Weight Management for Students with Attention-Deficit Hyperactivity Disorder (ADHD): A Qualitative Study



{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Participants’ Recruitment
2.3. Recruitment and Procedure
2.4. Data Analysis
3. Results
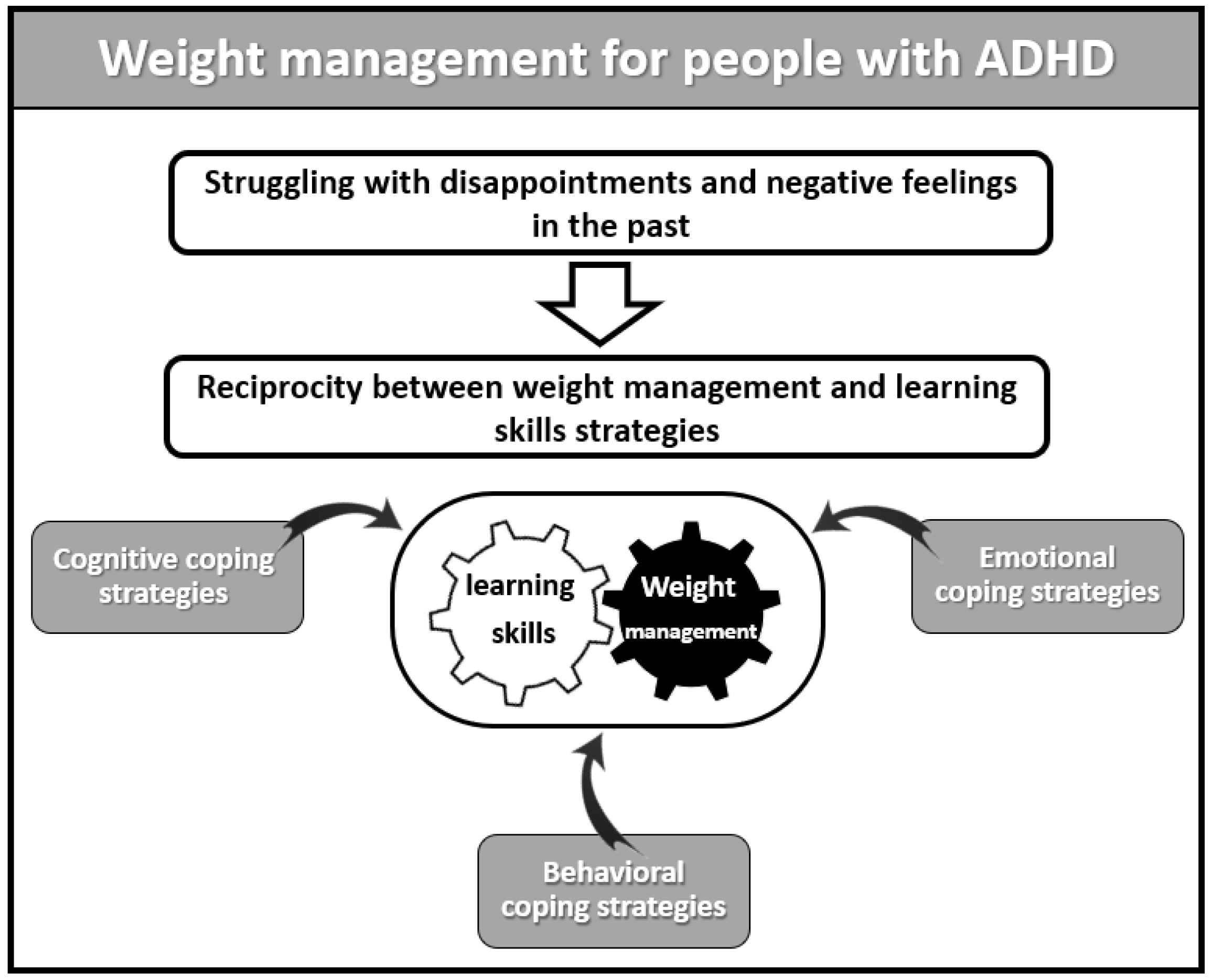
3.1. Struggling with Disappointments and Negative Feelings in the Past
“I used to cope with situations such as exams, which brought strong negative emotions. Food used to calm me down. Food was ‘my best friend’ and a source of comfort and reduction of fear, tension, and stress in moments of distress.”
“In the past, I tended to fantasize about and imagine high-fat and high-sugar foods, such as cakes and pastries, almost automatically, and in the end, I gave up and ate them.”
“Whenever I carried out the eating plan perfectly, I felt successful and valuable, and every time I ate something that wasn’t on the meal plan, I felt like a complete failure and self-blamed, like- you’re not worth anything, you’re damaged and incapable.”
3.2. Reciprocity between Weight Management and Learning Skills Strategies
- A.
- Cognitive Coping Strategies
“Nowadays, I see coping as a continuous process that has ups and downs, and I try to see my coping as containing different shades of grey and in terms of progress.”
“In the past, I used to focus on my suffering and on what I didn’t have, and I gained weight because others hurt me. But now, there is the language of action, and efficacy, focusing on positivity, optimism, and hope. I’ve become more active, cooking, and preparing food in advance and exercising according to a schedule.”
“I noticed that nowadays, I focus on positive feelings and achievements I have attained. I am experiencing a similar change in the academic field. I focus less on the struggles I had experienced in the past due to my ADHD and focus on the strengths that have led me to success and achievements today.”
“I’ve matured, and today, I am open to observing the unhealthy behaviors I had in the past. In the past, if one day I overate, then I would fast the next day. Today, when I overeat, I try to put myself together and continue with the healthy and balanced eating plan as usual.”
“Being attentive to myself also helped me discern real feelings of hunger and repletion…. This inner discussion helps me to identify what causes me to overeat. For example, watching chocolate commercials and smelling pastries are risky for me.”
“My weight change is due to a deep understanding of what is essential in life. For the first time in my life, I put myself and my health first and committed to taking actions that support this value.”
“I have proved to myself that I can finally make myself feel good and promote my health… I finally see that I can fill that void in me because of the failures I’ve experienced over the years.”
“The feeling of success in my process of weight-control and change of eating habits makes me feel good and encourages me to believe I can successfully cope with other challenges in my life.”
- B.
- Behavioral Coping Strategies
“The first stage of adopting healthy behaviors was changing the foods I brought into my home. I identified healthy foods that I find tasty and that give me pleasure and satisfaction.”
“My current journey shows abilities that I didn’t know I had, like being able to persevere. For example, if I didn’t finish my studies, I quit. But nowadays, for weight-maintenance and control, I find myself striving, coping, and succeeding.”
“Using a journal to write my eating gives me immediate feedback to control consumption and plan the rest of the day accordingly.”
“Documenting my eating in the journal allows me to create an inner dialogue and take care of the situation in real time. I find myself, albeit partially, managing to control other areas that are related to studying.”
“Promoting health isn’t just weight-control; instead, it’s about promoting a healthy lifestyle that must include exercise.”
“I use learning management skills, like creating a list of necessary ingredients. Thus, I’ve experienced a meaningful improvement in my organizational skills. From organizing material for an exam to organizing documents connected to my household affairs. I can better distinguish between what is essential and what isn’t.”
“I ask myself questions, like, what happened? What led me to deviate from the original plan? What do I really need right now? Is it really a particular food or something else? If the answer is still that I need food, I ask myself what type of food it will be, so it will give me pleasure and repletion.”
“I feel that this skill of reflecting and asking questions about my eating helps me cope with other areas, such as interpersonal conflicts, relations with professors, friends, and my partner.”
- C.
- Emotional Coping Strategies
“In the past, I ate whenever I felt anxious or stressed. Nowadays, when I think about the urge to eat, I turn to activities that please me, such as drawing mandalas. This activity helps me to be with myself, identify the cause of the distress or anxiety and calm down.”
“During the current change, I understood that there is no real danger; I was more scared of the discomfort of being stressed than of the actual occurrence itself.”
“In the support group, I received encouragement and compliments from the other participants. They strengthened my self-efficacy and my self-belief and made me feel very good about myself. When I feel good about myself, I manage to lose weight.”
“Every few months, I look at pictures from my fat period and remember the hard feeling I experienced, and this way, I reinforce myself to continue and change my situation.”
“I feel good about myself, also because the experience of success adds to my motivation. I have more energy and physical strength to perform tasks in my life than before. I feel lighter, more awake, and vital, and I am more willing to perform tasks in other areas of life that I used to put off until the last minute.”
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- LaRose, J.G.; Leahey, T.M.; Hill, J.O.; Wing, R.R. Differences in motivations and weight loss behaviors in young adults and older adults in the national weight control registry. Obesity 2013, 21, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Moreira-Maja, C.R.; St Fleur, D.; Morcillo-Peñalver, C.; Rohde, L.A.; Faraone, S.V. Association between ADHD and obesity: A systematic review and meta-analysis. Am. J. Psychiatry 2016, 173, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Tate, D.F.; Lytle, L.; Polzien, K.; Diamond, M.; Leonard, K.R.; Jakicic, J.M.; Johnson, K.C.; Olson, C.M.; Patrick, K.; Svetkey, L.P.; et al. Deconstructing weight management interventions for young adults: Looking inside the black box of the EARLY consortium trials. Obesity 2019, 27, 1085–1098. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Tate, D.; Espeland, M.; Gorin, A.; LaRose, J.G.; Robichaud, E.F.; Erickson, K.; Perdue, L.; Bahnson, J.; Lewis, C.E. Weight gain prevention in young adults: Design of the study of novel approaches to weight gain prevention (SNAP) randomized controlled trial. BMC Public Health 2013, 13, 300. [Google Scholar] [CrossRef] [PubMed]
- Hanć, T. ADHD as a risk factor for obesity. Current state of research. Psychiatr. Polska 2018, 52, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Altfas, J.R. Prevalence of attention deficit/hyperactivity disorder among adults in obesity treatment. BMC Psychiatry 2002, 2, 9. [Google Scholar] [CrossRef]
- Fleming, J.; Levy, L. Eating disorders in women with ADHD. In Gender Issues and AD/HD: Research, Diagnosis and Treatment; Silver Springs Advantage Books: Silver Spring, MD, USA, 2002; pp. 411–426. [Google Scholar]
- Nigg, J.T.; Johnstone, J.M.; Musser, E.D.; Long, H.G.; Willoughby, M.T.; Shannon, J. Attention-deficit/hyperactivity disorder (ADHD) and being overweight/obesity: New data and meta-analysis. Clin. Psychol. Rev. 2016, 43, 67–79. [Google Scholar] [CrossRef]
- Sung, H.; Siegel, R.L.; Torre, L.A.; Pearson-Stuttard, J.; Islami, F.; Fedewa, S.A.; Goding Sauer, A.; Shuval, K.; Gapstur, S.M.; Jacobs, E.J.; et al. Global patterns in excess body weight and the associated cancer burden. CA Cancer J. Clin. 2018, 69, 88–112. [Google Scholar] [CrossRef]
- Wong, M.C.; McCarthy, C.; Fearnbach, N.; Yang, S.; Shepherd, J.; Heymsfield, S.B. Emergence of the obesity epidemic: 6-decade visualization with humanoid avatars. Am. J. Clin. Nutr. 2022, 115, 1189–1193. [Google Scholar] [CrossRef]
- Hershko, S.; Cortese, S.; Ert, E.; Aronis, A.; Maeir, A.; Pollak, Y. Food perceptions in adults with and without ADHD. Psychopathology 2022, 55, 292–300. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®)—American Psychiatric Association. 2013. Available online: https://books.google.nl/books?id=-JivBAAAQBAJ&lr=&source=gbs_navlinks_s (accessed on 29 March 2021).
- Young, S.; Morris, R.; Toone, B.; Tyson, C. Planning ability in adults with attention-deficit/hyperactivity disorder. Neuropsychology 2007, 21, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S. Emotions and interpersonal relationships: Toward a person-centered conceptualization of emotions and coping. J. Personal. 2006, 74, 9–46. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Connor-Smith, J. Personality and coping. Annu. Rev. Psychol. 2010, 61, 679–704. [Google Scholar] [CrossRef]
- Park, C.L.; Fenster, J.R. Stress-related growth: Predictors of occurrence and correlates with psychological adjustment. J. Soc. Clin. Psychol. 2004, 23, 195–215. [Google Scholar] [CrossRef]
- Babb, K.A.; Levine, L.J.; Arseneault, J.M. Shifting gears: Coping flexibility in children with and without ADHD. Int. J. Behav. Dev. 2010, 34, 10–23. [Google Scholar] [CrossRef]
- Overbey, G.A.; Snell, W.E.; Callis, K.E. Subclinical ADHD, stress, and coping in romantic relationships of university students. J. Atten. Disord. 2011, 15, 67–78. [Google Scholar] [CrossRef]
- Weller, S.C.; Vickers, B.; Bernard, H.R.; Blackburn, A.M.; Borgatti, S.; Gravlee, C.C.; Johnson, J.C. Open-ended interview questions and saturation. PLoS ONE 2018, 13, e0198606. [Google Scholar] [CrossRef]
- LaDonna, K.A.; Taylor, T.; Lingard, L. Why open-ended survey questions are unlikely to support rigorous qualitative insights. Acad. Med. 2018, 93, 347–349. [Google Scholar] [CrossRef]
- Botes, A. Qualitative research in nursing—Advancing the humanistic imperative. Health SA Gesondheid 1996, 1, 31. [Google Scholar] [CrossRef]
- Smith, J.A. Evaluating the contribution of interpretative phenomenological analysis. Health Psychol. Rev. 2011, 5, 9–27. [Google Scholar] [CrossRef]
- El Archi, S.; Cortese, S.; Ballon, N.; Réveillère, C.; De Luca, A.; Barrault, S.; Brunault, P. Negative affectivity and emotion dysregulation as mediators between ADHD and disordered eating: A systematic review. Nutrients 2020, 12, 3292. [Google Scholar] [CrossRef] [PubMed]
- Brod, M.; Pohlman, B.; Lasser, R.; Hodgkins, P. Comparison of the burden of illness for adults with ADHD across seven countries: A qualitative study. Health Qual. Life Outcomes 2012, 10, 47. [Google Scholar] [CrossRef]
- Chung, Y.R.; Hong, J.W.; Kim, B.B.; Kim, J.S.; Noh, I.S.; Wee, J.H.; Kim, N.H.; Bae, S.M.; Lim, M.H. ADHD, suicidal ideation, depression, anxiety, self-esteem, and alcohol problem in Korean juvenile delinquency. Medicine 2020, 99, e19423. [Google Scholar] [CrossRef] [PubMed]
- Ahnemark, E.; Di Schiena, M.; Fredman, A.C.; Medin, E.; Söderling, J.K.; Ginsberg, Y. Health-related quality of life and burden of illness in adults with newly diagnosed attention-deficit/hyperactivity disorder in Sweden. BMC Psychiatry 2018, 18, 223. [Google Scholar] [CrossRef] [PubMed]
- Hodgkins, P.; Montejano, L.; Sasané, R.; Huse, D. Cost of illness and comorbidities in adults diagnosed with attention-deficit/hyperactivity disorder. Prim. Care Companion CNS Disord. 2011, 13, 26160. [Google Scholar] [CrossRef]
- Instanes, J.T.; Klungsøyr, K.; Halmøy, A.; Fasmer, O.B.; Haavik, J. Adult ADHD and comorbid somatic disease: A systematic literature review. J. Atten. Disord. 2018, 22, 203–228. [Google Scholar] [CrossRef]
- Bridgett, D.J.; Oddi, K.; Laake, L.M.; Murdock, K.W.; Bachmann, M.N. Integrating and differentiating aspects of self-regulation: Effortful control, executive functioning, and links to negative affectivity. Emotion 2013, 13, 47–63. [Google Scholar] [CrossRef]
- Kofler, M.J.; Irwin, L.N.; Soto, E.F.; Groves, N.B.; Harmon, S.L.; Sarver, D.E. Executive functioning heterogeneity in pediatric ADHD. J. Abnorm. Child Psychol. 2019, 47, 273–286. [Google Scholar] [CrossRef]
- Butzbach, M.; Fuermaier, A.; Aschenbrenner, S.; Weisbrod, M.; Tucha, L.; Tucha, O. Metacognition in adult ADHD: Subjective and objective perspectives on self-awareness of cognitive functioning. J. Neural Transm. 2021, 128, 939–955. [Google Scholar] [CrossRef]
- Beck, A.T. The current state of cognitive therapy. Arch. Gen. Psychiatry 2005, 62, 953. [Google Scholar] [CrossRef]
- Butler, A.; Chapman, J.; Forman, E.; Beck, A.T. The empirical status of cognitive-behavioral therapy: A review of meta-analyses. Clin. Psychol. Rev. 2006, 26, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Lopez, P.L.; Torrente, F.M.; Ciapponi, A.; Lischinsky, A.G.; Cetkovich-Bakmas, M.; Rojas, J.I.; Romano, M.; Manes, F.F. Cognitive-behavioural interventions for attention deficit hyperactivity disorder (ADHD) in adults. Cochrane Database Syst. Rev. 2018, 3. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Nimmo-Smith, V.; Merwood, A.; Hank, D.; Brandling, J.; Greenwood, R.; Skinner, L.; Law, S.; Patel, V.; Rai, D. Non-pharmacological interventions for adult ADHD: A systematic review. Psychol. Med. 2020, 50, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Poissant, H.; Mendrek, A.; Talbot, N.; Khoury, B.; Nolan, J. Behavioral and cognitive impacts of mindfulness-based interventions on adults with attention-deficit hyperactivity disorder: A systematic review. Behav. Neurol. 2019, 2019, 5682050. [Google Scholar] [CrossRef]
- Wadden, T.A.; Tronieri, J.S.; Butryn, M.L. Lifestyle modification approaches for the treatment of obesity in adults. Am. Psychol. 2020, 75, 235–251. [Google Scholar] [CrossRef]
- Dunn, C.; Haubenreiser, M.; Johnson, M.; Nordby, K.; Aggarwal, S.; Myer, S.; Thomas, C. Mindfulness approaches and weight loss, weight maintenance, and weight regain. Curr. Obes. Rep. 2018, 7, 37–49. [Google Scholar] [CrossRef]
- Anderson, E.; Durstine, J.L. Physical activity, exercise, and chronic diseases: A brief review. Sports Med. Health Sci. 2019, 1, 3–10. [Google Scholar] [CrossRef]
- Kushner, R.F. Weight loss strategies for treatment of obesity: Lifestyle management and pharmacotherapy. Prog. Cardiovasc. Dis. 2018, 61, 246–252. [Google Scholar] [CrossRef]
- Kayani, S.; Kiyani, T.; Wang, J.; Zagalaz Sánchez, M.L.; Kayani, S.; Qurban, H. Physical activity and academic performance: The mediating effect of self-esteem and depression. Sustainability 2018, 10, 3633. [Google Scholar] [CrossRef]
- Csikszentmihalyi, M. Beyond Boredom and Anxiety; Jossey-Bass: Hoboken, NJ, USA, 2000. [Google Scholar]
- Ashinoff, B.K.; Abu-Akel, A. Hyperfocus: The forgotten frontier of attention. Psychol. Res. 2021, 85, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Safer, D.L.; Telch, C.F.; Agras, W.S. Dialectical behavior therapy for bulimia nervosa. Am. J. Psychiatry 2001, 158, 632–634. [Google Scholar] [CrossRef] [PubMed]
- Lutz, K.F.; Burnson, C.; Hane, A.; Samuelson, A.; Maleck, S.; Poehlmann, J. Parenting stress, social support, and mother-child interactions in families of multiple and singleton preterm toddlers. Fam. Relat. 2012, 61, 642–656. [Google Scholar] [CrossRef] [PubMed]
- Byrne, S.; Barry, D.; Petry, N.M. Predictors of weight loss success. Exercise vs. dietary self-efficacy and treatment attendance. Appetite 2012, 58, 695–698. [Google Scholar] [CrossRef]
- Ahlgren, C.; Hammarström, A.; Sandberg, S.; Lindah, B.; Olsson, T.; Larsson, C.; Fjellman-Wiklund, A. Engagement in new dietary habits—Obese women’s experiences from participating in a 2-year diet intervention. Int. J. Behav. Med. 2016, 23, 84–93. [Google Scholar] [CrossRef]
- Ahmann, E.; Tuttle, L.J.; Saviet, M.; Wright, S.D. A descriptive review of ADHD coaching research: Implications for college students. J. Postsecond. Educ. Disabil. 2018, 31, 17–39. [Google Scholar]
- Eisenberg, N.; Spinrad, T.L.; Eggum, N.D. Emotion-related self-regulation and its relation to children’s maladjustment. Annu. Rev. Clin. Psychol. 2010, 6, 495–525. [Google Scholar] [CrossRef]
- Shaw, P.; Stringaris, A.; Nigg, J.; Leibenluft, E. Emotion dysregulation in attention deficit hyperactivity disorder. Am. J. Psychiatry 2014, 171, 276–293. [Google Scholar] [CrossRef]
- Deaver, C.M.; Miltenberger, R.G.; Smyth, J.; Meidinger, A.M.Y.; Crosby, R. An evaluation of affect and binge eating. Behav. Modif. 2003, 27, 578–599. [Google Scholar] [CrossRef]
- Galatzer-Levy, I.R.; Burton, C.; Bonanno, G.A. Coping flexibility, potentially traumatic life events, and resilience: A prospective study of college student adjustment. J. Soc. Clin. Psychol. 2012, 31, 542. [Google Scholar] [CrossRef]
- Kashdan, T.B.; Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 2010, 30, 865–878. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siman Tov, A.; Halevi Hochwald, I.; Tesler, R.; Green, G. Weight Management for Students with Attention-Deficit Hyperactivity Disorder (ADHD): A Qualitative Study. Healthcare 2022, 10, 2225. https://doi.org/10.3390/healthcare10112225
Siman Tov A, Halevi Hochwald I, Tesler R, Green G. Weight Management for Students with Attention-Deficit Hyperactivity Disorder (ADHD): A Qualitative Study. Healthcare. 2022; 10(11):2225. https://doi.org/10.3390/healthcare10112225
Chicago/Turabian StyleSiman Tov, Ayelet, Inbal Halevi Hochwald, Riki Tesler, and Gizell Green. 2022. "Weight Management for Students with Attention-Deficit Hyperactivity Disorder (ADHD): A Qualitative Study" Healthcare 10, no. 11: 2225. https://doi.org/10.3390/healthcare10112225
APA StyleSiman Tov, A., Halevi Hochwald, I., Tesler, R., & Green, G. (2022). Weight Management for Students with Attention-Deficit Hyperactivity Disorder (ADHD): A Qualitative Study. Healthcare, 10(11), 2225. https://doi.org/10.3390/healthcare10112225