
Melanoma Classification from Dermoscopy Images Using Ensemble of Convolutional Neural Networks

 ,
,  ,
,  ,
, 
 and
and 
Abstract
1. Introduction
- A novel stacked ensemble framework based on transfer learning is presented to address the task of acral lentiginous melanoma classification;
- Extensive experiments have been performed on the benchmark dataset with and without data augmentation to show the impact of data augmentation in improving the accuracy of the proposed model;
- The proposed method outperforms state-of-the-art methods for acral lentiginous melanoma classification.
2. Background
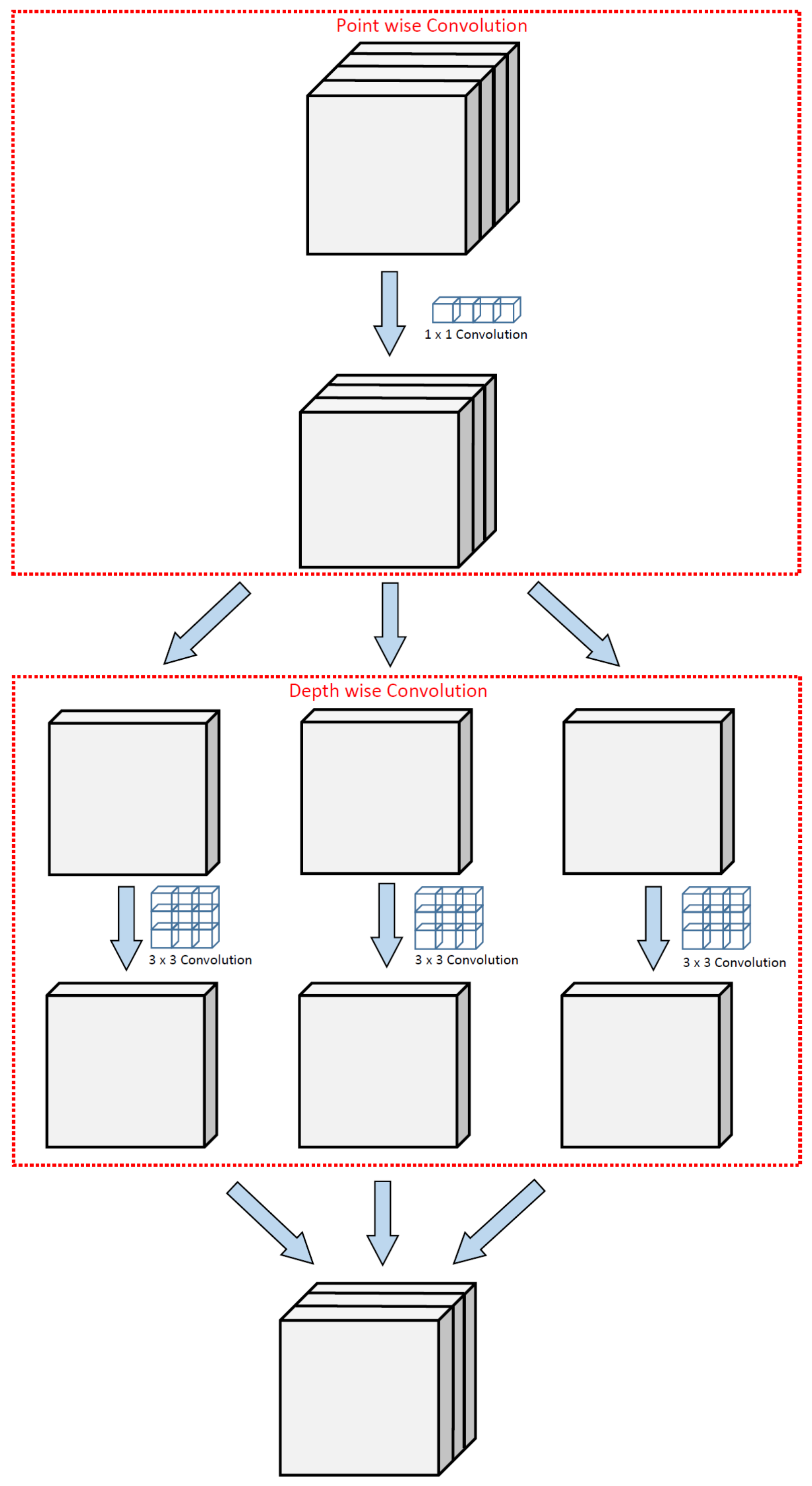
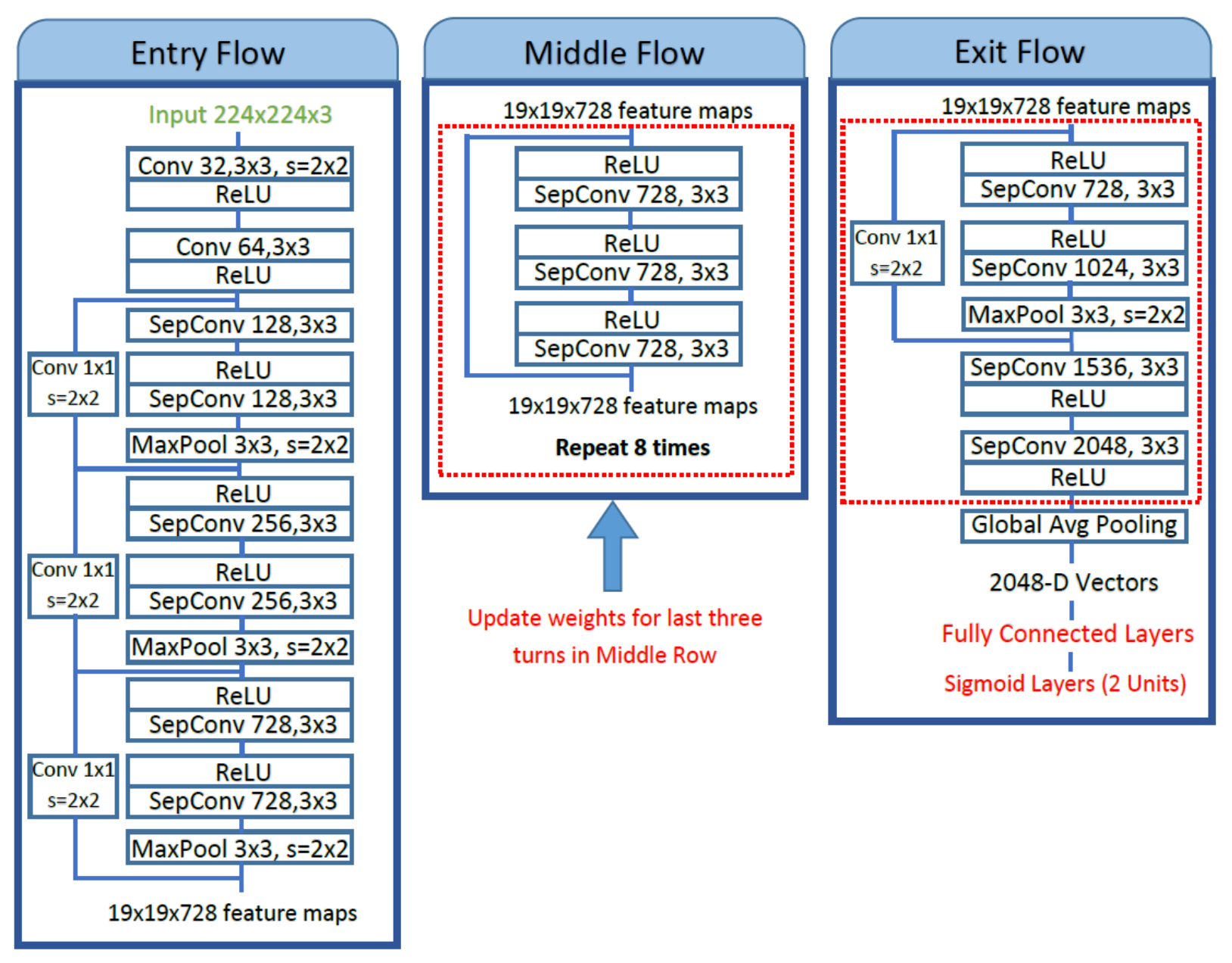
2.1. Pre-Trained Xception Model
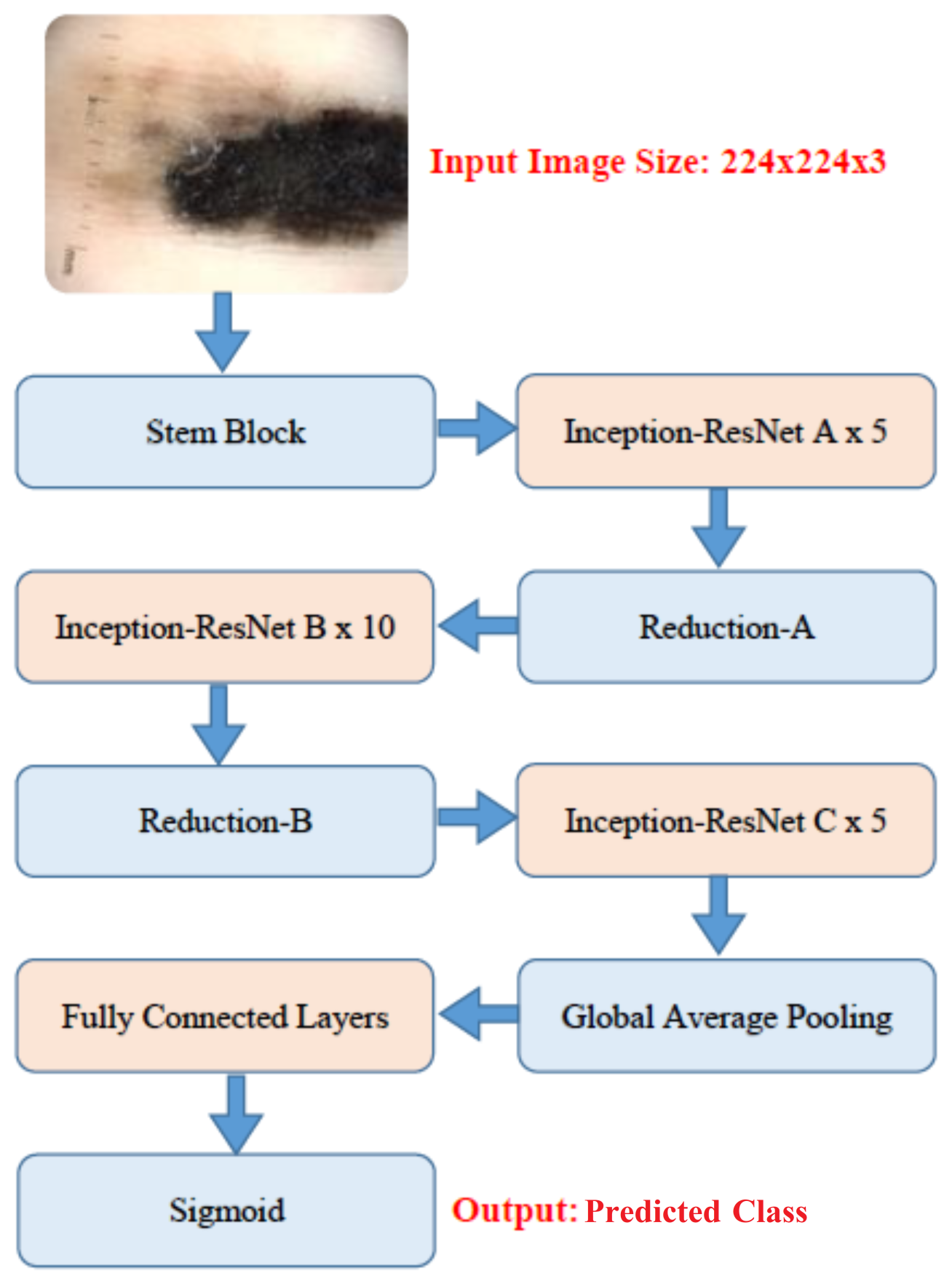
2.2. Pre-Trained InceptionResNet-v2 Model
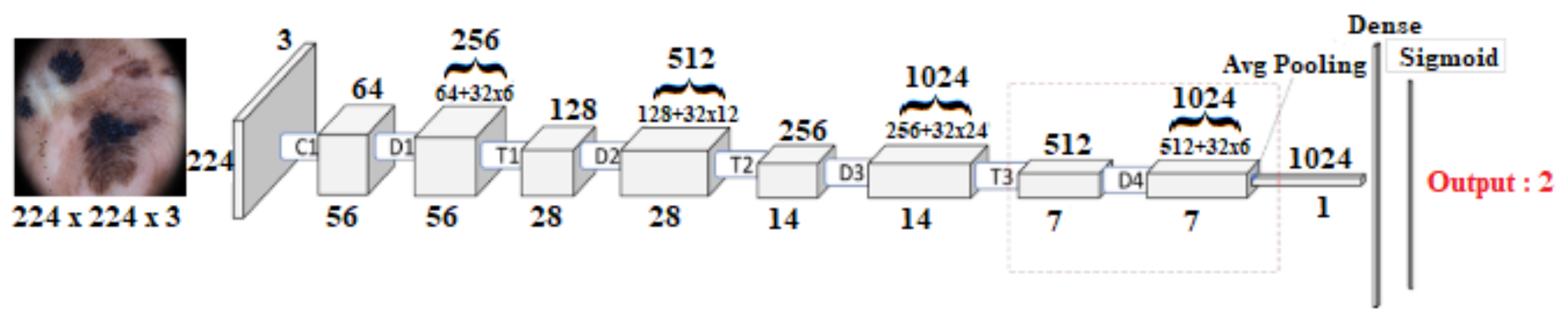
2.3. Pre-Trained DenseNet121 Model
2.4. Pre-Trained DenseNet201 Model
3. Related Work
3.1. Deep Learning-Based Techniques
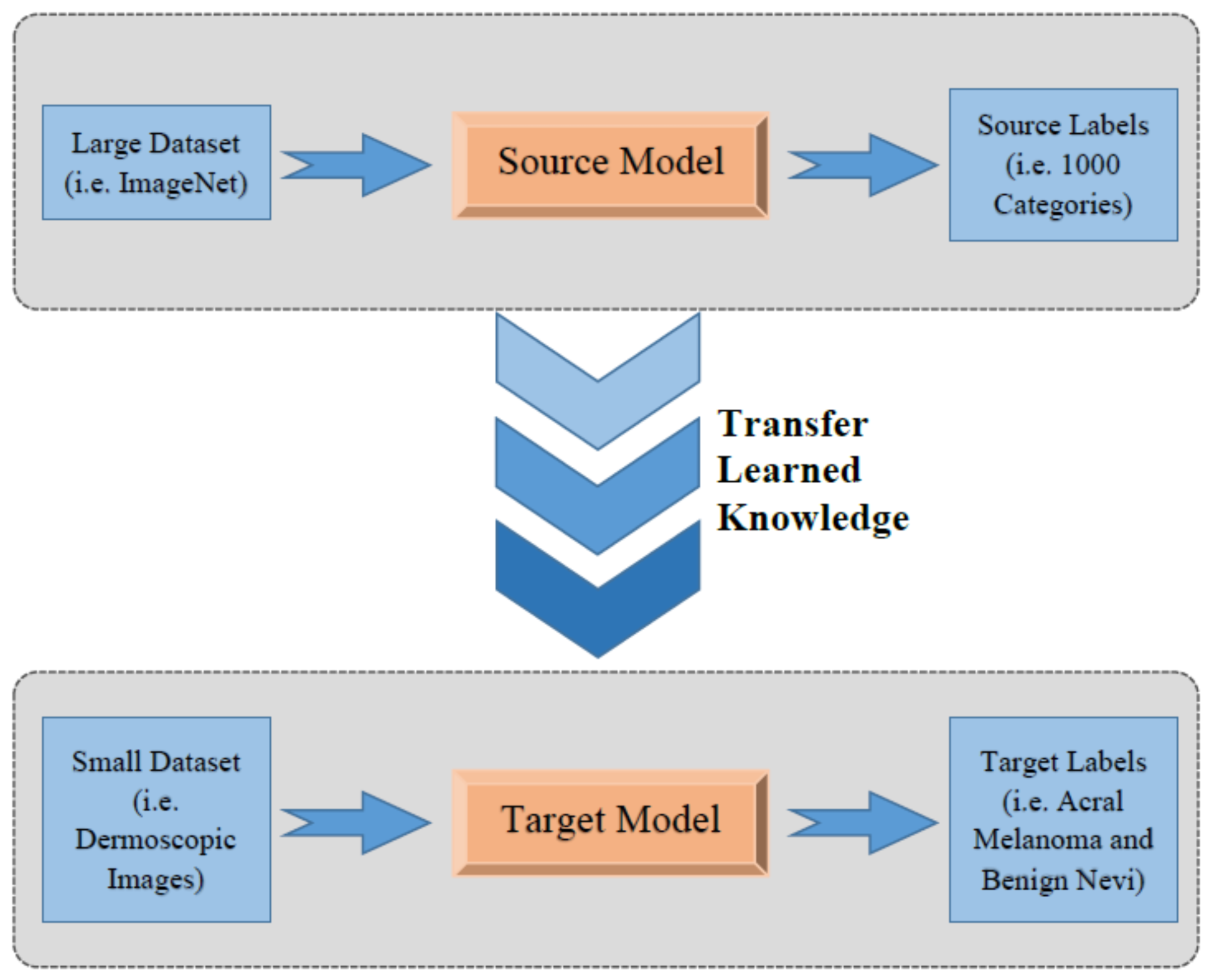
3.2. Transfer Learning-Based Techniques
3.3. Ensemble Learning-Based Techniques
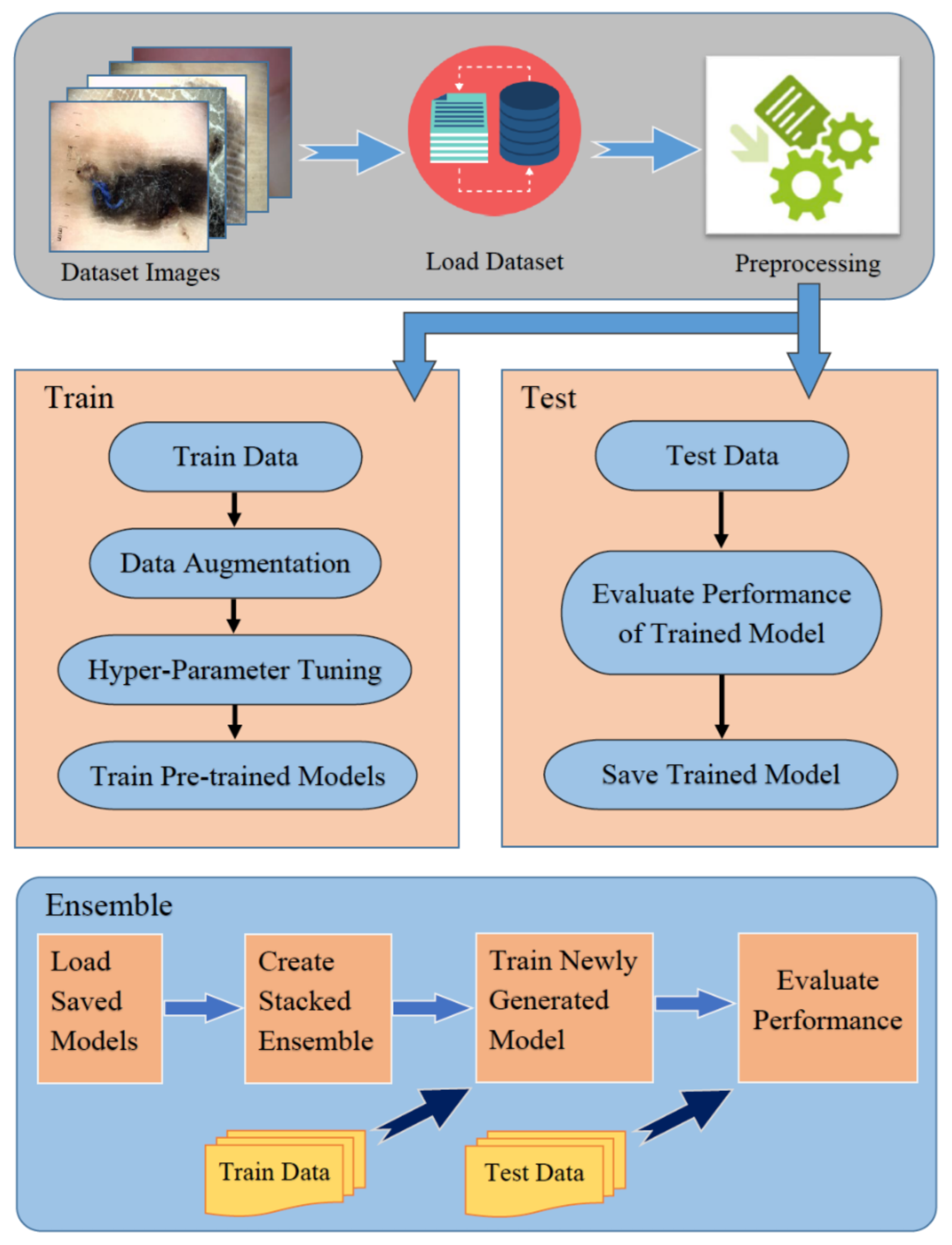
4. Methodology
4.1. Preprocessing
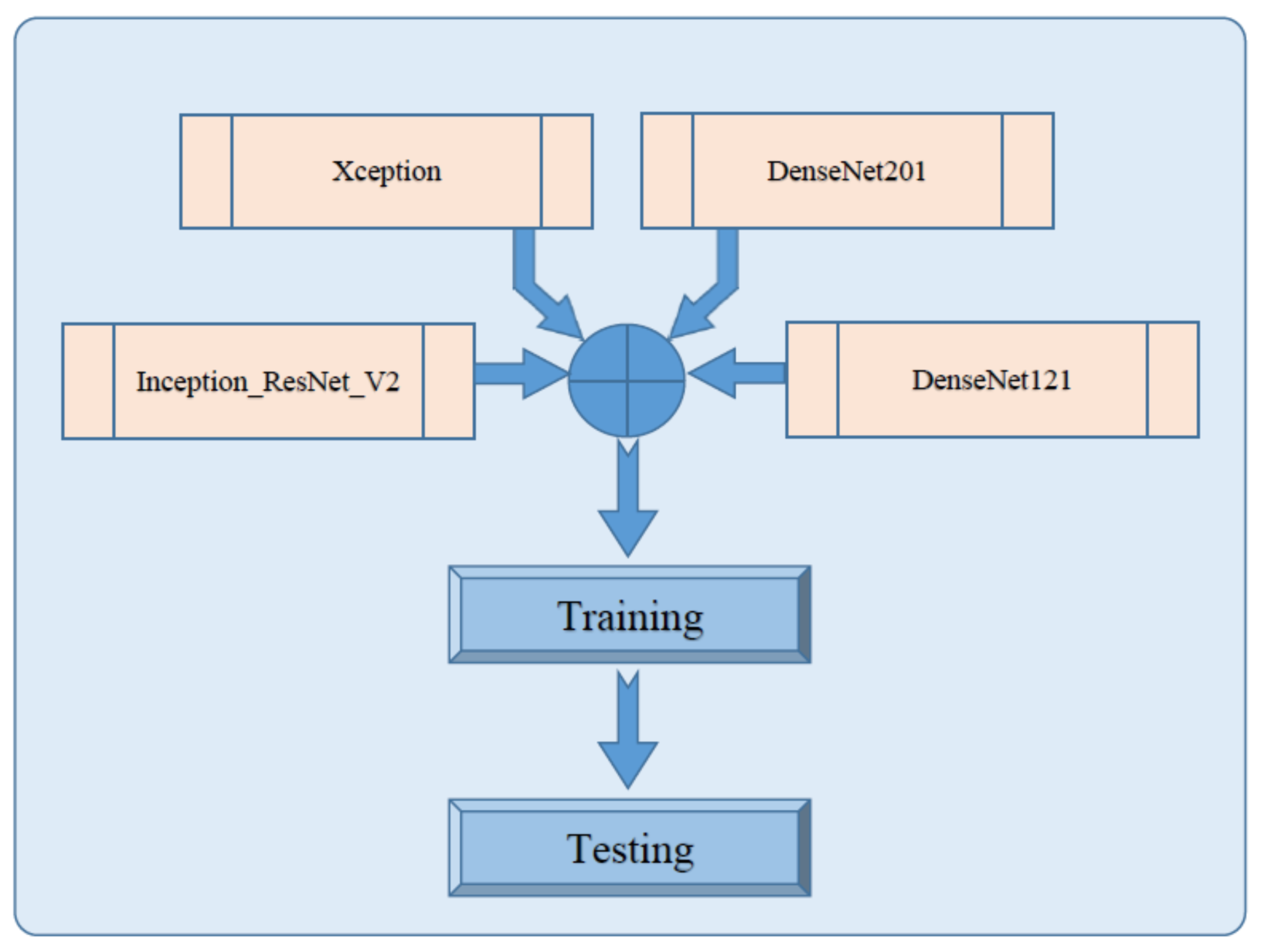
4.2. Stacked Ensemble of Fine-Tuned Pre-Trained CNN Architectures
5. Experimentations and Results
5.1. Experimental Setup
5.2. Comparison with State-of-the-Art Methods
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Codella, N.C.; Nguyen, Q.B.; Pankanti, S.; Gutman, D.A.; Helba, B.; Halpern, A.C.; Smith, J.R. Deep learning ensembles for melanoma recognition in dermoscopy images. IBM J. Res. Dev. 2017, 61, 5:1–5:15. [Google Scholar] [CrossRef]
- Alasadi, A.H.H.; Alsafy, B.M. Diagnosis of Malignant Melanoma of Skin Cancer Types. Int. J. Interact. Multimed. Artif. Intell. 2017, 4, 44–49. [Google Scholar] [CrossRef][Green Version]
- Darmawan, C.C.; Jo, G.; Montenegro, S.E.; Kwak, Y.; Cheol, L.; Cho, K.H.; Mun, J.H. Early detection of acral melanoma: A review of clinical, dermoscopic, histopathologic, and molecular characteristics. J. Am. Acad. Dermatol. 2019, 81, 805–812. [Google Scholar] [CrossRef]
- Vocaturo, E.; Perna, D.; Zumpano, E. Machine learning techniques for automated melanoma detection. In Proceedings of the 2019 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), San Diego, CA, USA, 18–21 November 2019; pp. 2310–2317. [Google Scholar]
- Yu, C.; Yang, S.; Kim, W.; Jung, J.; Chung, K.Y.; Lee, S.W.; Oh, B. Acral melanoma detection using a convolutional neural network for dermoscopy images. PLoS ONE 2018, 13, e0193321. [Google Scholar]
- Nezhadian, F.K.; Rashidi, S. Melanoma skin cancer detection using color and new texture features. In Proceedings of the 2017 Artificial Intelligence and Signal Processing Conference (AISP), Shiraz, Iran, 25–27 October 2017; pp. 1–5. [Google Scholar]
- Shorten, C.; Khoshgoftaar, T.M. A survey on image data augmentation for deep learning. J. Big Data 2019, 6, 1–48. [Google Scholar] [CrossRef]
- Ganster, H.; Pinz, P.; Rohrer, R.; Wildling, E.; Binder, M.; Kittler, H. Automated melanoma recognition. IEEE Trans. Med. Imaging 2001, 20, 233–239. [Google Scholar] [CrossRef]
- Rezaoana, N.; Hossain, M.S.; Andersson, K. Detection and Classification of Skin Cancer by Using a Parallel CNN Model. In Proceedings of the 2020 IEEE International Women in Engineering (WIE) Conference on Electrical and Computer Engineering (WIECON-ECE), Bhubaneswar, India, 26–27 December 2020; pp. 380–386. [Google Scholar]
- Hosny, K.M.; Kassem, M.A.; Foaud, M.M. Classification of skin lesions using transfer learning and augmentation with Alex-net. PLoS ONE 2019, 14, e0217293. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Chu, Y.; Yoo, S.; Choi, S.; Choe, S.; Koh, S.; Chung, K.; Xing, L.; Oh, B.; Yang, S. Augmented decision-making for acral lentiginous melanoma detection using deep convolutional neural networks. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1842–1850. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Chollet, F. Deep learning with separable convolutions. arXiv 2016, arXiv:1610.02357. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Haggenmüller, S.; Maron, R.C.; Hekler, A.; Utikal, J.S.; Barata, C.; Barnhill, R.L.; Beltraminelli, H.; Berking, C.; Betz-Stablein, B.; Blum, A.; et al. Skin cancer classification via convolutional neural networks: Systematic review of studies involving human experts. Eur. J. Cancer 2021, 156, 202–216. [Google Scholar] [CrossRef]
- Razmjooy, N.; Ashourian, M.; Karimifard, M.; Estrela, V.V.; Loschi, H.J.; Do Nascimento, D.; França, R.P.; Vishnevski, M. Computer-aided diagnosis of skin cancer: A review. Curr. Med. Imaging 2020, 16, 781–793. [Google Scholar] [CrossRef]
- Höhn, J.; Hekler, A.; Krieghoff-Henning, E.; Kather, J.N.; Utikal, J.S.; Meier, F.; Gellrich, F.F.; Hauschild, A.; French, L.; Schlager, J.G.; et al. Integrating patient data into skin cancer classification using convolutional neural networks: Systematic review. J. Med. Internet Res. 2021, 23, e20708. [Google Scholar] [CrossRef] [PubMed]
- Saeed, J.; Zeebaree, S. Skin lesion classification based on deep convolutional neural networks architectures. J. Appl. Sci. Technol. Trends 2021, 2, 41–51. [Google Scholar] [CrossRef]
- Kassani, S.H.; Kassani, P.H. A comparative study of deep learning architectures on melanoma detection. Tissue Cell 2019, 58, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Li, Y.; Shen, L. Skin lesion analysis towards melanoma detection using deep learning network. Sensors 2018, 18, 556. [Google Scholar] [CrossRef]
- Barata, C.; Marques, J.S. Deep learning for skin cancer diagnosis with hierarchical architectures. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 841–845. [Google Scholar]
- Adegun, A.A.; Viriri, S. Deep learning-based system for automatic melanoma detection. IEEE Access 2019, 8, 7160–7172. [Google Scholar] [CrossRef]
- Demir, A.; Yilmaz, F.; Kose, O. Early detection of skin cancer using deep learning architectures: Resnet-101 and inception-v3. In Proceedings of the 2019 Medical Technologies Congress (TIPTEKNO), Izmir, Turkey, 3–5 October 2019; pp. 1–4. [Google Scholar]
- Daghrir, J.; Tlig, L.; Bouchouicha, M.; Sayadi, M. Melanoma skin cancer detection using deep learning and classical machine learning techniques: A hybrid approach. In Proceedings of the 2020 5th International Conference on Advanced Technologies for Signal and Image Processing (ATSIP), Sousse, Tunisia, 2–5 September 2020; pp. 1–5. [Google Scholar]
- Mahbod, A.; Schaefer, G.; Wang, C.; Ecker, R.; Ellinger, I. Skin Lesion Classification Using Hybrid Deep Neural Networks. In Proceedings of the ICASSP 2019—2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; pp. 1229–1233. [Google Scholar] [CrossRef]
- Aburaed, N.; Panthakkan, A.; Al-Saad, M.; Amin, S.A.; Mansoor, W. Deep Convolutional Neural Network (DCNN) for Skin Cancer Classification. In Proceedings of the 2020 27th IEEE International Conference on Electronics, Circuits and Systems (ICECS), Glasgow, UK, 23–25 November 2020; pp. 1–4. [Google Scholar]
- Tschandl, P.; Rosendahl, C.; Kittler, H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci. Data 2018, 2018, 180161. [Google Scholar] [CrossRef]
- Sedigh, P.; Sadeghian, R.; Masouleh, M.T. Generating synthetic medical images by using GAN to improve CNN performance in skin cancer classification. In Proceedings of the 2019 7th International Conference on Robotics and Mechatronics (ICRoM), Tehran, Iran, 20–21 November 2019; pp. 497–502. [Google Scholar]
- Combalia, M.; Codella, N.C.; Rotemberg, V.; Helba, B.; Vilaplana, V.; Reiter, O.; Carrera, C.; Barreiro, A.; Halpern, A.C.; Puig, S.; et al. BCN20000: Dermoscopic lesions in the wild. arXiv 2019, arXiv:1908.02288. [Google Scholar]
- Gareau, D.S.; Browning, J.; Da Rosa, J.C.; Suarez-Farinas, M.; Lish, S.; Zong, A.M.; Firester, B.; Vrattos, C.; Renert-Yuval, Y.; Gamboa, M.; et al. Deep learning-level melanoma detection by interpretable machine learning and imaging biomarker cues. J. Biomed. Opt. 2020, 25, 112906. [Google Scholar] [CrossRef] [PubMed]
- Rehman, A.; Khan, M.A.; Mehmood, Z.; Saba, T.; Sardaraz, M.; Rashid, M. Microscopic melanoma detection and classification: A framework of pixel-based fusion and multilevel features reduction. Microsc. Res. Tech. 2020, 83, 410–423. [Google Scholar] [CrossRef]
- Parmar, B.; Talati, B. Automated Melanoma Types and Stages Classification for dermoscopy images. In Proceedings of the 2019 Innovations in Power and Advanced Computing Technologies (i-PACT), Vellore, India, 22–23 March 2019; Volume 1, pp. 1–7. [Google Scholar]
- Rahman, Z.; Ami, A.M. A Transfer Learning Based Approach for Skin Lesion Classification from Imbalanced Data. In Proceedings of the 2020 11th International Conference on Electrical and Computer Engineering (ICECE), Dhaka, Bangladesh, 17–19 December 2020; pp. 65–68. [Google Scholar]
- Zunair, H.; Hamza, A.B. Melanoma detection using adversarial training and deep transfer learning. Phys. Med. Biol. 2020, 65, 135005. [Google Scholar] [CrossRef] [PubMed]
- Al Nazi, Z.; Abir, T.A. Automatic skin lesion segmentation and melanoma detection: Transfer learning approach with u-net and dcnn-svm. In Proceedings of the International Joint Conference on Computational Intelligence; Springer: Singapore, 2020; pp. 371–381. [Google Scholar]
- Younis, H.; Bhatti, M.H.; Azeem, M. Classification of skin cancer dermoscopy images using transfer learning. In Proceedings of the 2019 15th International Conference on Emerging Technologies (ICET), Peshawar, Pakistan, 2–3 December 2019; pp. 1–4. [Google Scholar]
- Islam, M.K.; Ali, M.S.; Ali, M.M.; Haque, M.F.; Das, A.A.; Hossain, M.M.; Duranta, D.; Rahman, M.A. Melanoma Skin Lesions Classification using Deep Convolutional Neural Network with Transfer Learning. In Proceedings of the 2021 1st International Conference on Artificial Intelligence and Data Analytics (CAIDA), Riyadh, Saudi Arabia, 6–7 April 2021; pp. 48–53. [Google Scholar]
- Harangi, B.; Baran, A.; Hajdu, A. Classification of skin lesions using an ensemble of deep neural networks. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 2575–2578. [Google Scholar]
- Osowski, S.; Les, T. Deep Learning Ensemble for Melanoma Recognition. In Proceedings of the 2020 International Joint Conference on Neural Networks (IJCNN), Glasgow, UK, 19–24 July 2020; pp. 1–7. [Google Scholar]
- Milton, M.A.A. Automated skin lesion classification using ensemble of deep neural networks in ISIC 2018: Skin lesion analysis towards melanoma detection challenge. arXiv 2019, arXiv:1901.10802. [Google Scholar]
- Ashraf, R.; Kiran, I.; Mahmood, T.; Butt, A.U.R.; Razzaq, N.; Farooq, Z. An efficient technique for skin cancer classification using deep learning. In Proceedings of the 2020 IEEE 23rd International Multitopic Conference (INMIC), Bahawalpur, Pakistan, 5–7 November 2020; pp. 1–5. [Google Scholar]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Han, S.S.; Moon, I.J.; Lim, W.; Suh, I.S.; Lee, S.Y.; Na, J.I.; Kim, S.H.; Chang, S.E. Keratinocytic skin cancer detection on the face using region-based convolutional neural network. JAMA Dermatol. 2020, 156, 29–37. [Google Scholar] [CrossRef]
- Zhuang, J.; Yang, J.; Gu, L.; Dvornek, N. Shelfnet for fast semantic segmentation. In Proceedings of the IEEE/CVF International Conference on Computer Vision Workshops, Seoul, Korea, 27–28 October 2019. [Google Scholar]
- Mikolajczyk, A.; Grochowski, M. Data augmentation for improving deep learning in image classification problem. In 2018 International Interdisciplinary PhD Workshop (IIPhDW); IEEE: Piscatvey, NJ, USA, 2018; pp. 117–122. [Google Scholar]
- Lu, Y.; Zhang, L.; Wang, B.; Yang, J. Feature ensemble learning based on sparse autoencoders for image classification. In Proceedings of the 2014 International Joint Conference on Neural Networks (IJCNN), Beijing, China, 6–11 July 2014; pp. 1739–1745. [Google Scholar]
- Izmailov, P.; Podoprikhin, D.; Garipov, T.; Vetrov, D.; Wilson, A.G. Averaging weights leads to wider optima and better generalization. arXiv 2018, arXiv:1803.05407. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Acral Melanoma and Benign Data Set. Available online: https://figshare.com/s/a8c22c09f999f60a81bd (accessed on 15 March 2021).
- Ann, A.J.; Ruiz, C. Using deep learning for melanoma detection in dermoscopy images. Int. J. Mach. Learn. Comput. 2018, 8, 61–68. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hyper-Parameter | Parameter Value |
|---|---|
| Optimizer | Adam |
| Learning Rate | 0.0001 |
| Loss Function | binary crossentropy |
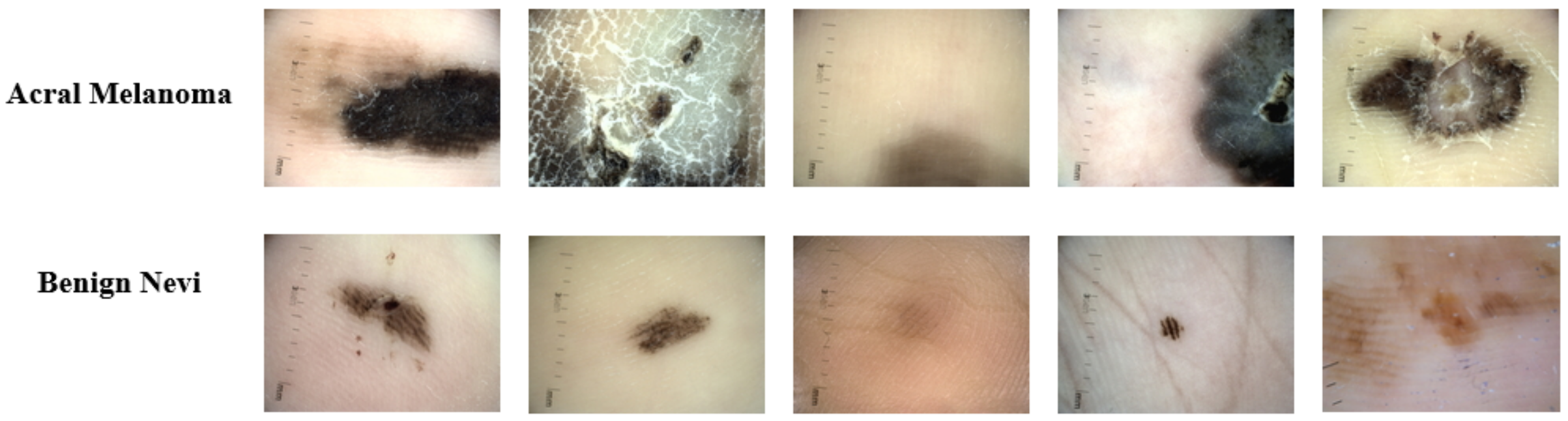
| Dermoscopy Images | Number of Instances |
|---|---|
| Acral Melanoma | 350 |
| Benign Nevi | 374 |
| Total | 724 |
| Pre-Trained Model | Validation Accuracy | Test Accuracy |
|---|---|---|
| VGG16 | 91.03% | 91.72% |
| InceptionV3 | 87.59% | 87.85% |
| Xception | 90.34% | 90.34% |
| InceptionResnetV2 | 91.72% | 91.72% |
| DenseNet121 | 91.72% | 91.72% |
| Pre-Trained Model | Validation Accuracy | Test Accuracy |
|---|---|---|
| VGG16 | 91.03% | 91.03% |
| InceptionV3 | 93.10% | 93.10% |
| Xception | 95.17% | 95.17% |
| InceptionResnetV2 | 95.17% | 95.17% |
| DenseNet121 | 94.48% | 94.48% |
| Class | Performance Metrics | Results |
|---|---|---|
| Acral Melanoma | Precision | 98% |
| Recall | 97% | |
| F1-score | 98% | |
| Sensitivity | 97% | |
| Specificity | 98% | |
| Accuracy | 96.77% | |
| Benign Nevi | Precision | 98% |
| Recall | 99% | |
| F1-score | 98% | |
| Sensitivity | 98.63% | |
| Specificity | 97% | |
| Accuracy | 98.79% |
| Models | No. of Epochs | Training Accuracy | Validation Accuracy | Test Accuracy |
|---|---|---|---|---|
| Xception | 25 | 100% | 95.17% | 95.17% |
| Inception-ResNet-V2 | 50 | 98.90% | 95.17% | 95.17% |
| DenseNet121 | 50 | 94.92% | 94.48% | 94.48% |
| DenseNet201 | 45 | 99.82% | 95.86% | 95.86% |
| Stacked Ensemble Model | 10 | 100% | 100% | 97.93% |
| Authors and Year | Method | Evaluation Metric | Results |
|---|---|---|---|
| C. Yu et al. [5] (2018) | Data Augmentation and Transfer Learning using Pre-trained VGG16 | Accuracy | 80.3% |
| Sensitivity | 92% | ||
| Specificity | 75% | ||
| S. Lee et al. [11] (2020) | Transfer Learning using Pre-trained ResNet50 | Accuracy | 83.51% |
| Sensitivity | N.A | ||
| Specificity | N.A | ||
| J. A. A [54] (2018) | Transfer Learning using Pre-trained AlexNet Without Hair Removal | Accuracy | 82.5% |
| Sensitivity | 74% | ||
| Specificity | 74% | ||
| J. A. A [54] (2018) | Transfer Learning using Pre-trained AlexNet With Hair Removal | Accuracy | 92.5% |
| Sensitivity | 90% | ||
| Specificity | 90% | ||
| Proposed Method | Stacking ensemble of fine-tuned models | Accuracy | 97.93% |
| Sensitivity | 97.83% | ||
| Specificity | 97.50% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raza, R.; Zulfiqar, F.; Tariq, S.; Anwar, G.B.; Sargano, A.B.; Habib, Z. Melanoma Classification from Dermoscopy Images Using Ensemble of Convolutional Neural Networks. Mathematics 2022, 10, 26. https://doi.org/10.3390/math10010026
Raza R, Zulfiqar F, Tariq S, Anwar GB, Sargano AB, Habib Z. Melanoma Classification from Dermoscopy Images Using Ensemble of Convolutional Neural Networks. Mathematics. 2022; 10(1):26. https://doi.org/10.3390/math10010026
Chicago/Turabian StyleRaza, Rehan, Fatima Zulfiqar, Shehroz Tariq, Gull Bano Anwar, Allah Bux Sargano, and Zulfiqar Habib. 2022. "Melanoma Classification from Dermoscopy Images Using Ensemble of Convolutional Neural Networks" Mathematics 10, no. 1: 26. https://doi.org/10.3390/math10010026
APA StyleRaza, R., Zulfiqar, F., Tariq, S., Anwar, G. B., Sargano, A. B., & Habib, Z. (2022). Melanoma Classification from Dermoscopy Images Using Ensemble of Convolutional Neural Networks. Mathematics, 10(1), 26. https://doi.org/10.3390/math10010026