Currently, in the field of spine surgery, various treatment strategies have been developed, are available, and will continue developing [
4]. The decision on which procedures to use is largely the responsibility of surgeons. This choice should be the preferred and familiar alternative for performing surgeons in order to minimize complications [
5,
6]. However, decisions should also be made based on “the conscientious, explicit, and judicious use of current best evidence”, as described by Sackett et al. [
7]. In an aging country with longer life expectancy, which is managed by a national healthcare system, a safer and effective treatment choice with less medical expense must be enthusiastically explored.
4.1. Database Creation
We need the information that would support the development and promotion of new safe surgical technologies, help surgeons select more effective treatment strategies with better outcomes, and that could be utilized as a resource for national healthcare policymakers to distribute public health insurance to cost-effective treatment by adjusting the surgical fee. Hence, a large-scale clinical database to record information and present an accurate view of the current Japanese situation in relation to spine surgery is essential. In the JSIS-DB, many items relating to clinical expense will be documented, for example, operative time, blood loss, and complications. These will provide us with the information required to compare various surgical procedures in terms of invasiveness and surgical risks. In addition, questions about the required resource, for example, the number of years of experience of the participating surgeons, the number of technicians/nurses, the types of implants used, and the number of days before discharge, are to be answered. This information will clarify what medical resource is required to treat the disease with the index procedures as well as the current trend of the treatment choice. As far as we could ascertain, the quality and quantity of human resources are unique items for a question about large-scale clinical databases. We believe the data from our database will help healthcare policymakers understand the effort required and difficulty of the procedures and regulate the surgical fee appropriately based on the practical costs.
Essentially, facilities with board members and councilors of the society were the intended participants, and participation in this database project was one of the requisites for applying or maintaining society councilor status. Even among these core members of the society, participation rate has not reached 100%. The cumbersome paperwork, including the application to the ethics committee and obligated e-learnings, is likely an obstacle to participation, and this complexity derives from the balance between the patients’ identity and their personal data protection. As meaningful information, particularly for revision surgeries, the individual cases have to be tracked chronologically as the same individuals. However, those individuals must not be identified personally. In the Personal Information Protection Law of our country, personal information can be utilized in an unidentifiable form if the academic research organization or group uses it for the purpose of academic research. For this reason, this registry must be conducted by the JSIS as a research organization in the form of multicenter joint research with one research plan; each facility participates as one of the joint research institutions, each with its own ethical approval for the shared research plan, and hash value is provided for each participating case to link the same individual without infringing upon his/her privacy. All the necessary documents for the procedure, including the research plan, document for the informed consent, and certificate of ethical approval by the institutional review board (IRB) at the flagship institutions, are available on the database website, with detailed information and frequently asked questions (FAQs) intending to lessen the burden of the surgeons. The database secretariat division repeatedly promoted this database and shared essential information via emails as well as on the website to encourage participation and answered any questions from participants. In this project, in addition to the ethical approval as multicenter database research by the society’s ethics committee, each participating facility was required to obtain its own ethical approval through their IRB, which makes the participating procedure more cumbersome. In some other countries, for example, the United States and certain European countries, this process has been simplified to facilitate clinical research. The United States Food and Drug Administration (FDA) makes some research exempt from IRB review, or accepts centralized IRB and joint reviews that cover all the participating facilities in multicenter clinical studies (FDA 45 CFR 46), for example, in American Academy of Orthopaedic Surgeons (AAOS) registries. Some European countries accept ethical approval by one single national ethical committee for facilities in the country to join multinational non-interventional observational clinical studies [
8]. The other reasons not to participate were that the facility had stopped operating and that there were no cases to register.
To promote data correction, non-medical data managers could start registering cases and continue to the end, including early complications within 14 days after surgery, but completing the system required a review and authentication of content by the surgeons. This registration/authentication system was intended to maintain the accuracy of the input information through the surgeons’ verification while lessening the burden on the surgeons with the help of data managers. For better data quality, we took various measures. A clear definition of each term is available in a pop-up sidebar next to the data form, and FAQs and email access to the database secretariat are available to guide a correct response (
Appendix B). In addition, several auto-check functions are built into the system. For example, when the required field is blank, red alert signs on the summary page appear one step before the completion button. Significantly deviated numbers, e.g., 105 years for age or 150 kg for body weight, require confirmation of the answer before finishing. However, the persistence of obviously wrong information, for example, 10 August 1937 as operation day, likely a case of mistaking date of surgery for date of birth, cannot be prevented. Data cleansing with perseverant correction is the ideal key, but its cost and manpower are problems that need to be solved.
4.2. Data Interpretation
More than 5400 cases were registered, and about 2500 cases were completed for all the items in the form. Roughly 3000–4500 valid answers were obtained in each item. This relatively low completion rate among the total cases can be attributed to the authentication step of the system, which must be completed by surgeons.
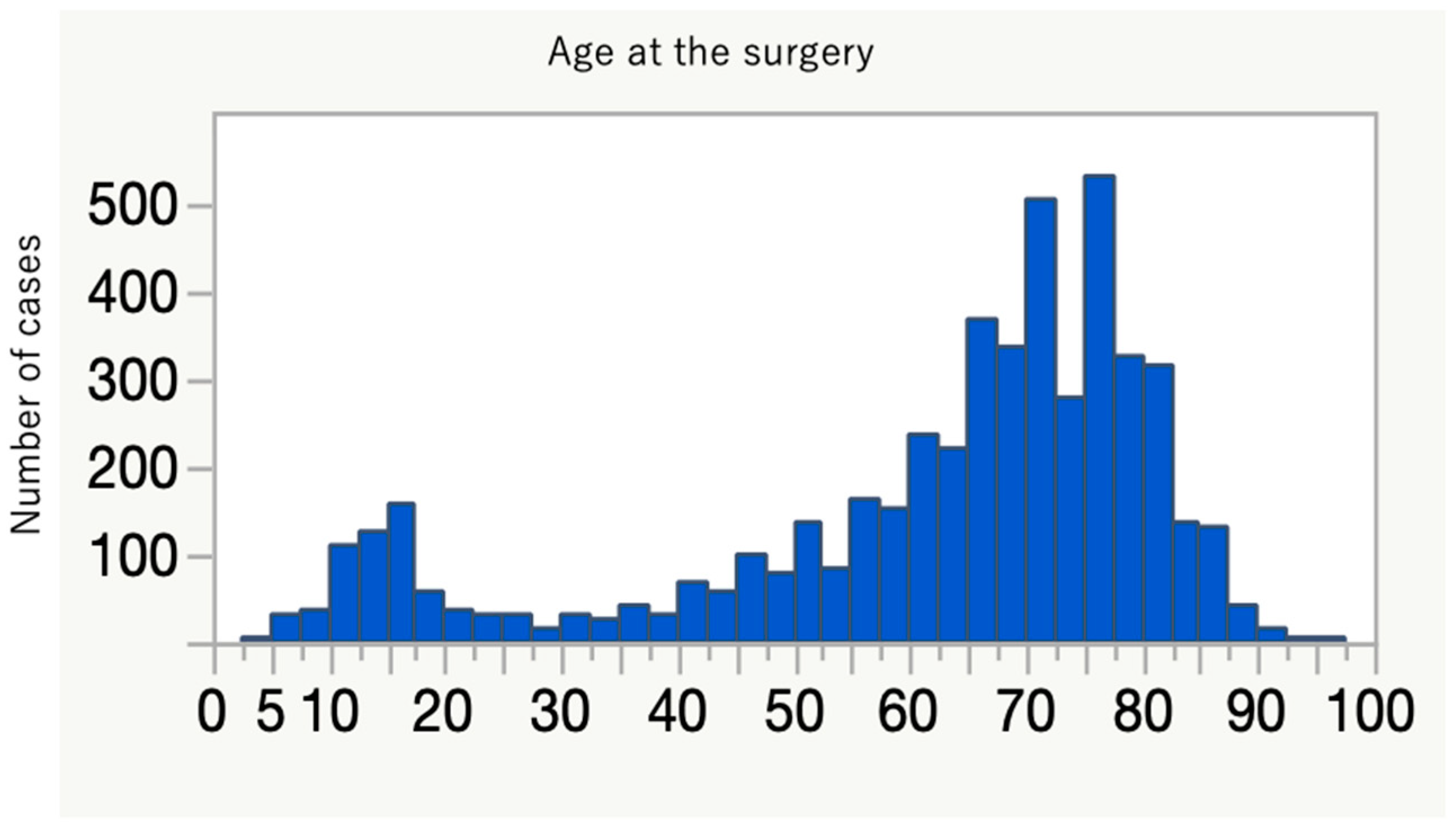
The collection of data from thousands of cases of spinal instrumentation surgeries in this short period of time in Japan is unprecedented. These data delineate the current trend of spinal instrumentation surgery in this country. The age distribution shows a two-peak pattern, with a larger spike in the elderly (
Figure 2). More than 600 people over 80 years old underwent spine instrumentation surgeries, and our patient population was much older than the reports from Italy and the U.S. on spinal fusion surgery trend [
9,
10]. The aging of Japanese spine surgery patients has been pointed out, and our result affirms this trend (
Table 9) [
3,
11]. Reflecting this aging, three-quarters of the patients had some systemic comorbidities and were classified as ASA-PS 2 to 4 (
Table 1). The younger age peak was during teenage years. There were 319 idiopathic scoliosis cases (8.9%) of primary diagnosis, and the characteristic age distribution of this disease likely explains the peak. Many of the participating facilities are regional spine centers to which scoliosis cases are referred, and this may also increase the density of surgical cases for this disease population in this database. The two most frequent diagnoses were spondylolisthesis and spinal canal stenosis (
Table 3), and the two most frequent procedures for primary surgery were posterior interbody fusion and posterior/posterolateral fusion (
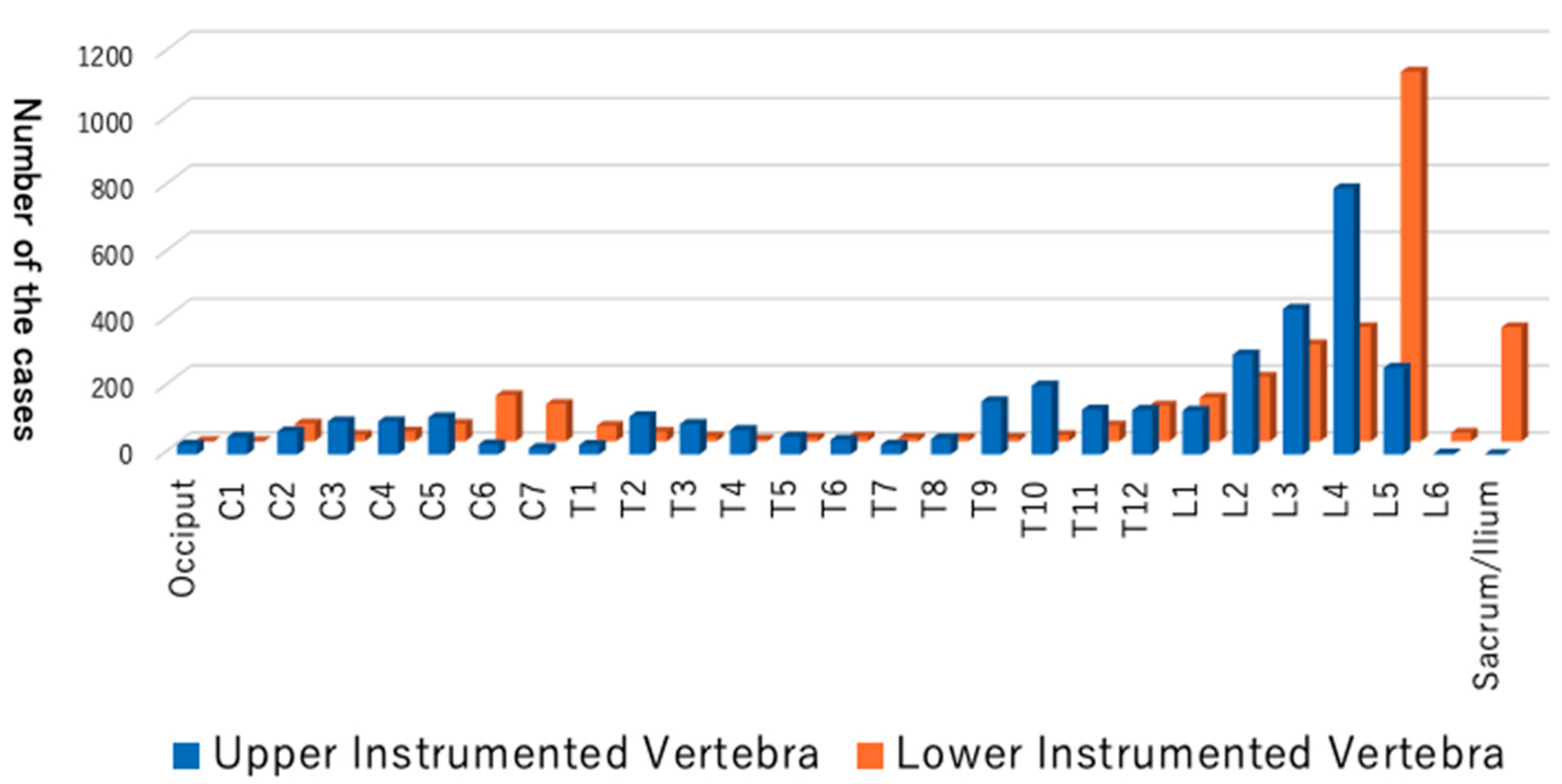
Table 4). One-third of the total cases were either of these two diagnoses for degenerative spine disease. Upper instrumented vertebra (UIV) and lower instrumented vertebra (LIV) are common in the lumbar spine (
Figure 3), and these suggest that many of the cases are degenerative lumbar spine treated with posterior procedures with short fusion levels. Kyphosis and scoliosis make up about 25% of the total cases. Traumas, including fractures and dislocations, explain less than 10% of the total (
Table 3).
In most of the cases, a certain kind of screw was used, such as pedicle screw, cortical bone trajectory, lateral mass screw, or vertebral screw. Hooks and tapes/wires are not as common anymore. Cervical artificial discs are not approved for general use at the time of this analysis, and these cases are from some trial facilities (
Table 7).
Now that the multi-center database is established and has started accumulating a large amount of data regarding spinal implant surgeries, more than 90 operating facilities have joined, and the number will increase. Geographically, these facilities cover the whole area of Japan, and this database will capture nationwide information. This report only contains the global trend of the first-year data, but more detailed information, for example, trends in age groups, geographic areas, or surgical approaches, could be extracted from this database.
One of the points to solve is the data quality and quantity. Ideally, all the surgeons thoroughly recognize the importance and the meaning of the data correction and are highly motivated to cooperate towards the better. Useful and meaningful information as the product from this database will motivate them. The requirement to stay as the councilor seems to be an effective means with which to increase the number of participating facilities. The Japanese Orthopaedic Association National Registry (JOANR) was launched in April 2020 as the surgical case registry for members accepting all kinds of orthopedic operative procedures, and it functions as the surgical case list of each surgeon to be assessed or the application and maintenance of accredited specialist status by the JOA. JSIS-DB has started sharing basic patient information with JOANR, which avoids inputting the same data twice. Concretely, after filling all the basic information in the JOANR site, the link to the JSIS-DB becomes available for spinal instrumentation cases. Through this link, basic information of the same patient is already filled in the JSIS-DB, and only additional fields should be filled out for more specific information of the spinal instrumentation surgery. This sharing is expected to collect not only more cases but also more facilities for the JSIS-DB, from those who are currently not participants of the JSIS.
In summary, JSIS-DB has been launched, and the data from the first 1.5 years have been analyzed. These data describe the trend of spinal instrumentation surgeries. The number of participating facilities is increasing, and more cases are expected to be registered. By accumulating more cases while maintaining the high quality of the data, JSIS-DB will provide powerful and useful information to improve healthcare policy and patient outcomes for spine surgery in Japan.


 ,
, 



{kind=link}
{kind=link}
{kind=link}