
Twelve-Week Lower Trapezius-Centred Muscular Training Regimen in University Archers

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
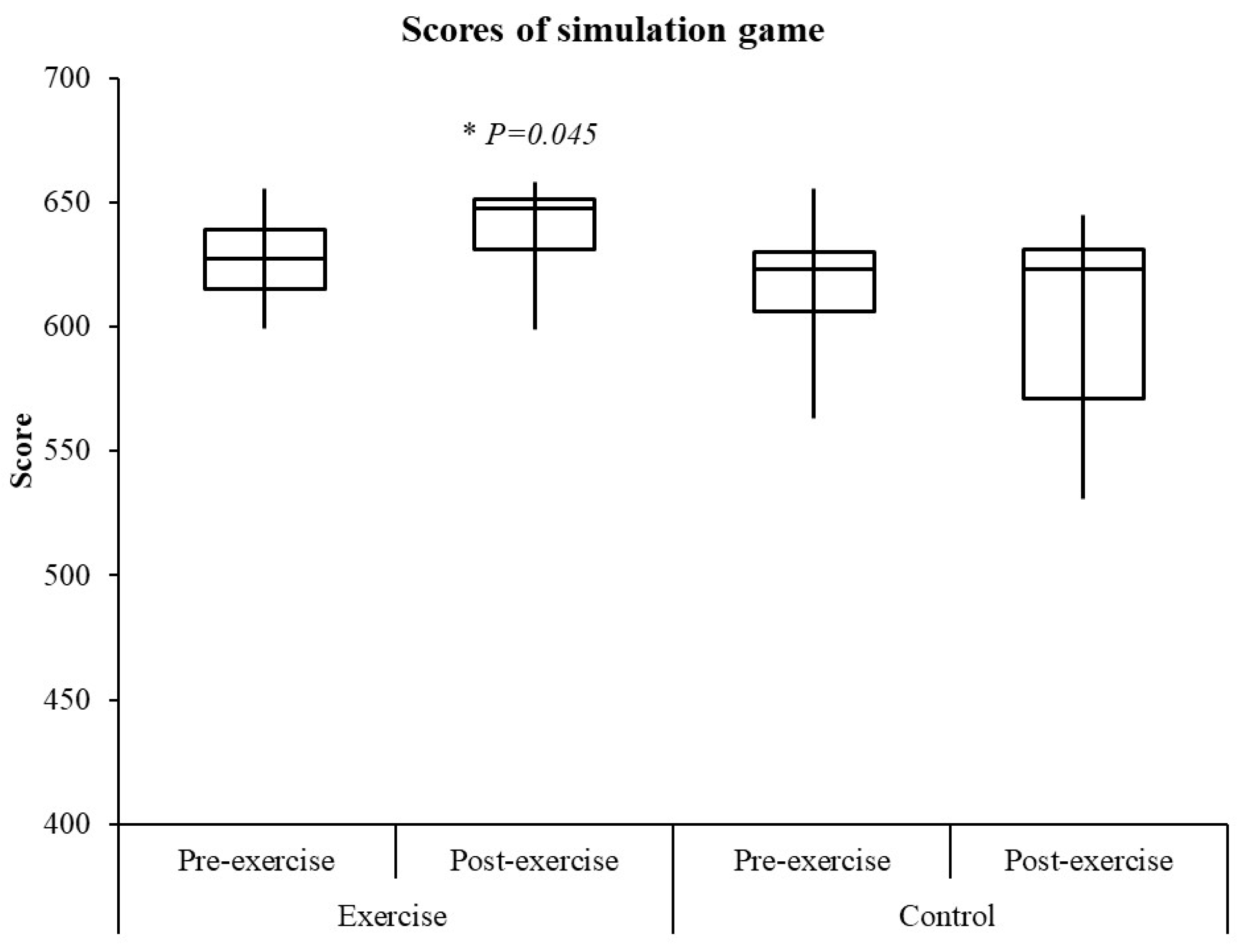
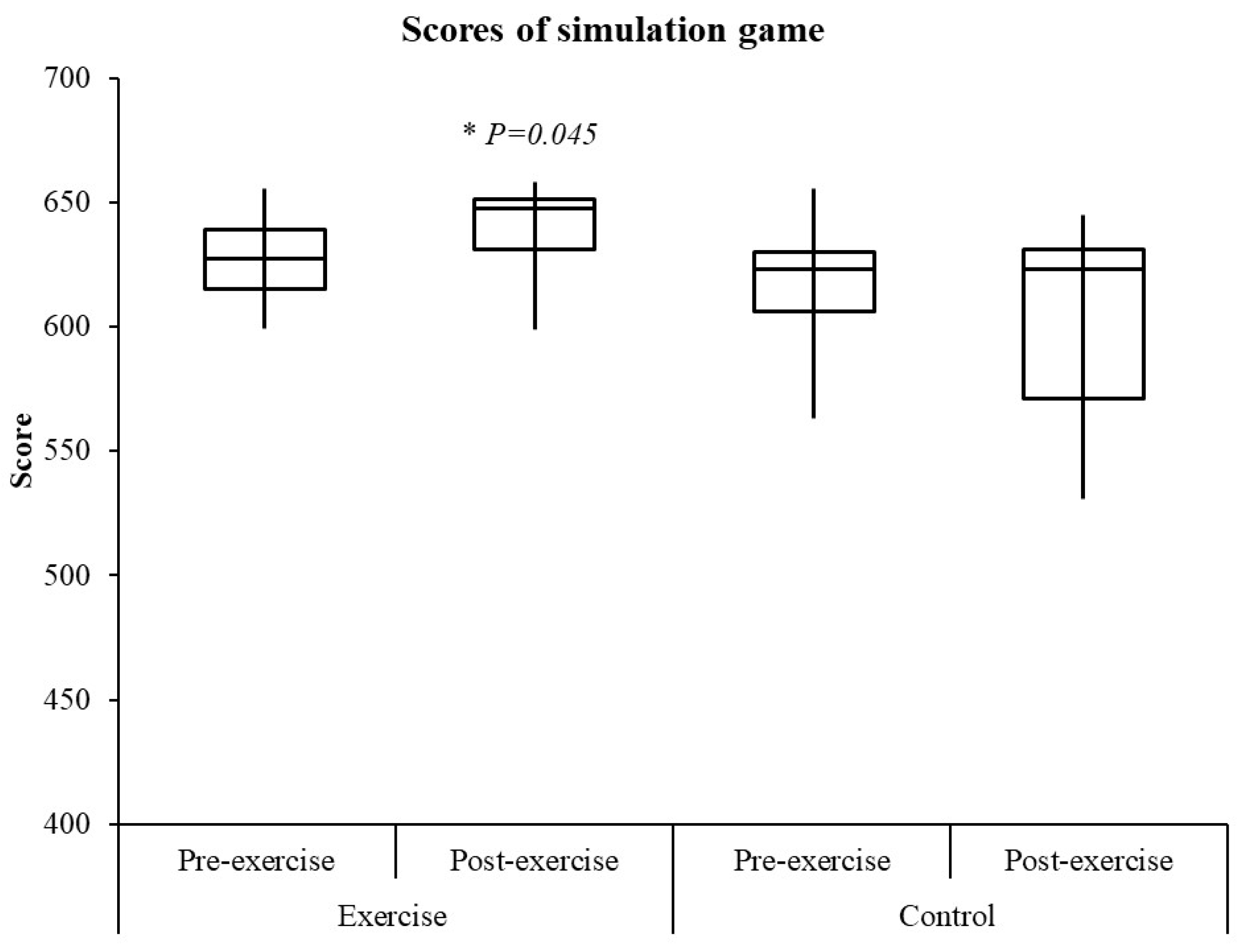
2.3. Simulation Game
2.4. Upper Limb Joint Angle Motion
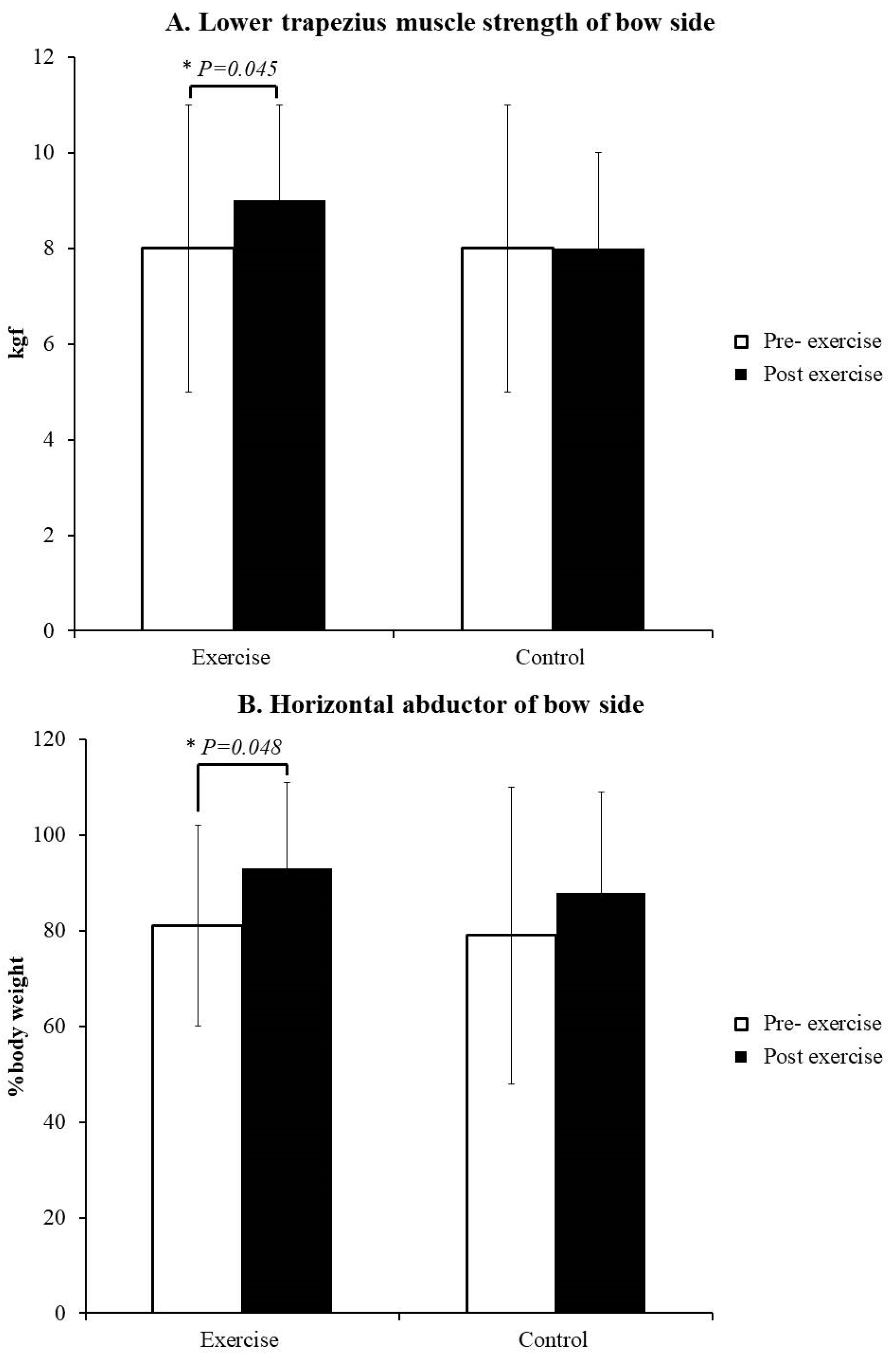
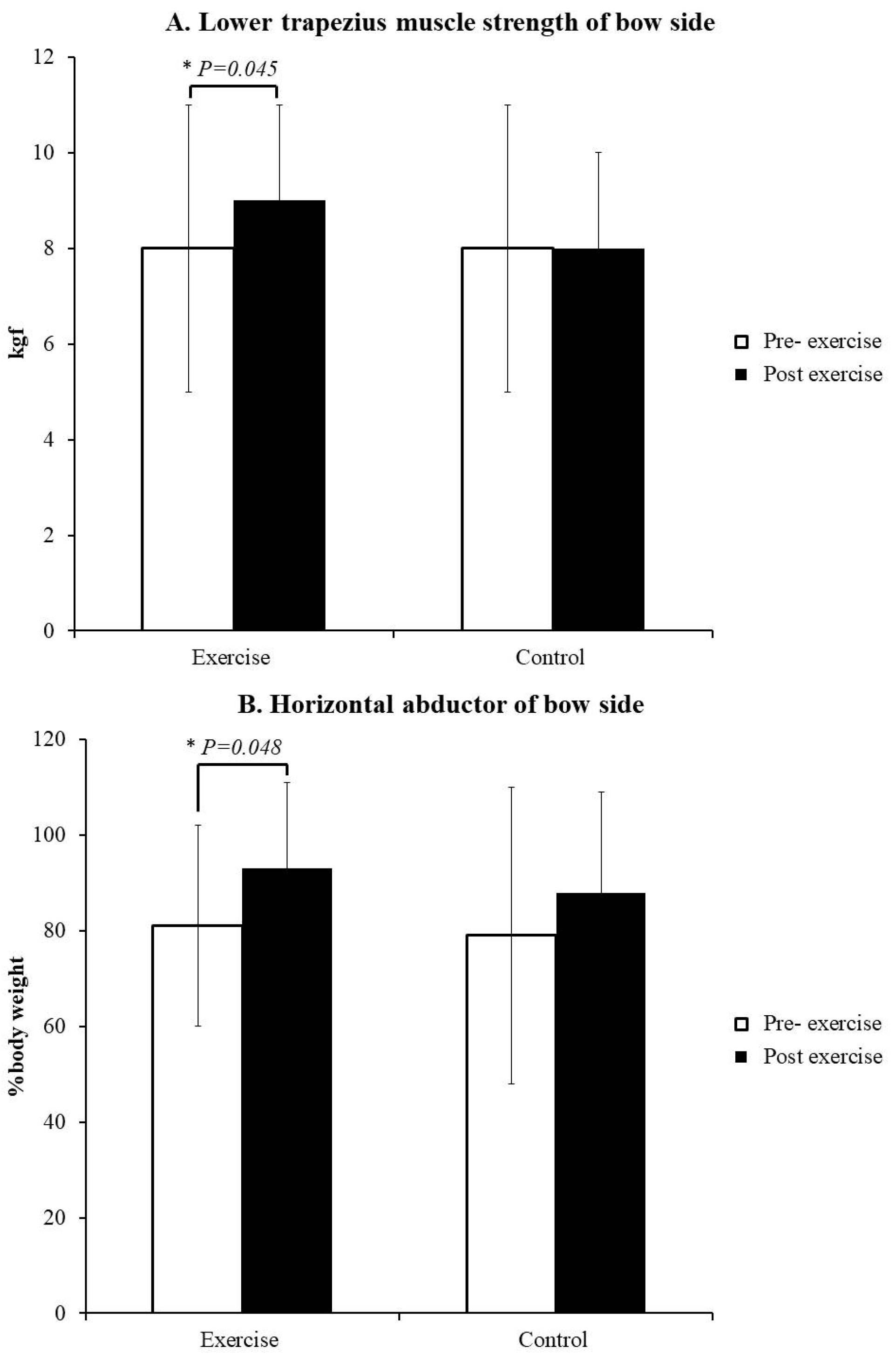
2.5. LT Strength
2.6. Shoulder Horizontal Abductor/Adductor Muscle Strength
2.7. Surface Electromyography
2.8. Additional Exercise Protocol
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taha, Z.; Musa, R.M.; Majeed, A.P.A.; Alim, M.M.; Abdullah, M.R. The identification of high potential archers based on fitness and motor ability variables: A support vector machine approach. Hum. Mov. Sci. 2018, 57, 184–193. [Google Scholar] [CrossRef]
- Leroyer, P.; van Hoecke, J.; Helal, J.N. Biomechanical study of the final push-pull in archery. J. Sports Sci. 1993, 11, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.E.; Siler, W.L.; Hoffman, D. Electromyographic analysis of bow string release in highly skilled archers. J. Sports Sci. 1990, 8, 215–221. [Google Scholar] [CrossRef]
- Mann, D.L.; Littke, N. Shoulder injuries in archery. Can. J. Sport Sci. 1989, 14, 85–92. [Google Scholar] [PubMed]
- Era, P.; Konttinen, N.; Mehto, P.; Saarela, P.; Lyytinen, H. Postural stability and skilled performance—A study on top-level and naive rifle shooters. J. Biomech. 1996, 29, 301–306. [Google Scholar] [CrossRef]
- Hung, T.C.; Liao, Y.H.; Tsai, Y.S.; Ferguson-Stegall, L.; Kuo, C.H.; Chen, C.Y. Hot water bathing impairs training adaptation in elite teen archers. Chin. J. Physiol. 2018, 61, 118–123. [Google Scholar] [CrossRef]
- Hideaki, T.; Yoko, K.; Masanobu, A. Characteristics of shooting time of the world’s top level male archery athletes. NSSU J. Sport Sci. 2012, 1, 8–12. [Google Scholar]
- Shinohara, H.; Urabe, Y. Analysis of muscular activity in archery: A comparison of skill level. J. Sports Med. Phys. Fitness 2018, 58, 1752–1758. [Google Scholar] [CrossRef]
- Clarys, J.P.; Cabri, J.; Bollens, E.; Sleeckx, R.; Taeymans, J.; Vermeiren, M.; van Reeth, G.; Voss, G. Muscular activity of different shooting distances, different release techniques, and different performance levels, with and without stabilizers, in target archery. J. Sports Sci. 1990, 8, 235–257. [Google Scholar] [CrossRef]
- Lin, J.J.; Hung, C.J.; Yang, C.C.; Chen, H.Y.; Chou, F.C.; Lu, T.W. Activation and tremor of the shoulder muscles to the demands of an archery task. J. Sports Sci. 2010, 28, 415–421. [Google Scholar] [CrossRef]
- Spratford, W.; Campbell, R. Postural stability, clicker reaction time and bow draw force predict performance in elite recurve archery. Eur. J. Sport Sci. 2017, 17, 539–545. [Google Scholar] [CrossRef]
- Shinohara, H.; Urabe, Y.; Maeda, N.; Xie, D.; Sasadai, J.; Fujii, E. Does shoulder impingement syndrome affect the shoulder kinematics and associated muscle activity in archers? J. Sports Med. Phys. Fitness 2014, 54, 772–779. [Google Scholar]
- De Mey, K.; Danneels, L.; Cagnie, B.; Borms, D.; T’Jonck, Z.; van Damme, E.; Cools, A.M. Shoulder muscle activation levels during four closed kinetic chain exercises with and without redcord slings. J. Strength Cond. Res. 2014, 28, 1626–1635. [Google Scholar] [CrossRef]
- Cools, A.M.; Johansson, F.R.; Cambier, D.C.; Velde, A.V.; Palmans, T.; Witvrouw, E.E. Descriptive profile of scapulothoracic position, strength and flexibility variables in adolescent elite tennis players. Br. J. Sports Med. 2010, 44, 678–684. [Google Scholar] [CrossRef]
- Sarro, K.J.; Viana, T.C.; de Barros, R.M.L. Relationship between bow stability and postural control in recurve archery. Eur. J. Sport Sci. 2021, 21, 515–520. [Google Scholar] [CrossRef]
- Ertan, H. Muscular activation patterns of the bow arm in recurve archery. J. Sci. Med. Sport 2009, 12, 357–360. [Google Scholar] [CrossRef]
- Ertan, H.; Soylu, A.R.; Korkusuz, F. Quantification the relationship between fita scores and emg skill indexes in archery. J. Electromyogr. Kinesiol. 2005, 15, 222–227. [Google Scholar] [CrossRef]
- Zhou, C.; Hopkins, W.G.; Mao, W.; Calvo, A.L.; Liu, H. Match performance of soccer teams in the chinese super league-effects of situational and environmental factors. Int. J. Environ. Res. Public Health 2019, 16, 4238. [Google Scholar] [CrossRef]
- Williams, C. Environmental factors affecting elite young athletes. Med. Sport Sci. 2011, 56, 150–170. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef]
- Petersen, S.M.; Wyatt, S.N. Lower trapezius muscle strength in individuals with unilateral neck pain. J. Orthop. Sports Phys. Ther. 2011, 41, 260–265. [Google Scholar] [CrossRef]
- Hu, G.; Jiang, Q.; Lee, J.Y.; Kim, Y.H.; Ko, D.H. Isokinetic strength and functional scores after rehabilitation in jiu-jitsu fighter with repair surgery of pectoralis major muscle rupture: A case report. Healthcare 2021, 9, 527. [Google Scholar] [CrossRef]
- Celik, D.; Sirmen, B.; Demirhan, M. The relationship of muscle strength and pain in subacromial impingement syndrome. Acta Orthop. Traumatol. Turc. 2011, 45, 79–84. [Google Scholar] [CrossRef]
- Iversen, V.M.; Mork, P.J.; Vasseljen, O.; Bergquist, R.; Fimland, M.S. Multiple-joint exercises using elastic resistance bands vs. Conventional resistance-training equipment: A cross-over study. Eur. J. Sport Sci. 2017, 17, 973–982. [Google Scholar] [CrossRef]
- Bergquist, R.; Iversen, V.M.; Mork, P.J.; Fimland, M.S. Muscle activity in upper-body single-joint resistance exercises with elastic resistance bands vs. Free weights. J. Hum. Kinet. 2018, 61, 5–13. [Google Scholar] [CrossRef]
- Colado, J.C.; Triplett, N.T. Effects of a short-term resistance program using elastic bands versus weight machines for sedentary middle-aged women. J. Strength Cond. Res. 2008, 22, 1441–1448. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Lee, T.D. Motor Control and Learning: A Behavioral, 5th ed.; Human Kinetics: Champaign, IL, USA, 2011. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; p. 567. [Google Scholar]
- Sawilowsky, S. New effect size rules of thumb. J. Mod. Appl. Stat. Methods 2009, 8, 467–474. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Opar, D.A.; Piatkowski, T.; Williams, M.D.; Shield, A.J. A novel device using the nordic hamstring exercise to assess eccentric knee flexor strength: A reliability and retrospective injury study. J. Orthop. Sports Phys. Ther. 2013, 43, 636–640. [Google Scholar] [CrossRef]
- Cools, A.M.; Witvrouw, E.E.; Declercq, G.A.; Vanderstraeten, G.G.; Cambier, D.C. Evaluation of isokinetic force production and associated muscle activity in the scapular rotators during a protraction-retraction movement in overhead athletes with impingement symptoms. Br. J. Sports Med. 2004, 38, 64–68. [Google Scholar] [CrossRef]
- Cools, A.M.; Witvrouw, E.E.; Declercq, G.A.; Danneels, L.A.; Cambier, D.C. Scapular muscle recruitment patterns: Trapezius muscle latency with and without impingement symptoms. Am. J. Sports Med. 2003, 31, 542–549. [Google Scholar] [CrossRef]
- Cools, A.M.; Borms, D.; Castelein, B.; Vanderstukken, F.; Johansson, F.R. Evidence-based rehabilitation of athletes with glenohumeral instability. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Ludewig, P.M.; Cook, T.M. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys. Ther. 2000, 80, 276–291. [Google Scholar] [CrossRef]
- Cools, A.M.; Declercq, G.A.; Cambier, D.C.; Mahieu, N.N.; Witvrouw, E.E. Trapezius activity and intramuscular balance during isokinetic exercise in overhead athletes with impingement symptoms. Scand. J. Med. Sci. Sports 2007, 17, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Contemori, S.; Panichi, R.; Biscarini, A. Effects of scapular retraction/protraction position and scapular elevation on shoulder girdle muscle activity during glenohumeral abduction. Hum. Mov. Sci. 2019, 64, 55–66. [Google Scholar] [CrossRef]
- Van de Velde, A.; de Mey, K.; Maenhout, A.; Calders, P.; Cools, A.M. Scapular-muscle performance: Two training programs in adolescent swimmers. J. Athl. Train. 2011, 46, 160–167, discussion 68–69. [Google Scholar] [CrossRef]
- Cools, A.M.; Palmans, T.; Johansson, F.R. Age-related, sport-specific adaptions of the shoulder girdle in elite adolescent tennis players. J. Athl. Train. 2014, 49, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Yamashiro, K.; Paulos, L.; Andrews, J.R. Shoulder muscle activity and function in common shoulder rehabilitation exercises. Sports Med. 2009, 39, 663–685. [Google Scholar] [CrossRef]
- Ludewig, P.M.; Cook, T.M.; Nawoczenski, D.A. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J. Orthop. Sports Phys. Ther. 1996, 24, 57–65. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Pre-Exercise | Post-Exercise | ES | ICC | CV(%) | TE | |||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||||||
| Exercise | Bow side | Shoulder abduction | 94 ± 6 | 91 ± 9 | 0.39 | 0.69 | 8 | 3 |
| Horizontal extension | 141 ± 20 | 140 ± 28 | 0.04 | 0.91 | 17 | 5 | ||
| Drawing side | Shoulder abduction | 120 ± 4 | 120 ± 4 | 0.01 | 0.76 | 3 | 2 | |
| Horizontal extension | 147 ± 5 | 146 ± 5 | 0.20 | 0.45 | 3 | 2 | ||
| Control | Bow side | Shoulder abduction | 95 ± 5 | 95 ± 5 | 0.01 | 0.61 | 5 | 2 |
| Horizontal extension | 130 ± 33 | 137 ± 21 | 0.25 | 0.68 | 20 | 5 | ||
| Drawing side | Shoulder abduction | 123 ± 6 | 120 ± 4 | 0.59 | 0.76 | 4 | 2 | |
| Horizontal extension | 144 ± 9 | 143 ± 9 | 0.11 | 0.94 | 6 | 3 | ||
| Pre-Exercise | Post-Exercise | ES | ICC | CV(%) | TE | |||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||||||
| Exercise | Bow side | Lower trapezius | 49 ± 24 | 42 ± 17 | 0.33 | 0.88 | 44 | 4 |
| Upper trapezius | 95 ± 35 | 69 ± 36 * | 0.73 | 0.80 | 44 | 6 | ||
| Drawing side | Lower trapezius | 38 ± 16 | 40 ± 10 | 0.15 | 0.84 | 33 | 4 | |
| Upper trapezius | 78 ± 22 | 44 ± 36 * | 1.14 | 0.47 | 55 | 6 | ||
| Deltoid posterior | 85 ± 13 | 74 ± 15 | 0.78 | 0.71 | 18 | 4 | ||
| Deltoid middle | 59 ± 12 | 59 ± 14 | 0.01 | 0.69 | 21 | 4 | ||
| Triceps brachii | 26 ± 10 | 19 ± 14 * | 0.58 | 0.88 | 55 | 4 | ||
| Biceps brachii | 42 ± 15 | 29 ± 12 *§ | 0.96 | 0.57 | 41 | 4 | ||
| Control | Bow side | Lower trapezius | 63 ± 25 | 52 ± 17 | 0.51 | 0.74 | 37 | 5 |
| Upper trapezius | 95 ± 17 | 95 ± 21 | 0.01 | 0.48 | 19 | 4 | ||
| Drawing side | Lower trapezius | 54 ± 30 | 50 ± 24 | 0.15 | 0.88 | 50 | 5 | |
| Upper trapezius | 77 ± 21 | 65 ± 30 | 0.46 | 0.37 | 36 | 5 | ||
| Deltoid posterior | 93 ± 10 | 88 ± 4 | 0.66 | 0.35 | 8 | 3 | ||
| Deltoid middle | 69 ± 16 | 56 ± 18 | 0.76 | 0.32 | 28 | 4 | ||
| Triceps brachii | 34 ± 13 | 23 ± 12 * | 0.88 | 0.77 | 46 | 4 | ||
| Biceps brachii | 54 ± 32 | 51 ± 24 | 0.11 | 0.97 | 51 | 5 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, C.-N.; Fan, C.-H.; Hsu, W.-H.; Chang, C.-F.; Yu, P.-A.; Kuo, L.-T.; Lu, B.-L.; Hsu, R.W.-W. Twelve-Week Lower Trapezius-Centred Muscular Training Regimen in University Archers. Healthcare 2022, 10, 171. https://doi.org/10.3390/healthcare10010171
Liao C-N, Fan C-H, Hsu W-H, Chang C-F, Yu P-A, Kuo L-T, Lu B-L, Hsu RW-W. Twelve-Week Lower Trapezius-Centred Muscular Training Regimen in University Archers. Healthcare. 2022; 10(1):171. https://doi.org/10.3390/healthcare10010171
Chicago/Turabian StyleLiao, Chien-Nan, Chun-Hao Fan, Wei-Hsiu Hsu, Chia-Fang Chang, Pei-An Yu, Liang-Tseng Kuo, Bo-Ling Lu, and Robert Wen-Wei Hsu. 2022. "Twelve-Week Lower Trapezius-Centred Muscular Training Regimen in University Archers" Healthcare 10, no. 1: 171. https://doi.org/10.3390/healthcare10010171
APA StyleLiao, C.-N., Fan, C.-H., Hsu, W.-H., Chang, C.-F., Yu, P.-A., Kuo, L.-T., Lu, B.-L., & Hsu, R. W.-W. (2022). Twelve-Week Lower Trapezius-Centred Muscular Training Regimen in University Archers. Healthcare, 10(1), 171. https://doi.org/10.3390/healthcare10010171