Confident Parents for Easier Children: A Parental Self-Efficacy Program to Improve Young Children’s Behavior


Abstract
1. Introduction
1.1. Contributing Factors to Child EB
1.2. Parenting Programs to Improve Child Behavior
1.3. Factors Influencing Parenting Programs’ Effectiveness
1.4. Current Study
2. Materials and Methods
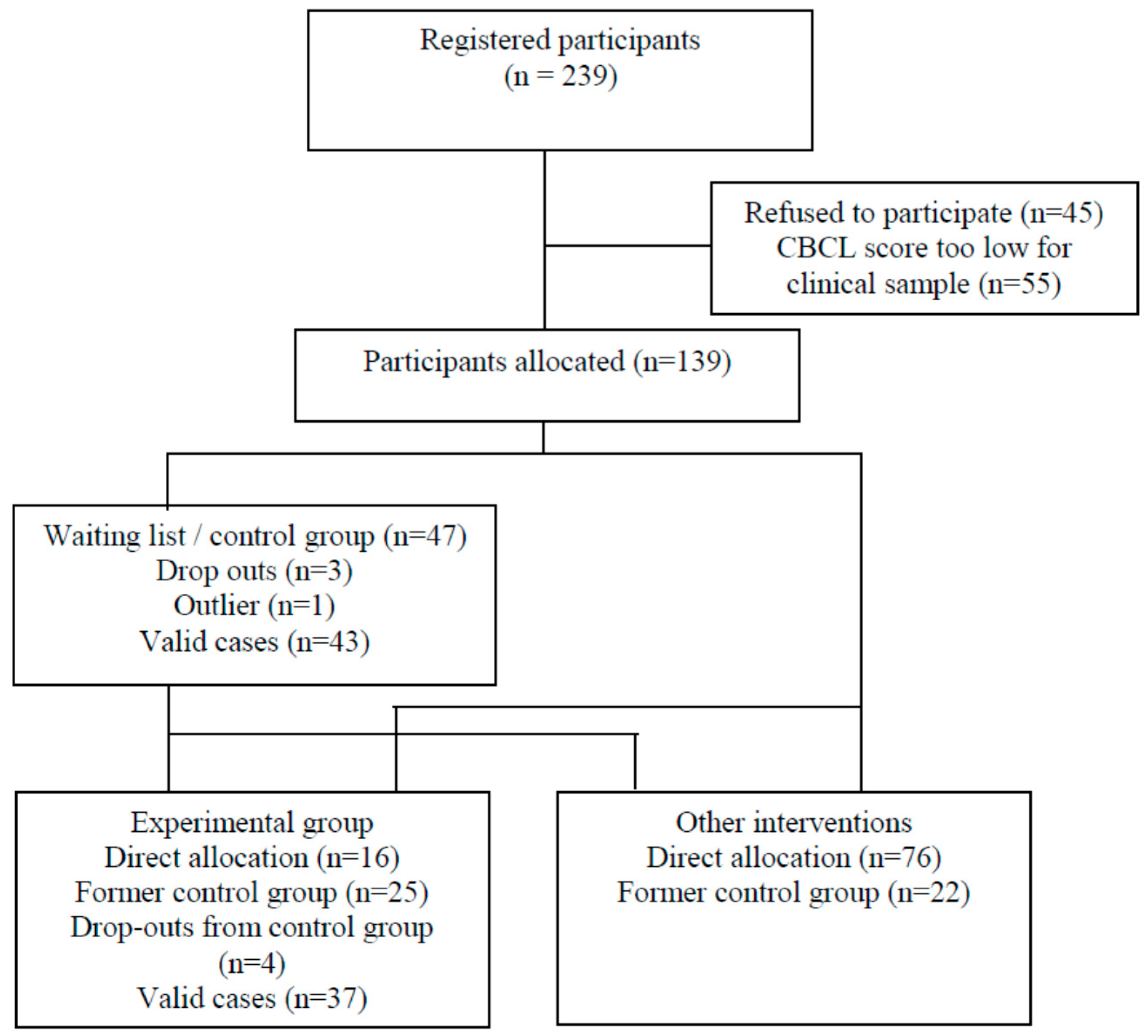
2.1. Participants
2.2. Procedure
2.3. The Confident Parents Program
3. Measures
3.1. Parental Self-Efficacy
3.2. Child Behavior
3.3. Treatment Satisfaction
3.4. Analysis Strategy
4. Results
4.1. Preliminary Analyses
4.2. Program Effect
4.2.1. Manipulation Check: Program Effect on PSE and Treatment Satisfaction
4.2.2. Program Effect on Parent-Reported Child EB
4.2.3. Program Effect on Observed Child Behavior
4.3. Predictors of Child Behavior Change
5. Discussion
5.1. Effects on Child Behavior
5.2. Moderators of Confident Parents’ Effectiveness
5.3. Clinical Implications
5.4. Limitations
5.5. Future Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Compliance with Ethical Standards
References
- Wakschlag, L.S.; Briggs-Gowan, M.J.; Carter, A.S.; Hill, C.; Danis, B.; Keenan, K.; McCarthy, K.J.; Leventhal, B.L. A developmental framework for distinguishing disruptive behavior from normative misbehavior in preschool children. J. Child Psychol. Psychiatry 2007, 48, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Bagner, D.; Rodríguez, G.; Blake, C.; Linares, D.; Carter, A. Assessment of behavioral and emotional problems in infancy: A systematic review. Clin. Child Fam. Psychol. Rev. 2012, 15, 113–128. [Google Scholar] [CrossRef] [PubMed]
- Nixon, R.D.V. Treatment of behavior problems in preschoolers: A review of parent training programs. Clin. Psychol. Rev. 2002, 22, 525–546. [Google Scholar] [CrossRef]
- Reyno, S.; McGrath, P. Predictors of parent training efficacy for child externalizing behavior problems—A meta-analytic review. J. Child Psychol. Psychiatry 2006, 47, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.B.; Shaw, D.S.; Gilliom, M. Early externalizing behavior problems: Toddlers and preschoolers at risk for later maladjustment. Dev. Psychopathol. 2000, 12, 467–488. [Google Scholar] [CrossRef] [PubMed]
- Gartstein, M.A.; Putnam, S.P.; Rothbart, M.K. Etiology of preschool behavior problems: Contributions of temperament attributes in early childhood. Infant Ment. Health J. 2012, 33, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Long, C.E.; Gurka, M.J.; Blackman, J.A. Family stress and children’s language and behavior problems: Results from the national survey of children’s health. Top. Early Child. Spec. Educ. 2008, 28, 148–157. [Google Scholar] [CrossRef]
- Martel, M.M.; Gremillion, M.L.; Roberts, B. Temperament and common disruptive behavior problems in preschool. Personal. Individ. Differ. 2012, 53, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Karreman, A.; van Tuijl, C.; van Aken, M.A.G.; Deković, M. Parenting and self-regulation in preschoolers: A meta-analysis. Infant Child Dev. 2006, 15, 561–579. [Google Scholar] [CrossRef]
- Roskam, I.; Meunier, J.C.; Stievenart, M.; Noël, M.P. When there seem to be no predetermining factors: Early child and proximal family risk predicting externalizing behavior in young children incurring no distal family risk. Res. Dev. Disabil. 2013, 34, 627–639. [Google Scholar] [CrossRef] [PubMed]
- Lorber, M.F.; Egeland, B. Parenting and infant difficulty: Testing a mutual exacerbation hypothesis to predict early onset conduct problems. Child Dev. 2011, 82, 2006–2020. [Google Scholar] [CrossRef] [PubMed]
- Stoltz, S.; Londen, M.; Deković, M.; Prinzie, P.; Orobio de Castro, B.; Lochman, J.E. Simultaneously testing parenting and social cognitions in children at-risk for aggressive behavior problems: Sex differences and ethnic similarities. J. Child. Fam. Stud. 2013, 22, 922–931. [Google Scholar] [CrossRef]
- Bornstein, M.H.; Cote, L.R.; Haynes, O.M.; Hahn, C.S.; Park, Y. Parenting knowledge: Experiential and sociodemographic factors in European American mothers of young children. Dev. Psychol. 2010, 46, 1677–1693. [Google Scholar] [CrossRef] [PubMed]
- Coleman, P.K.; Karraker, K.H. Parenting self-efficacy among mothers of school-age children: Conceptualization, measurement, and correlates. Fam. Relat. 2000, 49, 13–24. [Google Scholar] [CrossRef]
- De Montigny, F.; Lacharité, C. Perceived parental efficacy: Concept analysis. J. Adv. Nurs. 2005, 49, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Coleman, P.K.; Karraker, K.H. Maternal self-efficacy beliefs, competence in parenting, and toddlers’ behavior and developmental status. Infant Ment. Health J. 2003, 24, 126–148. [Google Scholar] [CrossRef]
- Jones, T.L.; Prinz, R.J. Potential roles of parental self-efficacy in parent and child adjustment: A review. Clin. Psychol. Rev. 2005, 25, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Heath, C.; Curtis, D.; Fan, W.; McPherson, R. The association between parenting stress, parenting self-efficacy, and the clinical significance of child ADHD symptom change following behavior therapy. Child Psychiatry Hum. Dev. 2015, 46, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.; Mash, E.J. A measure of parenting satisfaction and efficacy. J. Clin. Child Psychol. 1989, 18, 167–175. [Google Scholar] [CrossRef]
- Teti, D.; Gelfand, D. Behavioral competence among mothers of infants in the first year: The mediational role of maternal self-efficacy. Child Dev. 1991, 62, 918–929. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, M.C.; Normandeau, S.; Robaey, P. The social cognition of parents of ADHD children as a predictor of parenting practices after an intervention. Can. J. Behav. Sci. 2014, 46, 147–161. [Google Scholar] [CrossRef]
- Bugental, D.B.; Ellerson, P.C.; Lin, E.K.; Rainey, B.; Kokotovic, A.; O’Hara, N. A cognitive approach to child abuse prevention. Psychol. Violence 2010, 1, 84–106. [Google Scholar] [CrossRef]
- De Haan, A.D.; Prinzie, P.; Deković, M. Mothers’ and fathers’ personality and parenting: The mediating role of sense of competence. Dev. Psychol. 2009, 45, 1695–1707. [Google Scholar] [CrossRef] [PubMed]
- Deković, M.; Asscher, J.J.; Hermanns, J.; Reitz, E.; Prinzie, P.; Akker, A. Tracing changes in families who participated in the home-start parenting program: Parental sense of competence as mechanism of change. Prev. Sci. 2010, 11, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Leerkes, E.M.; Crockenberg, S.C. The development of maternal self-efficacy and its impact on maternal behavior. Infancy 2002, 3, 227–247. [Google Scholar] [CrossRef]
- Aunola, K.; Nurmi, J.-E. The role of parenting styles in children’s problem behavior. Child Dev. 2005, 76, 1144–1159. [Google Scholar] [CrossRef] [PubMed]
- Granic, I.; Patterson, G.R. Toward a comprehensive model of antisocial development: A dynamic systems approach. Psychol. Rev. 2006, 113, 101–131. [Google Scholar] [CrossRef] [PubMed]
- Dretzke, J.; Davenport, C.; Frew, E.; Barlow, J.; Stewart-Brown, S.; Bayliss, S.; Taylor, R.; Sandercock, J.; Hyde, C. The clinical effectiveness of different parenting programmes for children with conduct problems: A systematic review of randomised controlled trials. Child Adolesc. Psychiatry Ment. Health 2009, 3, 7. [Google Scholar] [CrossRef] [PubMed]
- Furlong, M.; McGilloway, S.; Bywater, T.; Hutchings, J.; Smith, S.M.; Donnelly, M. Behavioural and cognitive-behavioural group-based parenting programmes for early-onset conduct problems in children aged 3 to 12 years. Cochrane Database Syst. Rev. 2012, 2, CD008225. [Google Scholar]
- Kaminski, J.W.; Valle, L.A.; Filene, J.H.; Boyle, C.L. A meta-analytic review of components associated with parent training program effectiveness. J. Abnorm. Child Psychol. 2008, 36, 567–589. [Google Scholar] [CrossRef] [PubMed]
- Mouton, B.; Loop, L.; Stievenart, M.; Roskam, I. Parenting programs to reduce preschoolers’ externalizing behavior: A meta-analytic review of their behavioral or cognitive components. Child Fam. Behav. Ther. 2018, 1–33. [Google Scholar] [CrossRef]
- Weisz, J.R.; Kazdin, A.E. Evidence-Based Psychotherapies for Children and Adolescents, 2nd ed.; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Bor, W.; Sanders, M.; Markie-Dadds, C. The effects of the triple p-positive parenting program on preschool children with co-occurring disruptive behavior and attentional/hyperactive difficulties. J. Abnorm. Child Psychol. 2002, 30, 571–587. [Google Scholar] [CrossRef] [PubMed]
- Bugental, D.B.; Johnston, C. Parental and child cognitions in the context of the family. Annu. Rev. Psychol. 2000, 51, 315–344. [Google Scholar] [CrossRef] [PubMed]
- Mah, J.W.T.; Johnston, C. Parental social cognitions: Considerations in the acceptability of and engagement in behavioral parent training. Clin. Child Fam. Psychol. Rev. 2008, 11, 218–236. [Google Scholar] [CrossRef] [PubMed]
- Mouton, B.; Roskam, I. Confident mothers, easier children: A quasi-experimental manipulation of mothers’ self-efficacy. J. Child Fam. Stud. 2015, 24, 2485–2495. [Google Scholar] [CrossRef]
- Barlow, J.; Parsons, J. Group-based parent-training programmes for improving emotional and behavioural adjustment in 0–3 year old children. Cochrane Database Syst. Rev. 2002, 2, 1–33. [Google Scholar]
- Lundahl, B.; Risser, H.J.; Lovejoy, M.C. A meta-analysis of parent training: Moderators and follow-up effects. Clin. Psychol. Rev. 2006, 26, 86–104. [Google Scholar] [CrossRef] [PubMed]
- Leijten, P.; Dishion, T.J.; Thomaes, S.; Raaijmakers, M.A.J.; Orobio de Castro, B.; Matthys, W. Bringing parenting interventions back to the future: How randomized microtrials may benefit parenting intervention efficacy. Clin. Psychol. Sci. Pract. 2015, 22, 47–57. [Google Scholar] [CrossRef]
- Shelleby, E.C.; Shaw, D.S. Outcomes of parenting interventions for child conduct problems: A review of differential effectiveness. Child Psychiatry Hum. Dev. 2014, 45, 628–645. [Google Scholar] [CrossRef] [PubMed]
- Gross, D.; Garvey, C.; Julion, W.; Fogg, L.; Tucker, S.; Mokros, H. Efficacy of the Chicago parent program with low-income African American and Latino parents of young children. Prev. Sci. 2009, 10, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, B.P.; Brown, E.D.; Izard, C.E. The relations between contextual risk, earned income, and the school adjustment of children from economically disadvantaged families. Dev. Psychol. 2004, 40, 204–216. [Google Scholar] [CrossRef] [PubMed]
- McGilloway, S.; Mhaille, G.N.; Bywater, T.; Furlong, M.; Leckey, Y.; Kelly, P.; Comiskey, C.; Donnelly, M. A parenting intervention for childhood behavioral problems: A randomized controlled trial in disadvantaged community-based settings. J. Consult. Clin. Psychol. 2012, 80, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Beauchaine, T.P.; Webster-Stratton, C.; Reid, M.J. Mediators, moderators, and predictors of 1-year outcomes among children treated for early-onset conduct problems: A latent growth curve analysis. J. Consult. Clin. Psychol. 2005, 73, 371–388. [Google Scholar] [CrossRef] [PubMed]
- Gardner, F.; Hutchings, J.; Bywater, T.; Whitaker, C. Who benefits and how does it work? Moderators and mediators of outcome in an effectiveness trial of a parenting intervention. J. Clin. Child Adolesc. Psychol. 2010, 39, 568–580. [Google Scholar] [CrossRef] [PubMed]
- Leijten, P.; Raaijmakers, M.A.J.; Orobio de Castro, B.; Matthys, W. Does socioeconomic status matter? A meta-analysis on parent training effectiveness for disruptive child behavior. J. Clin. Child Adolesc. Psychol. 2013, 42, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Howe, G.W.; Beach, S.R.H.; Brody, G.H. Microtrial methods for translating gene-environment dynamics into preventive interventions. Prev. Sci. 2010, 11, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D.; Grégoire, J. Echelle D’intelligence de Wechsler Pour Enfants: Manuel: WISC-III; Les Editions du Centre de Psychologie Appliquée: Paris, France, 1996. [Google Scholar]
- Crowell, J.A.; Feldman, S.S. Mothers’ internal models of relationships and children’s behavioral and developmental status: A study of mother-child interaction. Child Dev. 1988, 59, 1273–1285. [Google Scholar] [CrossRef] [PubMed]
- Crowell, J.A.; Warner, D.E.; Davis, C.R.; Marraccini, M.; Dearing, E. The influence of childhood adversity on mothers’ behavior with preschoolers: Role of maternal attachment coherence, dissociative symptoms, and marital behaviors. Res. Hum. Dev. 2010, 7, 274–291. [Google Scholar] [CrossRef]
- Loop, L.; Mouton, B.; Brassart, E.; Roskam, I. The observation of child behavior during parent-child interaction: The psychometric properties of the crowell procedure. J. Child Fam. Stud. 2016, 26, 1040–1050. [Google Scholar] [CrossRef]
- Sanders, M.; Markie-Dadds, C.; Tully, L.; Bor, W. The triple p-positive parenting program: A comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. J. Consult. Clin. Psychol. 2000, 68, 624–640. [Google Scholar] [CrossRef] [PubMed]
- Coffee, P.; Rees, T. When the chips are down: Effects of attributional feedback on self-efficacy and task performance following initial and repeated failure. J. Sports Sci. 2011, 29, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Regulation of cognitive process through perceived self-efficacy. Dev. Psychol. 1989, 25, 729–735. [Google Scholar] [CrossRef]
- Gaviţa, O.A.; Joyce, M.R.; David, D. Cognitive behavioral parent programs for the treatment of child disruptive behavior. J. Cogn. Psychother. 2011, 25, 240–256. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Ellis, A. Can rational-emotive behavior therapy (REBT) and acceptance and commitment therapy (act) resolve their differences and be integrated? J. Ration.-Emotive Cogn.-Behav. Ther. 2005, 23, 153–168. [Google Scholar] [CrossRef]
- Juffer, F.; Bakermans-Kranenburg, M.J.; van Ijzendoorn, M.H. Promoting Positive Parenting: An Attachment-Based Intervention; Taylor & Francis Group: New York, NY, USA; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2008. [Google Scholar]
- Achenbach, T. Multicultural evidence-based assessment of child and adolescent psychopathology. Transcult. Psychiatry 2010, 47, 707–726. [Google Scholar] [CrossRef] [PubMed]
- Fombonne, E. The child behaviour checklist and the rutter parental questionnaire: A comparison between two screening instruments. Psychol. Med. 1989, 19, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Wewers, M.E.; Lowe, N.K. A critical review of visual analogue scales in the measurement of clinical phenomena. Res. Nurs. Health 1990, 13, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.B. Estimating effect sizes from pretest-posttest-control group designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Gavin, M. Review of hierarchical linear models: Applications and data analysis methods, 2nd ed. Organ. Res. Methods 2004, 7, 228–231. [Google Scholar] [CrossRef]
- Raudenbush, S.W.; Bryk, A.S.; Congdon, R. HLM 6 for Windows; Scientific Software International, Inc.: Skokie, IL, USA, 2004. [Google Scholar]
- Johnston, C.; Mah, J.W.T.; Regambal, M. Parenting cognitions and treatment beliefs as predictors of experience using behavioral parenting strategies in families of children with attention-deficit/hyperactivity disorder. Behav. Ther. 2010, 41, 491–504. [Google Scholar] [CrossRef] [PubMed]
- Gerdes, A.C.; Hoza, B. Maternal attributions, affect, and parenting in attention deficit hyperactivity disorder and comparison families. J. Clin. Child Adolesc. Psychol. 2006, 35, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Maughan, D.R.; Christiansen, E.; Jenson, W.R.; Olympia, D.; Clark, E. Behavioral parent training as a treatment for externalizing behaviors and disruptive behavior disorders: A meta-analysis. Sch. Psychol. Rev. 2005, 34, 267–286. [Google Scholar]
- Sofronoff, K.; Farbotko, M. The effectiveness of parent management training to increase self-efficacy in parents of children with Asperger syndrome. Autism 2002, 6, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Wittkowski, A.; Dowling, H.; Smith, D.M. Does engaging in a group-based intervention increase parental self-efficacy in parents of preschool children? A systematic review of the current literature. J. Child Fam. Stud. 2016, 25, 3173–3191. [Google Scholar] [CrossRef] [PubMed]
- Deković, M.; Asscher, J.J.; Manders, W.A.; Prins, P.J.M.; van der Laan, P. Within-intervention change: Mediators of intervention effects during multisystemic therapy. J. Consult. Clin. Psychol. 2012, 80, 574–587. [Google Scholar] [CrossRef] [PubMed]
- Donovan, W.L.; Leavitt, L.A.; Walsh, R.O. Maternal self-efficacy: illusory control and its effect on susceptibility to learned helplessness. Child Dev. 1990, 61, 1638–1647. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.R.; Gettings, P.E.; Guntzviller, L.M.; Munz, E.A. Parental self-efficacy and sensitivity during playtime interactions with young children: Unpacking the curvilinear association. J. Appl. Commun. Res. 2014, 42, 409–431. [Google Scholar] [CrossRef]
- Cassé, J.; Oosterman, M.; Schuengel, C. Verbal persuasion and resilience of parenting self-efficacy: Preliminary findings of an experimental approach. Fam. Sci. 2015, 6, 23–30. [Google Scholar] [CrossRef]
- Sanders, M.; Woolley, M. The relationship between maternal self-efficacy and parenting practices: Implications for parent training. Child Care Health Dev. 2005, 31, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.H.; Kellam, S.G.; Kaupert, S.; Muthén, B.O.; Wang, W.; Muthén, L.K.; Chamberlain, P.; PoVey, C.L.; Cady, R.; Valente, T.W.; et al. Partnerships for the design, conduct, and analysis of effectiveness, and implementation research: Experiences of the prevention science and methodology group. Adm. Policy Ment. Health Ment. Health Serv. Res. 2012, 39, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.H.; Liao, J. Principles for designing randomized preventive trials in mental health: An emerging developmental epidemiology paradigm. Am. J. Community Psychol. 1999, 27, 673–710. [Google Scholar] [CrossRef] [PubMed]
- Pierce, T.; Boivin, M.; Frenette, É.; Forget-Dubois, N.; Dionne, G.; Tremblay, R.E. Maternal self-efficacy and hostile-reactive parenting from infancy to toddlerhood. Infant Behav. Dev. 2010, 33, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Roskam, I.; Brassart, E.; Loop, L.; Mouton, B.; Schelstraete, M.A. Do parenting variables have specific or widespread impact on covariates? The power of self-efficacy or verbal responsiveness improvement. Child Fam. Behav. Ther. 2016, 38, 142–163. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Control (n = 43) | Experimental (n = 37) | Total (N = 80) | Tests T-Tests t(79) or X²(1) |
|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | ||
| Parent’s age | 37.15 (5.03) | 38.36 (6.18) | 37.69 (5.57) | 0.93 |
| Parent’s gender (%mothers) | 77% | 73% | 75% | 0.15 |
| Child’s age (months) | 53.84 (8.69) | 56.30 (7.53) | 54.98 (8.21) | 1.34 |
| Child’s gender (%boys) | 53.5% | 51.4% | 52.5% | 0.04 |
| Child’s IQ | 10.22 (2.35) | 11.02 (2.19) | 10.60 (2.30) | 1.56 |
| Educational level (years) | 14.37 (2.53) | 14.65 (2.24) | 14.50 (2.39) | 0.51 |
| Monthly income (%) | ||||
| <2000 euros | 27.9% | 18.92% | 23.8% | 1.04 |
| 2000–4000 euros | 34.9% | 43.24% | 38.8% | |
| >4000 euros | 37.2% | 37.84% | 37.5% | |
| Chaos | 5.91 (2.76) | 5.11 (2.96) | 5.54 (2.86) | 1.25 |
| Single parent families (%) | 14.0% | 8.1% | 11.3% | 0.68 |
| Socio-economic risk | 1.05 (1.02) | 0.76 (0.89) | 0.91 (0.97) | 1.34 |
| Previous counseling | 30.20% | 35.10% | 32.5% | 0.22 |
| Baseline | Post-Test | Follow-Up | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Child EB | Child in Free Play | Child in Frustration Tasks | Parental Self-Efficacy | Child EB | Child in Free Play | Child in Frustration Tasks | Parental Self-Efficacy | Child EB | Child in Free Play | Child in Frustration Tasks | Parental Self-Efficacy | |
| Child EB | - | −0.14 | −0.28 * | −0.53 ** | - | −0.18 | −0.23 * | −0.49 ** | - | −0.42 * | −0.42 * | −0.73 ** |
| Child in free play | - | 0.46 ** | 0.17 | - | 0.44 ** | 0.01 | - | 0.48 ** | 0.29 † | |||
| Child in frustration tasks | - | 0.22 * | - | 0.10 | - | 0.38 * | ||||||
| Parental self-efficacy | - | - | - | - | ||||||||
| Baseline | Post-Test | Follow-Up | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control (n = 43) | Experimental (n = 37) | t-test X² | Control (n = 43) | t-test with Base-Line | Cohen’s d | t-test Confi-Dence Intervals | Experimental (n = 37) | t-Test with Baseline | Cohen’s d | t-test Confi-Dence Intervals | Morris’s ES | Experimental (n = 37) | t- Test with Baseline | Cohen’s d | t-Test Confi-Dence Intervals | ||||||
| M | SD | M | SD | M | SD | M | SD | M | SD | ||||||||||||
| Parental self-efficacy | 2.96 | 0.69 | 3.09 | 0.76 | −0.85 | 3.12 | 0.69 | −2.73 ** | 0.42 | [−0.29 −0.04] | 3.45 | 0.65 | −4.47 *** | 0.75 | [−0.52 −0.20] | −0.27 | 3.65 | 0.64 | −7.99 *** | 1.35 | [−0.73 −0.43] |
| Children’s observed positive behavior in free play | 34.81 | 3.42 | 34.65 | 2.78 | 0.23 | 34.95 | 2.57 | −0.29 | 0.04 | [−1.12 0.84] | 35.28 | 2.85 | −0.92 | 0.15 | [−1.87 0.70] | −0.09 | 34.95 | 2.38 | −0.57 | 0.09 | [−1.36 0.77] |
| Children’s observed positive behavior in frustration tasks | 94.33 | 15.23 | 99.08 | 7.46 | −1.81 | 94.47 | 14.15 | −0.07 | 0.01 | [−4.17 3.89] | 100.67 | 8.08 | −0.92 | 0.15 | [−3.73 1.40] | −0.14 | 102.16 | 6.96 | −2.14 * | 0.35 | [−6.00 −0.16] |
| Child’s externalizing behavior (CBCL) | 23.26 | 9.24 | 21.24 | 8.12 | 1.03 | 21.60 | 8.24 | 1.65 | 0.25 | [−0.37 3.67] | 18.92 | 8.46 | 3.74 ** | 0.62 | [1.24 4.20] | 0.12 | 15.67 | 7.29 | 5.50 *** | 0.92 | [3.61 7.83] |
| Fixed Effects | Random Effects Variance | |||
|---|---|---|---|---|
| Coefficient | SE | t(36) | ||
| Child’s EB (CBCL) | ||||
| Intercept | 24.12 *** | 1.70 | 14.17 | 75.38 *** |
| slope | −2.74 *** | 0.51 | −5.38 | 2.46 † |
| Child’s observed positive behavior in frustration | ||||
| intercept | 97.55 *** | 1.77 | 54.97 | 46.74 ** |
| slope | 1.74 * | 0.71 | 2.16 | 3.58 |
| Fixed Effects | Child’s EB (CBCL) | Child’s Observed Positive Behavior in Frustration | ||||
|---|---|---|---|---|---|---|
| Coefficient | SE | t(31) | Coefficient | SE | t(31) | |
| Level 1: Prediction of time-varying fluctuations | ||||||
| Parental self-efficacy | −3.68 * | 1.55 | −2.37 | −2.86 | 2.68 | −1.07 |
| Level 2: Prediction of linear change | ||||||
| Intercept of the slope | −3.29 ** | 1.07 | −3.07 | 2.43 | 1.46 | 1.66 |
| Mean parental self-efficacy | −2.97 *** | 0.52 | −5.77 | 0.06 | 0.57 | 0.11 |
| Parents’ gender | 0.16 | 0.66 | 0.23 | 1.09 * | 0.53 | 2.05 |
| Socio-economic risk | 0.85 * | 0.38 | 2.25 | −0.51 | 0.35 | −1.45 |
| Child’s age | −0.09 * | 0.04 | −2.54 | 0.17 *** | 0.04 | 4.64 |
| Child’s gender | 0.88 | 0.60 | 1.46 | −1.07 | 0.56 | −1.92 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mouton, B.; Loop, L.; Stiévenart, M.; Roskam, I. Confident Parents for Easier Children: A Parental Self-Efficacy Program to Improve Young Children’s Behavior. Educ. Sci. 2018, 8, 134. https://doi.org/10.3390/educsci8030134
Mouton B, Loop L, Stiévenart M, Roskam I. Confident Parents for Easier Children: A Parental Self-Efficacy Program to Improve Young Children’s Behavior. Education Sciences. 2018; 8(3):134. https://doi.org/10.3390/educsci8030134
Chicago/Turabian StyleMouton, Bénédicte, Laurie Loop, Marie Stiévenart, and Isabelle Roskam. 2018. "Confident Parents for Easier Children: A Parental Self-Efficacy Program to Improve Young Children’s Behavior" Education Sciences 8, no. 3: 134. https://doi.org/10.3390/educsci8030134
APA StyleMouton, B., Loop, L., Stiévenart, M., & Roskam, I. (2018). Confident Parents for Easier Children: A Parental Self-Efficacy Program to Improve Young Children’s Behavior. Education Sciences, 8(3), 134. https://doi.org/10.3390/educsci8030134