
Exploring People’s Knowledge of Genetics and Attitude towards Genetic Testing: A Cross-Sectional Study in a Population with a High Prevalence of Consanguinity

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Instrument
2.2. Data Analyses
3. Results
3.1. Sociodemographic Characteristics
3.2. Knowledge of Genetics
3.3. Attitudes toward Genetic Testing
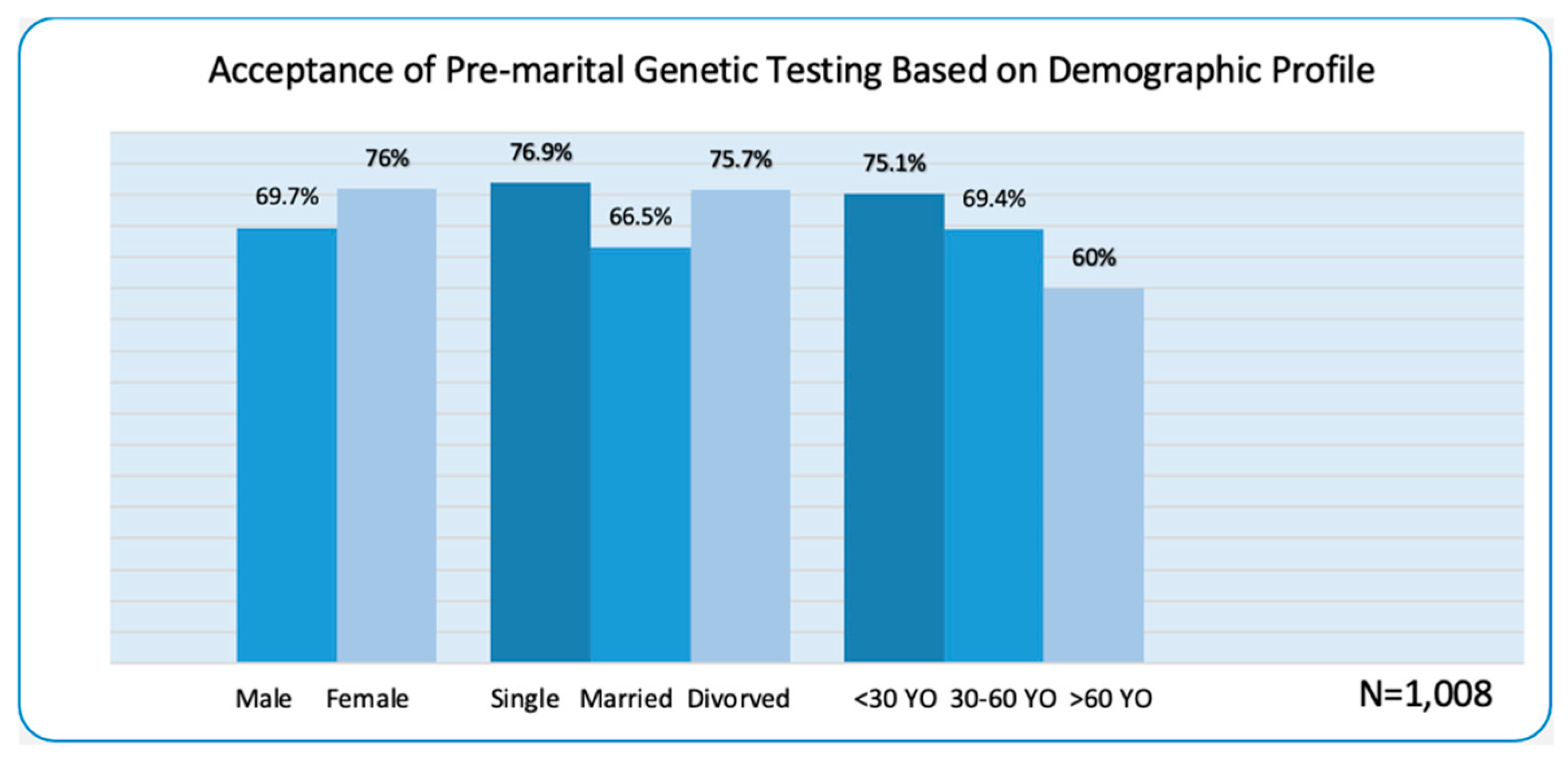
3.4. Premarital Genetic Testing
3.5. Association between Knowledge of Genetics and Attitudes to Genetic Testing with Socio-Demographic Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Turnpenny, P.; Ellard, S. Emery’s Elements of Medical Genetics, 15th ed.; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Čargonja, P.; Mavrinac, M.; Ostojić, S.; Pereza, N. The impact of needs-based education on the change of knowledge and attitudes towards medical genetics in medical students. Eur. J. Hum. Genet. 2021, 29, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Olwi, D.; Merdad, L.; Ramadan, E. Knowledge of Genetics and Attitudes Toward Genetic Testing among College Students in Saudi Arabia. Public Health Genom. 2016, 19, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.-J.; Tham, H.-W. Knowledge, Awareness, and Perception of Genetic Testing for Hereditary Disorders Among Malaysians in Klang Valley. Front. Genet. 2020, 11, 512582. [Google Scholar] [CrossRef] [PubMed]
- Jin, P. Medical genetics: Towards precision medicine. Journal of Genetics and Genomics. J. Genet. Genom. 2018, 45, 55–56. [Google Scholar] [CrossRef]
- Rubanovich, C.; Cheung, C.; Mandel, J.; Bloss, C.S. Physician preparedness for big genomic data: A review of genomic medicine education initiatives in the United States. Hum. Mol. Genet. 2018, 27, R250–R258. [Google Scholar] [CrossRef]
- Hyland, K.; Garber, K.; Dasgupta, S. From helices to health: Undergraduate medical education in genetics and genomics. Pers. Med. 2019, 16, 211–220. [Google Scholar] [CrossRef]
- McGuire, A.L.; Gabriel, S.; Tishkoff, S.A.; Wonkam, A.; Chakravarti, A.; Furlong, E.E.M.; Treutlein, B.; Meissner, A.; Chang, H.Y.; López-Bigas, N.; et al. The road ahead in genetics and genomics. Nat. Rev. Genet. 2020, 21, 581–596. [Google Scholar] [CrossRef]
- Phillips, K.A.; Deverka, P.A.; Hooker, G.W.; Douglas, M.P. Genetic test availability and spending: Where are we now? Where are we going? Health Aff. 2018, 37, 710–716. [Google Scholar] [CrossRef]
- Campion, M.; Goldgar, C.; Hopkin, R.J.; Prows, C.A.; Dasgupta, S. Genomic education for the next generation of healthcare providers. Genet. Med. 2019, 21, 2422–2430. [Google Scholar] [CrossRef]
- Felcone, L.H. Seeing patients through genetic lenses. Biotechnol. Health 2005, 2, 22–30. [Google Scholar]
- Etchegary, H.; Cappelli, M.; Potter, B.; Vloet, M.; Graham, I.; Walker, M.; Wilson, B. Attitude and knowledge about genetics and genetic testing. Public Health Genom. 2009, 13, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Collier, R. The downside of genetic screening. Can. Med. Assoc. J. 2012, 184, 862–864. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chokoshvili, D.; Vears, D.; Borry, P. Expanded carrier screening for monogenic disorders: Where are we now? Prenat. Diagn. 2018, 38, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Ellard, S.; Baple, E.L.; Callaway, A.; Berry, I.; Forrester, N.; Turnbull, C.; Owens, M.; Eccles, D.M.; Abbs, S.; Scott, R.; et al. ACGS Best Practice Guidelines for Variant Classification in Rare Disease 2020; ACGS Quality Subcommittee: London, UK, 2020. [Google Scholar]
- Burke, W. Genetic tests: Clinical validity and clinical utility. Curr. Protoc. Hum. Genet. 2014, 81, 9–15. [Google Scholar] [CrossRef]
- Holtzman, N.A.; Watson, M.S. Promoting safe and effective genetic testing in the United States. In Final Report of the Task Force on Genetic Testing; Johns Hopkins University Press: Baltimore, MD, USA, 1999. [Google Scholar]
- Al-Gazali, L.; Hamamy, H.; Al-Arrayad, S. Genetic disorders in the Arab world. Brit. Med. J. 2006, 333, 831–834. [Google Scholar] [CrossRef]
- Habib, F.; Varghese, J.; Afifi, N.; Barnawi, N. Genetics Counseling in Saudi Arabia. J. Nurs. Health Sci. 2015, 4, 01–06. [Google Scholar] [CrossRef]
- El Goundali, K.; Chebabe, M.; Laamiri, F.Z.; Hilali, A. The Determinants of Consanguineous Marriages among the Arab Population: A Systematic Review. Iran. J. Public Health 2022, 51, 253–265. [Google Scholar] [CrossRef]
- Bittles, A.H. Consanguinity in Context, Cambridge Studies in Biological and Evolutionary Anthropology; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Qari, A.A.; Balobaid, A.S.; Rawashdeh, R.R.; Al-Sayed, M.D. The development of genetic counseling services and training program in Saudi Arabia. J. Genet. Couns. 2013, 22, 835–838. [Google Scholar] [CrossRef]
- Lkuraya, F.S. Genetics and genomic medicine in Saudi Arabia. Mol. Genet. Genom. Med. 2014, 2, 369–378. [Google Scholar] [CrossRef]
- Mitra, A.K.; Al-Enezi, K. Knowledge, Attitude, and Satisfaction of University Students Regarding Premarital Screening Programs in Kuwait. Eur. J. Environ. Public Health 2017, 1, 7. [Google Scholar] [CrossRef][Green Version]
- Al-Aam, J.; Alhashem, A. Genetic Disorder in the Arab World: An Overview of Medical Genetic Services in Saudi Arabia. 2018. Available online: https://cags.org.ae/contentfiles/uploads/files/chapter%203.pdf (accessed on 13 December 2021).
- Memish, Z.A.; Owaidah, T.M.; Saeedi, M.Y. Marked regional variations in the prevalence of sickle cell disease and β-thalassemia in Saudi Arabia: Findings from the premarital screening and genetic counseling program. J. Epidemiol. Glob. Health 2011, 1, 61–68. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Melaibari, M.; Shilbayeh, S.; Kabli, A. University Students’ Knowledge, Attitudes, and Practices Towards the National Premarital Screening Program of Saudi Arabia. J. Egypt. Public Health Assoc. 2017, 92, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Moussa, S.; Al-Zaylai, F.; Al-Shammari, B.; Al-Malaq, K.; Al-Shammari, S.; Al-Shammari, T. Knowledge and attitude towards premarital screening and genetic counseling program among female university students, Hail region, Saudi Arabia. Int. J. Med. Health Res. 2018, 4, 1–6. [Google Scholar]
- Jallinoja, P.; Aro, A.R. Does Knowledge Make a Difference? The Association Between Knowledge About Genes and Attitudes Toward Gene Tests. J. Health Commun. 2000, 5, 29–39. [Google Scholar] [CrossRef]
- Molster, C.; Charles, T.; Samanek, A.; O’Leary, P. Australian study on public knowledge of human genetics and health. Public Health Genom. 2008, 12, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Chokoshvili, D.; Belmans, C.; Poncelet, R.; Sanders, S.; Vaes, D.; Vears, D.; Janssens, S.; Huys, I.; Borry, P. Public Views on Genetics and Genetic Testing: A Survey of the General Public in Belgium. Genet. Test. Mol. Biomark. 2017, 21, 195–201. [Google Scholar] [CrossRef]
- Almomani, B.A.; Al-Keilani, M.S.; Al-Sawalha, N.A. Knowledge, and views about genetics: A public-based cross-sectional study. Eur. J. Hum. Genet. 2020, 28, 417–423. [Google Scholar] [CrossRef]
- Gerard, A.; Noblin, S.; Hashmi, S.S.; Bean, A.J.; Bergstrom, K.; Hurst, C.B.; Mattox, W.; Stevens, B. Undergraduate Student Perceptions and Awareness of Genetic Counseling. J. Genet. Couns. 2018, 28, 27–39. [Google Scholar] [CrossRef]
- Hashemi-Soteh, M.B.; Nejad, A.V.; Ataei, G.; Tafazoli, A.; Ghasemi, D.; Siamy, R. Knowledge and attitude toward genetic diseases and genetic tests among pre-marriage individuals: A cross-sectional study in northern Iran. Int. J. Reprod. Biomed. 2019, 17, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Condit, C.M. Public Attitudes and Beliefs About Genetics. Annu. Rev. Genom. Hum. Genet. 2010, 11, 339–359. [Google Scholar] [CrossRef]
- Hamilton, J.G.; Hutson, S.P.; Frohnmayer, A.E.; Han, P.K.J.; Peters, J.A.; Carr, A.G.; Alter, B.P. Genetic Information-Seeking Behaviors and Knowledge among Family Members and Patients with Inherited Bone Marrow Failure Syndromes. J. Genet. Couns. 2014, 24, 760–770. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, M.S.; Irfan, U.M. The knowledge, attitude and perception of saudi adult population on consanguinity and genetic disorders. In Proceedings of the International Conference on Advances in Nursing, Pharmaceutical and Medical Sciences: ANPMS-2017, Kuala Lumpur, Malaysia, 20–21 November 2017. [Google Scholar]
- Madani, R. The new image of Saudi cultural shift; MDL Beast music festival; Saudi Vision 2030. Cogent Arts Humanit. 2022, 9, 2105511. [Google Scholar] [CrossRef]
- Karaeva, M.A.; Khaskov, E.B.; Mitberg, B.A.; Kulnitskiy, I.A.; Perezhogin, L.A.; Ivanov, V.N.; Denisov, A.N.; Kirichenko, V.Z. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Antoun, J.; Zgheib, N.K.; Ashkar, K. Education may improve the underutilization of genetic services by middle eastern primary care practitioners. Genet. Test Mol. Biomark. 2010, 14, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Etchegary, H. Public attitudes toward genetic risk testing and its role in healthcare. Pers. Med. 2014, 11, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Oliveri, S.; Masiero, M.; Arnaboldi, P.; Cutica, I.; Fioretti, C.; Pravettoni, G. Health Orientation, Knowledge, and Attitudes towards Genetic Testing and Personalized Genomic Services: Preliminary Data from an Italian Sample. BioMed Res. Int. 2016, 2016, 6824581. [Google Scholar] [CrossRef]
- Hann, K.E.J.; for the PROMISE Study Team; Freeman, M.; Fraser, L.; Waller, J.; Sanderson, S.C.; Rahman, B.; Side, L.; Gessler, S.; Lanceley, A. Awareness, knowledge, perceptions, and attitudes towards genetic testing for cancer risk among ethnic minority groups: A systematic review. BMC Public Health 2017, 17, 503. [Google Scholar] [CrossRef]
- Arafah, A.; AlJawadi, M.H.; Aldheefi, M.; Rehman, M.U. Attitude and awareness of public towards genetic testing in Riyadh, Saudi Arabia. Saudi J. Biol. Sci. 2020, 28, 255–261. [Google Scholar] [CrossRef]
- Kvaratskhelia, E.; Chokoshvili, D.; Kvintradze, M.; Surmava, S.; Dzagoevi, K.; Borry, P.; Abzianidze, E. Public attitudes towards the genetic testing in Georgia. J. Community Genet. 2021, 12, 407–414. [Google Scholar] [CrossRef]
- Abdo, N.; Ibraheem, N.; Obeidat, N.; Graboski-Bauer, A.; Batieha, A.; Altamimi, N.; Khatatbih, M. Knowledge, Attitudes, and Practices of Women Toward Prenatal Genetic Testing. Epigenet. Insights 2018, 11, 2516865718813122. [Google Scholar] [CrossRef]
- Balobaid, A.; Qari, A.; Al-Zaidan, H. Genetic counselors’ scope of practice and challenges in genetic counseling services in Saudi Arabia. Int. J. Pediatr. Adolesc. Med. 2016, 3, 1–6. [Google Scholar] [CrossRef] [PubMed]
- El-Mouzan, M.I.; Al-Salloum, A.A.; Al-Herbish, A.S.; Qurachi, M.M.; Al-Omar, A.A. Regional variations in the prevalence of consanguinity in Saudi Arabia. Saudi Med. J. 2007, 28, 1881–1884. [Google Scholar] [PubMed]
- Tadmouri, G.O.; Nair, P.; Obeid, T.; Ali, M.T.A.; Khaja, N.A.; Hamamy, H.A. Consanguinity and reproductive health among Arabs. Reprod. Health 2009, 6, 17. [Google Scholar] [CrossRef] [PubMed]
- Alhowiti, A.; Shaqran, T. Premarital screening program knowledge and attitude among Saudi University students in Tabuk city 2019. Int. J. Med. Res. Health Sci. 2019, 8, 75–84. [Google Scholar]
- Alnaqeb, D.; Hamamy, H.; Youssef, A.M.; Al-Rubeaan, K. Assessment of Knowledge, Attitude, and Practice towards Consanguineous Marriages among Cohort of Multiethnic Health Care Providers in Saudi Arabia. J. Biosoc. Sci. 2016, 50, 1–18. [Google Scholar] [CrossRef]
- General Authority for Statistics (GASTAT) Report. 2020. Available online: https://www.stats.gov.sa/en (accessed on 17 October 2022).


{kind=link}
| Socio-Demographic Characteristics | Frequency | Percentage |
|---|---|---|
| Age | ||
| Below 30-years old | 655 | 65 |
| 30–60-years old | 343 | 34 |
| Above 60-years old | 10 | 1 |
| Gender | ||
| Male | 475 | 47.1 |
| Female | 533 | 52.9 |
| Current Level of Education | ||
| Didn’t study | 9 | 0.9 |
| Elementary | 18 | 1.8 |
| Middle school | 33 | 3.3 |
| High school | 204 | 20.2 |
| Under-graduate | 641 | 63.6 |
| Post-graduate | 103 | 10.2 |
| Marital status | ||
| Single | 624 | 61.9 |
| Married | 337 | 33.4 |
| Divorced | 37 | 3.7 |
| Widow/widower | 10 | 1.0 |
| Family Income per month | ||
| Enough | 493 | 48.9 |
| Enough and allows saving | 388 | 38.5 |
| Not enough | 83 | 8.2 |
| Not enough and leads to financial debt | 44 | 4.4 |
| Residence | ||
| Riyadh | 777 | 77.1 |
| Other Regions | 231 | 22.9 |
| Consanguineous Marriage | ||
| Born from Consanguineous Marriage | 471 | 46.7 |
| Born from Non-Consanguineous Marriage | 537 | 53.3 |
| Statements | % of Correct Answers | % of Incorrect Answers | “I Am Not Sure Answers” |
|---|---|---|---|
| 1. It is possible to see a gene with the naked eye. (False) | 71.2 | 26.2 | 2.6 |
| 2. Genes control the characteristics we inherit from our parents. (True) | 78.4 | 19.3 | 2.3 |
| 3. All body parts have the same genes. (True) | 21.3 | 70.4 | 8.2 |
| 4. Each of us has variations in our genes that make it more likely to get certain diseases. (True) | 29.2 | 61.4 | 9.4 |
| 5. Half of your genes come from your mother and a half from your father. (True) | 66.5 | 28.7 | 4.8 |
| 6. Healthy parents can have a child with an inherited disease. (True) | 70.4 | 26.4 | 3.1 |
| 7. The carrier of a disease gene may be completely healthy. (True) | 65.7 | 29.2 | 4.7 |
| 8. If a person is a carrier of a disease gene, it means that they have the disease. (False) | 60.6 | 35.8 | 3.5 |
| 9. The child of a disease gene carrier is always also a carrier of the same disease. (False) | 41.4 | 51.8 | 6.8 |
| 10. All serious diseases (diseases that could be disabling or fatal at an early age), are here ditary. (False) | 39.2 | 53.3 | 7.5 |
| 11. If your close relatives have diabetes or cancer, you are more likely to develop the disease. (True) | 71.4 | 23.7 | 4.9 |
| 12. The onset of certain diseases not only depends on genes but also environment and lifestyle. (True) | 70.3 | 28.4 | 1.2 |
| 13. Some genetic diseases can be controlled by following a healthy lifestyle. (True) | 71.0 | 25.2 | 3.8 |
| 14. A person’s race and ethnicity can affect how likely they will get a disease. (True) | 61.5 | 34.4 | 4.1 |
| 15. Consanguineous marriages increase the risk of having a child with a genetic disease. (True) | 80.2 | 17.6 | 2.2 |
| Statements | % Agree to Strongly Agree | % Disagree to Strongly Disagree |
|---|---|---|
| 1. I am interested in my genetic predisposition to diseases. | 86.6 | 13.4 |
| 2. I would take a genetic profiling test to know whether I am at risk of developing diseases. | 81.0 | 19.0 |
| 3. I would get tested only for disorders that are considered treatable or preventable. | 61.4 | 38.5 |
| 4. I would consider having my newborn child genetically tested to learn which diseases they may develop in adulthood. | 82.3 | 17.7 |
| 5. I am afraid that the results of a genetic test may fall into the wrong hands. | 58.3 | 41.7 |
| 6. I am worried that due to genetic testing, disabled people will be less accepted in our society. | 40.4 | 59.6 |
| 7. I am apprehensive that a genetic test result may result in cancelation of marriage. | 42.4 | 57.6 |
| 8. All couples planning a pregnancy should have a possibility to have a carrier test. | 88.6 | 11.3 |
| 9. Carrier testing will lead to higher anxiety among women who want to become pregnant. | 63.2 | 36.8 |
| 10. Carrier testing for some diseases may lead to an inferior image of people affected with these diseases. | 44.8 | 55.2 |
| 11. Everyone should be able to decide whether or not to undergo carrier testing. | 70.0 | 30.0 |
| 12. It is irresponsible for couples who are willing to have children to refuse carrier testing. | 76.0 | 24.0 |
| Socio-Demographic Characteristics | Knowledge in Genetics | Attitude to Genetic Testing | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | p-Value | Mean | SD | p-Value | ||
| Gender | 0.001 * | 0.001 * | |||||
| Male | 9.371 | 0.123 | 2.677 | 0.015 | |||
| Female | 10.026 | 0.102 | 2.776 | 0.014 | |||
| Age | 0.035 * | 0.166 | |||||
| Below 30 | 9.815 | 0.098 | 2.745 | 0.013 | |||
| 30–60 | 9.889 | 0.144 | 2.696 | 0.185 | |||
| Above 60 | 9.900 | 0.983 | 2.725 | 0.115 | |||
| Level of Education | 0.001 * | 0.065 | |||||
| Elementary | 8.333 | 0.498 | 2.694 | 0.084 | |||
| Middle School | 8.576 | 0.413 | 2.654 | 0.047 | |||
| High School | 9.138 | 0.192 | 2.681 | 0.023 | |||
| College | 9.963 | 0.096 | 2.847 | 0.129 | |||
| Post-graduate | 10.146 | 0.246 | 2.734 | 0.034 | |||
| Did not study | 7.444 | 0.669 | 0.583 | 0.108 | |||
| Marital Status | 0.016 * | 0.098 | |||||
| Single | 9.774 | 0.102 | 2.744 | 0.013 | |||
| Married | 9.664 | 0.139 | 2.707 | 0.018 | |||
| Divorced | 9.540 | 0.392 | 2.673 | 0.048 | |||
| Widow | 8.600 | 0.618 | 2.592 | 0.110 | |||
| Family income | 0.001 * | 0.001 * | |||||
| Enough & allow saving | 9.525 | 0.115 | 2.712 | 0.015 | |||
| Enough | 10.235 | 0.118 | 2.780 | 0.017 | |||
| Not enough | 8.952 | 0.278 | 2.639 | 0.032 | |||
| Residence | 0.063 | 0.047 * | |||||
| Riyadh | 9.746 | 0.089 | 2.734 | 0.012 | |||
| Other Regions | 9.619 | 0.178 | 2.705 | 0.021 | |||
| Family History: | 0.043 * | 0.014 * | |||||
| Born from consanguineous Marriage | 9.607 | 0.119 | 2.697 | 0.015 | |||
| Non-consanguineous marriage | 9.814 | 0.108 | 2.755 | 0.014 | |||
| Socio-Demographic Characteristics | Knowledge in Genetics | Attitudes to Genetic Testing | ||||||
|---|---|---|---|---|---|---|---|---|
| Coefficients | Std. Error | t-Value | p-Value | Coefficients | Std. Error | t-Value | p-Value | |
| (Constant) | 6.430 | 0.682 | 9.428 | 0.000 | 2.467 | 0.089 | 27.864 | 0.000 |
| Age | 0.003 | 0.010 | 0.318 | 0.751 | −0.002 | 0.001 | −1.183 | 0.237 |
| Gender | 0.778 | 0.163 | 4.787 | 0.000 ** | 0.103 | 0.021 | 4.856 | 0.000 ** |
| Current Level of Education | 0.526 | 0.105 | 4.997 | 0.000 ** | 0.031 | 0.014 | 2.236 | 0.026 ** |
| Marital Status | −0.115 | 0.171 | −0.669 | 0.504 | −0.015 | 0.022 | −0.684 | 0.494 |
| Family Income (per Month) | −0.001 | 0.100 | −0.010 | 0.992 | −0.010 | 0.013 | −0.739 | 0.460 |
| Place of Origin (Riyadh or Other Regions) | −0.080 | 0.192 | −0.417 | 0.677 | −0.011 | 0.025 | −0.438 | 0.662 |
| Born from Consanguineous or Non-Consanguineous Marriage | 0.178 | 0.158 | 1.128 | 0.259 | 0.054 | 0.020 | 2.637 | 0.009 ** |
| Knowledge in Genetics | Attitudes to Genetic Testing | |||||||
| Regression | Residual | Total | Regression | Residual | Total | |||
| df | 7 | 1000 | 1007 | 7 | 1000 | 1007 | ||
| Sum of Squares | 286.550 | 6223.869 | 6510.419 | 4.761 | 104.926 | 109.687 | ||
| R2 | 0.044 | 0.043 | 0.044 | 0.043 | ||||
| R2 (adj) | 0.037 | 0.037 | 0.037 | 0.037 | ||||
| F | 6.577 | 6.483 | 6.577 | 6.483 | ||||
| Sig | 0.000 ** | 0.000 ** | 0.000 ** | 0.000 ** | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alotaibi, A.; Alkhaldi, N.K.; AlNassir, A.M.; AlAyoubi, L.A.; AlMalki, N.A.; Almughyiri, R.A.; AlDosary, R.H.; Cordero, M.A.W. Exploring People’s Knowledge of Genetics and Attitude towards Genetic Testing: A Cross-Sectional Study in a Population with a High Prevalence of Consanguinity. Healthcare 2022, 10, 2227. https://doi.org/10.3390/healthcare10112227
Alotaibi A, Alkhaldi NK, AlNassir AM, AlAyoubi LA, AlMalki NA, Almughyiri RA, AlDosary RH, Cordero MAW. Exploring People’s Knowledge of Genetics and Attitude towards Genetic Testing: A Cross-Sectional Study in a Population with a High Prevalence of Consanguinity. Healthcare. 2022; 10(11):2227. https://doi.org/10.3390/healthcare10112227
Chicago/Turabian StyleAlotaibi, Amal, Njoud Khaled Alkhaldi, Areej Mustafa AlNassir, Leenah Ayman AlAyoubi, Nada Abdulrahman AlMalki, Rahaf Abdullah Almughyiri, Reem Hussain AlDosary, and Mary Anne Wong Cordero. 2022. "Exploring People’s Knowledge of Genetics and Attitude towards Genetic Testing: A Cross-Sectional Study in a Population with a High Prevalence of Consanguinity" Healthcare 10, no. 11: 2227. https://doi.org/10.3390/healthcare10112227
APA StyleAlotaibi, A., Alkhaldi, N. K., AlNassir, A. M., AlAyoubi, L. A., AlMalki, N. A., Almughyiri, R. A., AlDosary, R. H., & Cordero, M. A. W. (2022). Exploring People’s Knowledge of Genetics and Attitude towards Genetic Testing: A Cross-Sectional Study in a Population with a High Prevalence of Consanguinity. Healthcare, 10(11), 2227. https://doi.org/10.3390/healthcare10112227