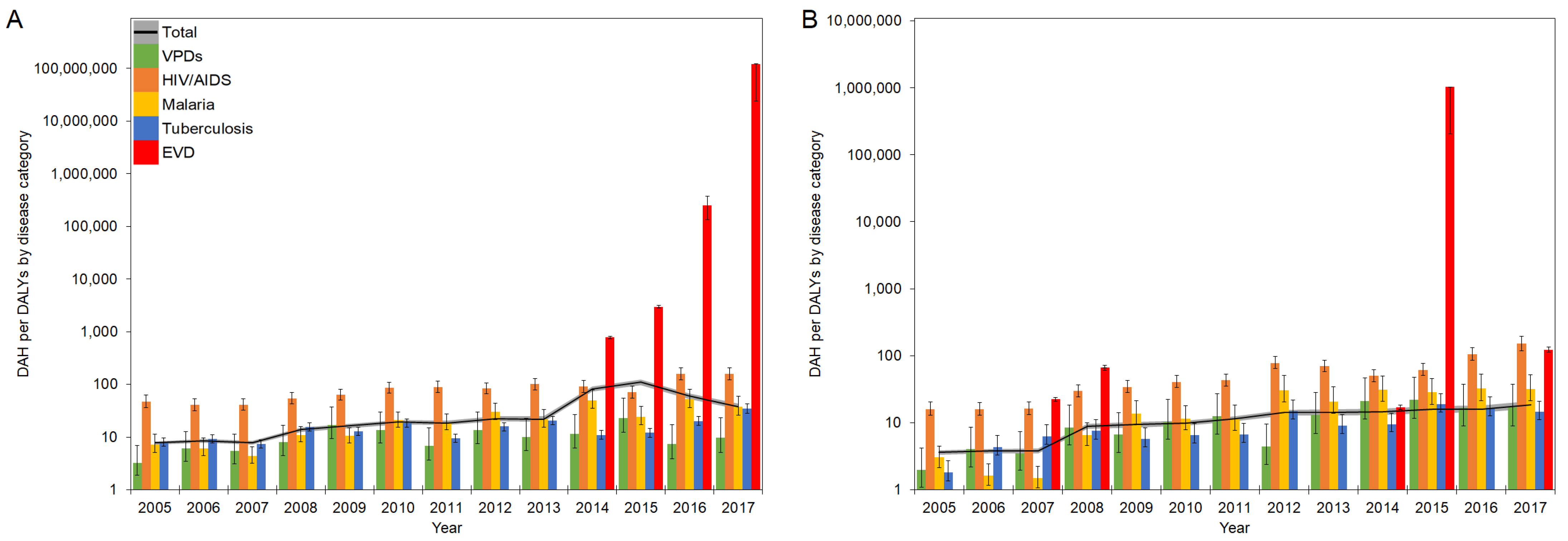
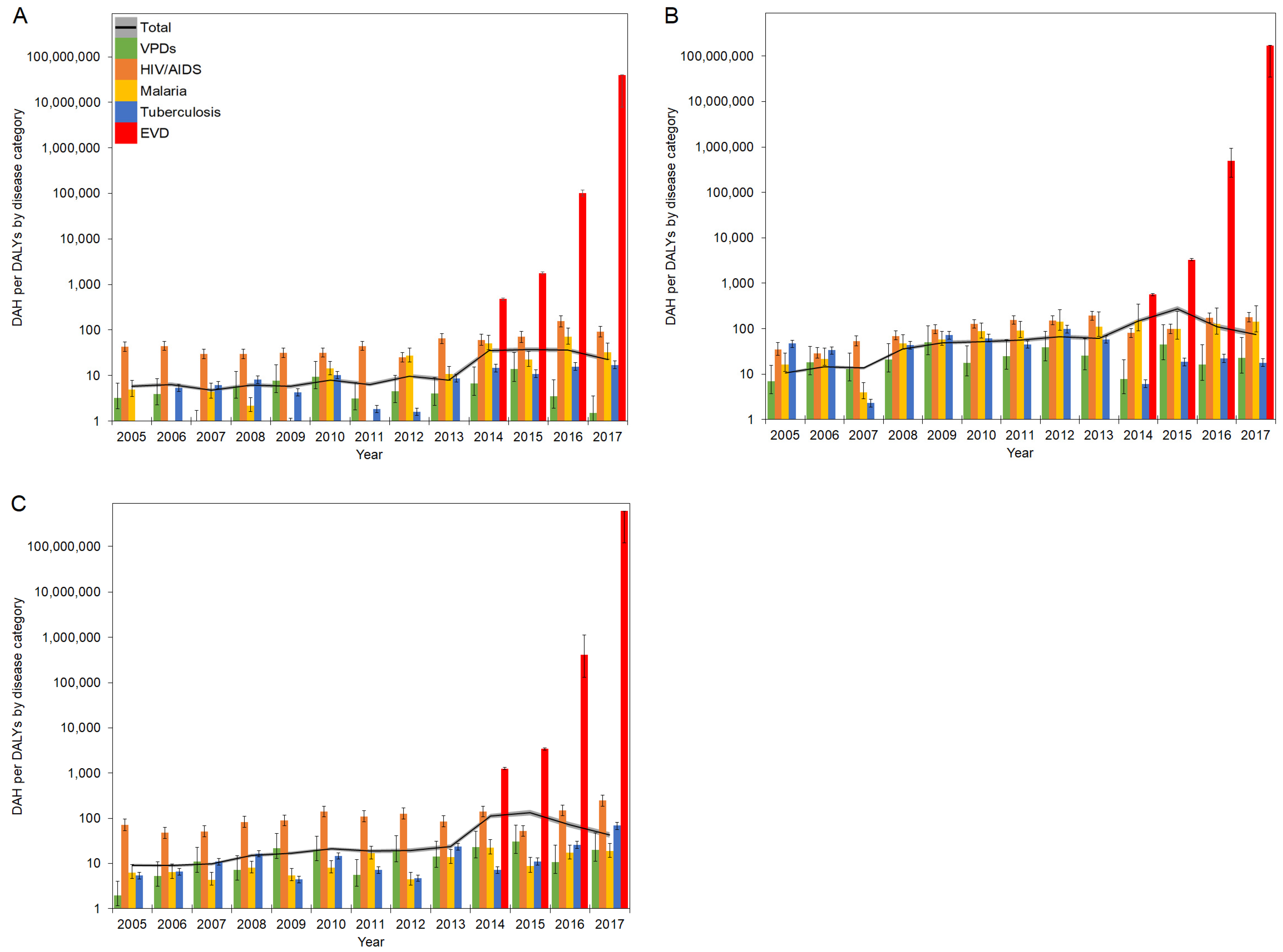
3.3. DAH per DALYs by Disease
4. Discussion
4.1. Skewed Funding Allocation in Pre-Emergency Period
4.2. Funding Prioritization during Health Emergencies
4.3. Utilization of Disease Burden for Health Financing
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Center for Disease Control and Prevention. Ebola Virus Disease Distribution Map: Cases of Ebola Virus Disease in Africa Since 1976. Available online: https://www.cdc.gov/vhf/ebola/history/distribution-map.html (accessed on 1 January 2021).
- Center for Disease Control and Prevention. 2014–2016 Ebola Outbreak Distribution in West Africa. Available online: https://www.cdc.gov/vhf/ebola/history/2014-2016-outbreak/distribution-map.html (accessed on 1 January 2021).
- World Health Organization. 10th Ebola Outbreak in the Democratic Republic of the Congo Declared over; Vigilance against Flare-Ups and Support for Survivors Must Continue. Available online: https://www.who.int/news-room/detail/25-06-2020-10th-ebola-outbreak-in-the-democratic-republic-of-the-congo-declared-over-vigilance-against-flare-ups-and-support-for-survivors-must-continue (accessed on 1 January 2021).
- Shepherd, A. Ebola: Epidemic in DRC Is One of World’s “Most Complex Health Emergencies”. BMJ 2019, 365, l4405. [Google Scholar] [CrossRef] [PubMed]
- Gostin, L.O.; Kavanagh, M.M.; Cameron, E. Ebola and War in the Democratic Republic of Congo. JAMA 2019, 321, 243. [Google Scholar] [CrossRef] [PubMed]
- Wells, C.R.; Pandey, A.; Ndeffo Mbah, M.L.; Gaüzère, B.-A.; Malvy, D.; Singer, B.H.; Galvani, A.P. The Exacerbation of Ebola Outbreaks by Conflict in the Democratic Republic of the Congo. Proc. Natl. Acad. Sci. USA 2019, 116, 24366–24372. [Google Scholar] [CrossRef]
- Helleringer, S.; Noymer, A. Magnitude of Ebola Relative to Other Causes of Death in Liberia, Sierra Leone, and Guinea. Lancet Glob. Health 2015, 3, e255–e256. [Google Scholar] [CrossRef]
- The Lancet Infectious Diseases. Rationality and Coordination for Ebola Outbreak in West Africa. Lancet Infect. Dis. 2014, 14, 1163. [Google Scholar] [CrossRef]
- Parpia, A.S.; Ndeffo-Mbah, M.L.; Wenzel, N.S.; Galvani, A.P. Effects of Response to 2014–2015 Ebola Outbreak on Deaths from Malaria, HIV/AIDS, and Tuberculosis, West Africa. Emerg. Infect. Dis. 2016, 22, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Hira, S.; Piot, P. The Counter Effects of the Ebola Epidemic on Control and Treatment of HIV/AIDS, Tuberculosis, and Malaria in West Africa. AIDS 2016, 30, 2555–2559. [Google Scholar] [CrossRef] [PubMed]
- Ansumana, R.; Keitell, S.; Roberts, G.M.T.; Ntoumi, F.; Petersen, E.; Ippolito, G.; Zumla, A. Impact of Infectious Disease Epidemics on Tuberculosis Diagnostic, Management, and Prevention Services: Experiences and Lessons from the 2014–2015 Ebola Virus Disease Outbreak in West Africa. Int. J. Infect. Dis. 2017, 56, 101–104. [Google Scholar] [CrossRef]
- Zachariah, R.; Ortuno, N.; Hermans, V.; Desalegn, W.; Rust, S.; Reid, A.J.; Boeree, M.J.; Harries, A.D. Ebola, Fragile Health Systems and Tuberculosis Care: A Call for Pre-Emptive Action and Operational Research. Int. J. Tuberc. Lung Dis. 2015, 19, 1271–1275. [Google Scholar] [CrossRef]
- Desta, K.T.; Kessely, D.B.; Daboi, J.G. Evaluation of the Performance of the National Tuberculosis Program of Liberia during the 2014–2015 Ebola Outbreak. BMC Public Health 2019, 19, 1221. [Google Scholar] [CrossRef]
- Elston, J.W.T.; Cartwright, C.; Ndumbi, P.; Wright, J. The Health Impact of the 2014–15 Ebola Outbreak. Public Health 2017, 143, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Hayden, E.C. Ebola Outbreak Shuts down Malaria-Control Efforts. Nature 2014, 514, 15–16. [Google Scholar] [CrossRef]
- Plucinski, M.M.; Guilavogui, T.; Sidikiba, S.; Diakité, N.; Diakité, S.; Dioubaté, M.; Bah, I.; Hennessee, I.; Butts, J.K.; Halsey, E.S.; et al. Effect of the Ebola-Virus-Disease Epidemic on Malaria Case Management in Guinea, 2014: A Cross-Sectional Survey of Health Facilities. Lancet Infect. Dis. 2015, 15, 1017–1023. [Google Scholar] [CrossRef][Green Version]
- Walker, P.G.T.; White, M.T.; Griffin, J.T.; Reynolds, A.; Ferguson, N.M.; Ghani, A.C. Malaria Morbidity and Mortality in Ebola-Affected Countries Caused by Decreased Health-Care Capacity, and the Potential Effect of Mitigation Strategies: A Modelling Analysis. Lancet Infect. Dis. 2015, 15, 825–832. [Google Scholar] [CrossRef]
- Samba, T.; Bhat, P.; Owiti, P.; Samuels, L.; Kanneh, P.J.; Paul, R.; Kargbo, B.; Harries, A.D. Non-Communicable Diseases in the Western Area District, Sierra Leone, before and during the Ebola Outbreak. Public Health Action 2017, 7, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Delamou, A.; Ayadi, A.M.E.; Sidibe, S.; Delvaux, T.; Camara, B.S.; Sandouno, S.D.; Beavogui, A.H.; Rutherford, G.W.; Okumura, J.; Zhang, W.-H.; et al. Effect of Ebola Virus Disease on Maternal and Child Health Services in Guinea: A Retrospective Observational Cohort Study. Lancet Glob. Health 2017, 5, e448–e457. [Google Scholar] [CrossRef]
- Iyengar, P.; Kerber, K.; Howe, C.J.; Dahn, B. Services for Mothers and Newborns during the Ebola Outbreak in Liberia: The Need for Improvement in Emergencies. PLoS Curr. 2015, 7, ecurrents.outbreaks.4ba318308719ac86fbef91f8e56cb6. [Google Scholar] [CrossRef]
- Camara, B.S.; Delamou, A.; Diro, E.; Béavogui, A.H.; El Ayadi, A.M.; Sidibé, S.; Grovogui, F.M.; Takarinda, K.C.; Bouedouno, P.; Sandouno, S.D.; et al. Effect of the 2014/2015 Ebola Outbreak on Reproductive Health Services in a Rural District of Guinea: An Ecological Study. Trans. R. Soc. Trop. Med. Hyg. 2017, 111, 22–29. [Google Scholar] [CrossRef]
- Jalloh, M.F.; Li, W.; Bunnell, R.E.; Ethier, K.A.; O’Leary, A.; Hageman, K.M.; Sengeh, P.; Jalloh, M.B.; Morgan, O.; Hersey, S.; et al. Impact of Ebola Experiences and Risk Perceptions on Mental Health in Sierra Leone, July 2015. BMJ Glob. Health 2018, 3, e000471. [Google Scholar] [CrossRef]
- O’Leary, A.; Jalloh, M.F.; Neria, Y. Fear and Culture: Contextualising Mental Health Impact of the 2014–2016 Ebola Epidemic in West Africa. BMJ Glob. Health 2018, 3, e000924. [Google Scholar] [CrossRef]
- Azman, A.S.; Legros, D.; Lessler, J.; Luquero, F.J.; Moore, S.M. Outbreaks of Cholera in the Time of Ebola: Pre-Emptive Action Needed. Lancet 2015, 385, 851. [Google Scholar] [CrossRef][Green Version]
- Suk, J.E.; Jimenez, A.P.; Kourouma, M.; Derrough, T.; Baldé, M.; Honomou, P.; Kolie, N.; Mamadi, O.; Tamba, K.; Lamah, K.; et al. Post-Ebola Measles Outbreak in Lola, Guinea, January–June 2015. Emerg. Infect. Dis. 2016, 22, 1106–1108. [Google Scholar] [CrossRef]
- Colavita, F.; Biava, M.; Castilletti, C.; Quartu, S.; Vairo, F.; Caglioti, C.; Agrati, C.; Lalle, E.; Bordi, L.; Lanini, S.; et al. Measles Cases during Ebola Outbreak, West Africa, 2013–2016. Emerg. Infect. Dis. 2017, 23, 1035–1037. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Metcalf, C.J.E.; Ferrari, M.J.; Moss, W.J.; Truelove, S.A.; Tatem, A.J.; Grenfell, B.T.; Lessler, J. Reduced Vaccination and the Risk of Measles and Other Childhood Infections Post-Ebola. Science 2015, 347, 1240–1242. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L. As Ebola Fades, a New Threat. Science 2015, 347, 1189. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Samba, T.T.; Yao, J.; Yin, W.; Xiao, L.; Liu, F.; Liu, X.; Zhou, J.; Kou, Z.; Fan, H.; et al. Impact of the Ebola Outbreak on Routine Immunization in Western Area, Sierra Leone—A Field Survey from an Ebola Epidemic Area. BMC Public Health 2017, 17, 363. [Google Scholar] [CrossRef]
- Arie, S. Congo Sees Rise in Deaths from Malaria, Measles, and Cholera as Ebola Outbreak Swallows up Resources. BMJ 2019, 366, l4522. [Google Scholar] [CrossRef]
- ReliefWeb. Democratic Republic of Congo (DRC)—Cholera Outbreak (UN, DRC Authorities, DG ECHO) (ECHO Daily Flash of 13 June 2019). Available online: https://reliefweb.int/report/democratic-republic-congo/democratic-republic-congo-drc-cholera-outbreak-un-drc-authorities (accessed on 1 January 2021).
- World Health Organization. Measles and Rubella Surveillance Data. Available online: https://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/active/measles_monthlydata/en/ (accessed on 15 August 2020).
- Hung, Y.W.; Law, M.R.; Cheng, L.; Abramowitz, S.; Alcayna-Stevens, L.; Lurton, G.; Mayaka, S.M.; Olekhnovitch, R.; Kyomba, G.; Ruton, H.; et al. Impact of a Free Care Policy on the Utilisation of Health Services during an Ebola Outbreak in the Democratic Republic of Congo: An Interrupted Time-Series Analysis. BMJ Glob. Health 2020, 5, e002119. [Google Scholar] [CrossRef]
- Li, Z.; Richter, L.; Lu, C. Tracking Development Assistance for Reproductive, Maternal, Newborn, Child and Adolescent Health in Conflict-Affected Countries. BMJ Glob. Health 2019, 4, e001614. [Google Scholar] [CrossRef]
- Suhrcke, M.; Rechel, B.; Michaud, C. Development Assistance for Health in Central and Eastern European Region. Bull. World Health Organ. 2005, 83, 920–927. [Google Scholar]
- Dieleman, J.L.; Graves, C.M.; Templin, T.; Johnson, E.; Baral, R.; Leach-Kemon, K.; Haakenstad, A.M.; Murray, C.J.L. Global Health Development Assistance Remained Steady In 2013 But Did Not Align with Recipients’ Disease Burden. Health Aff. 2014, 33, 878–886. [Google Scholar] [CrossRef]
- Hanlon, M.; Graves, C.M.; Brooks, B.P.C.; Haakenstad, A.; Lavado, R.; Leach-Kemon, K.; Dieleman, J.L. Regional Variation in the Allocation of Development Assistance for Health. Glob. Health 2014, 10, 8. [Google Scholar] [CrossRef]
- Skirbekk, V.; Ottersen, T.; Hamavid, H.; Sadat, N.; Dieleman, J.L. Vast Majority of Development Assistance for Health Funds Target Those Below Age Sixty. Health Aff. 2017, 36, 926–930. [Google Scholar] [CrossRef]
- Liese, B.H.; Schubert, L. Official Development Assistance for Health—How Neglected Are Neglected Tropical Diseases? An Analysis of Health Financing. Int. Health 2009, 1, 141–147. [Google Scholar] [CrossRef]
- Li, Z.; Li, M.; Patton, G.C.; Lu, C. Global Development Assistance for Adolescent Health from 2003 to 2015. JAMA Netw. Open 2018, 1, e181072. [Google Scholar] [CrossRef]
- Dieleman, J.L.; Schneider, M.T.; Haakenstad, A.; Singh, L.; Sadat, N.; Birger, M.; Reynolds, A.; Templin, T.; Hamavid, H.; Chapin, A.; et al. Development Assistance for Health: Past Trends, Associations, and the Future of International Financial Flows for Health. Lancet 2016, 387, 2536–2544. [Google Scholar] [CrossRef]
- Charlson, F.J.; Dieleman, J.; Singh, L.; Whiteford, H.A. Donor Financing of Global Mental Health, 1995–2015: An Assessment of Trends, Channels, and Alignment with the Disease Burden. PLoS ONE 2017, 12, e0169384. [Google Scholar] [CrossRef] [PubMed]
- Graves, C.M.; Haakenstad, A.; Dieleman, J.L. Tracking Development Assistance for Health to Fragile States: 2005–2011. Glob. Health 2015, 11, 12. [Google Scholar] [CrossRef] [PubMed]
- Warsame, A.; Patel, P.; Checchi, F. Patterns of Funding Allocation for Tuberculosis Control in Fragile States. Int. J. Tuberc. Lung Dis. 2014, 18, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation. Development Assistance for Health Database 1990–2019. Available online: http://ghdx.healthdata.org/record/ihme-data/development-assistance-health-database-1990-2019 (accessed on 15 August 2020).
- Institute for Health Metrics and Evaluation. Financing Global Health 2018: Countries and Programs in Transition. Available online: http://www.healthdata.org/policy-report/financing-global-health-2018-countries-and-programs-transition (accessed on 15 August 2020).
- Institute for Health Metrics and Evaluation. Terms Defined. Available online: http://www.healthdata.org/terms-defined (accessed on 15 August 2020).
- Murray, C.J.L.; Acharya, A.K. Understanding DALYs. J. Health Econ. 1997, 16, 703–730. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Lopez, A.D. Quantifying Disability: Data, Methods and Results. Bull. World Health Organ. 1994, 72, 481–494. [Google Scholar] [PubMed]
- Ad Hoc Committee on Health Research Relating to Future Intervention Options. In Investing in Health Research and Development; World Health Organization: Geneva, Switzerland, 1996.
- Institute for Health Metrics and Evaluation. Health Financing Publications. Available online: http://www.healthdata.org/health-financing/publications (accessed on 15 August 2020).
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2017 (GBD 2017) Results. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 15 August 2020).
- Joint United Nations Programme on HIV/AIDS. United Nations Declarations and Goals. Available online: https://www.unaids.org/en/goals/unitednationsdeclarationsandgoals (accessed on 1 January 2021).
- World Health Organization. Statement on the 1st meeting of the IHR Emergency Committee on the 2014 Ebola outbreak in West Africa. Available online: https://www.who.int/mediacentre/news/statements/2014/ebola-20140808/en/ (accessed on 1 January 2021).
- Abbas, K.; Procter, S.R.; van Zandvoort, K.; Clark, A.; Funk, S.; Mengistu, T.; Hogan, D.; Dansereau, E.; Jit, M.; Flasche, S.; et al. Routine Childhood Immunisation during the COVID-19 Pandemic in Africa: A Benefit–Risk Analysis of Health Benefits versus Excess Risk of SARS-CoV-2 Infection. Lancet Glob. Health 2020, 8, e1264–e1272. [Google Scholar] [CrossRef]
- Jewell, B.L.; Mudimu, E.; Stover, J.; ten Brink, D.; Phillips, A.N.; Smith, J.A.; Martin-Hughes, R.; Teng, Y.; Glaubius, R.; Mahiane, S.G.; et al. Potential Effects of Disruption to HIV Programmes in Sub-Saharan Africa Caused by COVID-19: Results from Multiple Mathematical Models. Lancet HIV 2020, 7, e629–e640. [Google Scholar] [CrossRef]
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Hamlet, A.; Smith, J.A.; Winskill, P.; Verity, R.; et al. Potential Impact of the COVID-19 Pandemic on HIV, Tuberculosis, and Malaria in Low-Income and Middle-Income Countries: A Modelling Study. Lancet Glob. Health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef]
- King, J.S. COVID-19 and the Need for Health Care Reform. N. Engl. J. Med. 2020, 382, e104. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Co-Operation and Development. Technical Guide to Terms and Data in the Creditor Reporting System (CRS) Aid Activities Database. Available online: https://www.oecd.org/dac/stats/crsguide.htm (accessed on 15 August 2020).
- United Nations Office for the Coordination of Humanitarian Affairs. Financial Tracking Service. Available online: https://fts.unocha.org/ (accessed on 15 August 2020).
- Anand, S.; Hanson, K. Disability-Adjusted Life Years: A Critical Review. J. Health Econ. 1997, 16, 685–702. [Google Scholar] [CrossRef]
- Solberg, C.T.; Sørheim, P.; Müller, K.E.; Gamlund, E.; Norheim, O.F.; Barra, M. The Devils in the DALY: Prevailing Evaluative Assumptions. Public Health Ethics 2010, 13, 259–274. [Google Scholar] [CrossRef]
- Lu, C.; Schneider, M.T.; Gubbins, P.; Leach-Kemon, K.; Jamison, D.; Murray, C.J. Public Financing of Health in Developing Countries: A Cross-National Systematic Analysis. Lancet 2010, 375, 1375–1387. [Google Scholar] [CrossRef]
- Dieleman, J.L.; Graves, C.M.; Hanlon, M. The Fungibility of Health Aid: Reconsidering the Reconsidered. J. Dev. Stud. 2013, 49, 1755–1762. [Google Scholar] [CrossRef]
- Dieleman, J.L.; Hanlon, M. Measuring the Displacement and Replacement of Government Health Expenditure. Health Econ. 2014, 23, 129–140. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease Category | Explanation | Variable Name |
|---|---|---|
| Total | Total funds for health disbursed from source to channel to recipient country | dah_19 |
| VPDs | Funds for health disbursed from source to channel to recipient country for newborn and child health, disaggregated by vaccines | nch_cnv_dah_19 |
| HIV/AIDS | Funds for health disbursed from source to channel to recipient country for HIV/AIDS | hiv_dah_19 |
| Malaria | Funds for health disbursed from source to channel to recipient country for malaria | mh_dah_19 |
| Tuberculosis | Funds for health disbursed from source to channel to recipient country for tuberculosis | tb_dah_19 |
| EVD | Funds for health disbursed from source to channel to recipient country for other infectious diseases, disaggregated by Ebola | oid_ebz_dah_19 |
| Age Group Name | Cause ID | Cause Name | Hierarchy |
|---|---|---|---|
| All ages | 294 | All causes | Total |
| 298 | HIV/AIDS | A.1.1 | |
| 345 | Malaria | A.4.1 | |
| 297 | Tuberculosis | A.2.1 | |
| 843 | Ebola | A.4.17 |
| Age Group Name | Cause ID | Cause Name | Hierarchy |
|---|---|---|---|
| Under 5 years | 333 | Pneumococcal meningitis | A.5.1.1 |
| 334 | H influenzae type B meningitis | A.5.1.2 | |
| 338 | Diphtheria | A.5.3 | |
| 339 | Whooping cough | A.5.4 | |
| 340 | Tetanus | A.5.5 | |
| 341 | Measles | A.5.6 | |
| 402 | Acute hepatitis B | A.5.8.2 | |
| Etiology ID | Etiology Name | ||
| 181 | Rotavirus | ||
| 188 | Pneumococcal pneumonia | ||
| 189 | H influenzae type B pneumonia | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, K.; Checchi, F.; Warsame, A. Disparities in Health Financing Allocation among Infectious Diseases in Ebola Virus Disease (EVD)-Affected Countries, 2005–2017. Healthcare 2022, 10, 179. https://doi.org/10.3390/healthcare10020179
Shimizu K, Checchi F, Warsame A. Disparities in Health Financing Allocation among Infectious Diseases in Ebola Virus Disease (EVD)-Affected Countries, 2005–2017. Healthcare. 2022; 10(2):179. https://doi.org/10.3390/healthcare10020179
Chicago/Turabian StyleShimizu, Kazuki, Francesco Checchi, and Abdihamid Warsame. 2022. "Disparities in Health Financing Allocation among Infectious Diseases in Ebola Virus Disease (EVD)-Affected Countries, 2005–2017" Healthcare 10, no. 2: 179. https://doi.org/10.3390/healthcare10020179
APA StyleShimizu, K., Checchi, F., & Warsame, A. (2022). Disparities in Health Financing Allocation among Infectious Diseases in Ebola Virus Disease (EVD)-Affected Countries, 2005–2017. Healthcare, 10(2), 179. https://doi.org/10.3390/healthcare10020179