
Aspects Concerning “Play” for the Promotion of Preschool Children with Severe Speech- and Language Impairment

Abstract
:
1. Introduction
2. Background
3. Aim
4. Material and Methods
- The child plays alone vs. plays in a group and alone;
- During play the child shows limited interest vs. shows versatile interest;
- Planning of actions during play is insecure vs. confident;
- Social skills during play are marginal vs. age-appropriate;
- The child’s frustration tolerance is low vs. adequate.
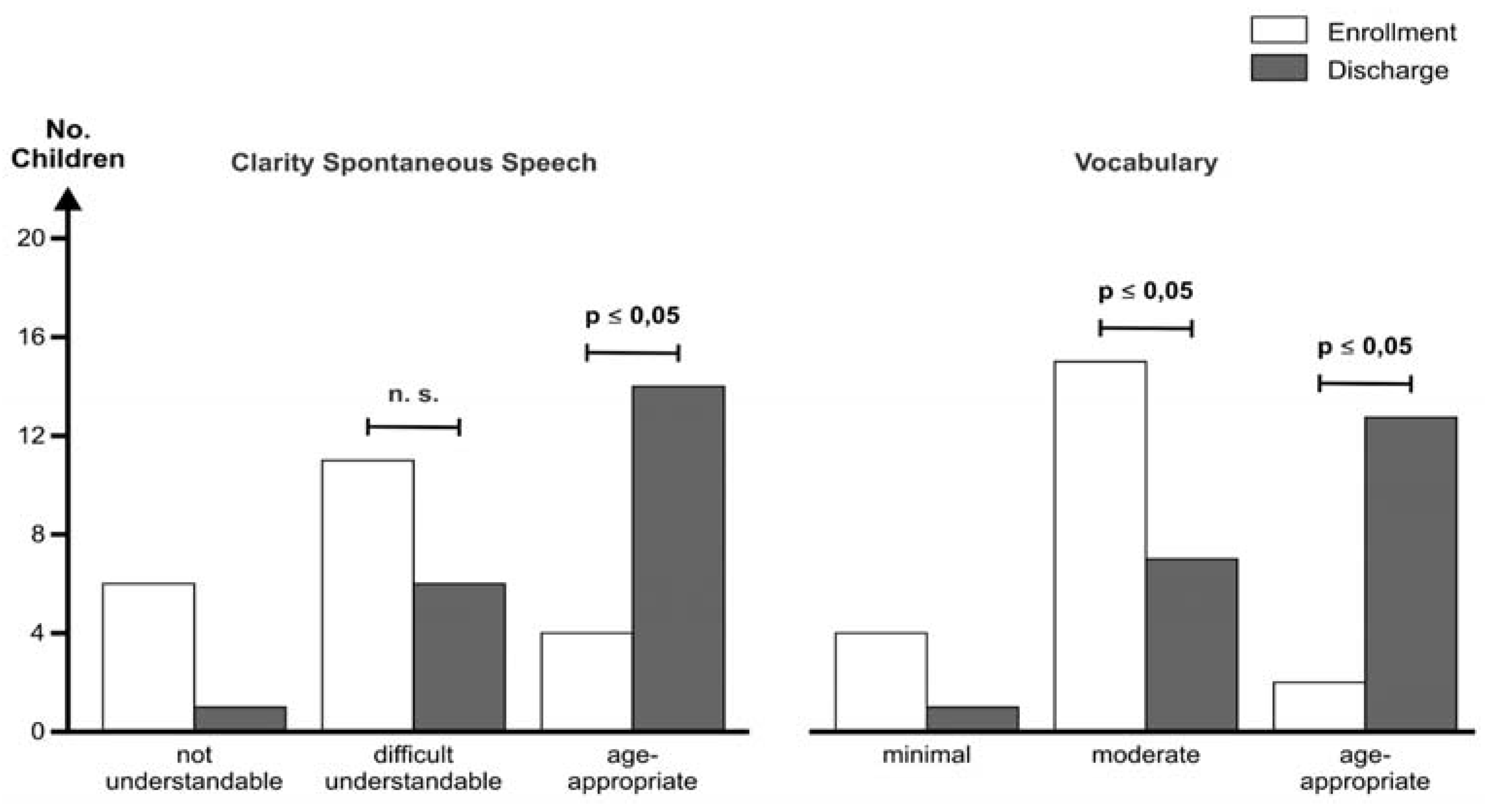
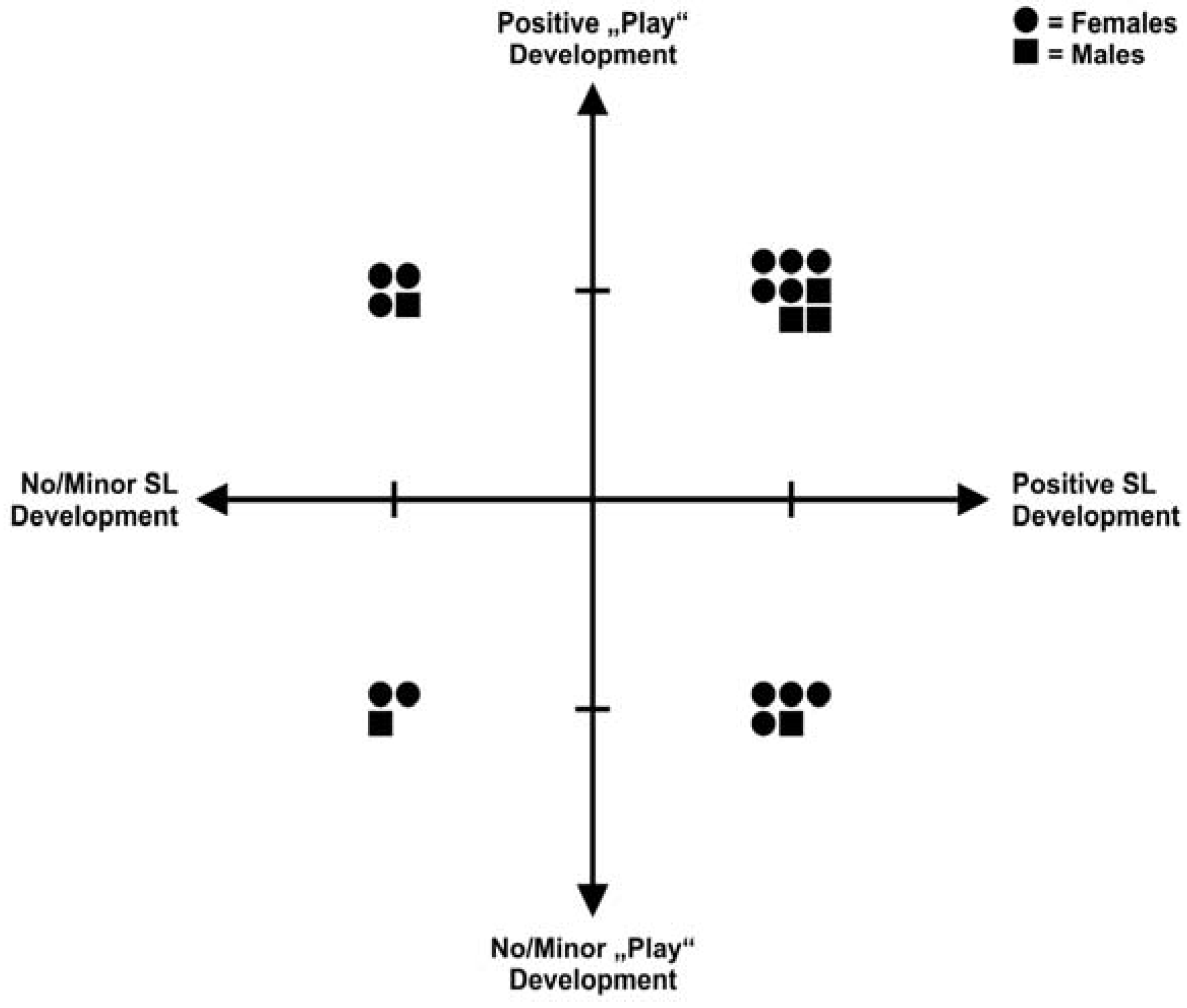
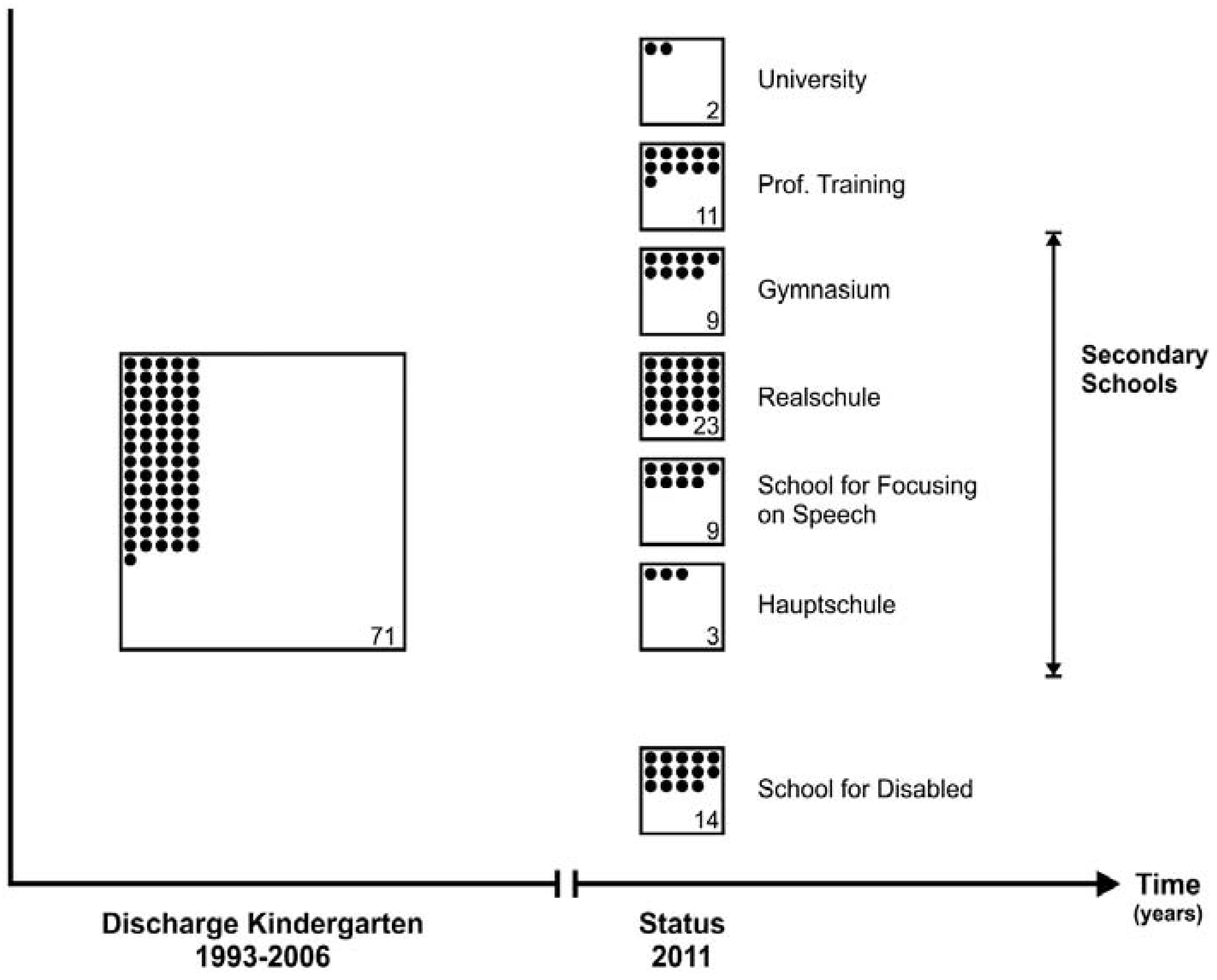
5. Results
6. Discussion
7. Conclusions
Author Contributions
Conflicts of Interest
Definitions
| Language | The set of symbols (usually words or signs) which are organized by convention to communicate ideas. |
| Speech | The physical production of language. |
| Articulation | The physical movement of the mouth and throat involved in making the different speech sounds. |
References
- Glogowska, M.; Roulstone, S.; Peters, T.J.; Enderby, P. Early speech- and language-impaired children: Linguistic, literacy, and social outcomes. Dev. Med. Child Neurol. 2006, 48, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Heckman, J.J. Integrating Personality Psychology into Economics; NBER Working Paper No. 17378; National Bureau of Economic Research: Cambridge, MA, USA, 2011. [Google Scholar]
- Bodrova, E. Make-believe play vs. academic skills: A Vygotskian approach to today’s dilemma of early childhood education. Eur. Early Child. Educ. 2008, 16, 369–381. [Google Scholar]
- Hoff, E.; Tian, C. Socioeconomic status and cultural influences on language. J. Commun. Disord. 2005, 38, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Hoff, E. How social context support and shape language development. Dev. Rev. 2006, 26, 55–88. [Google Scholar] [CrossRef]
- Vygotsky, L.S. The Role of Play in Development. In Mind in Society; Cole, M., John-Steiner, V., Scribner, S., Souberman, E., Eds.; Harvard University Press: Cambridge, MA, USA, 1978; [1933]. [Google Scholar]
- von Suchodoletz, W. Sprech- und Sprachstörungen, Reihe: Leitfaden Kinder- und Jugendpsychotherapie; Hogrefe: Göttingen, Germany; Bern, Switzerland; Vienna, Austria, 2013; pp. 16–18. [Google Scholar]
- Needlman, R. Growth and Development. In Nelson Textbook of Pediatrics, 15th ed.; Behrman, R., Kliegman, R., Arvin, A., Eds.; W.B. Saunders: London, UK; Toronto, ON, Canada; Philadelphia, PA, USA, 1996; pp. 30–72. [Google Scholar]
- Gallagher, A.L.; Chiat, S. Evaluation of speech and language therapy interventions for pre-school children with specific language impairment: A comparison of outcomes following specialist intensive, nursery-based and no intervention. Int. J. Lang. Commun. Dis. 2009, 44, 616–638. [Google Scholar] [CrossRef] [PubMed]
- Ullrich, D.; Ullrich, K.; Marten, M. A longitudinal assessment of early childhood education with integrated speech therapy for children with significant language impairment in Germany. Int. J. Lang. Commun. Dis. 2014, 49, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Law, J.; Boyle, J.; Harris, J.; Harkness, A.; Nye, C. Screening for speech and language delay: A systematic review of the literature. Health Technol. Assess. 1998, 2, 1–184. [Google Scholar] [CrossRef] [PubMed]
- Wake, M.; Biostas, E.; Tobin, Sh.; Levickis, P.; Gold, L.; Ukoumunne, O.C.; Zenes, N.; Goldfeld, Sh.; Law, J.; Reilly, S. Randomized trial of a population-base, home-delivered Intervention for preschool language delay. Pediatrics 2013, 132, e895–e904. [Google Scholar] [CrossRef] [PubMed]
- Flöther, M.; Schlüter, E.; Bruns, T. Interdisziplinaere Foerderung und Behandlung bei Hoer- und Sprachstoerungen—Ergebnisse zur Wirksamkeit eines Konzepts aus Niedersachen (Multidisciplinary assessment and management of children with hearing and language disorders—An assessment of the effectiveness of a concept from Lower Saxony, Germany). LOGOS Interdiszip. 2011, 19, 282–292. [Google Scholar]
- Durkin, K.; Conti-Ramsden, G. Language, Social behavior, and the quality of friendships in adolescents with and without a history of specific language impairment. Child Dev. 2007, 78, 1441–1457. [Google Scholar] [CrossRef] [PubMed]
- Miniscalco, C.; Hagberg, B.; Kadesjö, B.; Westerlund, M.; Gillberg, C. Narrative skills, cognitive profiles and neuropsychiatric disorders in 7–8-year-old children with late developing language. Int. J. Lang. Commun. Dis. 2007, 42, 665–681. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Declaration of Helsinki Ethical Principles of Medical Research Involving Human Subjects. 1964. Available online: http://www.wma.net/en/30publications/10policies/b3/ (accessed on 27 October 2010).
- Grimm, H. SETK 3–5: Sprachentwicklungstest für 3–5 jährige Kinder; Hogrefe: Göttingen, Germany, 2001. [Google Scholar]
- Kiese-Himmel, C. AWST-R: Aktiver Wortschatztest für 3–5 jährige Kinder; Hogrefe: Göttingen, Germany, 2005. [Google Scholar]
- Fox, A. TROG-D: Test zur Überprüfung des Grammatikverständnisses, 5th ed.; Schulz-Kirchner-Verlag: Idstein, Germany, 2011. [Google Scholar]
- Grimme, H.; Schöler, H. HSET—Heidelberger Sprachentwicklungstest; Hogrefe: Göttingen, Germany, 1991. [Google Scholar]
- Hild, U. Bilderbuch zur Aussprachediagnostik bei Kindern; Orca GbR: Kassel, Germany, 2002. [Google Scholar]
- Snijders-Oomen. Non-verbal Intelligence Test SON-R 2½—7; Hild, P., Winkel, M., Wijnberg-Williams, B., Laros, J., Eds.; Swets & Zeitlinger B.V.: Lisse, The Netherland, 1997. [Google Scholar]
- Ricken, G.; Fritz, A.; Schuck, K.; Preuss, U. (Eds.) HAWIVA III—Hannover-Wechsler-Intelligenztest für das Vorschulalter III; Huber-Verlag/Hogrefe: Göttingen, Germany, 2007.
- Cattell, R.; Weiss, R.; Osterland, J. CFT1: Grundintelligenztest Skala 1, 5th ed.; Hogrefe: Göttingen, Germany, 1997. [Google Scholar]
- Ziler, H.; Brosat, H.; Tötemeyer, N. Der Mann-Zeichen-Test; Hogrefe: Göttingen, Germany, 2007. [Google Scholar]
- Hammill, D.; Pearson, N.; Voress, J. Developmental Test of Visual Perception 2nd edit (DTVP-2); Hogrefe: Göttingen, Germany; Bern, Switzland; Vienna, Austria, 2007. [Google Scholar]
- Zimmer, R.; Volkamer, M. MOT 4–6: Motoriktest für vier- bis sechsjährige Kinder, 2nd ed.; Verlag Weinheim: Landsberg, Germany, 1987. [Google Scholar]
- Ayres, A.J.; Robbins, J. Sensory Integration and the Child; Western Psychological Services: Torrance, CA, USA, 1979. [Google Scholar]
- Zollinger, B. Die Entdeckung der Sprache, 6th ed.; Haupt: Bern, Switzerland; Stuttgart, Germany, 2004. [Google Scholar]
- Beyer, A.; Fastabend, S.; Liebers, E.; Per, G.; Schilling, M. Gelsenkirchener Entwicklungsbegleiter; DGVT Verlag: Tübingen, Germany, 2004. [Google Scholar]
- World Health Organization; ICF-CY. International Classification of Functioning, Disability and Health. Children & Youth Version (German Edition); Verlag Hans Huber: Bern, Switzerland, 2011. [Google Scholar]
- Stark, N.J. CDG Whitepapers: Registry Studies: Why and How. Available online: http://clinicaldevice.typepad.com/cdg_whitepapers/2011/07/registry-studies-why-and-how.html (accessed on 7 January 2016).
- Durkin, K.; Simkin, Z.; Knox, E.; Conti-Ramsden, G. Specific language impairment and school outcomes. II: Educational context, student satisfaction, and post-compulsory progress. Int. J. Lang. Commun. Dis. 2009, 44, 36–55. [Google Scholar] [CrossRef] [PubMed]
- Heckman, J.J. Investing in disadvantaged young children is an economically efficient policy. In Building the Economic Case for Investments in Preschool; Committee for Economic Development: New York, NY, USA, 2006. [Google Scholar]
- Goldberg, S.; Grusec, J.E.; Jenkins, J.M. Confidence in protection: Arguments for a narrow definition of attachment. J. Fam. Psychol. 1999, 13, 475–483. [Google Scholar] [CrossRef]
- Grossmann, K.; Grossmann, K.E. Bindungen—Das Gefüge Psychischer Sicherheit, 5th ed.; Klett-Cotta: Stuttgart, Germany, 2012. [Google Scholar]
- Nader-Grosbois, N.; Vieillevoye, S. Variability of self-regulatory strategies in children with intellectual disability and typically developing children in pretended play situations. J. Intellect. Disabil. Res 2012, 56, 140–156. [Google Scholar] [CrossRef] [PubMed]
- Achtergarde, S.; Müller, J.; Postert, Ch.; Wessing, I.; Mayer, A.; Romer, G. Der Zusammenhang von Bindungsmustern und der Entwicklung von Angstsymptomen im Kindes- und Jugendalter. (Attachment pattern and their relation to the development of anxiety symptoms in childhood and adolescence). Prax Kinderpsychol. Kinderpsychiatr. 2015, 64, 496–526. [Google Scholar] [CrossRef] [PubMed]
- Stagnitti, K.; Bailey, A.; Stevenson, E.H.; Reynolds, E.; Kidd, E. An investigation into the effect of play based instruction on the development of play skills and oral langauge: A 6-month longitudinal study. J. Child Res. 2015, 5, 1–18. [Google Scholar]
- Ervin-Tripp, S. Play in language development. In Play and the Social Context of Development in Early Care and Education; Scales, B., Almy, M., Nicolopoulou, A., Ervin-Tripp, S., Eds.; Teachers College, Columbia University: New York, NY, USA, 1991; pp. 84–97. [Google Scholar]
- Trevarthen, C.; Aitken, K.J. Infant intersubjectivity: Research, theory, and clinical applications. J. Child Psychol. Psychiatry 2001, 42, 3–48. [Google Scholar] [CrossRef] [PubMed]
- Uren, N.; Stagnitti, K. Pretend play, social competence and involvement in children aged 5–7 years: The concurrent validity of the Child-Initiated Pretend Play Assessment. Aust. Occup. Ther. J. 2009, 56, 33–40. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Skills | Sources | Test Procedure |
|---|---|---|
| Language Skills | Examination | SETK—3–5 Test for Speech Development of children aged 3–5 years; validated [17]. AWST-R—Vocabulary test for children aged 3–5 years; validated [18]. TROG-D—Grammar test; validated [19]. HSET—Test for Speech Development (Heidelberg); validated [20]. Assessment of Paediatric phonetics and pronunciation; not validated [21]. Status speech-/language development, not validated—Educator. |
| Number of siblings | Questionnaire, case files | |
| Family Income | Questionnaire | |
| Duration of STK attendance | Questionnaire | |
| IQ | Examination | SON-R; validated [22]. HAWIWA III; validated [23]. CFT1; validated [24]. Der Mann-Zeichen-Test; validated [25]. |
| Self-confidence | Examination | |
| Focus/Concentration | Examination | |
| Auditory Perception | Examination | |
| Visual perception | Examination | FEW-2: Frostig Test for Assessment of Visual Perception; validated [26]. |
| Ideas at crafts/construction | Examination | |
| Gross motor skills | Examination | MOT 4–6: Evaluation of Motor skills for children aged 4–6 years; validated [27]. |
| Criteria | Not Age-Appropriate | Age-Appropriate |
|---|---|---|
| Plays alone vs. Plays in Group and alone | 0 | 1 |
| During Play Limited Interest vs. Versatile Interests | 0 | 1 |
| Planning Actions Insecure vs. Confident | 0 | 1 |
| Social Skills Marginal vs Age-appropriate | 0 | 1 |
| Frustration Tolerance Low vs Adequate | 0 | 1 |
| TOTAL SCORE (Maximum 5) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullrich, D.; Marten, M. Aspects Concerning “Play” for the Promotion of Preschool Children with Severe Speech- and Language Impairment. Educ. Sci. 2016, 6, 9. https://doi.org/10.3390/educsci6010009
Ullrich D, Marten M. Aspects Concerning “Play” for the Promotion of Preschool Children with Severe Speech- and Language Impairment. Education Sciences. 2016; 6(1):9. https://doi.org/10.3390/educsci6010009
Chicago/Turabian StyleUllrich, Dieter, and Magret Marten. 2016. "Aspects Concerning “Play” for the Promotion of Preschool Children with Severe Speech- and Language Impairment" Education Sciences 6, no. 1: 9. https://doi.org/10.3390/educsci6010009
APA StyleUllrich, D., & Marten, M. (2016). Aspects Concerning “Play” for the Promotion of Preschool Children with Severe Speech- and Language Impairment. Education Sciences, 6(1), 9. https://doi.org/10.3390/educsci6010009