

What We Don’t Know Really Will Hurt Us: Examining Trauma Awareness Knowledge, Strategies, and Training in Ireland’s Early Childhood Education and Care Profession


Abstract
1. Introduction
1.1. Theoretical Framework and Literature Review
1.2. Trauma-Informed Practice
1.3. Early Childhood Education and Care in Ireland: Contextual Understanding
1.4. Relational Pedagogy
2. Materials and Methods
2.1. Research Design
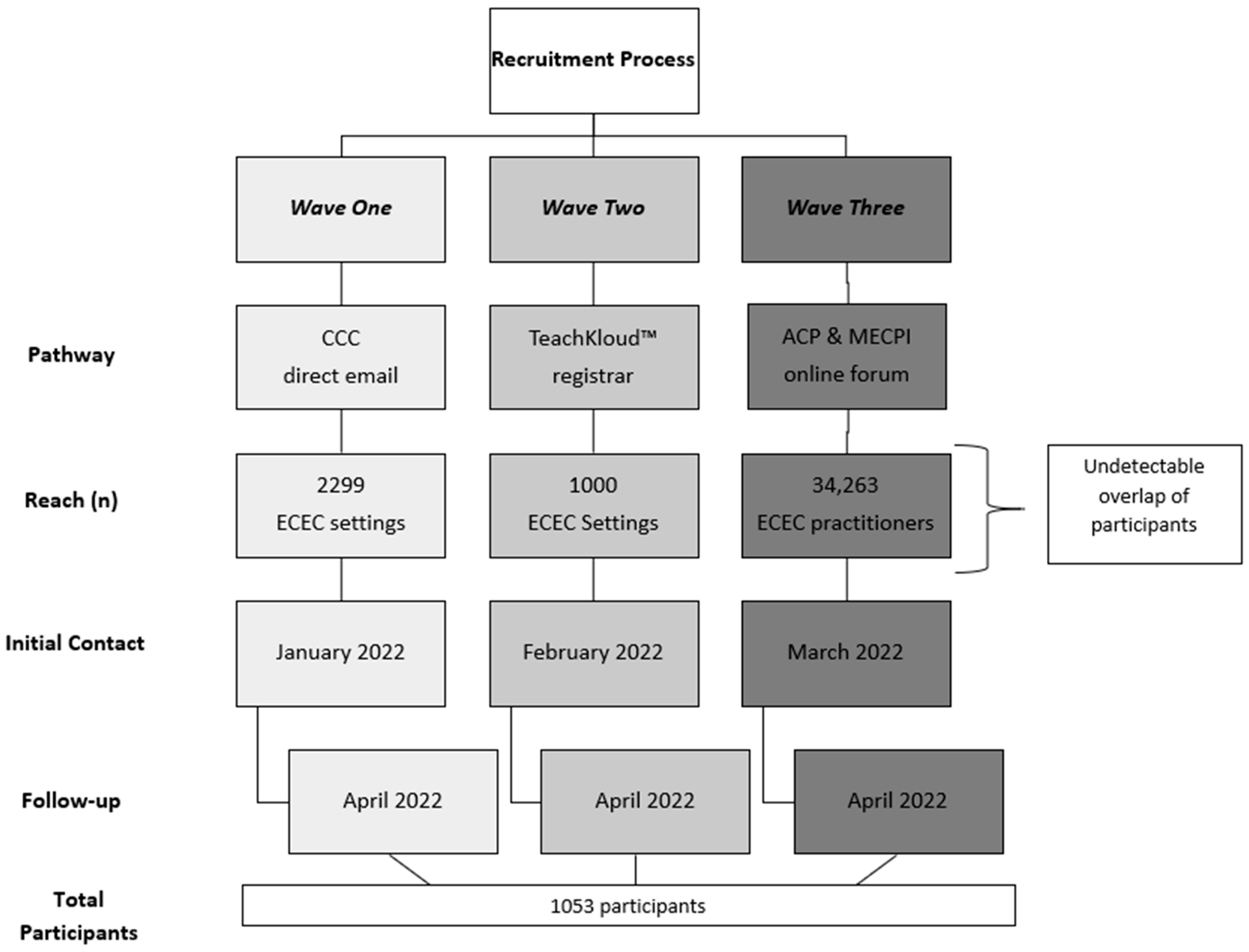
2.2. Participants
2.3. Instrument Development
2.4. Pilot
2.5. Procedures
2.6. Data Analysis
3. Results
3.1. Trauma-Related Knowledge
3.2. Trauma-Based Strategies
3.3. Trauma-Related Training and Education
3.3.1. Initial Practitioner Education (IPE)
3.3.2. Continuous Professional Development (CPD)
3.4. The Role of Formal Education
4. Discussion
4.1. Trauma-Related Knowledge
4.2. Trauma-Related Strategies
4.3. Trauma-Related Training
4.3.1. Initial Practitioner Education (IPE)
4.3.2. Continuous Professional Development (CPD)
4.4. The Role of Formal Education
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Butler, J.; Clerkin, F.; Cummins, A. Grounded in Love, Rooted in Relationships: Building Trauma-Sensitive Approaches in Early Childhood Education and Care. Leanbh Óg 2022, 15, 62–70. [Google Scholar]
- Butler, J. Trauma Sensitive Early Childhood Care and Education; Early Childhood Ireland: Dublin, Ireland, 2020; Available online: https://www.earlychildhoodireland.ie/scealta-blog/trauma-sensitive-early-childhood-care-and-education/ (accessed on 13 October 2023).
- Kennedy, F. Prevention & Early Intervention Series Focussed Policy Assessment No. 6 Family Services Supporting Children and Their Families; Department of Public Expenditure and Reform: Dublin, Ireland, 2019. [Google Scholar]
- Conners Edge, N.A.; Holmes, K.; Wilburn, E.H.; Sutton, M. Fostering Informed and Responsive Systems for Trauma in Early Care and Education (FIRST; ECE): A Preliminary Evaluation. Early Child. Educ. J. 2022, 52, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Loomis, A.M.; Felt, F. Knowledge, Skills, and Self-Reflection: Linking Trauma Training Content to Trauma-Informed Attitudes and Stress in Preschool Teachers and Staff. Sch. Ment. Health 2021, 13, 101–113. [Google Scholar] [CrossRef]
- Peterson, S. About Child Trauma; National Child Traumatic Stress Network: Los Angeles, CA, USA, 2023; Available online: https://www.nctsn.org/what-is-child-trauma/about-child-trauma (accessed on 6 September 2023).
- DeAngelis, T. The Legacy of Trauma: An Emerging Line of Research Is Exploring How Historical and Cultural Traumas Affect Survivors’ Children for Generations to Come; American Psychological Association: Washington, DC, USA, 2019; Available online: https://www.apa.org/monitor/2019/02/legacy-trauma (accessed on 21 July 2023).
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults. The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, K. ACEs and Intergenerational Trauma; Centre for Child Counselling: Palm Beach Gardens, FL, USA, 2020; Available online: https://www.centerforchildcounseling.org/aces-and-intergenerational-trauma/ (accessed on 5 November 2023).
- Counts, C.J.; Ginty, A.T.; Larsen, J.M.; Kampf, T.D.; John-Henderson, N.A. Childhood Trauma and Cortisol Reactivity: An Investigation of the Role of Task Appraisals. Front. Psychol. 2022, 13, 803339. [Google Scholar] [CrossRef] [PubMed]
- Coates, D. Impact of Childhood Abuse: Biopsychosocial Pathways through Which Adult Mental Health Is Compromised. Aust. Soc. Work 2010, 63, 391–403. [Google Scholar] [CrossRef]
- Franke, H.A. Toxic Stress: Effects, Prevention and Treatment. Children 2014, 1, 390–402. [Google Scholar] [CrossRef] [PubMed]
- Watters, E.R.; Martin, G. Health Outcomes Following Childhood Maltreatment: An Examination of the Biopsychosocial Model. J. Aging Health 2021, 33, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Bryce, I.; Collier, S. A Systematic Literature Review of the Contribution Accumulation Makes to Psychological and Physical Trauma Sustained through Childhood Maltreatment. Trauma Care 2022, 2, 307–329. [Google Scholar] [CrossRef]
- Kramer, D.N.; Landolt, M.A. Early Psychological Intervention in Accidentally Injured Children Ages 2–16: A Randomized Controlled Trial. Eur. J. Psychotraumatol. 2014, 5, 24402. [Google Scholar] [CrossRef]
- Smith, L. Adverse Childhood Experiences (ACEs): Interventions in Education; Iriss: Bradenton, FL, USA, 2018; Available online: https://www.iriss.org.uk/sites/default/files/2018-04/iriss-esss-outline-adverse-childhood-experiences-2018-4-23.pdf (accessed on 5 January 2024).
- Baldwin, J.R.; Danese, A. Are ACE Scores Useful for Identifying Individuals at Risk of Health Problems? The Association for Children and Adolescent Mental Health: London, UK, 2021. [Google Scholar] [CrossRef]
- Baldwin, J.R.; Caspi, A.; Meehan, A.J.; Ambler, A.; Arseneault, L.; Fisher, H.L.; Harrington, H.; Matthews, T.; Odgers, C.L.; Poulton, R.; et al. Population v.s. Individual Prediction of Poor Health from Results of Adverse Childhood Experiences Screening. JAMA Pediatr. 2021, 175, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Rod, N.H.; Bengtsson, J.; Elsenburg, L.K.; Taylor-Robinson, D.; Rieckmann, A. Hospitalisation Patterns Among Children Exposed to Childhood Adversity: A Population-Based Cohort Study of Half a Million Children. Lancet Public Health 2021, 6, e826–e835. [Google Scholar] [CrossRef] [PubMed]
- Ghosh Ippen, C.; Harris, W.W.; Van Horn, P.; Lieberman, A.F. Traumatic and Stressful Events in Early Childhood: Can Treatment Help Those at Highest Risk? Child Abuse Negl. 2011, 35, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.; Donkin, A. The Impact of Adverse Experiences in the Home on the Health of Children and Young People, and Inequalities in Prevalence and Effects; UCL Press Institute of Health Equity: London, UK, 2015. [Google Scholar]
- Bellis, M.A.; Hughes, K.; Leckenby, N.; Jones, L.; Baban, A.; Kachaeva, M.; Povilaitis, R.; Pudule, I.; Qirjako, G.; Ulukol, B.; et al. Adverse Childhood Experiences and Associations with Health-Harming Behaviours in Young Adults: Surveys in Eight Eastern European Countries. Bull. World Health Organ. 2014, 92, 641–655. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.; Ford, K.; Bellis, M.A.; Glendinning, F.; Harrison, E.; Passmore, J. Health and Financial Costs of Adverse Childhood Experiences in 28 European Countries: A Systematic Review and Meta-analysis. Lancet Public Health 2021, 6, e848–e857. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adverse Childhood Experiences International Questionnaire. 2018. Available online: https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq) (accessed on 28 September 2023).
- Karatekin, C.; Hill, M. Expanding the Original Definition of Adverse Childhood Experiences (ACEs). J. Child Adolesc. Trauma 2019, 12, 289–306. [Google Scholar] [CrossRef] [PubMed]
- Turner, H.A.; Finkelhor, D.; Mitchell, K.J.; Jones, L.M.; Henly, M. Strengthening the Predictive Power of Screening for Adverse Childhood Experiences (ACEs) in Younger and Older Children. Child Abuse Negl. 2020, 107, 104522. [Google Scholar] [CrossRef] [PubMed]
- Burke-Harris, N. Toxic Childhood Stress: The Legacy of Early Trauma and How to Heal; Bluebird: Duluth, GA, USA, 2018. [Google Scholar]
- Bernard, D.L.; Smith, Q.; Lanier, P. Racial Discrimination and Other Adverse Childhood Experiences as Risk Factors for Internalizing Mental Health Concerns Among Black Youth. J. Trauma. Stress 2022, 35, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Hartas, D. Assessing the Foundational Studies on Adverse Childhood Experiences. Soc. Policy Soc. 2019, 18, 435–443. [Google Scholar] [CrossRef]
- Kelly-Irving, M.; Delpierre, C. A Critique of the Adverse Childhood Experiences Framework in Epidemiology and Public Health: Uses and Misuses. Soc. Policy Soc. 2019, 18, 445–456. [Google Scholar] [CrossRef]
- Singer, M.; Bulled, N.; Ostrach, B.; Mendenhall, E. Syndemics and the Biosocial Conception of Health. Lancet 2017, 389, 941–950. [Google Scholar] [CrossRef] [PubMed]
- McKenchie, A. Stigma, Shame and the Aces Movement. The Best Start for Scotland’s Children; Upstart: Isle of Skye, UK, 2019; Available online: https://upstart.scot/stigma-shame-and-the-aces-movement/ (accessed on 5 January 2024).
- Allen, T.G.; Jackson, A.; Johnson, D.N.; Jordan, D.D. Preparing North Carolina Principals for Trauma-Sensitive Leadership. J. Organ. Educ. Leadersh. 2020, 5, 5. [Google Scholar]
- Berger, E.; O’Donohue, K.; La, C.; Quinones, G.; Barnes, M. Early Childhood Professionals’ Perspectives on Dealing with Trauma of Children. Sch. Ment. Health 2023, 15, 300–311. [Google Scholar] [CrossRef]
- Malcolm, A.; Pikoos, T.D.; Grace, S.A.; Castle, D.J.; Rossell, S.L. Childhood Maltreatment and Trauma Is Common and Severe in Body Dysmorphic Disorder. Compr. Psychiatry 2021, 109, 152256. [Google Scholar] [CrossRef] [PubMed]
- Dvir, Y.; Ford, J.D.; Hill, M.; Frazier, J.A. Childhood Maltreatment, Emotional Dysregulation, and Psychiatric Comorbidities. Harv. Rev. Psychiatry 2014, 22, 149–161. [Google Scholar] [CrossRef]
- Panlilio, C.C.; Ferrara, A.; MacNeill, L. Trauma, Self-Regulation, and Learning. In Trauma-Informed Schools; Springer: Cham, Switzerland, 2019; pp. 61–78. [Google Scholar] [CrossRef]
- Chen, P.; Zhang, Q.; Sun, X.; Ye, X.; Wang, Y.; Yang, X. How Do Childhood Abuse and Neglect Affect Prosocial Behavior? The Mediating Roles of Different Empathic Components. Front. Psychol. 2022, 13, 1051258. [Google Scholar] [CrossRef] [PubMed]
- Krasnoff, B. A Practitioner’s Guide to Educating Traumatized Children; Education Northwest: Portland, OR, USA, 2015. [Google Scholar]
- National Scientific Council on the Developing Child. Excessive Stress Disrupts the Architecture of the Developing Brain; Harvard University: Cambridge, MA, USA, 2007. [Google Scholar]
- Hunter-Dehn, A. A Trauma-Informed Transition Model for New Entrants with Dysregulated Behaviours. N. Z. J. Educ. Stud. 2021, 56, 301–314. [Google Scholar] [CrossRef]
- Kanine, R.M.; Jackson, Y.; Huffhines, L.; Barnett, A.; Stone, K.J. A Pilot Study of Universal Teacher–Child Interaction Training at a Therapeutic Preschool for Young Maltreated Children. Topics Early Child. Spec. Educ. 2018, 38, 146–161. [Google Scholar] [CrossRef]
- Smith, K.E.; Pollak, S.D. Early Life Stress and Development: Potential Mechanisms for Adverse Outcomes. J. Neurodev. Disord. 2020, 12, 34. [Google Scholar] [CrossRef]
- Centre on the Developing Child. Building the Brains ‘Air Traffic’ Control System: How Early Experiences Shape the Development of Executive Function; Working Paper No 11; Harvard University: Cambridge, MA, USA, 2010. [Google Scholar]
- Hale, R.; Wendler, M.C. Evidence-Based Practice: Implementing Trauma-Informed Care of Children and Adolescents in the Inpatient Psychiatric Setting. J. Am. Psychiatr. Nurs. Assoc. 2023, 29, 161–170. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. Trauma-Informed Care in Behavioral Health Services. 2014. Available online: https://store.samhsa.gov/product/TIP-57-Trauma-Informed-Care-in-Behavioral-Health-Services/SMA14-4816 (accessed on 9 December 2023).
- Menschner, C.; Maul, A. Key Ingredients for Successful Trauma-Informed Care Implementation; Center for Health Care Strategies: Hamilton, NJ, USA, 2016. Available online: https://www.samhsa.gov/sites/default/files/programs_campaigns/childrens_mental_health/atc-whitepaper-040616.pdf (accessed on 5 August 2023).
- Temkin, D.; Harper, K.; Stratford, B.; Sacks, V.; Rodriguez, Y.; Bartlett, J.D. Moving Policy Toward a Whole School, Whole Community, Whole Child Approach to Support Children Who Have Experienced Trauma. J. Sch. Health 2020, 90, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.S.; Crosby, S.; Vanderhaar, J. Trauma-Informed Practices in Schools Across Two Decades: An Interdisciplinary Review of Research. Rev. Res. Educ. 2019, 43, 422–452. [Google Scholar] [CrossRef]
- Brown, E.C.; Freedle, A.; Hurless, N.L.; Miller, R.D.; Martin, C.; Paul, Z.A. Preparing Teacher Candidates for Trauma-Informed Practices. Urban Educ. 2022, 57, 662–685. [Google Scholar] [CrossRef]
- Loomis, A.M. The Role of Preschool as a Point of Intervention and Prevention for Trauma-Exposed Children: Recommendations for Practice, Policy, and Research. Topics Early Child. Spec. Educ. 2018, 38, 134–145. [Google Scholar] [CrossRef]
- McClain, M.P. Teacher Candidates’ Perceptions of Preparedness of Teaching Students Who Experience Trauma. J. Teach. Educ. Educ. 2021, 10, 5–23. [Google Scholar]
- Miller, K.; Stipp, K. Preservice Teacher Burnout: Secondary Trauma and Self-Care Issues in Teacher Education. Issues Teach. Educ. 2019, 28, 28–45. [Google Scholar]
- Shamblin, S.; Graham, D.; Bianco, J.A. Creating Trauma-Informed Schools for Rural Appalachia: The Partnerships Program for Enhancing Resiliency, Confidence and Workforce Development in Early Childhood Education. Sch. Ment. Health 2016, 8, 189–200. [Google Scholar] [CrossRef]
- Kim, S.; Crooks, C.V.; Bax, K.; Shokoohi, M. Impact of Trauma-Informed Training and Mindfulness-Based Social-Emotional Learning Program on Teacher Attitudes and Burnout: A Mixed-Methods Study. Sch. Ment. Health 2021, 13, 55–68. [Google Scholar] [CrossRef]
- Education Scotland. Nurture, Adverse Childhood Experiences and Trauma Informed Practice: Making the Links between These Approaches; Education Scotland: Livingston, UK, 2018. Available online: https://education.gov.scot/media/qorfmno3/inc83-making-the-links-nurture-aces-and-trauma.pdf (accessed on 12 September 2023).
- Riley, G.S.; Bailey, J.W.; Bright, D.; Davies, A.R. Knowledge and Awareness of Adverse Childhood Experiences (ACEs) in the Public Service Workforce in Wales: A National Survey; Cardiff Public Health Wales NHS Trust: Cardiff, UK, 2019. [Google Scholar]
- Brunzell, T.; Stokes, H.; Waters, L. Why Do You Work with Struggling Students? Teacher Perceptions of Meaningful Work in Trauma-Impacted Classrooms. Aust. J. Teach. Educ. 2018, 43, 116–142. [Google Scholar] [CrossRef]
- Brunzell, T.; Stokes, H.; Waters, L. Shifting Teacher Practice in Trauma-Affected Classrooms: Practice Pedagogy Strategies within a Trauma-Informed Positive Education Model. Sch. Ment. Health 2019, 11, 600–614. [Google Scholar] [CrossRef]
- Rubbi Nunan, J.S. South African Teachers’ Perspectives of What Causes Students to Exhibit Challenging Behavior in Primary Schools. J. Educ. 2021, 202, 478–487. [Google Scholar] [CrossRef]
- Department of Children, Equality, Disability, Integration and Youth (DCEDIY). LINC Capitation & Incentives; DCEDYI: Dublin, Ireland, 2019; Available online: https://lincprogramme.ie/about__trashed/capitation-and-incentives/#:~:text=Only%20one%20LINC%20Graduate%20can,relation%20to%20one%20graduate%20only (accessed on 12 September 2023).
- Douglas, F. History of the Irish Pre-School Playgroups Association; Institute of Public Policy Analysis: Abuja, Nigeria, 1994. [Google Scholar]
- Centre for Early Childhood Development & Education. Siolta: The National Quality Framework for Early Childhood Education; Stationery Office: London, UK, 2006. [Google Scholar]
- National Council for Curriculum and Assessment. Aistear: The Early Childhood Curriculum Framework. 2009. Available online: https://ncca.ie/media/4151/aistear_theearlychildhoodcurriculumframework.pdf (accessed on 11 November 2023).
- Lynch, F. The Early Years Sector: A Case Study in Policy Development; UNESCO Child and Family Research Centre, University of Galway: Galway, Ireland, 2023. [Google Scholar]
- Tusla. Developing Policies, Procedures and Statements in Early Childhood Education and Care Services: A Practical Guide; Early Years Inspectorate, Tusla: Dublin, Ireland, 2018. [Google Scholar]
- European Commission. European Education Area Strategic Framework. Working Group on Early Childhood Education and Care (ECEC)—Conditions of Service for Teachers Working in Early and School Education. Available online: https://eurydice.eacea.ec.europa.eu/national-education-systems/ireland/conditions-service-teachers-working-early-childhood-and-school (accessed on 12 September 2023).
- Pobal. Annual Early Years Sector Profile Report; Pobal: Dublin, Ireland, 2021; Available online: https://www.pobal.ie/app/uploads/2022/05/Pobal_22_EY_20-21-Report_final_2.pdf (accessed on 12 September 2023).
- Prevention and Early Intervention Network (PEIN). Adverse Childhood Experiences (ACEs): Holding the Child’s Hand in Prevention and Early Intervention for Children and Families; PEIN: Limerick, Ireland, 2019; Available online: https://www.pein.ie/wp-content/uploads/2019/10/PEIN-ACEs-Policy-Paper_Every-Childhood-Lasts-a-Lifetime_2019-10.pdf (accessed on 12 September 2023).
- Lotty, M. Childhood trauma in mind: Integrating Trauma-Informed Care in ECEC. Leanbh Óg 2020, 13, 105–121. [Google Scholar]
- Department of Education and Skill. Professional Award Criteria and Guidelines for Initial Professional Education (Level 7 and Level 8) Degree Programmes for the Early Learning and Care (ELC) Sector in Ireland; Department of Education and Skill: London, UK, 2019. [Google Scholar]
- Brunzell, T.; Stokes, H.; Waters, L. Trauma-Informed Flexible Learning: Classrooms That Strengthen Regulatory Abilities. Int. J. Child Youth Fam. Stud. 2016, 7, 218–239. [Google Scholar] [CrossRef]
- Hickey, G.; Smith, S.; O’Sullivan, L.; McGill, L.; Kenny, M.; MacIntyre, D.; Gordon, M. Adverse Childhood Experiences and Trauma Informed Practices in Second Chance Education Setting in the Republic of Ireland: An Inquiry-Based Study. Child. Youth Serv. Rev. 2020, 118, 105338. [Google Scholar] [CrossRef]
- French, G. Key Elements of Good Practice to Support the Learning and Development of Children from Birth to Three; Department of Children and Youth Affairs: Dublin, Ireland, 2019; Available online: https://ncca.ie/media/4123/key-elements-of-good-practice-to-support-the-learning-and-development-of-children-birth-three-drgfrench.pdf (accessed on 21 August 2023).
- Craig, S. The Trauma-Sensitive Teacher. Educ. Leadersh. 2016, 74, 28–32. [Google Scholar]
- Page, J. Characterising the Principles of Professional Love in Early Childhood Care and Education. Int. J. Early Years Educ. 2018, 26, 125–141. [Google Scholar] [CrossRef]
- Grimmer, T. Developing a Loving Pedagogy in the Early Years—How Love Fits with Professional Practice; Routledge: London, UK, 2021. [Google Scholar]
- Buratti, S. The Importance of Trauma-Sensitive Language; Australian Childhood Foundation: Melbourne, Australia, 2024; Available online: https://professionals.childhood.org.au/prosody/2024/03/the-importance-of-trauma-sensitive-language/ (accessed on 12 September 2023).
- Bartlett, J.D.; Smith, S.; Bringewatt, E. Helping Young Children Who Have Experienced Trauma: Policies and Strategies for Early Care and Education; Child Trends: Washington, DC, USA, 2017. [Google Scholar]
- Whitaker, R.C.; Herman, A.N.; Dearth-Wesley, T.; Smith, H.G.; Burnim, S.B.; Myers, E.L.; Saunders, A.M.; Kainz, K. Effect of a Trauma-Awareness Course on Teachers’ Perceptions of Conflict with Preschool-Aged Children from Low-Income Urban Households: A Cluster Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e193193. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, C.; Butler, J.; O’ Neill, C. The Provision of Trauma Awareness Training in the Early Childhood Education & Care Profession: A Systematic Review. Early Child. Educ. J. 2023, 1–19. [Google Scholar] [CrossRef]
- Hambrick, E.P.; Brawner, T.W.; Perry, B.D. Timing of Early-Life Stress and the Development of Brain-Related Capacities. Front. Behav. Neurosci. 2019, 13, 183. [Google Scholar] [CrossRef]
- Nicholson, J.; Perez, L.; Kurtz, J. Trauma-Informed Practices for Early Childhood Educators: Relationship-Based Approaches That Reduce Stress, Build Resilience and Support Healing in Young Children; Routledge: London, UK, 2019. [Google Scholar]
- Siegel, D.; Payne Bryson, T. The Whole-Brain Child: 12 Proven Strategies to Nurture Your Child’s Developing Mind; Robinson: London, UK, 2012. [Google Scholar]
- Revilla, M.; Höhne, J.K. How Long Do Respondents Think Online Surveys Should Be? New Evidence from Two Online Panels in Germany. Int. J. Mark. Res. 2020, 62, 538–545. [Google Scholar] [CrossRef]
- Dye, H. The Impact and Long-Term Effects of Childhood Trauma. J. Hum. Behav. Soc. Environ. 2018, 28, 381–392. [Google Scholar] [CrossRef]
- Lindert, J.; von Ehrenstein, O.S.; Grashow, R.; Gal, G.; Braehler, E.; Weisskopf, M.G. Sexual and Physical Abuse in Childhood Is Associated with Depression and Anxiety over the Life Course: Systematic Review and Meta-analysis. Int. J. Public Health 2014, 59, 359–372. [Google Scholar] [CrossRef]
- Teague, C.M. Developmental Trauma Disorder: A Provisional Diagnosis. J. Aggress. Maltreat. Trauma 2013, 22, 611–625. [Google Scholar] [CrossRef]
- van der Kolk, B.A. The Developmental Impact of Childhood Trauma. In Understanding Trauma: Integrating Biological, Clinical, and Cultural Perspectives; Kirmayer, L.J., Lemelson, R., Barad, M., Eds.; Cambridge University Press: Cambridge, UK, 2007; pp. 224–241. [Google Scholar] [CrossRef]
- Nurius, P.S.; Logan-Greene, P.; Green, S. Adverse Childhood Experiences (ACE) within a Social Disadvantage Framework: Distinguishing Unique, Cumulative, and Moderated Contributions to Adult Mental Health. J. Prev. Interv. Community 2012, 40, 278–290. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B. Interfamily Violence and Its Impact on Traveller Mental Health; Exchange House Ireland National Traveller Service: Dublin, Ireland, 2019. [Google Scholar]
- Coogan, A. The Key Issues Affecting the Traveller Community; Oireachtas: Dublin, Ireland, 2019. [Google Scholar]
- Lambert, S.; Gill-Emerson, G.; Horan, A.; Naughton, A. Moving Towards Trauma Informed Care. A Model of Research and Practice; Cork Simon Community: Cork, Ireland, 2017; Available online: http://www.corksimon.ie/aces-at-cork-simon/ (accessed on 10 October 2023).
- Murray, A.; Morgan, M. Growing up in Ireland: National Longitudinal Study of Children; Department of Children and Youth Affairs: Dublin, Ireland, 2019. [Google Scholar]
- Sidamon-Eristoff, A.E.; Cohodes, E.M.; Gee, D.G.; Peña, C.J. Trauma Exposure and Mental Health Outcomes Among Central American and Mexican Children Held in Immigration Detention at the United States-Mexico Border. Dev. Psychobiol. 2022, 64, e22227. [Google Scholar] [CrossRef] [PubMed]
- The College of Psychiatrists of Ireland. Direct Provision: A Broken System That Must Be Fixed. 2017. Available online: https://www.irishpsychiatry.ie/blog/direct-provision-broken-system-must-be-fixed/ (accessed on 1 September 2023).
- Fazel, M.; Wheeler, J.; Danesh, J. Prevalence of Serious Mental Disorder in 7000 Refugees Resettled in Western Countries: A Systematic Review. Lancet 2005, 365, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Bernard, C. An Exploration of How Social Workers Engage Neglectful Parents from Affluent Backgrounds in the Child Protection System; Goldsmiths University of London: London, UK, 2017. [Google Scholar]
- Bernard, C. Recognizing and Addressing Child Neglect in Affluent Families. Child Fam. Soc. Work 2019, 24, 340–347. [Google Scholar] [CrossRef]
- Strauss, M.; Roderick, J. Handling Cases of Affluent Neglect in Schools; Farrer & Co.: London, UK, 2022; Available online: https://www.farrer.co.uk/globalassets/handling-cases-of-affluent-neglect-in-schools.pdf (accessed on 2 December 2023).
- Bilbrey, J.B.; Castanon, K.L.; Copeland, R.B.; Evanshen, P.A.; Trivette, C.M. Primary Early Childhood Educators’ Perspectives of Trauma-Informed Knowledge, Confidence, and Training. Aust. Educ. Res. 2024, 51, 67–88. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.D.; Smith, S. The Role of Early Care and Education in Addressing Early Childhood Trauma. Am. J. Community Psychol. 2019, 64, 359–372. [Google Scholar] [CrossRef]
- Morgan, M.; Rochford, S.; Sheehan, A. Adversity in Childhood—Outcomes, Risk and Resilience; Centre for Effective Services: Dublin, Ireland, 2016. [Google Scholar]
- Wilson-Ching, M.; Berger, E. Relationship Building Strategies within Trauma Informed Frameworks in Educational Settings: A Systematic Literature Review. Curr. Psychol. 2024, 43, 3464–3485. [Google Scholar] [CrossRef]
- Post, P.B.; Grybush, A.L.; Elmadani, A.; Lockhart, C.E. Fostering Resilience in Classrooms through Child-Teacher Relationship Training [Personnel Attitudes & Job Satisfaction 3650]. Int. J. Play Ther. 2020, 29, 9–19. [Google Scholar] [CrossRef]
- Saint Gilles, M.P.; Carlson, J.S. A Pilot Study on the Effects of a Supplemental Trauma Intervention within a Head Start Preschool Program. Res. Pract. Sch. 2020, 7, 49–69. [Google Scholar]
- Singh, C.D.; Andrews, N.C.Z.; Motz, M.; Pepler, D.J.; Leslie, M.; Zuberi, S. Trauma-Informed and Relational Approaches to Service Provision: Building Community-Based Project Capacity to Respond to Interpersonal Violence through a National Initiative. BMC Public Health 2020, 20, 1833. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R. The Trauma and Attachment-Aware Classroom: A Practical Guide to Supporting Children Who Have Encountered Trauma and Adverse Childhood Experiences; Jessica Kingsley Publishers: London, UK, 2019. [Google Scholar]
- De Thierry, B. The Simple Guide to Child Trauma; Jessica Kingsley Publishers: London, UK, 2016. [Google Scholar]
- Treisman, K. Good Relationships Are the Key to Healing Trauma. TEDx Talks. YouTube. 2018. Available online: https://www.youtube.com/watch?v=PTsPdMqVwBg (accessed on 6 January 2024).
- Wolpow, R.; Johnson, M.M.; Hertel, R.; Kincaid, S.O. The Heart of Learning and Teaching: Compassion, Resiliency, and Academic Success; Office of Superintendent of Public Instruction (OSPI) Compassionate Schools: Olympia, WA, USA, 2009; Available online: https://www.k12.wa.us/sites/default/files/public/compassionateschools/pubdocs/theheartoflearningandteaching.pdf (accessed on 10 January 2024).
- Murray, D.W.; Rackers, H.; Meyer, A.; McKenzie, K.J.; Malm, K.; Sepulveda, K.; Heath, C. Co-regulation as a Support for Older Youth in the Context of Foster Care: A Scoping Review of the Literature. Prev. Sci. 2023, 24, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Phillips, D.; Austin, L.J.E.; Whitebook, M. The Early Care and Education Workforce. Future Child. 2016, 26, 139–158. [Google Scholar] [CrossRef]
- Sun, Y.; Blewitt, C.; Minson, V.; Bajayo, R.; Cameron, L.; Skouteris, H. Trauma-Informed Interventions in Early Childhood Education and Care Settings: A Scoping Review. Trauma Violence Abus. 2024, 25, 648–662. [Google Scholar] [CrossRef]
- Jeong, D.; Aggarwal, S.; Robinson, J.; Kumar, N.; Spearot, A.; Park, D.S. Exhaustive or Exhausting? Evidence on Respondent Fatigue in Long Surveys. J. Dev. Econ. 2023, 161, 102992. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | % |
|---|---|---|
| Gender | ||
| Female | 1025 | 97.9 |
| Male | 19 | 1.8 |
| Nonbinary | 2 | 0.2 |
| Prefer not to say | 2 | 0.2 |
| Age | ||
| 18–25 years | 124 | 11.8 |
| 26–35 years | 278 | 26.4 |
| 36–45 years | 271 | 25.7 |
| 46–55 years | 256 | 24.3 |
| 55–60 years | 76 | 7.2 |
| ≥60 years | 48 | 4.6 |
| Role | ||
| Owner–Manager | 225 | 21.4 |
| Manager | 261 | 24.8 |
| Assistant Manager | 66 | 6.3 |
| Room Leader | 170 | 16.1 |
| ECEC Practitioner | 174 | 16.5 |
| ECCE Practitioner | 67 | 6.4 |
| AIM Practitioner | 19 | 1.8 |
| Other | 71 | 6.7 |
| Years of Experience | ||
| Less than 5 years | 230 | 22.1 |
| 5–9 years | 201 | 19.3 |
| 10–20 years | 385 | 36.9 |
| 21–29 years | 153 | 14.7 |
| ≥30 years | 73 | 7.0 |
| Setting Type | ||
| Private | 583 | 57.2 |
| Community | 409 | 40.1 |
| Unsure | 9 | 0.1 |
| Other | 19 | 1.9 |
| Trauma Experience | n | % |
|---|---|---|
| Of children from: | ||
| One-parent family | 857 | 89.8 |
| EAL family | 827 | 86.7 |
| The travelling community | 352 | 36.9 |
| Low-income families | 827 | 86.7 |
| Roma families | 198 | 20.1 |
| Of children living: | ||
| In foster care | 332 | 34.5 |
| In direct provision | 168 | 18.0 |
| In homeless services | 175 | 18.3 |
| In an unsafe neighbourhood | 281 | 30.0 |
| Of children with: | ||
| A diagnosed disability or additional need | 861 | 90.3 |
| An incarcerated parent | 244 | 25.6 |
| Of children who: | ||
| Lost a parent to deportation | 34 | 3.5 |
| Have family member(s) who come to the attention of An Garda Síochána | 168 | 18.0 |
| Education Level | (n) | (%) |
|---|---|---|
| QQ1 Level 5 | 56 | 5.3 |
| QQI Level 6 | 243 | 27.2 |
| Level 7 Ordinary Degree—in ECEC | 138 | 15.4 |
| Level 8 Honours Degree—in ECEC | 285 | 31.9 |
| Level 7 Ordinary Degree—Montessori Education | 22 | 2.5 |
| Level 8 Honours Degree—Montessori Education | 24 | 2.7 |
| Level 9 Master’s Degree | 73 | 8.2 |
| Level 10 Ph.D. | 3 | 0.3 |
| No Relevant Qualification | 7 | 0.8 |
| Other | 43 | 4.8 |
| Response Scale | Unsure | Did Not Experience | Experienced Sometimes | Experienced Frequently |
|---|---|---|---|---|
| Trauma and Adverse Childhood Experience | (%) | |||
| Parental separation, divorce, or bereavement | 1.1 | 9.8 | 35.0 | 54.1 |
| Emotional neglect | 6.4 | 27.6 | 42.5 | 23.5 |
| Household mental illness | 13.5 | 28.0 | 34.8 | 23.7 |
| Physical neglect | 5.1 | 39.0 | 39.4 | 16.4 |
| Emotional abuse | 8.7 | 35.5 | 35.9 | 20.0 |
| Household substance abuse | 17.7 | 30.1 | 31.6 | 20.7 |
| Exposure to domestic violence | 15.8 | 33.3 | 31.3 | 19.6 |
| Racism | 22.1 | 38.8 | 26.0 | 13.1 |
| Peer violence (bullying) | 17.8 | 47.5 | 24.4 | 10.3 |
| Witnessing community violence | 26.9 | 43.4 | 15.8 | 13.9 |
| Homelessness | 16.1 | 54.8 | 14.1 | 15.0 |
| Incarcerated household member | 15.8 | 56.9 | 17.3 | 10.0 |
| Halting sites | 13.9 | 60.1 | 13.7 | 12.2 |
| Direct provision | 14.3 | 61.9 | 15.2 | 8.6 |
| Response Percentage (%) of Areas Impacted by Trauma | |||
|---|---|---|---|
| Response Scale | Impacted | Not Impacted | Unsure |
| Child Development: Impacted Areas | |||
| Social Development | 94.8 | 2.8 | 2.4 |
| Emotional Development | 96.4 | 2.0 | 1.6 |
| Cognitive Development | 93.2 | 4.1 | 2.7 |
| Physical Development | 86.5 | 10.5 | 3.1 |
| Creativity | 89.8 | 6.1 | 4.0 |
| Speech and Language | 93.4 | 3.9 | 2.7 |
| Self-Esteem and Confidence | 96.7 | 2.0 | 1.3 |
| Distressing Behaviour | 97.1 | 1.5 | 1.5 |
| Self-Regulation | 94.3 | 3.5 | 2.2 |
| Holistic Development | 92.7 | 3.6 | 3.6 |
| Response Scale | Experienced | Did Not Experience | Unsure | |||
|---|---|---|---|---|---|---|
| Post Trauma Behaviours | (%) | (n) | (%) | (n) | (%) | (n) |
| Issues with fostering and maintaining relationships | 55.3 | 392 | 31.0 | 220 | 13.6 | 96 |
| Poor attention span and concentration | 79.3 | 567 | 12.2 | 87 | 8.5 | 61 |
| Irregular attendance | 75.0 | 472 | 18.3 | 130 | 6.8 | 48 |
| Appears disassociated, unresponsive, or detached | 70.2 | 499 | 21.5 | 153 | 8.3 | 59 |
| Difficulty regulating emotions | 81.2 | 575 | 12.4 | 88 | 6.4 | 45 |
| On high alert for threat | 54.5 | 385 | 32.7 | 231 | 12.9 | 91 |
| Expressions of anxiety and panic | 70.2 | 497 | 22 | 156 | 7.8 | 55 |
| Overly aggressive/angry/unpredictable/explosive | 73.3 | 519 | 18.8 | 133 | 7.9 | 56 |
| Increase of somatic symptoms (headaches, stomach aches) | 30.8 | 378 | 57.8 | 217 | 15.5 | 109 |
| Blocking their ears when voices are raised | 63.7 | 450 | 27.5 | 194 | 8.9 | 63 |
| Difficulty with transitions | 78.4 | 552 | 14.9 | 105 | 6.8 | 48 |
| Difficulty responding to authority and redirection | 75.1 | 532 | 17.1 | 121 | 7.8 | 55 |
| Tired or fatigue | 72.6 | 512 | 19.2 | 135 | 8.2 | 58 |
| Engages in self-injurious behaviour | 31.7 | 223 | 54.1 | 380 | 14.2 | 100 |
| Engages in ‘risky’ behaviour | 55.0 | 386 | 32.9 | 231 | 12.0 | 84 |
| Limited language for feeling and emotional states | 70.2 | 489 | 20.7 | 144 | 9.2 | 64 |
| Avoidant attachment style | 63.1 | 436 | 25.7 | 178 | 11.1 | 77 |
| Difficulty with logical thinking, reasoning, and problem solving | 68.1 | 476 | 22.9 | 160 | 9.0 | 63 |
| Poor self-worth, self-esteem, and confidence | 71.2 | 500 | 20.6 | 145 | 8.1 | 57 |
| Distressed behaviour | 71.3 | 497 | 21.2 | 148 | 7.5 | 52 |
| Response Percentage (%) of Participants Implementing Targeted Strategies | |||||
|---|---|---|---|---|---|
| Response Scale | Never | Rarely | Sometimes | Often | Very Often |
| Strategy | |||||
| Relationship-based approaches/key-person approach | 4.2 | 4.0 | 13.1 | 24.6 | 54.2 |
| Promote physical activity | 3.6 | 1.8 | 12.0 | 26.3 | 56.4 |
| Trauma-sensitive/non-triggering language | 8.9 | 14.2 | 27.9 | 25.9 | 23.2 |
| Consistent, predictable routine | 2.6 | 1.3 | 5.3 | 24.5 | 66.3 |
| Identify triggers | 6.4 | 7.0 | 17.6 | 31.3 | 37.8 |
| Understand trauma-response behaviour | 6.8 | 9.3 | 25.1 | 32.2 | 26.6 |
| Model non-violent relationships | 2.8 | 1.6 | 5.0 | 19.1 | 71.5 |
| Avoid exclusionary practices | 4.6 | 1.8 | 7.2 | 14.0 | 72.5 |
| Encourage self-regulation through appropriate learning opportunities | 2.7 | 1.8 | 7.7 | 21.1 | 66.7 |
| Unconditional positive regard | 2.4 | 2.1 | 10.4 | 25.6 | 59.4 |
| Co-regulation | 3.1 | 2.8 | 13.3 | 29.3 | 51.5 |
| 3R’s Model (Relate, Regulate, Reason) | 6.5 | 6.2 | 16.0 | 28.9 | 42.4 |
| Response Percentage (%) of Participants Received Type of Trauma Education | |||||
|---|---|---|---|---|---|
| Response Scale | None | Very Little | Some, but Not Much | Quite In-Depth | Very In-Depth |
| Educational Construct | |||||
| Attachment Theory | 14.0 | 13.8 | 31.7 | 30.3 | 10.1 |
| Adverse Childhood Experiences | 17.7 | 26.0 | 30.9 | 18.9 | 6.6 |
| Early Childhood Trauma | 24.7 | 25.5 | 30.9 | 13.3 | 5.6 |
| Types of Stress | 22.7 | 26.2 | 32.9 | 14.0 | 4.2 |
| Brain development/Neuroscience | 16.7 | 21.0 | 29.5 | 23.6 | 9.2 |
| Trauma-Sensitive Approaches | 31.9 | 27.3 | 26.1 | 10.7 | 3.9 |
| Trauma-Sensitive Language | 35.4 | 27.9 | 24.4 | 9.5 | 2.7 |
| Holistic Health and Wellbeing | 11.7 | 17.4 | 29.9 | 27.7 | 13.4 |
| Relationship-Based Approaches | 15.8 | 17.1 | 29.4 | 24.5 | 13.1 |
| Polyvagal Theory | 58.7 | 22.3 | 12.9 | 4.7 | 1.4 |
| Trauma-Informed Practice | 45.3 | 24.8 | 18.4 | 7.7 | 3.8 |
| Co-regulation and Self-regulation | 17.7 | 24.7 | 30.7 | 19.6 | 7.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheehan, C.; Butler, J.E.; O’Neill, C. What We Don’t Know Really Will Hurt Us: Examining Trauma Awareness Knowledge, Strategies, and Training in Ireland’s Early Childhood Education and Care Profession. Educ. Sci. 2024, 14, 704. https://doi.org/10.3390/educsci14070704
Sheehan C, Butler JE, O’Neill C. What We Don’t Know Really Will Hurt Us: Examining Trauma Awareness Knowledge, Strategies, and Training in Ireland’s Early Childhood Education and Care Profession. Education Sciences. 2024; 14(7):704. https://doi.org/10.3390/educsci14070704
Chicago/Turabian StyleSheehan, Catherine, Judith E. Butler, and Cian O’Neill. 2024. "What We Don’t Know Really Will Hurt Us: Examining Trauma Awareness Knowledge, Strategies, and Training in Ireland’s Early Childhood Education and Care Profession" Education Sciences 14, no. 7: 704. https://doi.org/10.3390/educsci14070704
APA StyleSheehan, C., Butler, J. E., & O’Neill, C. (2024). What We Don’t Know Really Will Hurt Us: Examining Trauma Awareness Knowledge, Strategies, and Training in Ireland’s Early Childhood Education and Care Profession. Education Sciences, 14(7), 704. https://doi.org/10.3390/educsci14070704