
A Non-Randomized Combined Program of Walking and Low-Load Resistance Exercise Improves Cognitive Function and Cardiometabolic Risk Factors in Community-Dwelling Elderly Women


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Exercise Intervention
2.3. Measurements
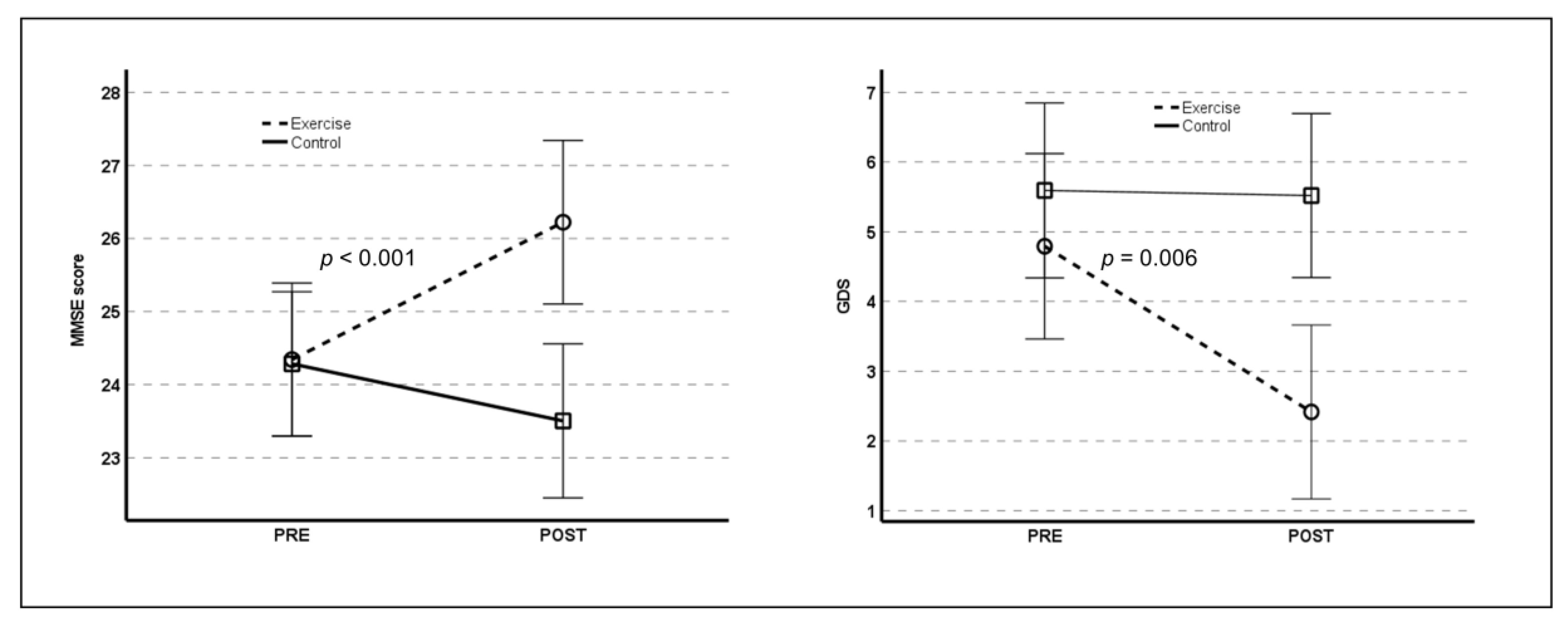
2.3.1. Cognitive Function
2.3.2. Depressive Symptoms
2.3.3. Functional Physical Capacity
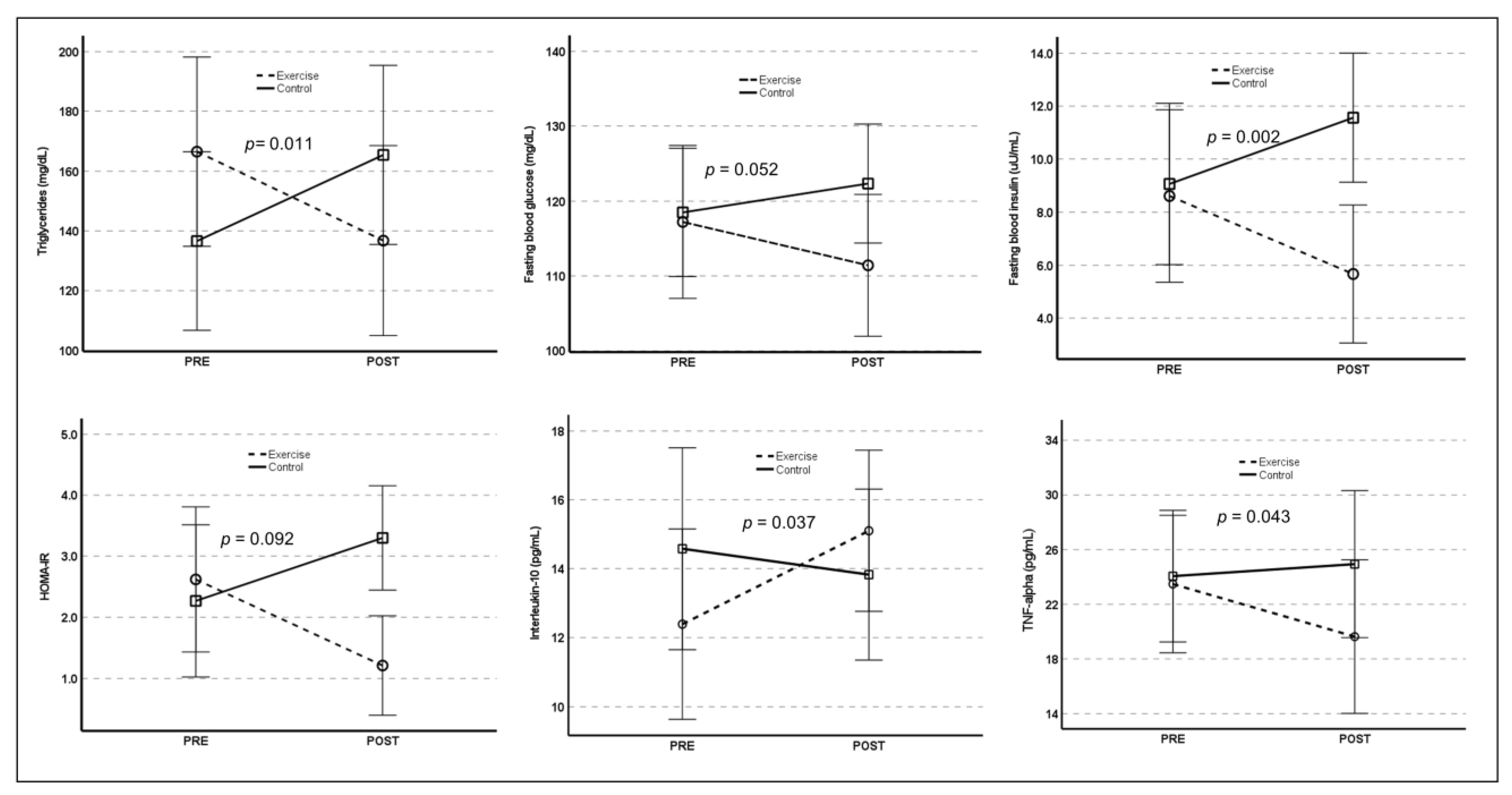
2.3.4. Cardiometabolic Risk Factors and Serum Cytokines
2.4. Statistics
3. Results
4. Discussion
4.1. Exercise Intervention and Functional Physical Capacity
4.2. Exercise Intervention and Cardiometabolic Risk Factors and Serum Cytokines
4.3. Exercise Intervention and Mental Health
4.4. Potential Explanations for the Cognitive Benefit of Exercise Intervention
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Department of Economic and Social Affairs, Population Division. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430); United Nations: New York, NY, USA, 2019.
- Marquez, P.V.; Saxena, S. Making Mental Health a Global Priority. Cerebrum 2016, 2016, cer-10-16. [Google Scholar] [PubMed]
- Klimova, B.; Valis, M.; Kuca, K. Cognitive decline in normal aging and its prevention: A review on non-pharmacological lifestyle strategies. Clin. Interv. Aging 2017, 12, 903–910. [Google Scholar] [CrossRef]
- Minhas, P.S.; Latif-Hernandez, A.; McReynolds, M.R.; Durairaj, A.S.; Wang, Q.; Rubin, A.; Joshi, A.U.; He, J.Q.; Gauba, E.; Liu, L.; et al. Restoring metabolism of myeloid cells reverses cognitive decline in ageing. Nature 2021, 590, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary behavior, exercise, and cardiovascular health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- Teixeira, C.V.; Gobbi, L.T.; Corazza, D.I.; Stella, F.; Costa, J.L.; Gobbi, S. Non-pharmacological interventions on cognitive functions in older people with mild cognitive impairment (MCI). Arch. Gerontol. Geriatr. 2021, 54, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Snowden, M.; Steinman, L.; Mochan, K.; Grodstein, F.; Prohaska, T.R.; Thurman, D.J.; Brown, D.R.; Laditka, J.N.; Soares, J.; Zweiback, D.J.; et al. Effect of exercise on cognitive performance in community-dwelling older adults: Review of intervention trials and recommendations for public health practice and research. J. Am. Geriatr. Soc. 2011, 59, 704–716. [Google Scholar] [CrossRef]
- Jin, Y.; Kim, D.; Hong, H.; Kang, H. A long-term exercise intervention reduces depressive symptoms in older Korean women. J. Sports Sci. Med. 2019, 18, 399–404. [Google Scholar]
- van de Rest, O.; van der Zwaluw, N.L.; Tieland, M.; Adam, J.J.; Hiddink, G.J.; van Loon, L.J.; de Groot, L.C. Effect of resistance-type exercise training with or without protein supplementation on cognitive functioning in frail and pre-frail elderly: Secondary analysis of a randomized, double-blind, placebo-controlled trial. Mech. Ageing Dev. 2014, 136–137, 85–93. [Google Scholar] [CrossRef]
- Fornaro, M.; Solmi, M.; Veronese, N.; De Berardis, D.; Buonaguro, E.F.; Tomasetti, C.; Perna, G.; Preti, A.; Carta, M.G. The burden of mood disorder/cerebrovascular disease comorbidity: Essential neurobiology, psychopharmacology, and physical activity interventions. Int. Rev. Psychiatry 2017, 29, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Lachman, M.E.; Neupert, S.D.; Bertrand, R.; Jette, A.M. The effects of strength training on memory in older adults. J. Aging Phys. Act. 2006, 14, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Zotcheva, E.; Håberg, A.K.; Wisløff, U.; Salvesen, Ø.; Selbæk, G.; Stensvold, D.; Ernstsen, L. Effects of 5 years aerobic exercise on cognition in older adults: The generation 100 study: A randomized controlled trial. Sports Med. 2022, 52, 1689–1699. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, P.; Suetta, C.; Caserotti, P.; Magnusson, S.P.; Kjær, M. Role of the nervous system in sarcopenia and muscle atrophy with aging: Strength training as a countermeasure. Scand. J. Med. Sci. Sports 2010, 20, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.S.; Aguiar, A.F.; Schoenfeld, B.J.; Nunes, J.P.; Cavalcante, E.F.; Cadore, E.L.; Cyrino, E.S. Effects of different resistance training systems on muscular strength and hypertrophy in resistance-trained older women. J. Strength Cond. Res. 2018, 32, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J.; Latham, N. Adverse events reported in progressive resistance strength training trials in older adults: 2 sides of a coin. Arch. Phys. Med. Rehabil. 2010, 91, 1471–1473. [Google Scholar] [CrossRef]
- Orssatto, L.D.R.; Moura, B.D.; Bezerra, E.D.S.; Andersen, L.L.; Oliveira, S.D.; Diefenthaeler, F. Influence of strength training intensity on subsequent recovery in elderly. Exp. Gerontol. 2018, 106, 232–239. [Google Scholar] [CrossRef]
- Colado, J.C.; Triplett, N.T. Effects of a short-term resistance program using elastic bands versus weight machines for sedentary middle-aged women. J. Strength Cond. Res. 2008, 22, 1441–1448. [Google Scholar] [CrossRef]
- Melchiorri, G.; Rainoldi, A. Muscle fatigue induced by two different resistances: Elastic tubing versus weight machines. J. Electromyogr. Kinesiol. 2011, 21, 954–959. [Google Scholar] [CrossRef]
- Park, J.H.; Kwon, Y.C. Modification of the mini-mental state examination for use in the elderly in a non-Western society: Part I. Development of Korean version of mini-mental state examination. Int. J. Geriatr. Psychiatry 1995, 5, 381–387. [Google Scholar] [CrossRef]
- Bae, J.N.; Cho, M.J. Development of the Korean version of the geriatric depression scale and its short form among elderly psychiatric patients. J. Psychosom. Res. 2004, 57, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Chase, J.D.; Phillips, L.J.; Brown, M. Physical activity intervention effects on physical function among community-dwelling older adults: A systematic review and meta-analysis. J. Aging Phys. Act. 2017, 25, 149–170. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, Y.; Du, S.; Wang, Q.; Xia, H.; Sun, R. Exercise interventions for improving physical function, daily living activities and quality of life in community-dwelling frail older adults: A systematic review and meta-analysis of randomized controlled trials. Geriatr. Nurs. 2020, 41, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Velilla, N.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Sáez de Asteasu, M.L.; Lucia, A.; Galbete, A.; García-Baztán, A.; Alonso-Renedo, J.; González-Glaría, B.; Gonzalo-Lázaro, M.; et al. Effect of exercise intervention on functional decline in very elderly patients during acute hospitalization: A randomized clinical trial. JAMA Intern. Med. 2019, 179, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Kwak, C.J.; Kim, Y.L.; Lee, S.M. Effects of elastic-band resistance exercise on balance, mobility and gait function, flexibility and fall efficacy in elderly people. J. Phys. Ther. Sci. 2016, 28, 3189–3196. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ji, L.; Tang, Z.; Ding, G.; Chen, X.; Lv, J.; Chen, Y.; Li, D. The association of metabolic syndrome and cognitive impairment in Jidong of China: A cross-sectional study. BMC Endocr. Disord. 2021, 21, 40. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Middleton, L.E.; Lui, L.Y.; Spira, A.P.; Stone, K.; Racine, C.; Ensrud, K.E.; Kramer, J.H. Mild cognitive impairment, dementia, and their subtypes in oldest old women. Arch. Neurol. 2011, 68, 631–636. [Google Scholar] [CrossRef]
- Campos-Peña, V.; Toral-Rios, D.; Becerril-Pérez, F.; Sánchez-Torres, C.; Delgado-Namorado, Y.; Torres-Ossorio, E.; Franco-Bocanegra, D.; Carvajal, K. Metabolic syndrome as a risk factor for Alzheimer’s disease: As Aβ a crucial factor in both pathologies? Antioxid. Redox Signal. 2017, 26, 542–560. [Google Scholar] [CrossRef] [PubMed]
- An, K.Y. Comparison between walking and moderate-to-vigorous physical activity: Associations with metabolic syndrome components in Korean older adults. Epidemiol. Health 2020, 42, e2020066. [Google Scholar] [CrossRef] [PubMed]
- Stewart, K.J.; Bacher, A.C.; Turner, K.; Lim, J.G.; Hees, P.S.; Shapiro, E.P.; Tayback, M.; Ouyang, P. Exercise and risk factors associated with metabolic syndrome in older adults. Am. J. Prev. Med. 2005, 28, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Mcleod, J.C.; Stokes, T.; Phillips, S.M. Resistance exercise training as a primary countermeasure to age-related chronic disease. Front. Physiol. 2019, 10, 645. [Google Scholar] [CrossRef] [PubMed]
- Mortimer, J.A.; Stern, Y. Physical exercise and activity may be important in reducing dementia risk at any age. Neurology 2019, 92, 362–363. [Google Scholar] [CrossRef] [PubMed]
- Guitar, N.A.; Connelly, D.M.; Nagamatsu, L.S.; Orange, J.B.; Muir-Hunter, S.W. The effects of physical exercise on executive function in community-dwelling older adults living with Alzheimer’s-type dementia: A systematic review. Ageing Res. Rev. 2018, 47, 159–167. [Google Scholar] [CrossRef]
- Galán-Arroyo, C.; Pereira-Payo, D.; Hernández-Mocholí, M.Á.; Merellano-Navarro, E.; Pérez-Gómez, J.; Rojo-Ramos, J.; Adsuar, J.C. Depression and exercise in older adults: Exercise looks after you program, user profile. Healthcare 2022, 10, 181. [Google Scholar] [CrossRef]
- Tasci, G.; Batkara, S.; Gurok, M.G.; Atmaca, M. Effect of exercise on therapeutic response in depression treatment. Psychiatry Clin. Psych. 2019, 29, 137–143. [Google Scholar] [CrossRef]
- Ernst, C.; Olson, A.K.; Pinel, J.P.; Lam, R.W.; Christie, B.R. Antidepressant effects of exercise: Evidence for an adult-neurogenesis hypothesis? J. Psychiatry Neurosci. 2006, 31, 84–92. [Google Scholar] [PubMed]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sport. Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Patten, R.K.; Pascoe, M.C.; Moreno-Asso, A.; Boyle, R.A.; Stepto, N.K.; Parker, A.G. Effectiveness of exercise interventions on mental health and health-related quality of life in women with polycystic ovary syndrome: A systematic review. BMC Public Health 2021, 21, 2310. [Google Scholar] [CrossRef] [PubMed]
- Yates, K.F.; Sweat, V.; Yau, P.L.; Turchiano, M.M.; Convit, A. Impact of metabolic syndrome on cognition and brain: A selected review of the literature. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2060–2067. [Google Scholar] [CrossRef] [PubMed]
- Peng, T.C.; Chen, W.L.; Wu, L.W.; Chang, Y.W.; Kao, T.W. Sarcopenia and cognitive impairment: A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 2695–2701. [Google Scholar] [CrossRef]
- Kim, M.; Won, C.W. Sarcopenia is associated with cognitive impairment mainly due to slow gait speed: Results from the Korean frailty and aging cohort study (KFACS). Int. J. Environ. Res. Public Health 2019, 16, 1491. [Google Scholar] [CrossRef] [PubMed]
- Sleiman, S.F.; Henry, J.; Al-Haddad, R.; El Hayek, L.; Abou Haidar, E.; Stringer, T.; Ulja, D.; Karuppagounder, S.S.; Holson, E.B.; Ratan, R.R.; et al. Exercise promotes the expression of brain-derived neurotrophic factor (BDNF) through the action of the ketone body β-hydroxybutyrate. eLife 2016, 5, e15092. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 30) | Exercise (n = 30) | Total (n = 60) | p-Value | |
|---|---|---|---|---|
| Age (years) | 73.3 ± 4.9 | 72.7 ± 4.2 | 73.0 ± 4.5 | 0.612 |
| Body mass index (kg/m2) | 24.7 ± 3.2 | 24.2 ± 3.1 | 24.5 ± 3.1 | 0.485 |
| Systolic BP (mmHg) | 128.4 ± 13.4 | 129.5 ± 10.2 | 128.9 ± 11.8 | 0.730 |
| Diastolic BP (mmHg) | 73.8 ± 9.3 | 71.1 ± 8.1 | 72.5 ± 8.7 | 0.235 |
| FBG (mg/dL) | 117.5 ± 21.3 | 118.5 ± 22.0 | 118.0 ± 21.5 | 0.868 |
| TC (mg/dL) | 166.4 ± 35.9 | 186.6 ± 42.8 | 176.5 ± 40.5 | 0.052 |
| TG (mg/dL) | 129.7 ± 86.0 | 145.5 ± 69.3 | 137.6 ± 77.8 | 0.435 |
| HDLC (mg/dL) | 49.8 ± 13.4 | 54.1 ± 12.1 | 51.9 ± 12.8 | 0.197 |
| LDLC (mg/dL) | 94.0 ± 28.8 | 102.9 ± 37.2 | 98.4 ± 33.3 | 0.308 |
| Insulin (μU/mL) | 8.9 ± 7.7 | 9.4 ± 8.6 | 9.2 ± 8.1 | 0.813 |
| HOMA-IR | 2.2 ± 2.0 | 2.5 ± 2.8 | 2.4 ± 2.5 | 0.602 |
| IL-4 (pg/mL) | 5.5 ± 2.9 | 6.6 ± 2.0 | 6.1 ± 2.5 | 0.485 |
| IL-10 (pg/mL) | 7.4 ± 3.1 | 9.6 ± 4.1 | 8.4 ± 3.5 | 0.280 |
| IL-6 (pg/mL) | 5.6 ± 2.6 | 6.5 ± 3.9 | 6.1 ± 3.3 | 0.362 |
| IL-1beta (pg/mL) | 2.3 ± 2.1 | 2.5 ± 2.0 | 2.4 ± 2.0 | 0.726 |
| TNF-α (ng/mL) | 23.7 ± 14.3 | 23.1 ± 7.9 | 23.4 ± 11.6 | 0.912 |
| UBMS (reps/30 s) | 21.4 ± 4.6 | 20.3 ± 4.7 | 20.8 ± 4.6 | 0.330 |
| LBMS (reps/30 s) | 15.8 ± 5.8 | 16.7 ± 4.4 | 16.3 ± 5.1 | 0.500 |
| Endurance (steps/2 min) | 94.0 ± 23.8 | 102.5 ± 18.4 | 98.2 ± 21.5 | 0.129 |
| UBFLX (cm) | −12.1 ± 11.0 | −13.3 ± 9.7 | −12.7 ± 10.3 | 0.657 |
| LBFLX (cm) | 9.6 ± 12.8 | 4.3 ± 10.3 | 6.9 ± 11.8 | 0.080 |
| Agility (sec) | 6.2 ± 1.6 | 5.8 ± 1.2 | 6.0 ± 1.4 | 0.284 |
| GDS (score) | 5.6 ± 3.8 | 4.7 ± 2.8 | 5.2 ± 3.4 | 0.306 |
| MMSE (score) | 24.3 ± 4.3 | 25.0 ± 2.0 | 24.7 ± 3.4 | 0.382 |
| Predictors | Unstandardized β | SE | t | 95% CI | p-Value |
|---|---|---|---|---|---|
| ΔGDS | −0.342 | 0.073 | −4.659 | −0.491~−0.190 | <0.001 |
| ΔInsulin | −0.185 | 0.044 | −4.205 | −0.275~−0.094 | <0.001 |
| ΔUBMS | 0.214 | 0.066 | 3.257 | 0.079~0.350 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kang, S.; Hong, H.; Joo, M.; Kang, H. A Non-Randomized Combined Program of Walking and Low-Load Resistance Exercise Improves Cognitive Function and Cardiometabolic Risk Factors in Community-Dwelling Elderly Women. Healthcare 2022, 10, 2106. https://doi.org/10.3390/healthcare10102106
Kim J, Kang S, Hong H, Joo M, Kang H. A Non-Randomized Combined Program of Walking and Low-Load Resistance Exercise Improves Cognitive Function and Cardiometabolic Risk Factors in Community-Dwelling Elderly Women. Healthcare. 2022; 10(10):2106. https://doi.org/10.3390/healthcare10102106
Chicago/Turabian StyleKim, Jeonghyeon, Seamon Kang, Haeryun Hong, Mingyu Joo, and Hyunsik Kang. 2022. "A Non-Randomized Combined Program of Walking and Low-Load Resistance Exercise Improves Cognitive Function and Cardiometabolic Risk Factors in Community-Dwelling Elderly Women" Healthcare 10, no. 10: 2106. https://doi.org/10.3390/healthcare10102106
APA StyleKim, J., Kang, S., Hong, H., Joo, M., & Kang, H. (2022). A Non-Randomized Combined Program of Walking and Low-Load Resistance Exercise Improves Cognitive Function and Cardiometabolic Risk Factors in Community-Dwelling Elderly Women. Healthcare, 10(10), 2106. https://doi.org/10.3390/healthcare10102106