Abstract
In this paper, operating room planning and scheduling problems have been studied. In operating room planning, the allocation of patients to operating rooms and their sequencing are critical in determining the performance of operating rooms. In this paper, three surgery scheduling decisions are considered, including the number of operating rooms to open, the allocation of surgeries to operating rooms, and the sequencing of surgeries in allocated operating rooms. All the surgeries under consideration are elective, and surgery durations are considered deterministic. Further, it is considered that the surgeries have different specialties, and each operating room can accommodate a particular specialty of surgeries, i.e., heterogeneous operating rooms are considered in the current study. Before performing a surgery, setup time is required for operating room turnover and sterilization, and it is considered sequence dependent. A mixed integer nonlinear programming (MINLP) model is developed to minimize the overtime costs of operating rooms for allocation and surgery sequencing with sequence dependent setup times. An outer approximation (OA) method is proposed to solve the problem near optimally. Experiments are conducted to compare the performance of the proposed OA method with the standard mixed integer nonlinear programming model. Computational results show the efficiency of the proposed OA method. Later, a case data from a case hospital is collected and a case study is solved.
Keywords:
advanced scheduling; allocation scheduling; heterogenous operating room; mixed integer nonlinear programming; outer approximation; sequence dependent setup time MSC:
90C30
1. Introduction
The healthcare industry is one of the largest industries in the service sector [1]. Hospitals are the main units of the healthcare system. Operating rooms are considered to be one of the most critical resources of hospitals. More than 40% of the total revenue of a hospital is generated by operating rooms, and a large proportion of expenses is also associated with operating rooms [2]. In most situations, the operating rooms do not reach target utilization and hence the optimal allocation of surgeries to operating rooms is required to improve operating room utilization and cost saving. Thus, operating room planning and scheduling has attracted the attention of many researchers [3,4,5,6,7].
In literature, operating room planning and scheduling is divided into three hierarchical decision levels: strategic (long term), tactical (medium term), and operational levels (short term) [8,9]. At the strategic level, the hospital case mix is decided, hence it is also called case mix planning. Case mix planning aims to choose the ideal composition and volume of patients in a hospital [10]. At the tactical level, operating room time is divided among surgical specialties. Three scheduling policies are normally used at tactical level. In block scheduling, the operating room is fully reserved for surgeons. In modified block scheduling, some of the capacity is reserved for surgeons and the remaining capacity is shared by other surgeons. In open scheduling, surgeons share operating rooms and can move among them within a day [11,12,13]. Due to the flexibility of open scheduling, a greater number of patients can be accommodated, and hence it has been used by many researchers recently [13,14,15,16,17]. In the open scheduling policy, requests are made by the surgeons for the operating room time. These requests are made prior to the day of surgery and hence the list of elective patients is known in advance [1]. Due to its flexibility and greater patient admissions, an open scheduling policy to schedule elective patients in the operating rooms is used in the current study.
At the operational level, two major scheduling decisions are made. Firstly, a surgical case is assigned to a day and an operating room in the planning horizon, which is also known as advanced scheduling. Secondly, the sequence of surgeries in an operating room is planned, which is referred to as allocation scheduling [18]. In literature, operational level problems are the most studied problems [3,19,20,21,22,23]. However, the literature focuses more on advanced scheduling [2,9,24,25]. Some studies considered advanced and allocation scheduling simultaneously [3,13,22,23]. The present study investigates simultaneously the advanced scheduling and allocation scheduling of surgeries in operating rooms at operational level.
In operating rooms, surgeries of different types are performed that require different equipment during operations. Each operating room is equipped with different types of equipment and resources, which limits the ability of operating rooms to accommodate all surgery types [1]. In the current study, operating rooms are considered heterogeneous, and each operating room can only perform certain types of surgeries.
One surgery scheduling problem that occurs when operating rooms are shared among patients from different specialties in an open scheduling policy is that some setup work is required for preparing and sterilizing the operating room before the start of surgery. This is referred to as operating room turnover time. This setup work is dependent on the preceding surgery and is hence referred to as sequence dependent setup time. In literature, mostly the turnover time is incorporated into the surgery duration [26,27,28]. The reason for this is convenience or compliance with the practice of the hospital under study. Some researchers linked the cleaning or turnover time with the duration of surgeries; for example, smaller cleaning times for smaller surgeries and vice versa [4,29]. However, it is not realistic to incorporate operating room turnover time in surgery duration because it is dependent on the preceding surgery. Moreover, it is not practical to assume turnover or sterilization time based on the length of the surgery. Thus, it needs to be considered separately, and the current study explicitly considers the sequence dependent setup times for advanced and allocation scheduling of surgeries in heterogeneous operating rooms, which is limited in literature [1,30,31].
In the literature, various mathematical programming methods are used to formulate operating room planning and scheduling problems, including linear programming [32,33,34,35], goal programming [36,37,38], integer programming [39,40,41], mixed integer programming [15,19,42,43,44], quadratic programming [45,46,47,48], and constraint programming [1].
Within mixed integer programming, mixed integer linear programming is most widely used. Moosavi and Ebrahimnejad [4] developed a mixed integer linear programming model to solve tactical and operational problems integrated with upstream and downstream wards. In another study, Moosavi and Ebrahimnejad [3] solved combined advanced and allocation scheduling problems. They developed a mixed integer linear programming model for the solution of the problem. Oliveira et al. [20] developed an integer linear programming model to incorporate patient prioritization with the patient scheduling problem.
In some articles, mixed integer nonlinear programming is used to solve patient scheduling problems. Heydari and Soudi [49] developed a mixed integer nonlinear programming model (MINLP) for advanced and allocation scheduling problems. They proposed two stage stochastic programming methods to solve the problem. Batun et al. [12] determined the allocation and start time of surgeries in operating rooms using stochastic programming. Zhao and Li [1] developed a mixed integer nonlinear programming model to solve the elective surgery scheduling problem. They also developed a constraint programming model and compared the performance of a constraint programming model with a MINLP model.
In the literature, various solution methods, such as the exact method, heuristics, and metaheuristics, have been used to solve operating room planning and scheduling problems. Exact solution methods optimally solve operating room planning and scheduling problems. The advantage of exact solution methods is that they provide a single optimal solution. The exact methods used in literature include column generation [24,50,51,52,53], dynamic programming [54,55,56,57,58], branch and bound [42,59,60,61,62], branch and price [54,55,63,64,65], and branch and cut methods [66,67]. In addition, researchers have considered heuristics [68,69,70], hybrid methods [71,72], and metaheuristics [44,62,73] for operating room planning and scheduling problems. The operating room planning and scheduling is NP-hard [74], and therefore, different metaheuristics have also been applied to solve this problem in reasonable computation to get near-optimal results [75,76]. Most researchers have studied operating room planning and scheduling problems using simulated annealing [77], genetic algorithm [44], constructive heuristics [4], hybrid simulated annealing [72], Tabu search [23,78], hill climbing algorithms [79], artificial bee colony algorithm [31], and ant colony algorithm [80,81], etc. The metaheuristics are the most common in operating room planning and scheduling literature [44,62,72,82]. Due to the complexity of mixed integer nonlinear programming models, difficulties can arise in solving the problems. For large sized problems, using exact methods takes a lot of time, and in many situations a feasible solution is not obtained within a reasonable computational time [1]. Hence the present study is focused on developing a solution method of MINLP to obtain a near-optimal solution within a reasonable computational time without affecting the quality of the solution.
In the current study, a mixed integer nonlinear programming model like that of Zhao and Li [1] is developed and solved using the outer approximation method. Our study is different from that of Zhao and Li [1] in that the method we have used to solve the developed model has not been reported as being used for operating room planning and scheduling so far. Hence, the current study solved the advanced and allocation scheduling of elective patients with sequence dependent set up times and considering heterogenous operating rooms. Further, it proposes a method to approximately solve the developed MINLP model and investigates the quality of the solution obtained by the proposed method.
The primary contribution of the study is to consider the sequence dependent setup times between the successive surgeries in multiple heterogeneous operating rooms. In addition, a solution method based on the outer approximation method has been proposed to solve the operating room planning and scheduling problem. The rest of the paper is organized as follows: the problem description and mathematical formulation is presented in Section 2, Section 3 presents the proposed outer approximation method, Section 4 shows computational experiments and results, and Section 5 concludes the paper and gives some future research directions.
2. Problem Description and Mathematical Formulation
The problem considered in the current study is to determine the number of open operating rooms, the allocation of patients to operating rooms, and the sequencing of patients within the allocated operating rooms. The operating rooms are heterogeneous, i.e., only specific types of surgeries can be performed in the operating rooms. Elective patients are considered, and their surgery durations are taken as deterministic. On a tactical level, an open scheduling policy is used, i.e., operating rooms are shared among specialties. When operating rooms are shared by surgeons from different specialties, sequence dependent setup times occur, which are given special consideration in the current study. Further, it is assumed that surgeons, anesthesiologists, and other supporting staff are available and do not become the bottleneck. This section presents the mixed integer nonlinear program (MINLP) built for the elective surgery scheduling problem. Before formulating the model, the following notations are defined in Table 1:

Table 1.
Notations.
The mixed integer nonlinear programing model of the problem is developed as:
The objective function (1) consists of two terms. The first term represents fixed costs, and the second term represents the overtime costs of operating rooms. In the objective function, the decision variable is used, which is binary variable. This decision variable is 1 if the operating room is open and its value is 0 if the operating room is closed, which is first decision, i.e., the number of open operating rooms. The decision variable is used in the objective function, which is the overtime, and is calculated in Equation (6), which is based on the allocation and sequence of patients in the operating room and uses the value of . The binary decision variable is used for the allocation of a surgery and its position in the sequence in the operating room.
Constraint (2) specifies that the surgery type must meet the requirements of an operating room. It gives the condition that a surgery can only be performed in a compatible operating room with the required equipment. Constraint (3) guarantees that each surgery should be scheduled once and avoids the scheduling of the same surgery in multiple operating rooms at the same time. Constraint (4) represents the precedence of surgeries in the operating room. This constraint maintains the sequence of surgeries and ensures that all positions in a sequence are occupied in a numerical order. Constraint (5) states that surgeries can only be scheduled in open operating rooms and that if an operating room is closed, no surgeries can be assigned to that operating room. Constraints (6) and (7) define the length of overtime of the operating room. Note that constraint (6) is quadratic, as set-up times are sequence dependent. Equation (6) consists of three terms: the first term calculates the total surgery duration of all the patients assigned to an operating room, the second term calculates the sequence-dependent setup times, and the third indicates the standard operating time in an operating room. This equation provides information on whether there will be overtime in the considered operating room based on the sequence provided by a particular solution. It is important to note that even if the overtime is 0 in a particular instance, the quadratic Equation (6) cannot be eliminated as this provides information about the overtime’s value. The model will remain nonlinear even if the overtime value is 0 in a particular set of instances. Constraint (8) states that the operating room’s maximum allowable time limit must be followed. Constraints (9) and (10) define the binary domain of decision variables.
3. Solution Method
This section explains the solution method adopted to solve the developed mixed integer nonlinear problem. The proposed outer approximation method is based on the cutting plane method [83,84,85]. Consider the following MINLP problem:
The decision variables are represented by vectors a and b and , are two continuously differentiable functions. If we fix the vector of integer variables for any iteration, we get a sub-problem in the following form:
If this problem is feasible, it is solved to get an optimal solution, and if the problem is infeasible, infeasibility is minimized by solving the problem. We get gradients of functions and at , then a mixed integer problem that is equivalent to a mixed integer nonlinear problem (11)–(13) can be obtained:
where represents the number of trials for which the problem is solved. Problems (17)–(20) are the master problem. In this problem. Constraints (18)–(20) are used to outer approximate the objective function and constraints, respectively.
The sub-problem for the mixed integer nonlinear problem in this study is defined as:
subject to:
The hat indicates that the integer variables are fixed. The infeasibility can be minimized by solving the following problem:
The feasibility problem of the proposed model is formulated as:
The outer approximation master problem is defined as:
subject to:
where and represent the solution trials when the solution was feasible and infeasible, respectively. The accuracy of the algorithm is determined by . For example, if the sub-problem gives an optimal solution, the proposed OA method will obtain an -optimal solution. Further, it is unnecessary to get an optimal solution by solving the master problem; a feasible solution is sufficient. However, the number of iterations may increase if we get sub-optimal solutions. The proposed outer approximation method is explained in Figure 1 below. In Figure 1, and are the sets of iterations when the sub-problem (21)–(24) is feasible or infeasible respectively. Their values are initially represented as empty sets because both sets of iterations are empty at the start of the method. As the iterations of the proposed OA method proceed, the sets are populated with respective feasible or infeasible iterations, as given in step (2) of the pseudocode in Figure 1.
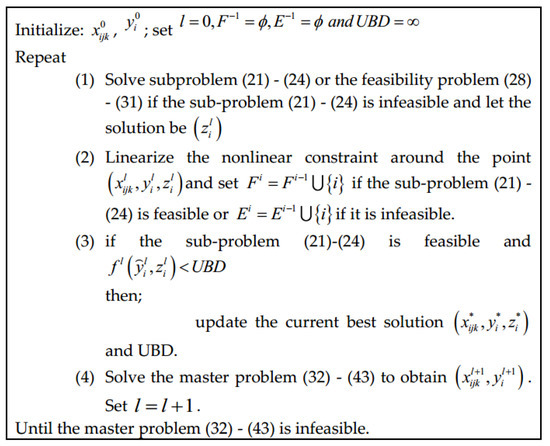
Figure 1.
Pseudocode for the procedure of the proposed OA method.
4. Computational Experiments and Results
In this section, several operating room problems are solved to investigate the performance of the proposed OA method and compare it with the standard model. Further, a case study from a hospital is solved, and the results are discussed. The experiments are performed using CPLEX and are run on a laptop with an Intel Core i3 processor of 2.00 GHz and 4.00 GB of RAM.
The data used for comparison of the performance of the proposed OA method is generated randomly. For the arrival of elective surgery patients, it is assumed that the elective patients follow a discrete uniform distribution derived from historical data. Patients’ length of stay in an operating room is generated using lognormal distribution [9,86]. Sequence dependent setup times are generated randomly for different specialties. For the case study, data from a case hospital are collected and the case study is solved for a period of two weeks.
Various instances of different sizes are solved to compare the performance of the proposed method. For each instance, CPU time, objective function values, and data sample specifications are recorded and presented in Table 2.
Table 2.
CPU time and objective function values along with data samples specifications.
In Table 2, ORs represents the number of open operating rooms. Objective function values and CPU time for both the standard model and the proposed OA method are compared. It can be observed that the OA model provides better results with lesser CPU time as compared to the standard model. The OA model gives the value of the objective function with a minimum optimality gap of 2%. The optimality gap used in the current study is calculated using (44):
where, is the minimum value of the objective function and is obtained through the standard model, and is the value of the objective function obtained using the OA method at each iteration. It is observed that OA obtained better results in a shorter time. This indicates the efficiency of the OA method.
Further, a comparison of the optimality gap with the percentage reduction in CPU time is drawn in Figure 2. It can be seen from Figure 2 that for all of the considered problem instances, the proposed method provided near-optimal results with lesser optimality gaps and a significant reduction in the computational time. For example, for problem 1, the optimality gap with the proposed OA method is 7%, and the percentage reduction in CPU time is 78%. Similarly, for problem 9, the optimality gap is 5%, with a 74% reduction in computational time.
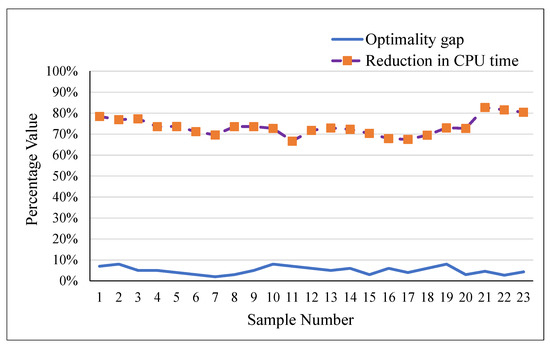
Figure 2.
Plot of Optimality Gap and Reduction in CPU Time.
Equation (45) represents the formula for calculating the percentage reduction in CPU time, where is the CPU time using the standard model and is the CPU time for the proposed OA method. It is observed from Figure 2 that the OA method provides better results in lesser CPU time.
Hence, it can be concluded that the proposed OA method provides good quality near-optimal results in shorter CPU times as compared to the exact method.
The convergence graph of the proposed method is presented in Figure 3 for 23 test problems. It is observed that OA converges after two iterations in the majority of instances. Equation (46) represents the formula used to find the percentage convergence value in the current study:
where, is the minimum value of the objective function out of all the iterations of the OA method, and is the value of the objective function obtained using the OA method at each iteration.
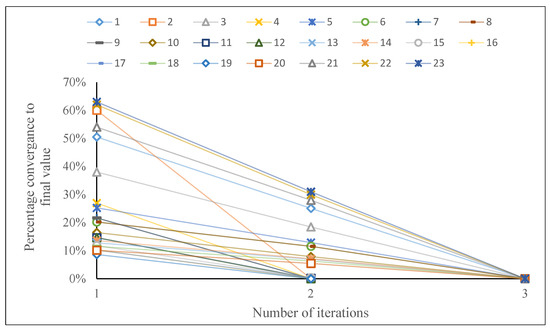
Figure 3.
Performance of OA method based on number of iterations.
Case Study
To further investigate the performance of the proposed OA method, surgery data from a case hospital is collected and a case study is solved for a period of two weeks. The results of the case study are summarized in Table 3. The hospital under study has eight operating rooms with two operating rooms reserved for emergency patients. There are patients of six different specialties and the aim is to minimize the operating room costs of both regular and overtime costs.
Table 3.
Summary of case study results.
Regular time costs can be minimized by deciding how many operating rooms to leave open for a given day. Similarly, overtime costs can be reduced by minimizing the average overtime in operating rooms. The results in Table 3 show that the proposed method results in less overtime values with the average overutilization of operating rooms up to 6%.
5. Conclusions and Suggestions for Future Research
In this paper, a method based on outer approximation is proposed to solve patient scheduling problems considering sequence dependent setup times in multiple heterogeneous operating rooms. Initially, a mixed integer nonlinear model is developed and solved using CPLEX solver. Moreover, an efficient outer approximation method is proposed to solve the problem near-optimally. The results obtained using the OA method are compared with the standard model. The performance metrics considered are the quality of the solution and the efficiency of the method. The computational results indicate the efficiency of the proposed OA method. Specifically, the proposed method outperforms the original MINLP model in terms of CPU time. It obtains near optimal results in comparatively less CPU time. This study extends the current operating room planning and scheduling literature in that it proposes a method to efficiently solve nonlinear problems. However, the current study has some limitations. In the current study, only the operating rooms are considered; it can be further extended to include upstream and downstream wards as well as other personnel, such as anesthesiologists, and material resources along with the scheduling of operating rooms.
Moreover, as the proposed OA method relies on the feasibility of the obtained solution and infeasible solutions can increase the number of iterations. The feasibility of the obtained solution is greatly affected by the value of the Boolean variables provided for each iteration. Thus, a good quality initial set of Boolean decision variables can result in better solutions with lesser number of iterations. Hence, it is proposed that this method may be used as a hybrid with some efficient heuristics to find good quality feasible solutions to avoid the unnecessary greater number of iterations that can further reduce the computational time.
Author Contributions
Conceptualization, A.T., S.U. and M.F.B.; methodology, A.T.; Coding, M.F.B.; analysis and data curation, S.U.; original draft preparation, A.T.; review and editing, S.U.; Supervision, M.F.B.; Funding acquisition, S.U. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Research Program of Universities (NRPU), Higher Education Commission of Pakistan, under Project 20-17024. The third author was supported by a discovery grant from the Natural Sciences and Engineering Research Council grant of Canada.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
Authors are thankful to the Department of Industrial Engineering University of Engineering and Technology Taxila, Pakistan, Higher Education Commission of Pakistan and Odette School of Business, University of Windsor, Canada.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhao, Z.; Li, X. Scheduling elective surgeries with sequence-dependent setup times to multiple operating rooms using constraint programming. Oper. Res. Health Care 2014, 3, 160–167. [Google Scholar] [CrossRef]
- Denton, B.T.; Miller, A.J.; Balasubramanian, H.J.; Huschka, T.R. Optimal allocation of surgery blocks to operating rooms under uncertainty. Oper. Res. 2010, 58, 802–816. [Google Scholar] [CrossRef]
- Moosavi, A.; Ebrahimnejad, S. Scheduling of elective patients considering upstream and downstream units and emergency demand using robust optimization. Comput. Ind. Eng. 2018, 120, 216–233. [Google Scholar] [CrossRef]
- Moosavi, A.; Ebrahimnejad, S. Robust operating room planning considering upstream and downstream units: A new two-stage heuristic algorithm. Comput. Ind. Eng. 2020, 143, 106387. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Tang, J. A distributionally robust optimization approach for surgery block allocation. Eur. J. Oper. Res. 2019, 273, 740–753. [Google Scholar] [CrossRef]
- Bargetto, R.; Garaix, T.; Xie, X. A branch-and-price-and-cut algorithm for operating room scheduling under human resource constraints. Comput. Oper. Res. 2023, 152, 106136. [Google Scholar] [CrossRef]
- De Simone, B.; Agnoletti, V.; Rosato, C.; Kaafarani, H.; Stahel, P.F.; Collaborative, O.; Catena, R.; Catena, F. The “Operating Room Surgical Activity”(ORSA) study: A snap-shot international survey on the global management of the operating theatres for emergency surgery. When to persist is diabolical…. Res. Sq. 2023; preprint. [Google Scholar]
- Cardoen, B.; Demeulemeester, E.; Beliën, J. Operating room planning and scheduling: A literature review. Eur. J. Oper. Res. 2010, 201, 921–932. [Google Scholar] [CrossRef]
- Jebali, A.; Diabat, A. A stochastic model for operating room planning under capacity constraints. Int. J. Prod. Res. 2015, 53, 7252–7270. [Google Scholar] [CrossRef]
- Hof, S.; Fügener, A.; Schoenfelder, J.; Brunner, J.O. Case mix planning in hospitals: A review and future agenda. Health Care Manag. Sci. 2017, 20, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Guerriero, F.; Guido, R. Operational research in the management of the operating theatre: A survey. Health Care Manag. Sci. 2011, 14, 89–114. [Google Scholar] [CrossRef] [PubMed]
- Batun, S.; Denton, B.T.; Huschka, T.R.; Schaefer, A.J. Operating room pooling and parallel surgery processing under uncertainty. INFORMS J. Comput. 2011, 23, 220–237. [Google Scholar] [CrossRef]
- Hashemi Doulabi, S.H.; Rousseau, L.-M.; Pesant, G. A constraint-programming-based branch-and-price-and-cut approach for operating room planning and scheduling. INFORMS J. Comput. 2016, 28, 432–448. [Google Scholar] [CrossRef]
- Fei, H.; Chu, C.; Meskens, N. Solving a tactical operating room planning problem by a column-generation-based heuristic procedure with four criteria. Ann. Oper. Res. 2009, 166, 91. [Google Scholar] [CrossRef]
- Marques, I.; Captivo, M.E.; Pato, M.V. An integer programming approach to elective surgery scheduling. OR Spectr. 2012, 34, 407–427. [Google Scholar] [CrossRef]
- Marques, I.; Captivo, M.E.; Pato, M.V. Scheduling elective surgeries in a Portuguese hospital using a genetic heuristic. Oper. Res. Health Care 2014, 3, 59–72. [Google Scholar] [CrossRef]
- Fei, H.; Meskens, N.; Chu, C. A planning and scheduling problem for an operating theatre using an open scheduling strategy. Comput. Ind. Eng. 2010, 58, 221–230. [Google Scholar] [CrossRef]
- Denton, B.; Viapiano, J.; Vogl, A. Optimization of surgery sequencing and scheduling decisions under uncertainty. Health Care Manag. Sci. 2007, 10, 13–24. [Google Scholar] [CrossRef]
- Pham, D.-N.; Klinkert, A. Surgical case scheduling as a generalized job shop scheduling problem. Eur. J. Oper. Res. 2008, 185, 1011–1025. [Google Scholar] [CrossRef]
- Oliveira, M.; Bélanger, V.; Marques, I.; Ruiz, A. Assessing the impact of patient prioritization on operating room schedules. Oper. Res. Health Care 2020, 24, 100232. [Google Scholar] [CrossRef]
- Younespour, M.; Atighehchian, A.; Kianfar, K.; Esfahani, E.T. Using mixed integer programming and constraint programming for operating rooms scheduling with modified block strategy. Oper. Res. Health Care 2019, 23, 100220. [Google Scholar] [CrossRef]
- Addis, B.; Carello, G.; Grosso, A.; Tànfani, E. Operating room scheduling and rescheduling: A rolling horizon approach. Flex. Serv. Manuf. J. 2016, 28, 206–232. [Google Scholar] [CrossRef]
- Landa, P.; Aringhieri, R.; Soriano, P.; Tànfani, E.; Testi, A. A hybrid optimization algorithm for surgeries scheduling. Oper. Res. Health Care 2016, 8, 103–114. [Google Scholar] [CrossRef]
- Neyshabouri, S.; Berg, B.P. Two-stage robust optimization approach to elective surgery and downstream capacity planning. Eur. J. Oper. Res. 2017, 260, 21–40. [Google Scholar] [CrossRef]
- Rachuba, S.; Werners, B. A fuzzy multi-criteria approach for robust operating room schedules. Ann. Oper. Res. 2017, 251, 325–350. [Google Scholar] [CrossRef]
- Bam, M.; Denton, B.T.; Van Oyen, M.P.; Cowen, M.E. Surgery scheduling with recovery resources. IISE Trans. 2017, 49, 942–955. [Google Scholar] [CrossRef]
- Kroer, L.R.; Foverskov, K.; Vilhelmsen, C.; Hansen, A.S.; Larsen, J. Planning and scheduling operating rooms for elective and emergency surgeries with uncertain duration. Oper. Res. Health Care 2018, 19, 107–119. [Google Scholar] [CrossRef]
- Marques, I.; Captivo, M.E.; Barros, N. Optimizing the master surgery schedule in a private hospital. Oper. Res. Health Care 2019, 20, 11–24. [Google Scholar] [CrossRef]
- Jebali, A.; Alouane, A.B.H.; Ladet, P. Operating rooms scheduling. Int. J. Prod. Econ. 2006, 99, 52–62. [Google Scholar] [CrossRef]
- Tayyab, A.; Ullah, S.; Mahmood, T.; Ghadi, Y.Y.; Latif, B.; Aljuaid, H. Modeling of Multi-Level Planning of Shifting Bottleneck Resources Integrated with Downstream Wards in a Hospital. Appl. Sci. 2023, 13, 3616. [Google Scholar] [CrossRef]
- Tayyab, A.; Saif, U. A Two-Stage Genetic Artificial Bee Colony Algorithm for Solving Integrated Operating Room Planning and Scheduling Problem With Capacity Constraints of Downstream Wards. IEEE Access 2022, 10, 131109–131127. [Google Scholar] [CrossRef]
- Kuo, P.C.; Schroeder, R.A.; Mahaffey, S.; Bollinger, R.R. Optimization of operating room allocation using linear programming techniques. J. Am. Coll. Surg. 2003, 197, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Mulholland, M.W.; Abrahamse, P.; Bahl, V. Linear programming to optimize performance in a department of surgery. J. Am. Coll. Surg. 2005, 200, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Dexter, F.; Blake, J.T.; Penning, D.H.; Lubarsky, D.A. Calculating a potential increase in hospital margin for elective surgery by changing operating room time allocations or increasing nursing staffing to permit completion of more cases: A case study. Anesth. Analg. 2002, 94, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Dexter, F.; Blake, J.T.; Penning, D.H.; Sloan, B.; Chung, P.; Lubarsky, D.A. Use of linear programming to estimate impact of changes in a hospital's operating room time allocation on perioperative variable costs. J. Am. Soc. Anesthesiol. 2002, 96, 718–724. [Google Scholar] [CrossRef]
- Cappanera, P.; Visintin, F.; Banditori, C. Addressing conflicting stakeholders’ priorities in surgical scheduling by goal programming. Flex. Serv. Manuf. J. 2018, 30, 252–271. [Google Scholar] [CrossRef]
- Blake, J.T.; Carter, M.W. A goal programming approach to strategic resource allocation in acute care hospitals. Eur. J. Oper. Res. 2002, 140, 541–561. [Google Scholar] [CrossRef]
- Adan, I.; Bekkers, J.; Dellaert, N.; Jeunet, J.; Vissers, J. Improving operational effectiveness of tactical master plans for emergency and elective patients under stochastic demand and capacitated resources. Eur. J. Oper. Res. 2011, 213, 290–308. [Google Scholar] [CrossRef]
- Testi, A.; Tànfani, E. Tactical and operational decisions for operating room planning: Efficiency and welfare implications. Health Care Manag. Sci. 2009, 12, 363–373. [Google Scholar] [CrossRef]
- Tànfani, E.; Testi, A. A pre-assignment heuristic algorithm for the Master Surgical Schedule Problem (MSSP). Ann. Oper. Res. 2010, 178, 105–119. [Google Scholar] [CrossRef]
- Ballestín, F.; Pérez, Á.; Quintanilla, S. Scheduling and rescheduling elective patients in operating rooms to minimise the percentage of tardy patients. J. Sched. 2019, 22, 107–118. [Google Scholar] [CrossRef]
- Vissers, J.M.; Adan, I.J.; Bekkers, J.A. Patient mix optimization in tactical cardiothoracic surgery planning: A case study. IMA J. Manag. Math. 2005, 16, 281–304. [Google Scholar] [CrossRef]
- Van Huele, C.; Vanhoucke, M. Operating theatre modelling: Integrating social measures. J. Simul. 2015, 9, 121–128. [Google Scholar] [CrossRef]
- Aringhieri, R.; Landa, P.; Soriano, P.; Tanfani, E.; Testi, A. A two level metaheuristic for the operating room scheduling and assignment problem. Comput. Oper. Res. 2015, 54, 21–34. [Google Scholar] [CrossRef]
- Beliën, J.; Demeulemeester, E. Building cyclic master surgery schedules with leveled resulting bed occupancy. Eur. J. Oper. Res. 2007, 176, 1185–1204. [Google Scholar] [CrossRef]
- Beliën, J.; Demeulemeester, E.; Cardoen, B. A decision support system for cyclic master surgery scheduling with multiple objectives. J. Sched. 2009, 12, 147–161. [Google Scholar] [CrossRef]
- Cappanera, P.; Visintin, F.; Banditori, C. Comparing resource balancing criteria in master surgical scheduling: A combined optimisation-simulation approach. Int. J. Prod. Econ. 2014, 158, 179–196. [Google Scholar] [CrossRef]
- Heider, S.; Schoenfelder, J.; McRae, S.; Koperna, T.; Brunner, J.O. Tactical scheduling of surgeries to level bed utilization in the intensive care unit. IISE Trans. Healthc. Syst. Eng. 2020, 10, 229–242. [Google Scholar] [CrossRef]
- Heydari, M.; Soudi, A. Predictive/reactive planning and scheduling of a surgical suite with emergency patient arrival. J. Med. Syst. 2016, 40, 30. [Google Scholar] [CrossRef]
- Akbarzadeh, B.; Moslehi, G.; Reisi-Nafchi, M.; Maenhout, B. The re-planning and scheduling of surgical cases in the operating room department after block release time with resource rescheduling. Eur. J. Oper. Res. 2019, 278, 596–614. [Google Scholar] [CrossRef]
- Kamran, M.A.; Karimi, B.; Dellaert, N. A column-generation-heuristic-based benders’ decomposition for solving adaptive allocation scheduling of patients in operating rooms. Comput. Ind. Eng. 2020, 148, 106698. [Google Scholar] [CrossRef]
- Wang, Y.; Tang, J.; Fung, R.Y. A column-generation-based heuristic algorithm for solving operating theater planning problem under stochastic demand and surgery cancellation risk. Int. J. Prod. Econ. 2014, 158, 28–36. [Google Scholar] [CrossRef]
- Zhang, J.; Dridi, M.; El Moudni, A. Column-generation-based heuristic approaches to stochastic surgery scheduling with downstream capacity constraints. Int. J. Prod. Econ. 2020, 229, 107764. [Google Scholar] [CrossRef]
- Beliën, J.; Demeulemeester, E. A branch-and-price approach for integrating nurse and surgery scheduling. Eur. J. Oper. Res. 2008, 189, 652–668. [Google Scholar] [CrossRef]
- Cardoen, B.; Demeulemeester, E.; Beliën, J. Sequencing surgical cases in a day-care environment: An exact branch-and-price approach. Comput. Oper. Res. 2009, 36, 2660–2669. [Google Scholar] [CrossRef]
- Luo, L.; Luo, Y.; Qin, C. Admission control policies for surgery patients. J. Med. Syst. 2017, 41, 131. [Google Scholar] [CrossRef]
- Barz, C.; Rajaram, K. Elective patient admission and scheduling under multiple resource constraints. Prod. Oper. Manag. 2015, 24, 1907–1930. [Google Scholar] [CrossRef]
- Zhang, J.; Dridi, M.; El Moudni, A. A two-level optimization model for elective surgery scheduling with downstream capacity constraints. Eur. J. Oper. Res. 2019, 276, 602–613. [Google Scholar] [CrossRef]
- Cardoen, B.; Demeulemeester, E.; Beliën, J. Optimizing a multiple objective surgical case sequencing problem. Int. J. Prod. Econ. 2009, 119, 354–366. [Google Scholar] [CrossRef]
- Berg, B.P.; Denton, B.T. Fast approximation methods for online scheduling of outpatient procedure centers. INFORMS J. Comput. 2017, 29, 631–644. [Google Scholar] [CrossRef]
- Stuart, K.; Kozan, E. Reactive scheduling model for the operating theatre. Flex. Serv. Manuf. J. 2012, 24, 400–421. [Google Scholar] [CrossRef]
- Fügener, A.; Hans, E.W.; Kolisch, R.; Kortbeek, N.; Vanberkel, P.T. Master surgery scheduling with consideration of multiple downstream units. Eur. J. Oper. Res. 2014, 239, 227–236. [Google Scholar] [CrossRef]
- Nemati, S.; Shylo, O.V.; Prokopyev, O.A.; Schaefer, A.J. The surgical patient routing problem: A central planner approach. INFORMS J. Comput. 2016, 28, 657–673. [Google Scholar] [CrossRef]
- Ma, G.; Demeulemeester, E. A multilevel integrative approach to hospital case mix and capacity planning. Comput. Oper. Res. 2013, 40, 2198–2207. [Google Scholar] [CrossRef]
- Zhang, Z.; Denton, B.T.; Xie, X. Branch and price for chance-constrained bin packing. INFORMS J. Comput. 2020, 32, 547–564. [Google Scholar] [CrossRef]
- Zhang, Z.; Xie, X.; Geng, N. Dynamic surgery assignment of multiple operating rooms with planned surgeon arrival times. IEEE Trans. Autom. Sci. Eng. 2013, 11, 680–691. [Google Scholar] [CrossRef]
- Deng, Y.; Shen, S.; Denton, B. Chance-constrained surgery planning under conditions of limited and ambiguous data. INFORMS J. Comput. 2019, 31, 559–575. [Google Scholar] [CrossRef]
- Marques, I.; Captivo, M.E.; Pato, M.V. A bicriteria heuristic for an elective surgery scheduling problem. Health Care Manag. Sci. 2015, 18, 251–266. [Google Scholar] [CrossRef]
- Vali-Siar, M.M.; Gholami, S.; Ramezanian, R. Multi-period and multi-resource operating room scheduling under uncertainty: A case study. Comput. Ind. Eng. 2018, 126, 549–568. [Google Scholar] [CrossRef]
- Hans, E.; Wullink, G.; Van Houdenhoven, M.; Kazemier, G. Robust surgery loading. Eur. J. Oper. Res. 2008, 185, 1038–1050. [Google Scholar] [CrossRef]
- Ewen, H.; Mönch, L. A simulation-based framework to schedule surgeries in an eye hospital. IIE Trans. Healthc. Syst. Eng. 2014, 4, 191–208. [Google Scholar] [CrossRef]
- Spratt, B.; Kozan, E. Waiting list management through master surgical schedules: A case study. Oper. Res. Health Care 2016, 10, 49–64. [Google Scholar] [CrossRef]
- Molina-Pariente, J.M.; Hans, E.W.; Framinan, J.M.; Gomez-Cia, T. New heuristics for planning operating rooms. Comput. Ind. Eng. 2015, 90, 429–443. [Google Scholar] [CrossRef]
- Roshanaei, V.; Booth, K.E.; Aleman, D.M.; Urbach, D.R.; Beck, J.C. Branch-and-check methods for multi-level operating room planning and scheduling. Int. J. Prod. Econ. 2020, 220, 107433. [Google Scholar] [CrossRef]
- Hamid, M.; Hamid, M.; Musavi, M.; Azadeh, A. Scheduling elective patients based on sequence-dependent setup times in an open-heart surgical department using an optimization and simulation approach. Simulation 2019, 95, 1141–1164. [Google Scholar] [CrossRef]
- Van Essen, J.T.; Hans, E.W.; Hurink, J.L.; Oversberg, A. Minimizing the waiting time for emergency surgery. Oper. Res. Health Care 2012, 1, 34–44. [Google Scholar] [CrossRef]
- Schneider, A.T.; van Essen, J.T.; Carlier, M.; Hans, E.W. Scheduling surgery groups considering multiple downstream resources. Eur. J. Oper. Res. 2020, 282, 741–752. [Google Scholar] [CrossRef]
- Van den Broek d’Obrenan, A.; Ridder, A.; Roubos, D.; Stougie, L. Minimizing bed occupancy variance by scheduling patients under uncertainty. Eur. J. Oper. Res. 2020, 286, 336–349. [Google Scholar] [CrossRef]
- Vancroonenburg, W.; De Causmaecker, P.; Berghe, G.V. Chance-constrained admission scheduling of elective surgical patients in a dynamic, uncertain setting. Oper. Res. Health Care 2019, 22, 100196. [Google Scholar] [CrossRef]
- Nazif, H. Operating room surgery scheduling with fuzzy surgery durations using a metaheuristic approach. Adv. Oper. Res. 2018, 2018, 8637598. [Google Scholar] [CrossRef]
- Xiang, W.; Yin, J.; Lim, G. An ant colony optimization approach for solving an operating room surgery scheduling problem. Comput. Ind. Eng. 2015, 85, 335–345. [Google Scholar] [CrossRef]
- Saremi, A.; Jula, P.; ElMekkawy, T.; Wang, G.G. Appointment scheduling of outpatient surgical services in a multistage operating room department. Int. J. Prod. Econ. 2013, 141, 646–658. [Google Scholar] [CrossRef]
- Duran, M.A.; Grossmann, I.E. An outer-approximation algorithm for a class of mixed-integer nonlinear programs. Math. Program. 1986, 36, 307–339. [Google Scholar] [CrossRef]
- Fletcher, R.; Leyffer, S. Solving mixed integer nonlinear programs by outer approximation. Math. Program. 1994, 66, 327–349. [Google Scholar] [CrossRef]
- Grossmann, I.E.; Kravanja, Z. Mixed-integer nonlinear programming techniques for process systems engineering. Comput. Chem. Eng. 1995, 19, 189–204. [Google Scholar] [CrossRef]
- Freeman, N.; Zhao, M.; Melouk, S. An iterative approach for case mix planning under uncertainty. Omega 2018, 76, 160–173. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).