
Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Survey Instrument
2.3. Study Measures
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
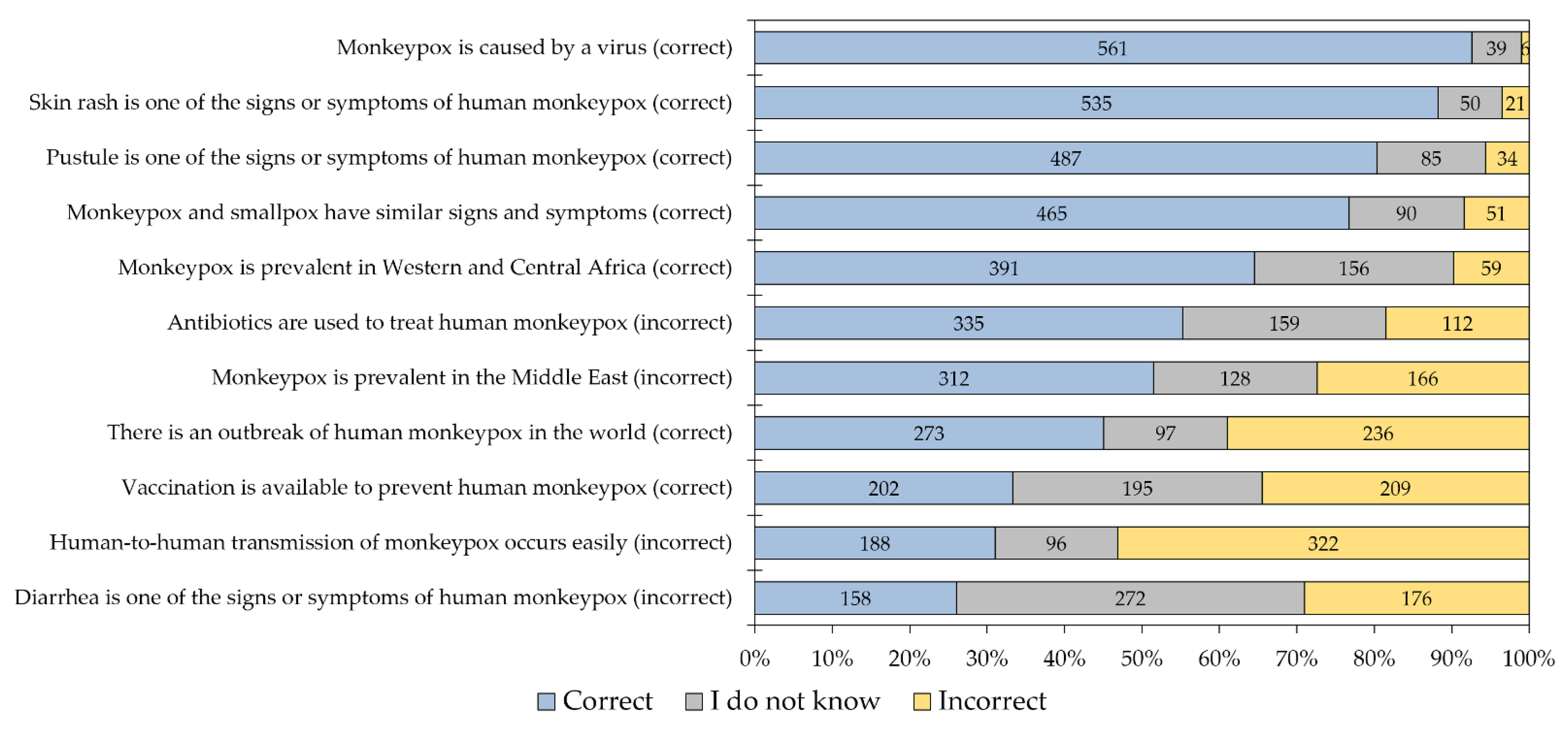
3.2. Human Monkeypox Knowledge among Jordanian HCWs
3.3. The Attitude of the Study Respondents towards the Role of Male Homosexuals in HMPX Spread
3.4. Confidence among Jordanian HCWs to Diagnose and Manage HMPX Cases
3.5. The Determinants of Conspiracy Beliefs Regarding Emerging Virus Infections
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO|World Health Organization. WHO Director-General’s Statement at the Press Conference Following IHR Emergency Committee Regarding the Multi-Country Outbreak of Monkeypox—23 July 2022. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-statement-on-the-press-conference-following-IHR-emergency-committee-regarding-the-multi--country-outbreak-of-monkeypox--23-july-2022 (accessed on 25 July 2022).
- Nuzzo, J.B.; Borio, L.L.; Gostin, L.O. The WHO Declaration of Monkeypox as a Global Public Health Emergency. JAMA 2022, 328, 615–617. [Google Scholar] [CrossRef] [PubMed]
- Kozlov, M. Monkeypox declared a global emergency: Will it help contain the outbreaks? Nature, 2022; online ahead of print. [Google Scholar] [CrossRef]
- WHO|World Health Organization. Monkeypox, COVID-19 & Other Global Health Issues Virtual Press Conference Transcript—27 July 2022. Available online: https://www.who.int/publications/m/item/monkeypox--covid-19---other-global-health-issues-virtual-press-conference-transcript---27-july-2022 (accessed on 2 August 2022).
- WHO|World Health Organization. Multi-Country Monkeypox Outbreak: Situation Update. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396 (accessed on 2 August 2022).
- Al-Tammemi, A.B.; Albakri, R.; Alabsi, S. The Outbreak of Human Monkeypox in 2022: A Changing Epidemiology or an Impending Aftereffect of Smallpox Eradication? Front. Trop. Dis. 2022, 3, 951380. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). 2022 Monkeypox Outbreak Global Map. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 10 August 2022).
- Centers for Disease Control and Prevention (CDC). 2022 Outbreak Cases and Data. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/index.html (accessed on 31 August 2022).
- Adegboye, O.A.; Eugenia Castellanos, M.; Alele, F.O.; Pak, A.; Ezechukwu, H.C.; Hou, K.; Emeto, T.I. Travel-Related Monkeypox Outbreaks in the Era of COVID-19 Pandemic: Are We Prepared? Viruses 2022, 14, 1283. [Google Scholar] [CrossRef] [PubMed]
- Sklenovská, N.; Van Ranst, M. Emergence of Monkeypox as the Most Important Orthopoxvirus Infection in Humans. Front. Public Health 2018, 6, 241. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.; Abubakar, I.; Ihekweazu, C.; Heymann, D.; Ntoumi, F.; Blumberg, L.; Asogun, D.; Mukonka, V.; Lule, S.A.; Bates, M.; et al. Monkeypox—Enhancing public health preparedness for an emerging lethal human zoonotic epidemic threat in the wake of the smallpox post-eradication era. Int. J. Infect. Dis. 2019, 78, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, A.; Aarons, E.; Astbury, J.; Balasegaram, S.; Beadsworth, M.; Beck, C.R.; Chand, M.; O’Connor, C.; Dunning, J.; Ghebrehewet, S.; et al. Two cases of monkeypox imported to the United Kingdom, September 2018. Euro Surveill. 2018, 23, 1800509. [Google Scholar] [CrossRef] [PubMed]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox—A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- Silva, N.I.O.; de Oliveira, J.S.; Kroon, E.G.; Trindade, G.S.; Drumond, B.P. Here, There, and Everywhere: The Wide Host Range and Geographic Distribution of Zoonotic Orthopoxviruses. Viruses 2020, 13, 43. [Google Scholar] [CrossRef]
- Townsend, M.B.; Keckler, M.S.; Patel, N.; Davies, D.H.; Felgner, P.; Damon, I.K.; Karem, K.L. Humoral immunity to smallpox vaccines and monkeypox virus challenge: Proteomic assessment and clinical correlations. J. Virol. 2013, 87, 900–911. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Monkeypox and Smallpox Vaccine Guidance. Available online: https://www.cdc.gov/poxvirus/monkeypox/clinicians/smallpox-vaccine.html (accessed on 2 August 2022).
- Titanji, B.K.; Tegomoh, B.; Nematollahi, S.; Konomos, M.; Kulkarni, P.A. Monkeypox: A Contemporary Review for Healthcare Professionals. Open Forum Infect. Dis. 2022, 9, ofac310. [Google Scholar] [CrossRef]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: A prospective observational cohort study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef]
- McCollum, A.M.; Damon, I.K. Human monkeypox. Clin. Infect. Dis. 2014, 58, 260–267. [Google Scholar] [CrossRef]
- Patel, A.; Bilinska, J.; Tam, J.C.H.; Da Silva Fontoura, D.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C.; et al. Clinical features and novel presentations of human monkeypox in a central London centre during the 2022 outbreak: Descriptive case series. BMJ 2022, 378, e072410. [Google Scholar] [CrossRef] [PubMed]
- Kaler, J.; Hussain, A.; Flores, G.; Kheiri, S.; Desrosiers, D. Monkeypox: A Comprehensive Review of Transmission, Pathogenesis, and Manifestation. Cureus 2022, 14, e26531. [Google Scholar] [CrossRef] [PubMed]
- Likos, A.M.; Sammons, S.A.; Olson, V.A.; Frace, A.M.; Li, Y.; Olsen-Rasmussen, M.; Davidson, W.; Galloway, R.; Khristova, M.L.; Reynolds, M.G.; et al. A tale of two clades: Monkeypox viruses. J. Gen. Virol. 2005, 86, 2661–2672. [Google Scholar] [CrossRef]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Kong, J.D.; Mahroum, N.; Tsigalou, C.; Khamisy-Farah, R.; Converti, M.; Wu, J. Epidemiological trends and clinical features of the ongoing monkeypox epidemic: A preliminary pooled data analysis and literature review. J. Med. Virol. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Vivancos, R.; Anderson, C.; Blomquist, P.; Balasegaram, S.; Bell, A.; Bishop, L.; Brown, C.S.; Chow, Y.; Edeghere, O.; Florence, I.; et al. Community transmission of monkeypox in the United Kingdom, April to May 2022. Euro Surveill. 2022, 27, 2200422. [Google Scholar] [CrossRef]
- Iñigo Martínez, J.; Gil Montalbán, E.; Jiménez Bueno, S.; Martín Martínez, F.; Nieto Juliá, A.; Sánchez Díaz, J.; García Marín, N.; Córdoba Deorador, E.; Nunziata Forte, A.; Alonso García, M.; et al. Monkeypox outbreak predominantly affecting men who have sex with men, Madrid, Spain, 26 April to 16 June 2022. Euro Surveill. 2022, 27, 2200471. [Google Scholar] [CrossRef]
- Endo, A.; Murayama, H.; Abbott, S.; Ratnayake, R.; Pearson, C.A.B.; Edmunds, W.J.; Fearon, E.; Funk, S. Heavy-tailed sexual contact networks and the epidemiology of monkeypox outbreak in non-endemic regions, May 2022. medRxiv, 2022; preprint. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Khamisy-Farah, R.; Tsigalou, C.; Mahroum, N.; Converti, M. Attaching a stigma to the LGBTQI+ community should be avoided during the monkeypox epidemic. J. Med. Virol. 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop Med Infect Dis 2022, 7, 135. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.; Abdelaal, A.; Asija, A.; Basnyat, S.; Sedhai, Y.R.; Ghimire, S.; Sah, S.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Monkeypox Virus Containment: The Application of Ring Vaccination and Possible Challenges. J. Travel Med. 2022; taac085, online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. Conspiracy Beliefs Are Associated with Lower Knowledge and Higher Anxiety Levels Regarding COVID-19 among Students at the University of Jordan. Int. J. Environ. Res. Public Health 2020, 17, 4915. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Higgins, M. Monkeypox Conspiracy Theories May Be Spreading Faster Than the Virus, Survey Reveals. Available online: https://www.studyfinds.org/monkeypox-theories/ (accessed on 7 August 2022).
- Dow, B.J.; Wang, C.S.; Whitson, J.A.; Deng, Y. Mitigating and managing COVID-19 conspiratorial beliefs. BMJ Lead. 2022; published online first. [Google Scholar] [CrossRef]
- De Coninck, D.; Frissen, T.; Matthijs, K.; d’Haenens, L.; Lits, G.; Champagne-Poirier, O.; Carignan, M.-E.; David, M.D.; Pignard-Cheynel, N.; Salerno, S.; et al. Beliefs in Conspiracy Theories and Misinformation About COVID-19: Comparative Perspectives on the Role of Anxiety, Depression and Exposure to and Trust in Information Sources. Front. Psychol. 2021, 12, 646394. [Google Scholar] [CrossRef]
- Wilkason, C.; Lee, C.; Sauer, L.M.; Nuzzo, J.; McClelland, A. Assessing and Reducing Risk to Healthcare Workers in Outbreaks. Health Secur. 2020, 18, 205–211. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Dardas, L.A.; Al-Tammemi, A.B.; Al-Majali, L.; Al-Naimat, H.; Jardaneh, L.; AlHadidi, F.; Al-Salahat, K.; Al-Ajlouni, E.; et al. Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses. Medicina 2022, 58, 924. [Google Scholar] [CrossRef]
- World Health Organization|Regional Office for the Eastern Mediterranean. Health Workforce Snapshot Jordan. Available online: https://apps.who.int/iris/handle/10665/332429 (accessed on 12 May 2022).
- Epitools—Epidemiological Calculators. Sample Size to Estimate a Simple Proportion (Apparent Prevalence). Available online: https://epitools.ausvet.com.au/oneproportion (accessed on 24 May 2022).
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Knowledge of human monkeypox viral infection among general practitioners: A cross-sectional study in Indonesia. Pathog. Glob. Health 2020, 114, 68–75. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Confidence in managing human monkeypox cases in Asia: A cross-sectional survey among general practitioners in Indonesia. Acta Tropica 2020, 206, 105450. [Google Scholar] [CrossRef]
- Freeman, D.; Waite, F.; Rosebrock, L.; Petit, A.; Causier, C.; East, A.; Jenner, L.; Teale, A.-L.; Carr, L.; Mulhall, S.; et al. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychol. Med. 2020, 52, 251–263. [Google Scholar] [CrossRef]
- WHO|World Health Organization. Second Meeting of the International Health Regulations (2005) (IHR) Emergency Committee Regarding the Multi-Country Outbreak of Monkeypox. Available online: https://www.who.int/news/item/23-07-2022-second-meeting-of-the-international-health-regulations-(2005)-(ihr)-emergency-committee-regarding-the-multi-country-outbreak-of-monkeypox (accessed on 8 August 2022).
- WHO|World Health Organization. Technical Series on Safer Primary Care: Education and Training. Available online: https://www.who.int/publications/i/item/9789241511605 (accessed on 10 August 2022).
- Harapan, H.; Wagner, A.L.; Yufika, A.; Setiawan, A.M.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; et al. Acceptance and willingness to pay for a hypothetical vaccine against monkeypox viral infection among frontline physicians: A cross-sectional study in Indonesia. Vaccine 2020, 38, 6800–6806. [Google Scholar] [CrossRef]
- Alsanafi, M.; Al-Mahzoum, K.; Sallam, M. Monkeypox Knowledge and Confidence in Diagnosis and Management with Evaluation of Emerging Virus Infection Conspiracies among Health Professionals in Kuwait. Pathogens 2022, 11, 994. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Al-Zyadat, D.; Jordan News. Jordan Is Prepared to Deal with Monkeypox, Says Health Official: Absence of Vaccines Makes Prevention Challenging, Despite Assurances to the Contrary. Available online: https://www.jordannews.jo/Section-106/Features/Jordan-is-prepared-to-deal-with-monkeypox-says-health-official-19658 (accessed on 31 August 2022).
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Mandate or Not Mandate: Knowledge, Attitudes, and Practices of Italian Occupational Physicians towards SARS-CoV-2 Immunization at the Beginning of Vaccination Campaign. Vaccines 2021, 9, 889. [Google Scholar] [CrossRef]
- Lecce, M.; Biganzoli, G.; Agnello, L.; Belisario, I.; Cicconi, G.; D’Amico, M.; De Giorgi, F.; Ferilli, A.; Ferraguzzi, G.; Guzzardi, F.; et al. COVID-19 and Influenza Vaccination Campaign in a Research and University Hospital in Milan, Italy. Int. J. Environ. Res. Public Health 2022, 19, 6500. [Google Scholar] [CrossRef]
- Dettori, M.; Arghittu, A.; Deiana, G.; Azara, A.; Masia, M.D.; Palmieri, A.; Spano, A.L.; Serra, A.; Castiglia, P. Influenza Vaccination Strategies in Healthcare Workers: A Cohort Study (2018–2021) in an Italian University Hospital. Vaccines 2021, 9, 971. [Google Scholar] [CrossRef]
- Li, M.; Luo, Y.; Watson, R.; Zheng, Y.; Ren, J.; Tang, J.; Chen, Y. Healthcare workers’ (HCWs) attitudes and related factors towards COVID-19 vaccination: A rapid systematic review. Postgrad. Med. J. 2021; epub ahead of print. [Google Scholar] [CrossRef]
- McKay, K.A.; Narasimhan, S. Bridging the gap between doctors and nurses. J. Nurs. Educ. Pract. 2012, 2, 52–55. [Google Scholar] [CrossRef]
- Zhu, M.; Ji, J.; Shi, D.; Lu, X.; Wang, B.; Wu, N.; Wu, J.; Yao, H.; Li, L. Unusual global outbreak of monkeypox: What should we do? Front. Med. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Alzahrani, F.; Alarifi, A.M.; Algethami, M.R.; Alhumam, M.N.; Ayied, H.A.; Awan, A.Z.; Almutairi, A.F.; Bamakhrama, S.A.; Almushari, B.S.; et al. Assessment of Knowledge of Monkeypox Viral Infection among the General Population in Saudi Arabia. Pathogens 2022, 11, 904. [Google Scholar] [CrossRef]
- Youssef, D.; Abboud, E.; Kawtharni, M.; Zheim, Z.; Abou Arrage, N.; Youssef, J. When a Neglected Tropical Zoonotic Disease Emerges in Non-Endemic Countries: Need to Proactively Fill the Unveiled Knowledge Gaps towards Human Monkeypox among the Lebanese Population. Available online: https://www.researchgate.net/publication/363134855_When_a_neglected_tropical_zoonotic_disease_emerges_in_non-endemic_countries_Need_to_proactively_fill_the_unveiled_knowledge_gaps_towards_human_monkeypox_among_the_Lebanese_population (accessed on 30 August 2022).
- Ahmed, S.K.; Abdulqadirb, S.O.; Omar, R.M.; Essa, R.A.; Hussein, S.H.; Khdir, A.A.; Abdulla, A.Q. Study of Knowledge, Attitude and Anxiety in Kurdistan-Region of Iraqi Population during the Monkeypox Outbreak in 2022. Available online: https://www.researchgate.net/publication/362711169_Study_of_knowledge_attitude_and_anxiety_in_Kurdistan-region_of_Iraqi_population_during_the_monkeypox_outbreak_in_2022_An_online_cross-sectional_study (accessed on 1 September 2022).
- Cordeiro, L.; Gnatta, J.R.; Ciofi-Silva, C.L.; Price, A.; de Oliveira, N.A.; Almeida, R.M.A.; Mainardi, G.M.; Srinivas, S.; Chan, W.; Levin, A.S.S.; et al. Personal protective equipment implementation in healthcare: A scoping review. Am. J. Infect. Control 2022, 50, 898–905. [Google Scholar] [CrossRef]
- Wagner, G.J.; Aunon, F.M.; Kaplan, R.L.; Rana, Y.; Khouri, D.; Tohme, J.; Mokhbat, J. A qualitative exploration of sexual risk and HIV testing behaviors among men who have sex with men in Beirut, Lebanon. PLoS ONE 2012, 7, e45566. [Google Scholar] [CrossRef][Green Version]
- Mumtaz, G.; Hilmi, N.; McFarland, W.; Kaplan, R.L.; Akala, F.A.; Semini, I.; Riedner, G.; Tawil, O.; Wilson, D.; Abu-Raddad, L.J. Are HIV epidemics among men who have sex with men emerging in the Middle East and North Africa?: A systematic review and data synthesis. PLoS Med. 2010, 8, e1000444. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Alabbadi, A.M.; Abdel-Razeq, S.; Battah, K.; Malkawi, L.; Al-Abbadi, M.A.; Mahafzah, A. HIV Knowledge and Stigmatizing Attitude towards People Living with HIV/AIDS among Medical Students in Jordan. Int. J. Environ. Res. Public Health 2022, 19, 745. [Google Scholar] [CrossRef]
- Akour, A.; AlMuhaissen, S.A.; Nusair, M.B.; Al-Tammemi, A.a.B.; Mahmoud, N.N.; Jalouqa, S.; Alrawashdeh, M.N. The untold story of the COVID-19 pandemic: Perceptions and views towards social stigma and bullying in the shadow of COVID-19 illness in Jordan. SN Soc. Sci. 2021, 1, 240. [Google Scholar] [CrossRef] [PubMed]
- Bogart, L.M.; Thorburn, S. Are HIV/AIDS conspiracy beliefs a barrier to HIV prevention among African Americans? J. Acquir. Immune Defic. Syndr. 2005, 38, 213–218. [Google Scholar] [CrossRef]
- Nera, K.; Mora, Y.L.; Klein, P.; Roblain, A.; Van Oost, P.; Terache, J.; Klein, O. Looking for Ties with Secret Agendas During the Pandemic: Conspiracy Mentality is Associated with Reduced Trust in Political, Medical, and Scientific Institutions—But Not in Medical Personnel. Psychol. Belg. 2022, 62, 193–207. [Google Scholar] [CrossRef]
- Bogart, L.M.; Kalichman, S.C.; Simbayi, L.C. Endorsement of a genocidal HIV conspiracy as a barrier to HIV testing in South Africa. J. Acquir. Immune Defic. Syndr. 2008, 49, 115–116. [Google Scholar] [CrossRef]
- Ross, M.W.; Essien, E.J.; Torres, I. Conspiracy beliefs about the origin of HIV/AIDS in four racial/ethnic groups. J. Acquir. Immune Defic. Syndr. 2006, 41, 342–344. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Taim, D.; Eid, H.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. COVID-19 misinformation: Mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS ONE 2020, 15, e0243264. [Google Scholar] [CrossRef]
- Hartman, T.K.; Marshall, M.; Stocks, T.V.A.; McKay, R.; Bennett, K.; Butter, S.; Gibson Miller, J.; Hyland, P.; Levita, L.; Martinez, A.P.; et al. Different Conspiracy Theories Have Different Psychological and Social Determinants: Comparison of Three Theories About the Origins of the COVID-19 Virus in a Representative Sample of the UK Population. Front. Polit. Sci. 2021, 3, 642510. [Google Scholar] [CrossRef]
- Francis, A. Monkeypox Conspiracy Theories: Five False Claims about the Virus Debunked as Misinformation Spreads Online. Available online: https://inews.co.uk/news/monkeypox-conspiracy-theories-false-claims-virus-debunked-misinformation-online-1645306 (accessed on 10 August 2022).
- Agence France-Presse. ‘Very Ignorant Rumour’: Misinformation Abounds about Monkeypox. Available online: https://www.france24.com/en/live-news/20220607-very-ignorant-rumour-misinformation-abounds-about-monkeypox (accessed on 10 August 2022).
- Bettelheim, A. 1 in 5 Americans Fear They’ll Get Monkeypox. Available online: https://www.axios.com/2022/07/29/monkeypox-cases-virus-vaccine-us (accessed on 10 August 2022).
- Al Awaidy, S.T.; Khamis, F.; Sallam, M.; Ghazy, R.M.; Zaraket, H. Monkeypox Outbreak: More Queries Posed as Cases Globally Soar. Available online: https://www.researchgate.net/publication/362888810_Monkeypox_Outbreak_More_queries_posed_as_cases_globally_soar (accessed on 30 August 2022).




{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Occupational Category n (%) | ||||
|---|---|---|---|---|---|---|
| Nurse (n = 190) | Physician (n = 204) | Dentist (n = 68) | Pharmacist (n = 74) | Medical Technician 2 (n = 70) | ||
| Age in years (mean ± SD 1, median) | 39 ± 9, 39 | 33 ± 10, 29 | 32 ± 8, 30 | 35 ± 9, 33 | 35 ± 9, 34 | |
| Age | <34 years | 49 (25.79) | 140 (68.63) | 43 (63.24) | 39 (52.70) | 32 (45.71) |
| ≥34 years | 141 (74.21) | 64 (31.37) | 25 (36.76) | 35 (47.30) | 38 (54.29) | |
| Sex | Male | 44 (23.16) | 129 (63.24) | 28 (41.18) | 25 (33.78) | 12 (17.14) |
| Female | 146 (76.84) | 75 (36.76) | 40 (58.82) | 49 (66.22) | 58 (82.86) | |
| Educational level | Undergraduate | 158 (83.16) | 139 (68.14) | 51 (75.00) | 58 (78.38) | 44 (62.86) |
| Postgraduate | 32 (16.84) | 65 (31.86) | 17 (25.00) | 16 (21.62) | 26 (37.14) | |
| Residence | The Capital (Amman) | 85 (44.74) | 137 (67.16) | 49 (72.06) | 49 (66.22) | 48 (68.57) |
| Outside the Capital | 105 (55.26) | 67 (32.84) | 19 (27.94) | 25 (33.78) | 22 (31.43) | |
| Factors Associated with Higher Confidence in Diagnosis and Management of HMPX 1 | Odds Ratio (95% Confidence Interval) | p Value |
|---|---|---|
| HMPX K-Score 2 > 4 vs. HMPX K-Score ≤ 4 | 1.575 (1.044–2.378) | 0.030 |
| Nurses vs. physicians | 0.724 (0.441–1.188) | 0.201 |
| Covariates | ||
| Age < 34 years vs. ≥34 years | 1.029 (0.654–1.619) | 0.902 |
| Males vs. females | 0.927 (0.595–1.446) | 0.739 |
| Undergraduates vs. postgraduates | 0.851 (0.526–1.379) | 0.513 |
| Residence in Amman vs. outside Amman | 0.776 (0.509–1.182) | 0.238 |
| Factors Associated with Higher Embrace of Conspiracy Beliefs about Emerging Virus Infections 1 | Odds Ratio (95% Confidence Interval) | p Value |
|---|---|---|
| HMPX K-Score 2 ≤ 4 vs. HMPX K-Score > 4 | 1.496 (1.059–2.113) | 0.022 |
| Nurses vs. medical technicians | 1.792 (0.999–3.213) | 0.050 |
| Physicians vs. medical technicians | 0.495 (0.273–0.895) | 0.020 |
| Dentists vs. medical technicians | 0.670 (0.333–1.346) | 0.260 |
| Pharmacists vs. medical technicians | 0.852 (0.434–1.674) | 0.642 |
| Participants with agreement or neutral/no opinion belief in the role of male homosexuals in HMPX spread vs. those who disagreed | 2.768 (1.764–4.345) | <0.001 |
| Covariates | ||
| Age < 34 years vs. ≥34 years | 0.957 (0.665–1.377) | 0.812 |
| Males vs. females | 0.719 (0.497–1.042) | 0.081 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sallam, M.; Al-Mahzoum, K.; Al-Tammemi, A.B.; Alkurtas, M.; Mirzaei, F.; Kareem, N.; Al-Naimat, H.; Jardaneh, L.; Al-Majali, L.; AlHadidi, A.; et al. Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare 2022, 10, 1722. https://doi.org/10.3390/healthcare10091722
Sallam M, Al-Mahzoum K, Al-Tammemi AB, Alkurtas M, Mirzaei F, Kareem N, Al-Naimat H, Jardaneh L, Al-Majali L, AlHadidi A, et al. Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare. 2022; 10(9):1722. https://doi.org/10.3390/healthcare10091722
Chicago/Turabian StyleSallam, Malik, Kholoud Al-Mahzoum, Ala’a B. Al-Tammemi, Mohammed Alkurtas, Fatemeh Mirzaei, Nariman Kareem, Hala Al-Naimat, Laila Jardaneh, Laith Al-Majali, Akram AlHadidi, and et al. 2022. "Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country" Healthcare 10, no. 9: 1722. https://doi.org/10.3390/healthcare10091722
APA StyleSallam, M., Al-Mahzoum, K., Al-Tammemi, A. B., Alkurtas, M., Mirzaei, F., Kareem, N., Al-Naimat, H., Jardaneh, L., Al-Majali, L., AlHadidi, A., Al-Salahat, K., Al-Ajlouni, E., AlHadidi, N. M., Bakri, F. G., Harapan, H., & Mahafzah, A. (2022). Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare, 10(9), 1722. https://doi.org/10.3390/healthcare10091722