
Serostatus and Epidemiological Characteristics for Atypical Pneumonia Causative Bacteria among Healthy Individuals in Medina, Saudi Arabia, a Retrospective Study
Abstract
1. Introduction
2. Methodology
2.1. Study Design and Participant Samples and Data
2.2. Serological Detection
2.2.1. Indirect ELISA for C. pneumoniae and L. pneumophila
2.2.2. Indirect Enzyme-Linked Immunosorbent Assay (ELISA) for M. pneumoniae
2.3. Statistical Analyses
3. Results
3.1. Demographic Information
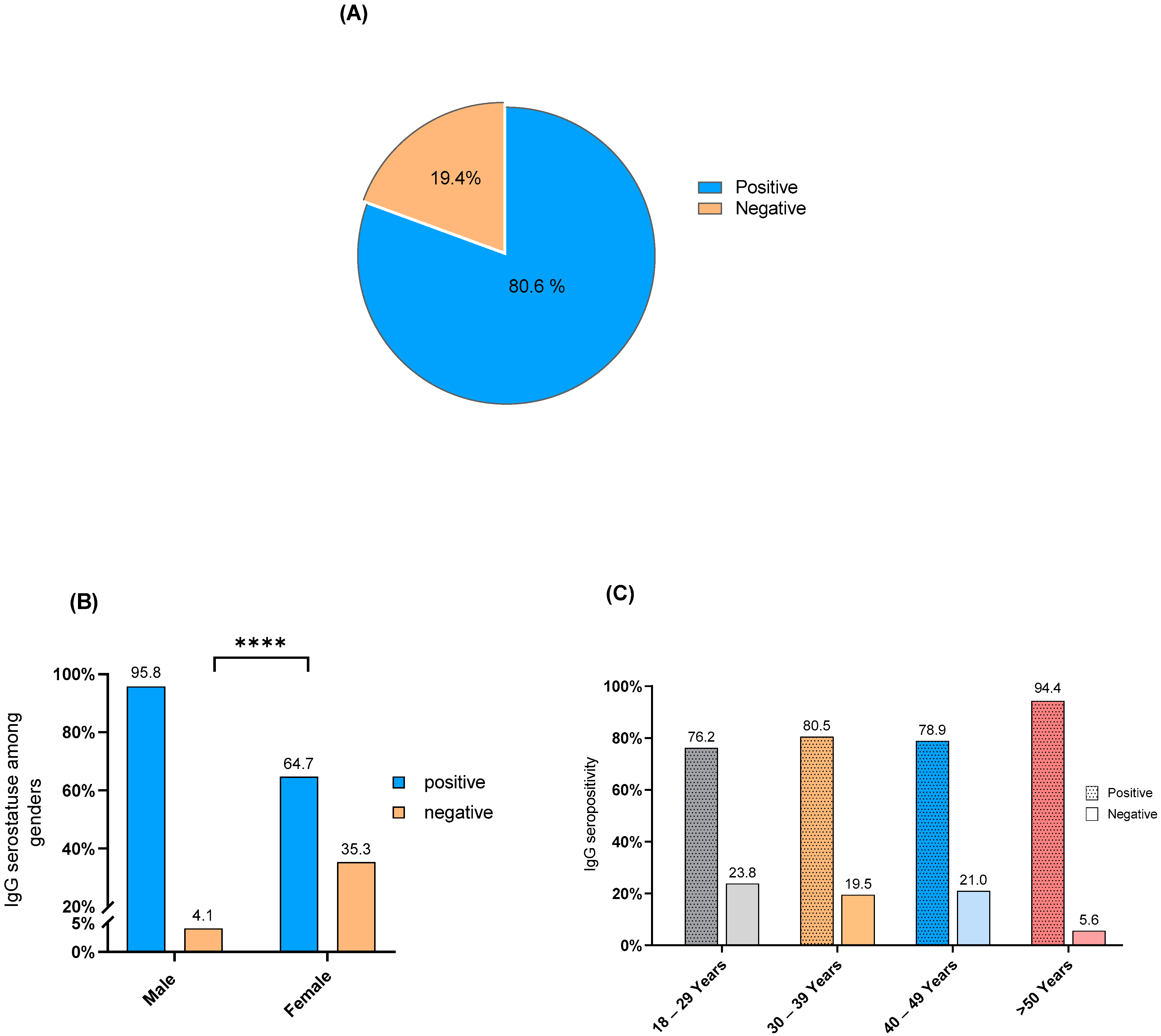
3.2. C. pneumoniae IgG Seropositivity
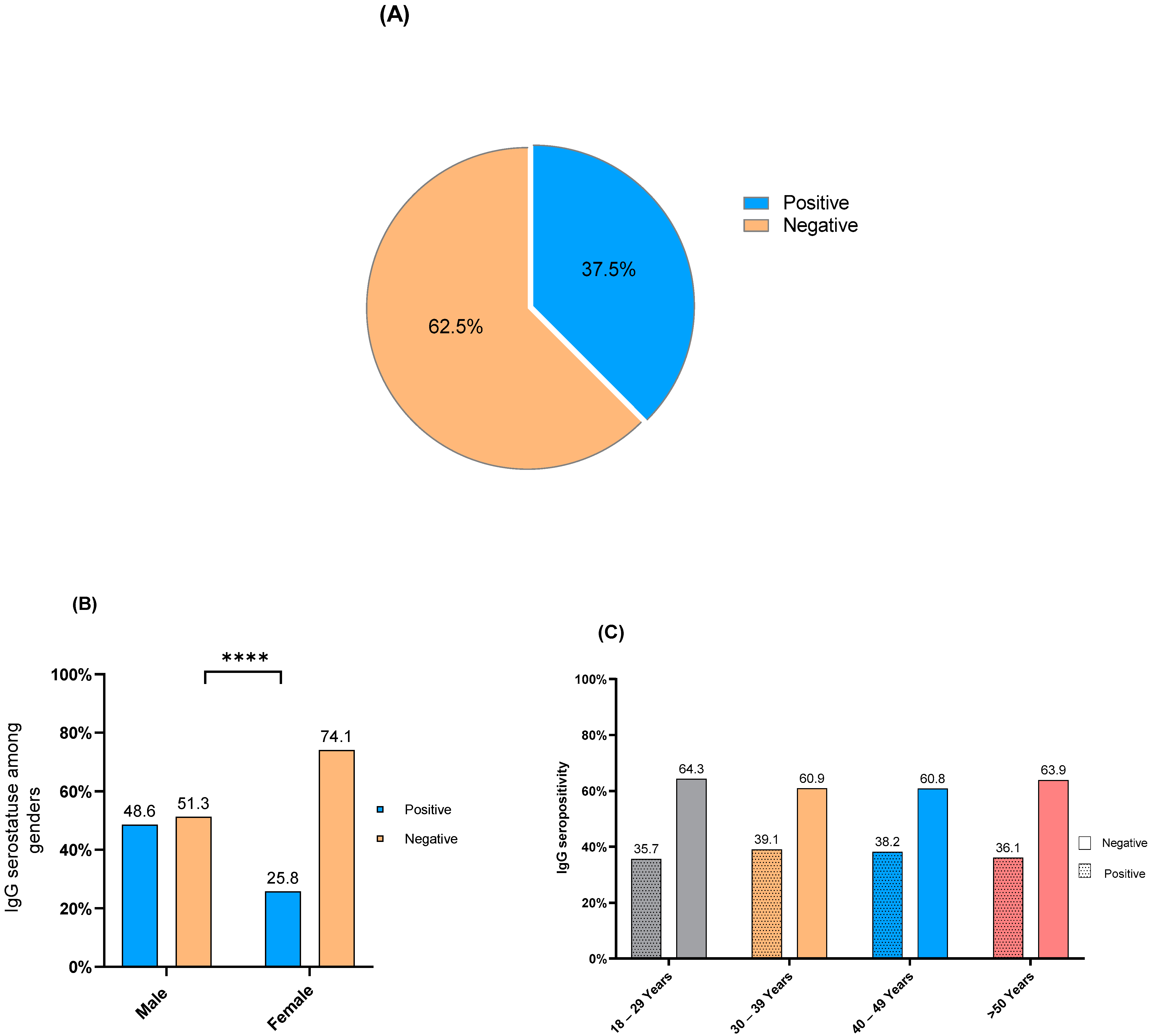
3.3. L. pneumophila IgG Seropositivity
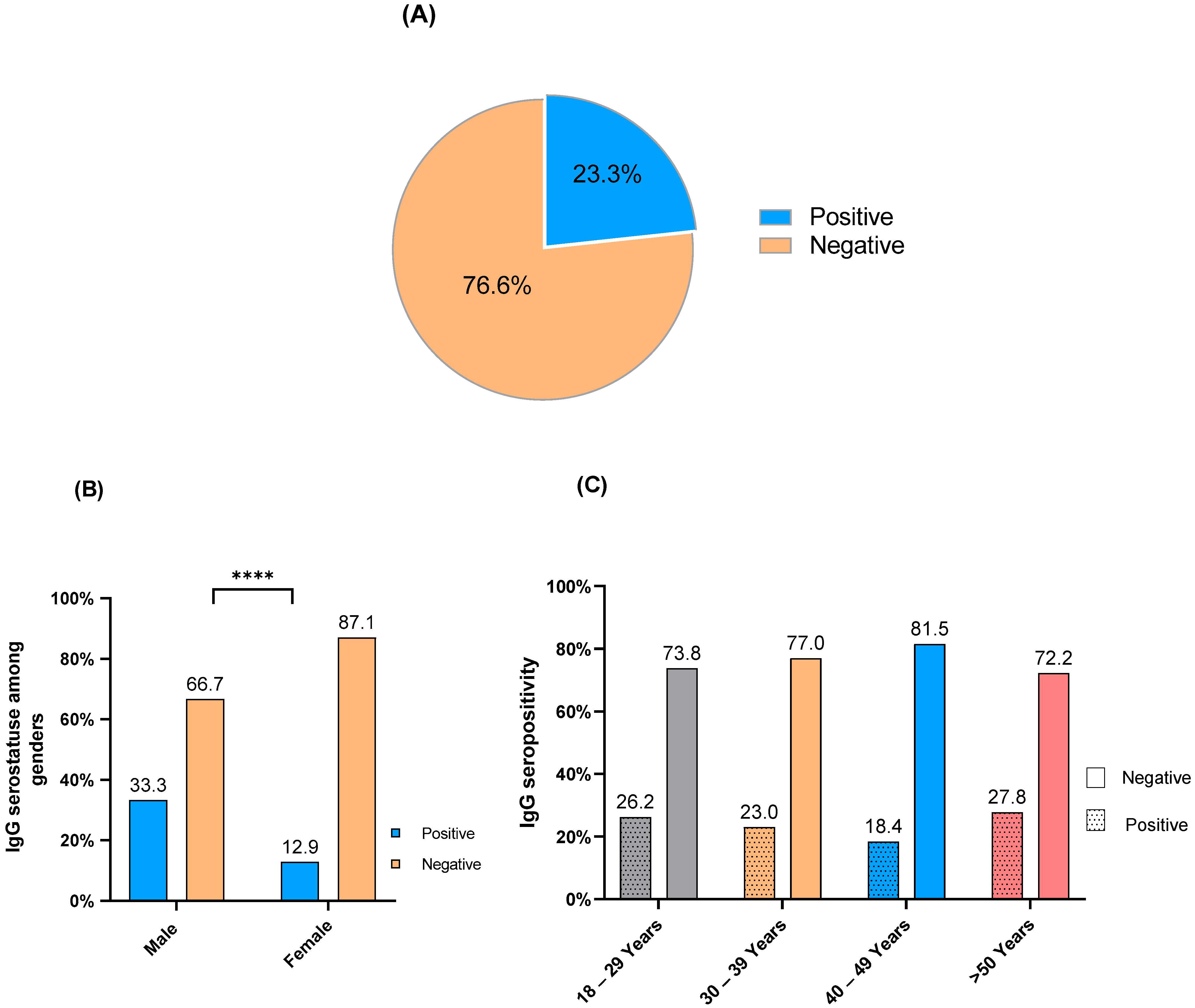
3.4. M. pneumoniae IgG Seropositivity
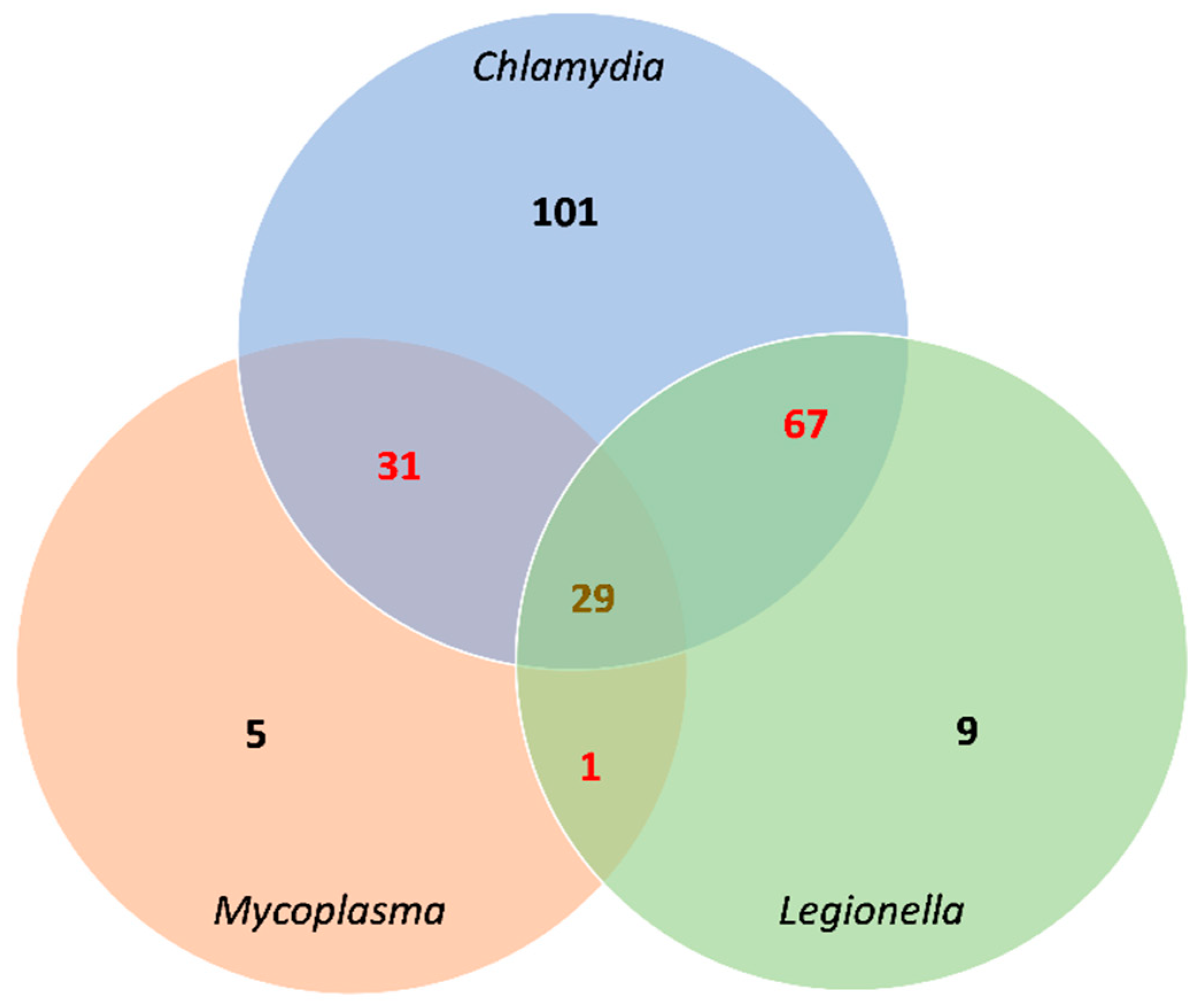
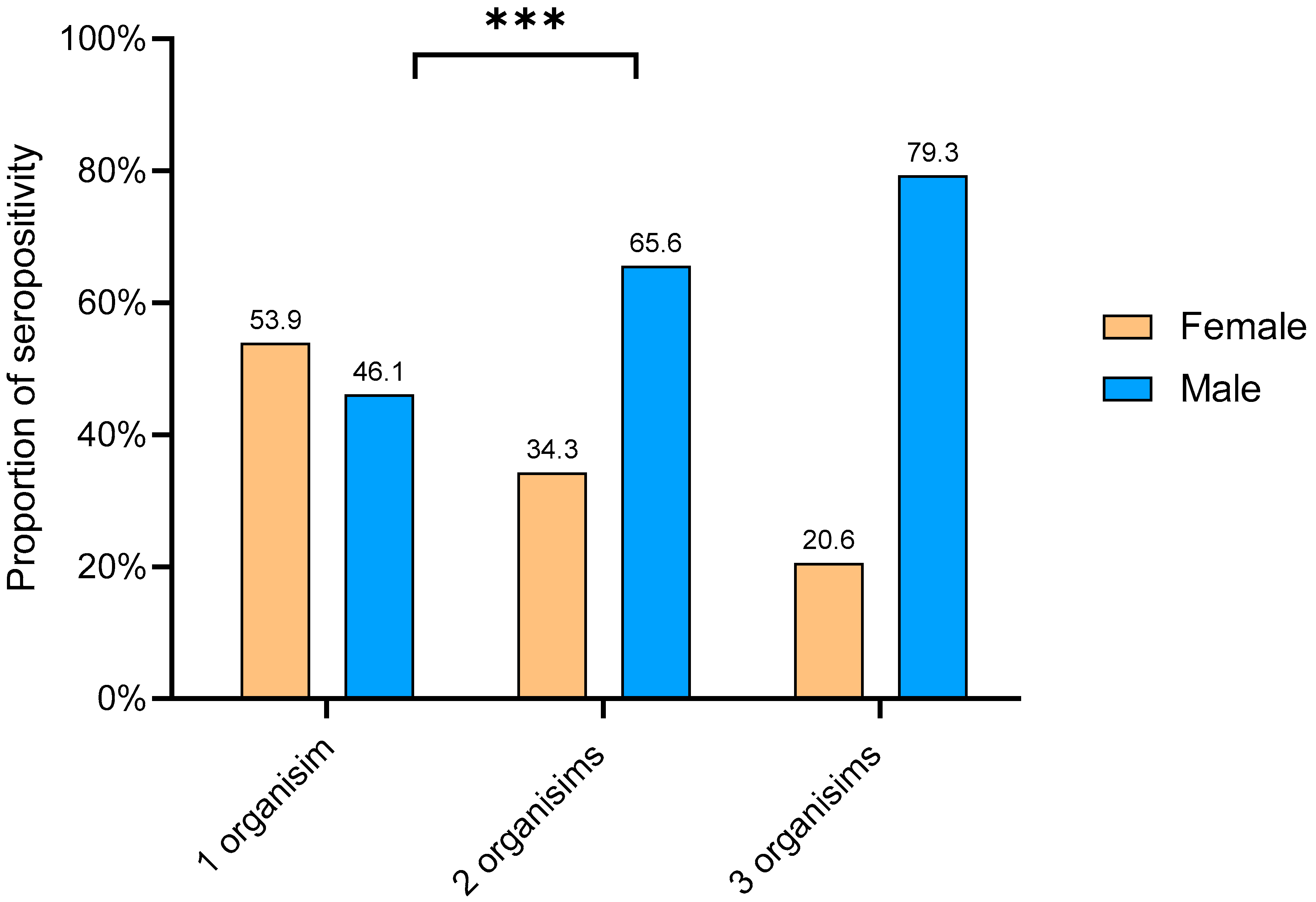
3.5. IgG seropositivity and overlapping
4. Discussion
5. Limitations of the Study
6. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lim, W.S. Pneumonia—Overview. Ref. Modul. Biomed. Sci. 2020, 185–197. [Google Scholar] [CrossRef]
- Bauer, T.T.; Ewig, S.; Rodloff, A.C.; Müller, E.E. Acute Respiratory Distress Syndrome and Pneumonia: A Comprehensive Review of Clinical Data. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2006, 43, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Aston, S.J. Pneumonia in the Developing World: Characteristic Features and Approach to Management. Respirology 2017, 22, 1276–1287. [Google Scholar] [CrossRef]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT Guidelines for the Management of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia: Guidelines for the Management of Hospital-Acquired Pneumonia (HAP)/Ventilator-Associated Pneumonia (VAP) of the European. Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef] [PubMed]
- Marchello, C.; Dale, A.P.; Thai, T.N.; Han, D.S.; Ebell, M.H. Prevalence of Atypical Pathogens in Patients with Cough and Community-Acquired Pneumonia: A Meta-Analysis. Ann. Fam. Med. 2016, 14, 552–566. [Google Scholar] [CrossRef]
- Cillóniz, C.; Ewig, S.; Polverino, E.; Marcos, M.A.; Esquinas, C.; Gabarrús, A.; Mensa, J.; Torres, A. Microbial Aetiology of Community-Acquired Pneumonia and Its Relation to Severity. Thorax 2011, 66, 340–346. [Google Scholar] [CrossRef]
- Zubairi, A.B.S.; Zafar, A.; Salahuddin, N.; Haque, A.S.; Waheed, S.; Khan, J.A. Atypical Pathogens Causing Community-Acquired Pneumonia in Adults. J. Pak. Med. Assoc. 2012, 62, 653–656. [Google Scholar]
- Capelastegui, A.; España, P.P.; Bilbao, A.; Gamazo, J.; Medel, F.; Salgado, J.; Gorostiaga, I.; Lopez de Goicoechea, M.J.; Gorordo, I.; Esteban, C.; et al. Etiology of Community-Acquired Pneumonia in a Population-Based Study: Link between Etiology and Patients Characteristics, Process-of-Care, Clinical Evolution and Outcomes. BMC Infect. Dis. 2012, 12, 134. [Google Scholar] [CrossRef]
- Arnold, F.W.; Summersgill, J.T.; Ramirez, J.A. Role of Atypical Pathogens in the Etiology of Community-Acquired Pneumonia. Semin. Respir. Crit. Care Med. 2016, 37, 819–828. [Google Scholar] [CrossRef]
- Tao, L.-L.; Hu, B.-J.; He, L.-X.; Wei, L.; Xie, H.-M.; Wang, B.-Q.; Li, H.-Y.; Chen, X.-H.; Zhou, C.-M.; Deng, W.-W. Etiology and Antimicrobial Resistance of Community-Acquired Pneumonia in Adult Patients in China. Chin. Med. J. 2012, 125, 2967–2972. [Google Scholar]
- Gramegna, A.; Sotgiu, G.; Di Pasquale, M.; Radovanovic, D.; Terraneo, S.; Reyes, L.F.; Vendrell, E.; Neves, J.; Menzella, F. Atypical Pathogens in Hospitalized Patients with Community-Acquired Pneumonia: A Worldwide Perspective. BMC Infect. Dis. 2018, 18, 677. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.R.E.; Price Evans, D.A. The Spectrum of Pneumonia in 1983 at the Riyadh Armed Forces Hospital. J. Infect. 1987, 14, 31–37. [Google Scholar] [CrossRef]
- Kurashi, N.Y.; Al-Hamdan, A.; Ibrahim, E.M.; Al-Idrissi, H.Y.; Al-Bayari, T.H. Community Acquired Acute Bacterial and Atypical Pneumonia in Saudi Arabia. Thorax 1992, 47, 115–118. [Google Scholar] [CrossRef][Green Version]
- Farahat, F.M.; Bukhari, O.K.; Basfar, I.A.; Alammari, A.M.; Zaatari, A.Z.; Alsaedi, A.A.; Alshamrani, M.M. Clinical Characteristics and Outcomes of Community-Acquired Pneumonia in Western Saudi Arabia: A Four-Year Retrospective Analysis of Medical Records. J. Infect. Public Health 2021, 14, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Alshahwan, S.I.; Alsowailmi, G.; Alsahli, A.; Alotaibi, A.; Alshaikh, M.; Almajed, M.; Omair, A.; Almodaimegh, H. The Prevalence of Complications of Pneumonia among Adults Admitted to a Tertiary Care Center in Riyadh from 2010–2017. Ann. Saudi Med. 2019, 39, 29–36. [Google Scholar] [CrossRef]
- Mahallawi, W.H.; Ibrahim, N.A.; Alahmadi, K.S.; Al-Harbi, A.K.; Almughthawi, M.A.; Alhazmi, O.A.; Alsehli, F.H.; Khabour, O.F. Natural immunity to influenza A and B among Saudi blood donors in Al Madinah Al Munawarah, Saudi Arabia. Saudi Med. J. 2020, 41, 1301. [Google Scholar] [CrossRef] [PubMed]
- Mahallawi, W.H.; Ibrahim, N.A.; Aljohani, A.S.; Shaikh, E.A.; Nafe, R.H.; Khan, A.M.; Mumena, W.A. Assessment of SARS-CoV-2 anti-spike IgG antibody in women and children in Madinah, Saudi Arabia: A single-center study. Int. J. Environ. Res. Public Health 2021, 18, 9971. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.C.; Jackson, L.A.; Campbell, L.A.; Grayston, J.T. Chlamydia Pneumoniae (TWAR). Clin. Microbiol. Rev. 1995, 8, 451–461. [Google Scholar] [CrossRef]
- Sobieszczańska, B.M.; Kasprzykowska, U.; Duda-Madej, A.; Secewicz, A.; Marciniak, J.; Gósciniak, G. Relevance of Serology for Mycoplasma pneumoniae Infection among Children with Persistent Cough. Adv. Clin. Exp. Med. 2014, 23, 185–190. [Google Scholar] [CrossRef]
- Lin, T.M.; Kuo, C.C.; Chen, W.J.; Lin, F.J.H.; Eng, H.L. Seroprevalence of Chlamydia Pneumoniae Infection in Taiwan. J. Infect. 2004, 48, 91–95. [Google Scholar] [CrossRef]
- Al-Younes, H.M. High Prevalence of Chlamydia Pneumoniae Infection in an Asymptomatic Jordanian Population. J. Microbiol. Immunol. Infect. 2014, 47, 412–417. [Google Scholar] [CrossRef]
- Al-Younes, H.M. Seroprevalence of Chlamydia Pneumoniae in Male Adults in Jordan. Dirasat Pure Sci. 2009, 36, 1–6. [Google Scholar]
- Wellinghausen, N.; Straube, E.; Freidank, H.; von Baum, H.; Marre, R.; Essig, A. Low Prevalence of Chlamydia Pneumoniae in Adults with Community-Acquired Pneumonia. Int. J. Med. Microbiol. 2006, 296, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Holter, J.C.; Müller, F.; Bjørang, O.; Samdal, H.H.; Marthinsen, J.B.; Jenum, P.A.; Ueland, T.; Frøland, S.S.; Aukrust, P.; Husebye, E.; et al. Etiology of Community-Acquired Pneumonia and Diagnostic Yields of Microbiological Methods: A 3-Year Prospective Study in Norway. BMC Infect. Dis. 2015, 15, 64. [Google Scholar] [CrossRef]
- Al-Aydie, S.N.; Obeidat, N.M.; Al-Younes, H.M. Role of Chlamydia Pneumoniae in Community-Acquired Pneumonia in Hospitalized Jordanian Adults. J. Infect. Dev. Ctries. 2016, 10, 227–236. [Google Scholar] [CrossRef]
- Noori Goodarzi, N.; Pourmand, M.R.; Rajabpour, M.; Arfaatabar, M.; Mosadegh, M.; Syed Mohamad, S.A. Frequency of Mycoplasma pneumoniae, Legionella pneumophila and Chlamydia spp. among Patients with Atypical Pneumonia in Tehran. New Microbes New Infect. 2020, 37. [Google Scholar] [CrossRef]
- Keše, D.; Obreza, A.; Rojko, T.; Kišek, T.C. Legionella Pneumophila-Epidemiology and Characterization of Clinical Isolates, Slovenia, 2006–2020. Diagnostics 2021, 11, 1201. [Google Scholar] [CrossRef]
- Ashgar, S.S.; Al-Said, H.M. Detection of Legionella Pneumophila as the Cause of Atypical Pneumonia in the Water Sources of the Holy Places of Makkah. Afr. J. Microbiol. Res. 2021, 15, 429–432. [Google Scholar] [CrossRef]
- Cunha, B.A.; Burillo, A.; Bouza, E. Legionnaires’ Disease. Lancet 2016, 387, 376–385. [Google Scholar] [CrossRef]
- Noori Goodarzi, N.; Pourmand, M.R.; Arfaatabar, M.; Azimi, G.; Masoorian, E.; Rahimi Foroushani, A.; Aminharati, F.; Heidarzadeh, S.; Baghani, A. First Detection and Characterization of Macrolide-Resistant Mycoplasma pneumoniae from People with Community-Acquired Pneumonia in Iran. Microb. Drug Resist. 2020, 26, 245–250. [Google Scholar] [CrossRef]
- Marie, M.A.M. Incidence and Antimicrobial Susceptibility of Mycoplasma pneumoniae in Saudi Arabia. J. Bacteriol. Virol. 2010, 40, 159–162. [Google Scholar] [CrossRef][Green Version]
- Al-Janabi, M.K.W.; Ali, S.H.M.; Nasir, N.A.; Wehby, M. Detecting Mycoplasma pneumoniae Infections in Nasopharyngeal Specimens from Paediatric Patients with Asthma Exacerbations in Baghdad: A Polymerase Chain Reaction—Gene Based Study. Egypt. J. Med. Hum. Genet. 2018, 19, 117–121. [Google Scholar] [CrossRef]
- Zirakishvili, D.; Chkhaidze, I.; Barnabishvili, N. Mycoplasma pneumoniae and Chlamydophila pneumoniae in hospitalized children with bronchiolitis. Georgian Med. News 2015, 73–78. [Google Scholar]
- Alhuofie, S.T.S. An Elderly COVID-19 Patient with Community-Acquired Legionella and Mycoplasma Coinfections: A Rare Case Report. Healthcare 2021, 9, 1598. [Google Scholar] [CrossRef]
- chou Kuo, C.; Shor, A.; Campbell, L.A.; Fukushi, H.; Patton, D.L.; Grayston, J.T.; chou Kuo, C.; Shor, A.; Campbell, L.A.; Fukushi, H.; et al. Demonstration of Chlamydia Pneumoniae in Atherosclerotic Lesions of Coronary Arteries. J. Infect. Dis. 1993, 167, 841–849. [Google Scholar] [CrossRef]
- Saikku, P. Chlamydia Pneumoniae in Atherosclerosis. J. Intern. Med. 2000, 247, 391–396. [Google Scholar] [CrossRef]
- Zhan, P.; Suo, L.J.; Qian, Q.; Shen, X.K.; Qiu, L.X.; Yu, L.K.; Song, Y. Chlamydia Pneumoniae Infection and Lung Cancer Risk: A Meta-Analysis. Eur. J. Cancer 2011, 47, 742–747. [Google Scholar] [CrossRef]
- Hahn, D.L.; Schure, A.; Patel, K.; Childs, T.; Drizik, E.; Webley, W. Chlamydia Pneumoniae-Specific IgE Is Prevalent in Asthma and Is Associated with Disease Severity. PLoS ONE 2012, 7, e35945. [Google Scholar] [CrossRef]
- Kashyap, S.; Sarkar, M. Mycoplasma Pneumonia: Clinical Features and Management. Lung India 2010, 27, 75. [Google Scholar] [CrossRef]
- Valade, S.; Biard, L.; Lemiale, V.; Argaud, L.; Pène, F.; Papazian, L.; Bruneel, F.; Seguin, A.; Kouatchet, A.; Oziel, J.; et al. Severe Atypical Pneumonia in Critically Ill Patients: A Retrospective Multicenter Study. Ann. Intensive Care 2018, 8. [Google Scholar] [CrossRef]
- Welte, T.; Torres, A.; Nathwani, D. Clinical and Economic Burden of Community-Acquired Pneumonia among Adults in Europe. Thorax 2012, 67, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Baik, I.; Curhan, G.C.; Rimm, E.B.; Bendich, A.; Willett, W.C.; Fawzi, W.W. A Prospective Study of Age and Lifestyle Factors in Relation to Community-Acquired Pneumonia in US Men and Women. Arch. Intern. Med. 2000, 160, 3082–3088. [Google Scholar] [CrossRef] [PubMed]
- Mannino, D.M.; Davis, K.J.; Kiri, V.A. Chronic Obstructive Pulmonary Disease and Hospitalizations for Pneumonia in a US Cohort. Respir. Med. 2009, 103, 224–229. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | N (%) |
|---|---|
| Gender | |
| Male | 144 (50.9) |
| Female | 139 (49.1) |
| Total | 283 |
| Age groups | |
| 18–29 | 84 (29.7) |
| 30–39 | 87 (30.7) |
| 40–49 | 76 (26.9) |
| >50 | 36 (12.7) |
| Total | 283 |
| Seropositivity Overlap Groups | N (%) | Total | p-Value | |
|---|---|---|---|---|
| Male | Female | |||
| One organism | 53 (46.1%) | 62 (53.9 %) | 115 | 0.0007 |
| Two organisms | 65 (65.6 %) | 34 (34.3%) | 99 | |
| Three organisms | 23 (79.3%) | 6 (20.6%) | 29 | |
| Total | 141 (58%) | 102 (42%) | 243 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhoufie, S.T.; Alhhazmi, A.A.; Mahallawi, W.H.; Alfarouk, K.O.; Ibrahim, N.A. Serostatus and Epidemiological Characteristics for Atypical Pneumonia Causative Bacteria among Healthy Individuals in Medina, Saudi Arabia, a Retrospective Study. Healthcare 2022, 10, 2316. https://doi.org/10.3390/healthcare10112316
Alhoufie ST, Alhhazmi AA, Mahallawi WH, Alfarouk KO, Ibrahim NA. Serostatus and Epidemiological Characteristics for Atypical Pneumonia Causative Bacteria among Healthy Individuals in Medina, Saudi Arabia, a Retrospective Study. Healthcare. 2022; 10(11):2316. https://doi.org/10.3390/healthcare10112316
Chicago/Turabian StyleAlhoufie, Sari T., Areej A. Alhhazmi, Waleed H. Mahallawi, Khalid O. Alfarouk, and Nadir A. Ibrahim. 2022. "Serostatus and Epidemiological Characteristics for Atypical Pneumonia Causative Bacteria among Healthy Individuals in Medina, Saudi Arabia, a Retrospective Study" Healthcare 10, no. 11: 2316. https://doi.org/10.3390/healthcare10112316
APA StyleAlhoufie, S. T., Alhhazmi, A. A., Mahallawi, W. H., Alfarouk, K. O., & Ibrahim, N. A. (2022). Serostatus and Epidemiological Characteristics for Atypical Pneumonia Causative Bacteria among Healthy Individuals in Medina, Saudi Arabia, a Retrospective Study. Healthcare, 10(11), 2316. https://doi.org/10.3390/healthcare10112316